Back to Journals » International Journal of Women's Health » Volume 17
Study on the Relationship Between Postpartum Birth Trauma Symptoms and the Gap in Social Support Expectations at 42 Days Postpartum
Authors Li L, Xiao L, Wu J, Li J, Chen X, Wang B
Received 29 May 2025
Accepted for publication 7 August 2025
Published 22 August 2025 Volume 2025:17 Pages 2651—2659
DOI https://doi.org/10.2147/IJWH.S535334
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Vinay Kumar
Lingling Li,1,* Lanlan Xiao,1,* Jie Wu,2 Jinxiao Li,1 Xiuping Chen,3 Bei Wang4
1Department of Obstetrics and Gynecology, Second Affiliated Hospital of Naval Medical University, Shanghai, 200003, People’s Republic of China; 2Department of Nursing, Shanghai Jiading District Maternal and Child Health Care Hospital, Shanghai, 201821, People’s Republic of China; 3Department of Obstetrics and Gynecology, Huashan Hospital, Fudan University, Shanghai, 201907, People’s Republic of China; 4Department of Nursing, Second Affiliated Hospital of Naval Medical University, Shanghai, 200003, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bei Wang, Department of Nursing, Second Affiliated Hospital of Naval Medical University, No. 415 Fengyang Road, Huangpu District, Shanghai, 200003, People’s Republic of China, Email [email protected] Xiuping Chen, Department of Obstetrics and Gynecology, Huashan Hospital, Fudan University, No. 415 Fengyang Road, Huangpu District, Shanghai, 201907, People’s Republic of China, Email [email protected]
Objective: Birth trauma affects 9% to 44% of postpartum women and significantly impacts maternal health. In China, changes in social structures have led to discrepancies between expected and actual social support, yet few studies have explored the relationship with birth trauma. This study examines the association between birth trauma symptoms at 42 days postpartum and the gap between expected and received social support.
Methods: A total of 204 postpartum women were recruited from four hospitals in Shanghai between January and March 2024. Participants completed the Chinese City Birth Trauma Scale and the Postpartum Social Support Scale. Pearson’s correlation and multiple linear regression analyses were used to evaluate associations between trauma symptoms and the social support expectation gap.
Results: Among the participants, 52.5% (107/204) were diagnosed with birth trauma. The mean trauma score was 45.01 ± 16.48. Actual social support was significantly negatively correlated with trauma symptom severity (r = – 0.426 to – 0.053, all P < 0.05), whereas the gap between expected and received support showed a significant positive correlation (r = 0.145 to 0.281, all P < 0.05). Emotional and informational support gaps had the strongest associations. Multiple linear regression further confirmed that lower household income (β = 0.171, P = 0.015), educational level below college (β = 0.282, P < 0.001), and formula feeding (β = 0.179, P = 0.010) were independent predictors of more severe birth trauma symptoms.
Conclusion: Birth trauma symptoms are common at 42 days postpartum. Significant associations were observed between higher trauma scores and both inadequate actual support and larger expectation gaps—especially in emotional and informational domains. Bridging these gaps, particularly among women of lower socioeconomic status, may help reduce psychological trauma and improve postpartum recovery.
Keywords: postpartum women, birth trauma, social support, expectation gap
Introduction
Birth trauma (BT) refers to the physical and psychological injuries or discomforts experienced or perceived by women during childbirth, representing a significant factor affecting postpartum physical and mental health.1 Recent studies indicate that the incidence of birth trauma ranges from 9% to 44% globally.2 Birth trauma not only has the potential to lead to psychological disorders such as postpartum post-traumatic stress disorder (PTSD) and postpartum depression, but it can also undermine a mother’s confidence and ability to breastfeed, which in turn affects the mother-infant relationship. These consequences may even have long-term detrimental effects on the newborn’s early development.3–5
In the context of China’s unique socio-cultural landscape, expectations for postpartum support are shaped by several historical and structural factors. The legacy of the one-child policy has led to reduced family size and the so-called “4-2-1” family structure, where two parents often bear the caregiving responsibilities for four grandparents and one child.6 This shift has placed tremendous pressure on new mothers to fulfill multiple family roles with limited intergenerational support. Additionally, pronounced rural-urban disparities persist, with rural women often lacking access to high-quality maternal health services and structured postpartum care. Migrant women living in urban areas may experience isolation due to the hukou (household registration) system, which limits access to public services and hinders the presence of extended family support. These unique factors can lead to a substantial mismatch between the support women expect and what they actually receive during the postpartum period, thereby influencing their vulnerability to birth trauma. Understanding this context is essential for tailoring support interventions that address the culturally specific needs of Chinese postpartum women.
Adequate social support is regarded as a key factor in alleviating birth trauma symptoms and facilitating maternal psychological recovery. International research has demonstrated that sufficient social support can significantly mitigate maternal psychological stress and counteract the negative effects of birth trauma.7,8 However, the transformation of China’s social structure, the prevalence of nuclear families, and the erosion of traditional family support systems have led to discrepancies between the actual social support received and the level of support that postpartum women subjectively expect or deem necessary.9,10 In this study, social support refers to tangible and intangible assistance perceived or received by the mother from family, healthcare providers, and society—covering emotional, informational, material, and comparison-based domains. The expectation gap, by contrast, is defined as the difference between the perceived importance of each type of support and the actual amount received, as measured by paired subscales in the Postpartum Social Support Scale. Such gaps may indicate unmet needs, which can trigger or worsen psychological distress during postpartum recovery. Furthermore, rural-urban disparities, the household registration system, and the growing mobility of populations have further exacerbated this gap, potentially influencing women’s experiences of birth trauma.11,12
Domestic research has primarily focused on the impact of social support on maternal emotional issues, with relatively few studies examining the relationship between the gap in social support expectations and birth trauma. In recent years, national policies have increasingly highlighted maternal health, as seen in the “China Women’s Development Outline (2021–2030)”,13 which aims to enhance maternal health protection.
Choosing 42 days postpartum as the research time point is of significant importance. Physiologically, the 42nd day postpartum marks a critical period for the recovery of maternal organs (excluding the mammary glands) to pre-pregnancy status. At this stage, maternal bodily functions stabilize, and physiological changes become relatively fixed, allowing for a more accurate evaluation of recovery from childbirth-induced trauma. Additionally, this period provides an opportunity to observe the persistence of birth trauma symptoms while minimizing the impact of unstable factors during the early postpartum recovery phase. Psychologically, by the 42nd day postpartum, most mothers have adapted to their new roles, yet emotional fluctuations remain common. The psychological effects of birth trauma are more evident and stable at this stage, facilitating the capture of postpartum mental health symptoms and their relationship with the social support expectation gap. Furthermore, the 42nd day postpartum is when most mothers return for follow-up visits, facilitating data collection and enhancing the representativeness and scientific rigor of the findings.
Thus, this study focuses on postpartum women at the 42-day follow-up to explore the relationship between birth trauma symptoms and the social support expectation gap. The study aims to clarify how this gap influences birth trauma and enriches existing research on postpartum mental health. By concentrating on the social support expectation gap, the research contributes to a deeper understanding of postpartum mental health and provides a theoretical foundation for clinical nursing practices. It also supports the development of targeted intervention strategies to improve maternal psychological well-being.
Materials and Methods
Study Participants
A convenience sampling method was adopted due to practical constraints in accessing the postpartum population within the limited study timeframe and to enable efficient recruitment across multiple hospital sites. To mitigate potential selection bias from the use of convenience sampling, recruitment was conducted across both general and specialized hospitals in Shanghai, targeting a demographically diverse postpartum population. However, the non-random nature of sampling may still limit the representativeness of the findings.
A total of 204 postpartum women were recruited from two general hospitals and two specialized hospitals in Shanghai between January and March 2024 during their routine postpartum follow-up visits. The inclusion criteria were as follows: (1) women aged 18 years or older, within 42 days postpartum; (2) those with normal communication abilities who could understand the content of the questionnaire; and (3) women diagnosed with birth trauma based on the City BiTS criteria, specifically meeting DSM-5-based Criteria A through E, with Criterion H excluded. Any participant meeting these conditions was categorized as experiencing birth trauma, regardless of total score magnitude. The exclusion criteria were: (1) women who could not cooperate due to severe postpartum complications and refused to participate after being informed of the study’s purpose; and (2) women with a score of zero on the City Birth Trauma Scale who had not experienced birth trauma.
Sample size calculation: As this study aimed to examine the association between postpartum social support expectation gaps and birth trauma symptoms, the primary independent variable was social support rather than the trauma outcome itself. Therefore, the sample size was calculated based on the structure of the Postpartum Social Support Scale, which contains 34 items. According to the general guideline for regression analysis—requiring at least 5 participants per variable—a minimum sample size of 170 participants was necessary. After accounting for an anticipated 15% non-response rate, the final required sample size was estimated to be at least 196 participants.
The study was approved by the Ethics Committee of the Second Affiliated Hospital of Naval Medical University. All participants voluntarily agreed to participate and provided written informed consent. This study was conducted in accordance with the ethical principles of the Declaration of Helsinki.
Survey Tools
Demographic Questionnaire
A self-designed demographic questionnaire was used to collect basic information on the participants. The items included age, maternal household registration, spouse’s household registration, parity, educational level, occupation, family monthly income, primary caregiver of the infant, and infant feeding methods at 42 days postpartum. This questionnaire was developed based on a review of relevant literature on maternal sociodemographic and clinical characteristics,12 and refined through discussions within the research team to ensure content relevance and cultural appropriateness.
Chinese Version of the City Birth Trauma Scale (City BiTS)
The City BiTS was developed by Ayers et al in 2018 based on the latest PTSD diagnostic criteria in DSM-5. The scale consists of two dimensions: birth-related symptoms and general symptoms, with a total of 29 items. The scale assesses whether participants experienced a traumatic event (Criterion A, 0=no, 1=yes), the frequency of related symptoms (Criteria B-E, 0=none, 1=once, 2=2-4 times, 3=more than 5 times), the duration of symptoms (Criterion F, 0=less than one month, 1=1-3 months, 2=more than three months), the level of distress and social impairment (Criterion G, 0=no, 1=sometimes, 2=yes), and whether symptoms are related to medication (Criterion H, 0=no, 1=sometimes, 2=yes). Birth trauma is diagnosed if Criteria A-E are met and Criterion H is excluded. Higher scores indicate more severe birth trauma. The scale’s Cronbach’s alpha coefficient is 0.934, with individual dimensions ranging from 0.896 to 0.906. The overall content validity index is 0.93, with individual dimensions ranging from 0.83 to 1.00. The Chinese version of the City BiTS was developed using a forward–backward translation process and underwent expert review for content validity and pilot testing for comprehension. Its psychometric properties have been validated in Chinese postpartum populations, ensuring its cultural relevance and reliability.14
Chinese Version of the Postpartum Social Support Scale (PSQ)
The PSQ was used to evaluate the postpartum social support of participants. This scale is widely used in international research and has demonstrated good reliability and validity. It consists of two subscales: the perceived importance of social support and the actual social support received, comprising 34 items across four dimensions: material support (9 items), emotional support (10 items), informational support (10 items), and comparison support (5 items). A 1–7 point Likert scale was used, with 1 indicating the least important and 7 the most important. Higher scores on the importance subscale indicate greater perceived need for support, while higher scores on the actual support subscale reflect more social support received. To quantify the social support expectation gap, we calculated the difference between the score on the importance subscale and the corresponding score on the actual support subscale for each of the four dimensions. A positive value indicates that the received support was lower than expected in that domain. Expectation gap scores were treated as continuous variables and included as predictors in subsequent statistical analyses. The Chinese version of the PSQ was adapted using standardized translation and back-translation procedures, and its content validity was confirmed through expert consultation. Previous studies have demonstrated its high internal consistency and construct validity among Chinese postpartum populations.15
Data Collection
Participants were recruited during their 42-day postpartum follow-up visits in obstetrics clinics. A face-to-face interview was conducted to collect demographic information, and participants completed the Chinese City Birth Trauma Scale and the Chinese Postpartum Social Support Scale via a QR code. The researcher provided explanations for any unclear items. To ensure completeness and reliability of the data, the electronic questionnaire included mandatory fields, dropdown menus, and response time limitations. After data collection, the researcher downloaded the raw data from the system and verified its accuracy. Questionnaires with consistent patterns of responses were excluded. A total of 240 questionnaires were distributed, and 204 valid questionnaires were returned, yielding a response rate of 85.0%. Data cleaning and statistical analysis were performed after data collection.
Statistical Methods
Statistical analyses were performed using SPSS version 27.0. Continuous variables with approximately normal distributions were presented as mean ± standard deviation and compared using independent-samples t-tests. Categorical variables were expressed as frequencies and percentages, with group comparisons conducted using chi-square tests. Normality of continuous variables was assessed using the Shapiro–Wilk test prior to conducting parametric analyses. Variables that met the assumption of normality were included in Pearson correlation analyses. Pearson’s correlation was applied to assess the relationships between postpartum trauma symptoms and the social support expectation gap, as well as the associations between the perceived importance of support, the actual support received, and the severity of birth trauma. Multiple linear regression analysis was conducted to identify independent factors associated with the severity of birth trauma symptoms. Multicollinearity among independent variables was evaluated using variance inflation factor (VIF), and all variables included in the final model had VIF values < 5, indicating acceptable levels of multicollinearity. A two-tailed P-value of <0.05 was considered statistically significant.
Results
General Demographic Information of the Participants
A total of 204 postpartum women completed the 42-day follow-up and were included in the analysis. As shown in Table 1, most participants were under 30 years old, primiparous, and held a college degree or above. The majority reported a monthly household income exceeding 8000 RMB, and mixed feeding was the most common infant feeding method.
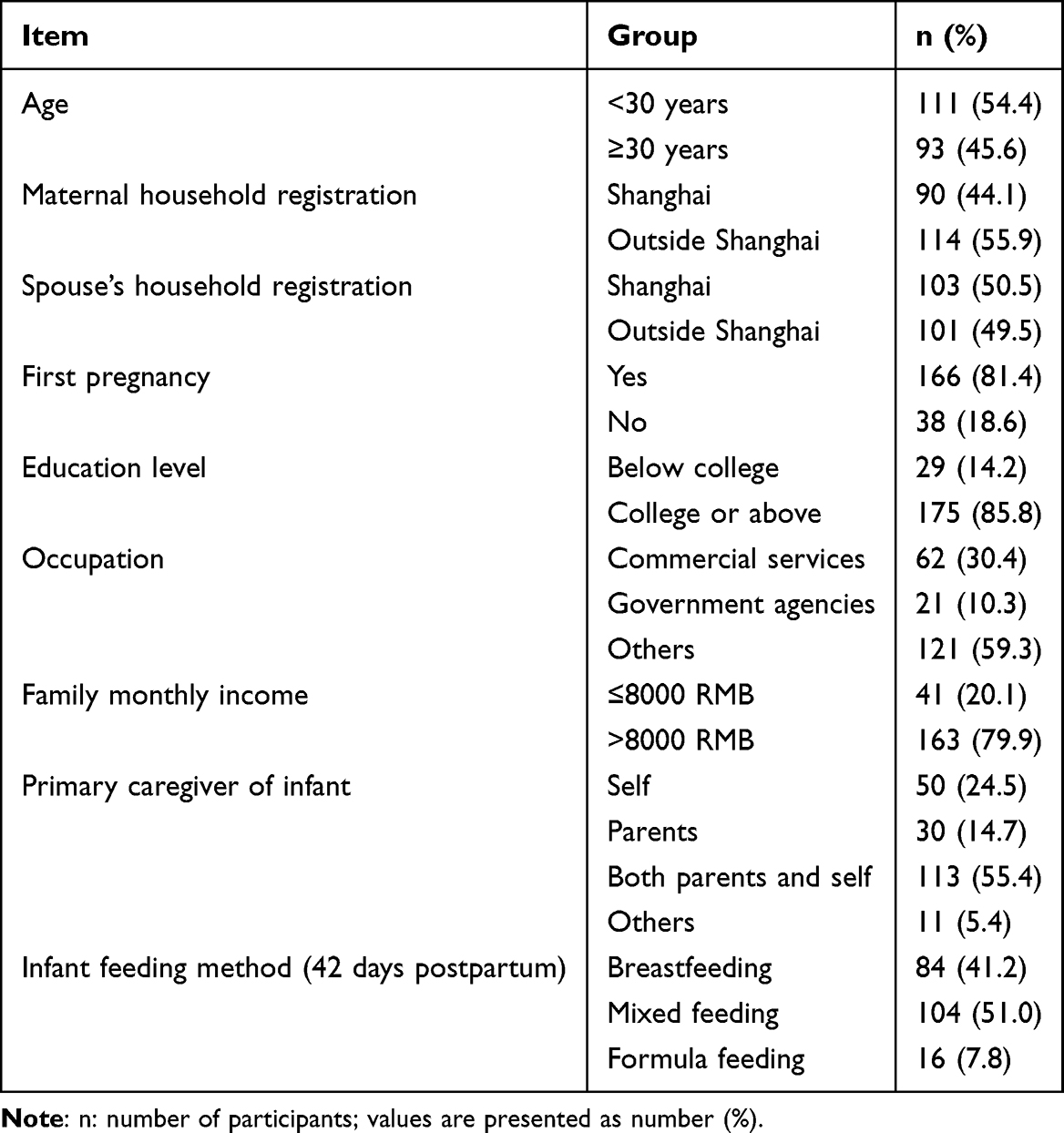 |
Table 1 General Demographic Information of Participants (n=204) |
Analysis of Birth Trauma Symptoms
Among the 204 participants, 107 women were diagnosed with birth trauma, accounting for 52.5% of the sample. According to the Chinese version of the City BiTS, the severity of birth trauma symptoms ranged from 29 to 112 points, with an average score of 45.01 ± 16.48. This result indicates that more than half of the women experienced varying degrees of birth trauma.
Analysis of Postpartum Social Support
The Postpartum Social Support Scale was used to assess both the importance and actual receipt of support. The mean score for perceived importance was 186.47 ± 40.79, while the mean score for actual received support was 180.83 ± 40.85. The average total expectation gap score was 11.81 ± 1.92. Among the four dimensions, the largest expectation gaps were observed in informational support (4.16 ± 1.63) and emotional support (3.87 ± 0.81), followed by material support (2.32 ± 0.92) and comparison support (1.45 ± 0.32) (Table 2).
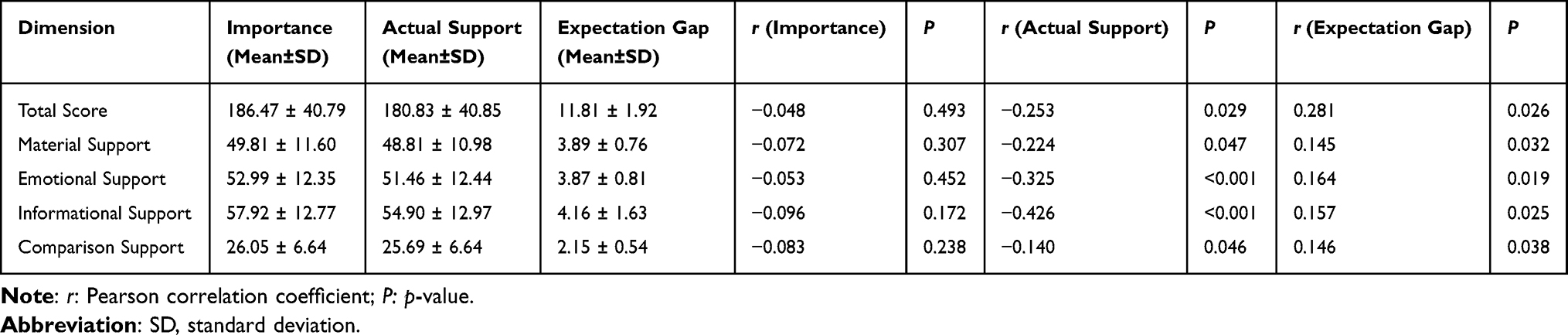 |
Table 2 Scores for Postpartum Social Support and Their Correlation with Birth Trauma Symptoms at 42 Days Postpartum (n=204) |
Relationship Between Postpartum Social Support and Birth Trauma Symptoms
Pearson correlation analysis revealed no significant correlation between perceived importance of social support and birth trauma symptoms (r = –0.048, P = 0.493). Actual received support was negatively correlated with trauma symptoms (r = –0.253, P = 0.029), while the expectation gap was positively correlated (r = 0.281, P = 0.026). Among the support dimensions, informational support (r = –0.426, P < 0.001) and emotional support (r = –0.325, P < 0.001) showed the strongest negative correlations with birth trauma symptoms based on actual support scores (Table 2).
Multivariate Linear Regression Analysis of Factors Affecting Birth Trauma Symptoms at 42 days Postpartum
A multivariate linear regression analysis was conducted with birth trauma symptom scores at 42 days postpartum as the dependent variable. The independent variables were assigned as follows: maternal household registration (1=Shanghai, 2=non-Shanghai), spouse’s household registration (1=Shanghai, 2=non-Shanghai), whether it was the first pregnancy (1=yes, 2=no), educational level (1=college degree or higher, 2=below college degree), occupation (1=commercial services, 2=government institutions, 3=other), family monthly income (1≤8000 RMB, 2=≤8000 RMB), primary caregiver of the infant (1=self, 2=parents, 3=both parents and self, 4=other), and infant feeding method at 42 days postpartum (1=breastfeeding, 2=mixed feeding, 3=formula feeding). The four social support expectation gap scores were also included as independent variables in the regression analysis. The results showed that lower family monthly income, educational level below college, and formula feeding were significant risk factors for more severe birth trauma symptoms (P<0.05), as shown in Table 3.
 |
Table 3 Multivariate Linear Regression Analysis of Factors Affecting Birth Trauma Symptoms at 42 days Postpartum (n=204) |
Discussion
In this study, 107 out of 204 women (52.5%) were diagnosed with birth trauma, which is consistent with findings from international literature, where the incidence of traumatic childbirth has been reported to range from 9.1% to 45.5%.16,17 However, there is a lack of relevant domestic research on this phenomenon. A systematic review of low- and middle-income countries indicated a higher incidence of perineal trauma related to childbirth, especially in hospital deliveries, where the incidence of episiotomy reached 46.0%, second-degree perineal tears occurred in 24.0%, and obstetric anal sphincter injuries occurred in 1.4% of cases.18 Verreault et al19 conducted a study on postpartum post-traumatic stress disorder (PTSD) and found that 16.6% of women experienced PTSD. Additionally, domestic studies have shown that the level of social support in first-time mothers is significantly negatively correlated with psychological birth trauma (P<0.05),20 suggesting that adequate social support may help reduce the psychological impact of birth trauma.
Previous studies have indicated that the mode of delivery may influence the risk of birth trauma symptoms, with assisted vaginal delivery and emergency cesarean section being potential contributing factors due to associated physical and emotional stressors.21–23 Although mode of delivery was not assessed in this study, findings from the literature underscore the multifactorial nature of postpartum trauma and highlight areas for further investigation. This study found that the social support expectation gap was positively correlated with birth trauma symptoms at 42 days postpartum, with deficiencies in emotional support and informational support having a significant impact on these symptoms (P<0.05). Garthus et al24 pointed out that when a woman’s expectations for the mode of delivery do not align with the actual delivery experience, it may increase the risk of postpartum PTSD symptoms. Additionally, discrepancies between a woman’s expectations of childbirth and her actual experience are closely associated with postpartum traumatic stress symptoms.25
Emotional support and informational support play important roles in alleviating birth trauma symptoms at 42 days postpartum, and women lacking these forms of support are more likely to experience birth trauma.26 During childbirth, emotional support from family members and professional information from medical staff significantly influence the mother’s psychological state. Good companionship and timely information can help reduce the incidence of postpartum traumatic stress symptoms.27,28 Furthermore, maternal satisfaction with medical staff, the perception of the childbirth experience, and the state of postpartum recovery are important predictive factors for postpartum traumatic stress.29,30 Therefore, families and medical institutions should provide adequate emotional support and accurate information to help women cope more effectively with the challenges of childbirth, thus reducing the risk of birth trauma symptoms and improving maternal satisfaction with the childbirth experience.
Multivariate linear regression analysis in this study indicated that lower family monthly income, educational level below college, and formula feeding were significant risk factors for more severe birth trauma symptoms (P<0.05). A qualitative study on low-income families found that economic instability and lack of social support put mothers in these families at a higher risk of postpartum depression.31 Moreover, mothers with lower education levels may face a greater psychological burden due to a lack of knowledge and resources when dealing with postpartum mental health issues.32
In terms of infant feeding methods, mothers who formula-fed their infants may experience guilt or stress due to not breastfeeding, which can negatively impact their mental health.33 Horwood et al34 found a correlation between formula feeding and postpartum depression symptoms, which may be related to dissatisfaction with the feeding method or societal pressures. Furthermore, mothers in low-income households may experience greater economic stress postpartum, which not only affects their mental health but also reduces their quality of life and increases family relationship tension.35 Studies have shown that economic stress is closely linked to family conflicts and parental depression symptoms, which may negatively affect children’s behavioral development.36,37 Therefore, social and healthcare institutions should strengthen support measures, such as providing mental health counseling, financial assistance, and parenting education, to help mothers cope more effectively with birth trauma risk, reduce psychological burden, and improve their overall quality of life.
This study has several limitations that should be acknowledged. First, the use of convenience sampling may introduce selection bias, limiting the representativeness of the sample and potentially overestimating or underestimating certain associations. Second, as all participants were recruited from a single tertiary hospital in Shanghai, the findings may not be generalizable to postpartum women in other regions, especially those in rural or less-developed settings. Third, the cross-sectional design precludes any causal inference between postpartum support gaps and trauma symptoms; longitudinal studies are warranted to explore temporal relationships and long-term outcomes. Lastly, the reliance on self-reported data may be subject to recall bias and social desirability bias, which could affect the accuracy of responses regarding support experiences and psychological symptoms.
Future research should consider longitudinal designs to examine how social support trajectories influence the development and resolution of birth trauma symptoms over time. Additionally, qualitative studies are warranted to explore the lived experiences of postpartum women in diverse sociocultural contexts in China. These approaches could provide deeper insights into the mechanisms underlying birth trauma and inform the development of more culturally responsive interventions.
Conclusions
This study demonstrates that the postpartum period and its extended duration have a profound impact on maternal physical and mental health, with a high incidence of birth trauma symptoms. The expectation gap for emotional support and informational support plays a crucial role in the development of birth trauma symptoms at 42 days postpartum. Additionally, women with lower family incomes, lower educational levels, and those who formula-feed their infants are at a higher risk of experiencing more severe birth trauma symptoms. Therefore, it is essential to establish a comprehensive social support system throughout the entire life cycle, integrating family, medical institutions, and social resources to provide continuous and multi-layered care for postpartum women. In particular, health policymakers should consider incorporating emotional and informational support services into postpartum follow-up and maternal-child healthcare programs. This could involve the development of targeted screening tools to identify women at risk of birth trauma, training for healthcare providers in psychosocial support, and the implementation of community-based education and support networks. By providing psychological interventions, emotional support, and informational support, it is possible to enhance women’s sense of social support, improve their childbirth experiences, and reduce the occurrence of trauma. Moreover, this study did not account for the influence of different modes of delivery on birth trauma symptoms at 42 days postpartum. Further research should focus on the specific characteristics of the population in China to optimize intervention strategies and support evidence-based maternal health policymaking.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author, Dr. Bei Wang, on reasonable request.
Ethical Approval
The study was approved by the Ethics Committee of the Second Affiliated Hospital of Naval Medical University. All participants voluntarily agreed to participate and provided written informed consent. This study was conducted in accordance with the ethical principles of the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study has been supported by Naval Medical University’s Deep Blue Nursing Research Project – Peak Talent Program (2022KYD11) and Scientific Research Project of Shanghai Municipal Health Commission (20234Y0059).
Disclosure
Lingling Li and Lanlan Xiao are co-first authors for this study. The authors have no conflicts of interest to declare in this work.
References
1. Australasian Birth Trauma Association. Birth-related trauma explained [EB/OL]. [2025-02-01] (2025-03-01). Available from: https://birthtrauma.org.au/downloadable-guides/.
2. Zhang K, Dai L, Wu M, et al. Women’s experience of psychological birth trauma in China: a qualitative study. BMC Pregnancy Childbirth. 2020;20(1):651. doi:10.1186/s12884-020-03342-8
3. Turkmen H, Yalniz DH, Akin B. The effect of labor comfort on traumatic childbirth perception, post-traumatic stress disorder, and breastfeeding. Breastfeed Med. 2020;15(12):779–788. doi:10.1089/bfm.2020.0138
4. Horsch A, Garthus-Niegel S, Ayers S, et al. Childbirth-related posttraumatic stress disorder: definition, risk factors, pathophysiology, diagnosis, prevention, and treatment. Am J Obstet Gynecol. 2024;230(3S):S1116–S1127. doi:10.1016/j.ajog.2023.09.089
5. Erickson N, Julian M, Muzik M. Perinatal depression, PTSD, and trauma: impact on mother-infant attachment and interventions to mitigate the transmission of risk. Int Rev Psychiatry. 2019;31(3):245–263. doi:10.1080/09540261.2018.1563529
6. Bifarin O, Quinn C, Breen L, et al. Exploration of meaning, motivation, and preparedness to care amongst the one-child policy generation in China. Int J Geriatr Psychiatry. 2023;38(2):e5887. doi:10.1002/gps.5887
7. Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychol Bull. 1985;98(2):310–357. doi:10.1037/0033-2909.98.2.310
8. Pidd D, Newton M, Wilson I, et al. Optimising maternity care for a subsequent pregnancy after a psychologically traumatic birth: a scoping review. Women Birth. 2023;36(5):e471–e480. doi:10.1016/j.wombi.2023.03.006
9. Li T, Fan W, Song J. The household structure transition in China: 1982-2015. Demography. 2020;57(4):1369–1391. doi:10.1007/s13524-020-00891-7
10. Chen F, Korinek K. Family life course transitions and rural household economy during China’s market reform. Demography. 2010;47(4):963–987. doi:10.1007/BF03213735
11. Lu J, Jiang M, Li L, et al. Relaxation in the Chinese Hukou system: effects on psychosocial wellbeing of children affected by migration. Int J Environ Res Public Health. 2019;16(19):3744. doi:10.3390/ijerph16193744
12. Yang F, Jiang Y. Heterogeneous influences of social support on physical and mental health: evidence from China. Int J Environ Res Public Health. 2020;17(18):6838. doi:10.3390/ijerph17186838
13. State Council Women and Children Working Committee. China women’s development outline (2021-2030) [EB/OL]. [2021-09-27] (2025-03-01). Available from: https://www.nwccw.gov.cn/2021/09/27/99337075.html.
14. Shen ZC, Zhou Y, Zhu DM, et al. The Chinese version of the city birth trauma scale: translation and validity testing. Chin Nurs J. 2020;55(11):1757–1761.
15. Lu T, Gao YL, Zhang JJ, et al. Study on the reliability and validity of the Chinese version of the postpartum social support scale. Chin Pract Nurs. 2014;30(15):26–28.
16. Creedy DK, Shochet IM, Horsfall J. Childbirth and the development of acute trauma symptoms: incidence and contributing factors. Birth. 2000;27(2):104–111. doi:10.1046/j.1523-536x.2000.00104.x
17. O’Donovan A, Alcorn KL, Patrick JC, et al. Predicting posttraumatic stress disorder after childbirth. Midwifery. 2014;30(8):935–941. doi:10.1016/j.midw.2014.03.011
18. Aguiar M, Farley A, Hope L, et al. Birth-related perineal trauma in low- and middle-income countries: a systematic review and meta-analysis. Matern Child Health J. 2019;23(8):1048–1070. doi:10.1007/s10995-019-02732-5
19. Verreault N, Da Costa D, Marchand A, et al. PTSD following childbirth: a prospective study of incidence and risk factors in Canadian women. J Psychosom Res. 2012;73(4):257–263. doi:10.1016/j.jpsychores.2012.07.010
20. Ju D, Zhang K, Yuan M, et al. Mediating role of childbirth readiness in the relationship between social support and psychological birth trauma in primiparous women: a nationwide cross-sectional study in China. BMJ Open. 2024;14(9):e080481. doi:10.1136/bmjopen-2023-080481
21. Fang L, Peng ZB. The influence of prenatal delivery fear and social support on postpartum PTSD in late pregnancy women. Chin J Psychiatr Health. 2024;38(4):848.
22. Gauthaman N, Henry D, Ster IC, et al. Kielland’s forceps: does it increase the risk of anal sphincter injuries? An observational study. Int Urogynecol J. 2015;26(10):1525–1532. doi:10.1007/s00192-015-2717-6
23. Reshef S, Mouadeb D, Sela Y, et al. Childbirth, trauma, and family relationships. Eur J Psychotraumatol. 2023;14(1):2157481. doi:10.1080/20008066.2022.2157481
24. Garthus-Niegel S, Von Soest T, Knoph C, et al. The influence of women’s preferences and actual mode of delivery on post-traumatic stress symptoms following childbirth: a population-based, longitudinal study. BMC Pregnancy Childbirth. 2014;14:191. doi:10.1186/1471-2393-14-191
25. Buyukcan-Tetik A, Seefeld L, Bergunde L, et al. Birth expectations, birth experiences, and childbirth-related post-traumatic stress symptoms in mothers and birth companions: dyadic investigation using response surface analysis. Br J Health Psychol. 2024;29(4):925–942. doi:10.1111/bjhp.12738
26. Hui L, Zhang H, Zhang R. The influence of childbirth fear and social support on late-pregnancy women’s postpartum PTSD. Chin J Psychiatr Health. 2024;38(4):808–812.
27. Cevik A, Aksut Akcay E, Gozuyesil E, et al. Impact of trauma, support, and control perceptions during childbirth on post-traumatic stress disorder among Syrian immigrant adolescent pregnant women. Midwifery. 2023;127:103870. doi:10.1016/j.midw.2023.103870
28. Lin SS. The impact of couple’s self-disclosure intervention on postpartum PTSD in women. Nanhua Univ. 2022.
29. Çapik A, Durmaz H. Fear of childbirth, postpartum depression, and birth-related variables as predictors of posttraumatic stress disorder after childbirth. Worldviews Evid Based Nurs. 2018;15(6):455–460. doi:10.1111/wvn.12326
30. Joensuu JM, Saarijärvi H, Rouhe H, et al. Maternal childbirth experience and induction of labor in each mode of delivery: a retrospective seven-year cohort study of 95,051 parturients in Finland. BMC Pregnancy Childbirth. 2022;22(1):508. doi:10.1186/s12884-022-04830-9
31. Chee CYI, JQX N, Liu VC, et al. Strength amidst struggles: a descriptive qualitative study of maternal experiences of low socioeconomic status mothers in the third month postpartum. J Adv Nurs. 2025;81(4):2026–2038. doi:10.1111/jan.16426
32. Dagne AH, Zewude SB, Semahegn AM. Appropriate complementary feeding practice and its associated factors among mothers who have children aged between 6 and 24 months in Ethiopia: systematic review and meta-analysis. J Nutr Metab. 2022;2022:1548390. doi:10.1155/2022/1548390
33. Kossakowska K, Bielawska-Batorowicz E. Postpartum depressive symptoms and their selected psychological predictors in breast-, mixed-, and formula-feeding mothers. Front Psychiatry. 2022;13:813469. doi:10.3389/fpsyt.2022.813469
34. Horwood C, Luthuli S, Pereira-Kotze C, et al. An exploration of pregnant women and mothers’ attitudes, perceptions and experiences of formula feeding and formula marketing, and the factors that influence decision-making about infant feeding in South Africa. BMC Public Health. 2022;22(1):393. doi:10.1186/s12889-022-12784-y
35. Politi MC, Yen RW, Elwyn G, et al. Women who are young, non-white, and with lower socioeconomic status report higher financial toxicity up to 1 year after breast cancer surgery: a mixed-effects regression analysis. Oncologist. 2021;26(1):e142–e152. doi:10.1002/onco.13544
36. Ponnet K. Financial stress, parent functioning, and adolescent problem behavior: an actor-partner interdependence approach to family stress processes in low-, middle-, and high-income families. J Youth Adolesc. 2014;43(10):1752–1769. doi:10.1007/s10964-014-0159-y
37. Margolis RHF, Bellin MH, Bookman JRM, et al. Fostering effective asthma self-management transfer in high-risk children: gaps and opportunities for family engagement. J Pediatr Health Care. 2019;33(6):684–693. doi:10.1016/j.pedhc.2019.05.004
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.