Back to Journals » International Journal of Women's Health » Volume 18
Study on the Association Between the Systemic Immune-Inflammation Index and Polycystic Ovary Syndrome in Women Undergoing in vitro Fertilization for Subfertility
Authors Li H, Tang H, Wang M, Guan H, Tang L, Chen X
Received 18 May 2026
Accepted for publication 8 July 2026
Published 14 July 2026 Volume 2026:18 625630
DOI https://doi.org/10.2147/IJWH.S625630
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Hui Li,1,* Huaiyun Tang,1,* Mei Wang,1,2 Huijuan Guan,1 Lisha Tang,1 Xu Chen2
1Reproductive Medical Center, Lianyungang Maternal and Child Health Hospital, Lianyungang, Jiangsu, People’s Republic of China; 2Science and Education Department, Lianyungang Maternal and Child Health Hospital, Lianyungang, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lisha Tang, Email [email protected] Xu Chen, Email [email protected]
Purpose: Polycystic ovary syndrome (PCOS) is closely associated with chronic low-grade inflammation. Systemic immune-inflammation index (SII) based on complete blood cell count has shown superior discriminative value in a variety of diseases, but its role in PCOS is still unclear. This study aimed to investigate the association between SII and PCOS in women undergoing their first in vitro fertilization (IVF) treatment with a gonadotropin-releasing hormone (GnRH) antagonist protocol.
Materials and Methods: A total of 334 women undergoing their first IVF treatment with a GnRH antagonist protocol from January 2019 to December 2025 were included in this study. They were divided into the PCOS group (n=160) and the non-PCOS group (n=174). Demographic and physical indicators, reproductive endocrine indicators, systemic inflammatory indicators, infertility situation, ovulation induction treatment parameters, and trigger day indicators were collected. Binary logistic regression was used to identify the independent associated factors of PCOS.
Results: The results of the multivariate analysis indicated that anti-Mullerian hormone (AMH) (OR=1.437, 95% CI: 1.222– 1.690, P< 0.001), basal follicle-stimulating hormone (FSH) (OR=0.718, 95% CI: 0.519– 0.993, P= 0.046), luteinising hormone (LH) (OR=1.293, 95% CI: 1.100– 1.519, P=0.002), testosterone (T) (OR=14.533, 95% CI: 2.162– 97.677, P=0.006), SII (OR=2.030, 95% CI: 1.079– 3.819, P=0.028), and LH level on the trigger day (OR=1.284, 95% CI: 1.061– 1.554, P=0.010) were independently associated with PCOS.
Conclusion: Among patients undergoing their first IVF treatment, SII was independently associated with PCOS. This further supported the crucial role of chronic low-grade inflammation in the pathophysiology of PCOS. In the future, its efficacy needs to be verified through large-scale studies. Before it is fully confirmed, it is not recommended to use it as an independent clinical tool.
Keywords: polycystic ovary syndrome, systemic immune-inflammation index, associated factor, reproductive endocrine, antagonist protocol
Introduction
Polycystic ovary syndrome (PCOS) is the most common endocrine and metabolic disorder in women of reproductive age, which is characterized by abnormal menstruation, ovarian polycystic changes, and hyperandrogenism.1 It is often accompanied by insulin resistance, obesity, and increased cardiometabolic risk,2 which seriously impair the patient’s reproductive health and long-term quality of life.3–5 Due to its complex etiology and high heterogeneity of clinical manifestations, the core pathological mechanism is still unclear, and individualized clinical management faces continuous challenges.2,6 In recent years, chronic low-grade inflammation has been established as the core pathological basis connecting multiple metabolic and reproductive abnormalities in PCOS.7,8 Therefore, finding biomarkers that can conveniently and objectively evaluate this inflammatory state has become a research hotspot.
Notably, research has shifted from single inflammatory factors, such as C-reactive protein (CRP), to composite indices based on complete blood counts.9 Among them, neutrophil-lymphocyte ratio (NLR) and platelet-lymphocyte ratio (PLR) have attracted attention due to their practicability, but their results in PCOS are inconsistent and susceptible to confounding factors.10 Systemic immune-inflammation index (SII), which is obtained by integrating platelet, neutrophil and lymphocyte counts, is considered to be a more systematic and stable reflection of the body’s immune balance and has shown superior diagnostic value in a variety of chronic inflammatory diseases.11,12 However, there are still significant limitations to the evidence for SII in the field of PCOS. A review indicated that most existing studies had used healthy women as the control group, and the sample size was limited, failing to control for the bias caused by inflammation due to infertility.13 This significantly limited the ability to interpret the increase in SII levels as a characteristic pathological change of PCOS. The core potential special value of SII in PCOS lied in its integration of platelet count.14 Platelets were not only passive markers of inflammation, but also key effector cells that were activated and actively amplified inflammation under the condition of PCOS.15 Patients with PCOS often had elevated platelet counts, which were closely related to insulin resistance and endothelial damage.16 Activation of platelets could release pro-inflammatory mediators such as interleukin-1β (IL-1β), and it worked in synergy with neutrophils to directly act on the ovarian microenvironment, exacerbating the inflammatory infiltration during the follicular development process.15 In contrast, C-reactive protein only reflected the liver’s response to systemic inflammation.17 Neither NLR nor PLR includes platelets. This further highlighted the unique advantages of SII. Therefore, SII could simultaneously reflect the activation of neutrophils and the platelet-related inflammatory-thrombotic pre-state, thereby providing a more comprehensive reflection of the abnormal “metabolic-inflammatory-coagulation” axis in PCOS. It became an advantageous biomarker for evaluating the local inflammatory load and functional disorders of the ovary. In addition, the heterogeneity of ovarian stimulation protocols, a key confounding factor, has not been adequately accounted for when comparing PCOS women with assisted reproductive technology (ART) and controls.18 The traditional gonadotropin-releasing hormone (GnRH) agonist protocol will create a “superphysiological” state, significantly alter the endocrine and immune microenvironment, and increase the risk of ovarian hyperstimulation syndrome (OHSS), which may confound the observation of the inherent inflammatory features of PCOS.19,20 In contrast, the GnRH antagonist protocol is closer to the physiological state, preserves the natural physiological hormone feedback pathway to the greatest extent, and significantly reduces the risk of OHSS.21 It has now become the first choice for ART treatment in patients with PCOS.22–24 Therefore, the selection of homogeneous patients receiving GnRH antagonist protocol can effectively exclude the heterogeneous effects caused by different stimulation regimens, and provide an ideal window for accurate assessment of the inherent inflammatory pathological features of PCOS.
To obtain more accurate results, the current study addressed the two limitations of the selection of the control population and the heterogeneity of treatment regimens. This study aimed to compare the demographic and physical indicators, reproductive endocrine indicators, systemic inflammatory indicators, infertility situation, ovulation induction treatment parameters, and trigger day indicators between patients with PCOS and those with unexplained infertility (UI) undergoing the first in vitro fertilization (IVF) treatment with a GnRH antagonist protocol, and to explore the association between SII and PCOS. This study was expected to provide new evidence for further understanding the immune-inflammatory mechanism of PCOS and optimizing its clinical evaluation strategy.
Materials and Methods
Study Design
This study retrospectively analyzed the medical records of 334 women undergoing their first IVF treatment in the Reproductive Medical Center of Lianyungang Maternal and Child Health Hospital, Jiangsu Province, China, from January 2019 to December 2025. All the clinical data of all patients were completed with entry and verification before December 31, 2025. All the included cases had been fully documented, with no cases of missing data. Figure 1 illustrated the detailed process from the initial screening to the final inclusion of 334 patients.
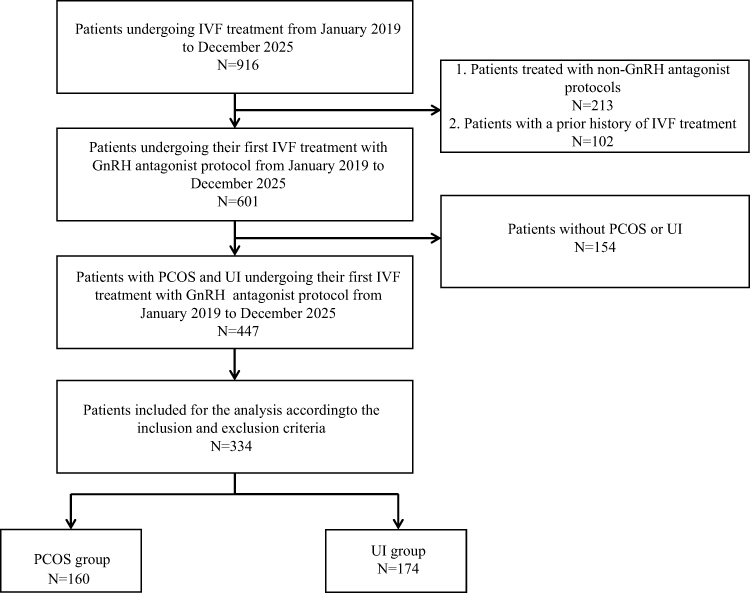 |
Figure 1 Participant flowchart. Abbreviations: IVF, in vitro fertilization; GnRH, gonadotropin-releasing hormone; PCOS, polycystic ovary syndrome; UI, unexplained infertility. |
Participants
Inclusion and Exclusion Criteria
To control confounding factors and enhance population homogeneity, the following inclusion and exclusion criteria were established in this study. Patients had to meet the following criteria: (1) patients received IVF treatment for the first time; (2) patients were treated with a GnRH antagonist protocol. Patients were excluded if they met any of the following criteria: (1) missing key data; (2) patients with other major infertility factors, including male factor infertility (according to the World Health Organization criteria) or definite tubal infertility; (3) patients with diseases affecting systemic inflammatory state (acute and chronic infections, autoimmune diseases, hematological diseases or pelvic inflammatory diseases) or medication history (use of glucocorticoids, immunosuppressants, non-steroidal anti-inflammatory drugs, oral contraceptives or drugs that may affect metabolism within the past 6 months); (4) patients with other chronic diseases that might interfere with the study, including endocrine diseases (eg, thyroid dysfunction, hyperprolactinemia), hypertension, diabetes, serious organic diseases of the heart, liver and kidney, and malignant tumors; (5) patients with a history of major surgery (including splenectomy history, any surgery in the past 6 months) or specific living habits (such as long-term smoking and drinking habits).
GnRH Antagonist Protocol
All enrolled subjects were treated with the GnRH antagonist protocol. They underwent vaginal ultrasound and sex hormone levels (follicle-stimulating hormone (FSH), luteinising hormone (LH), estradiol (E2), testosterone (T)) on day 3 of the menstrual period, and injections of 150 to 250 IU of recombinant human follicle-stimulating hormone (rFSH; follitropin alfa, GonalF, Merck Serono, Rome, Italy) were initiated. Daily injections of 0.125 to 0.25 mg GnRH-ant (Cetrorelix; Merck Group, Darmstadt, Germany) were started when the largest follicle diameter exceeded 12 to 14 mm. Follicle growth was monitored by means of vaginal ultrasound and serum hormone levels (LH, E2, progesterone (P)), and gonadotropin (Gn) doses were adjusted accordingly. Trigger drug injections were given when at least two follicles were ≥18 mm in diameter or three follicles were ≥17 mm in diameter. Oocyte retrieval was performed 36 hours later.
Grouping
The PCOS group (n=160) was diagnosed based on the Rotterdam criteria,25 which required the presence of at least two of the following three conditions, while excluding other causes of hyperandrogenism (such as congenital adrenal hyperplasia, Cushing’s syndrome, and androgen-secreting tumors): (1) oligoovulation or anovulation (menstrual cycle >35 days or less than 2 menstrual periods in the past 6 months); (2) clinical or biochemical hyperandrogenism; (3) ultrasound indicates polycystic ovarian changes (single or bilateral ovarian antral follicle count ≥20, and/or ovarian volume ≥10 mL). The non-PCOS group (ie, the group of UI, n = 174) was diagnosed according to the guidelines of the European Society of Human Reproduction and Embryology (ESHRE),26 which meant that after a comprehensive assessment of both the husband and the wife (including ovulation monitoring of the female, tubal patency examination, and semen analysis of the male), no clear cause of infertility was found.
Data Collection and Measurement
Demographic and Physical Indicators
Demographic and physical indicators included age and body mass index (BMI). Among them, the BMI calculation formula was weight (kg) divided by the square of height (m).
Reproductive Endocrine Indicators
Reproductive endocrine indicators included anti-Mullerian hormone (AMH), basal FSH, LH, and T. AMH was randomly collected during the menstrual cycle and was tested using the chemiluminescence method (CL-6000i automated chemiluminescence immunoassay analyzer, Mindray, Shenzhen, China). FSH, LH, and T were measured on the 3rd day of the menstrual cycle using an automatic chemiluminescence immunoassay analyzer (Cell-Dyn 3700, Abbott, USA).
Systemic Inflammatory Indicators
Systemic inflammatory indicators included SII, NLR, and PLR. Peripheral venous blood samples were collected before initiating ovarian stimulation. Blood routine analysis was conducted using an automatic blood analyzer (SC-120, Mindray, Shenzhen, China), resulting in the determination of platelet count (×109/L), neutrophil count (×109/L), and lymphocyte count (×109/L). SII was calculated by the formula of platelet count × neutrophil count / lymphocyte count.27 NLR was calculated by dividing the neutrophil count by the lymphocyte count. PLR was calculated based on platelet count / lymphocyte count.
Infertility Situation
Infertility situation included the type of infertility and the duration of infertility. Type of infertility was classified into primary infertility (defined as a couple having regular sexual intercourse without any form of contraception for at least 12 months, and the woman has never achieved clinical pregnancy) and secondary infertility (defined as a couple having regular sexual intercourse without any form of contraception for at least 12 months, and the woman has had at least one clinical pregnancy in the past, but is currently unable to conceive again).28
Ovulation Induction Treatment Parameters
Ovulation induction treatment parameters included the days of Gn use, the total dose of Gn, and the starting dose of Gn. Among them, the days of Gn use referred to the number of days elapsed from the start date of Gn to the trigger date. The total dose of Gn was the sum of all the doses of Gn used in this cycle. The starting dose of Gn was mainly determined based on the patient’s BMI and AMH, after careful consideration.
Trigger Day Indicators
Trigger day indicators included the number of follicles with a diameter of ≥14 mm, LH, E2, and P. Among them, the number of follicles with a diameter of ≥14 mm was obtained through transvaginal ultrasound examination. All patients underwent a baseline ultrasound examination before ovarian stimulation to rule out pelvic lesions and to measure the antral follicle count (AFC) (the total number of 2 to 5-millimeter-diameter antral follicles) on both ovaries. Ultrasound monitoring during ovulation induction was conducted by trained physicians using an 8 MHz high-resolution vaginal probe.
Data Analysis
Statistical analyses were performed using IBM SPSS version 21.0 (IBM Corporation, Armonk, State of New York, USA) software. Normality of continuous variables was tested using the Kolmogorov–Smirnov test. Normally distributed continuous variables were described with the use of means and standard deviations (SDs), and non-normally distributed continuous variables were described with the use of medians and quartiles. Categorical variables were described as frequencies and percentages. Univariate analysis was performed using t-test, non-parametric test, and chi-square test to evaluate the differences of each variable between different groups. The statistically significant variables in univariate analysis were included in the binary logistic regression model to evaluate the independent associated factors of PCOS. To improve clinical interpretability, SII was scaled by dividing by 100 in the binary logistic regression model, and the odds ratio was reported per 100-unit increase. Other continuous variables were presented per their original 1-unit increments. Variables were considered statistically significant at P values <0.05.
Ethical Approval and Informed Consent
The study was approved by the Ethics Committee of Lianyungang Maternal and Child Health Hospital (Number: 2024-xm-004). The study implementation adhered to the principles of the Declaration of Helsinki. As this study utilized anonymous medical records for retrospective analysis, patient privacy was protected, and the ethics committee waived written informed consent.
Results
Characteristics of participants
A total of 334 patients were included in this study, including 160 patients with PCOS and 174 patients without PCOS (ie, UI patients). Table 1 presented the demographic and physical indicators, reproductive endocrine indicators, systemic inflammatory indicators, infertility situation, ovulation induction treatment parameters, and trigger day indicators of all patients. The median age of the patients in this study was 31.00 (29.00, 34.00) years, and the average BMI was 23.81 ± 3.68 kg/m2. The majority of the patients suffered from primary infertility (64.67%), and the median duration of infertility was 4.00 (2.00, 5.25) years.
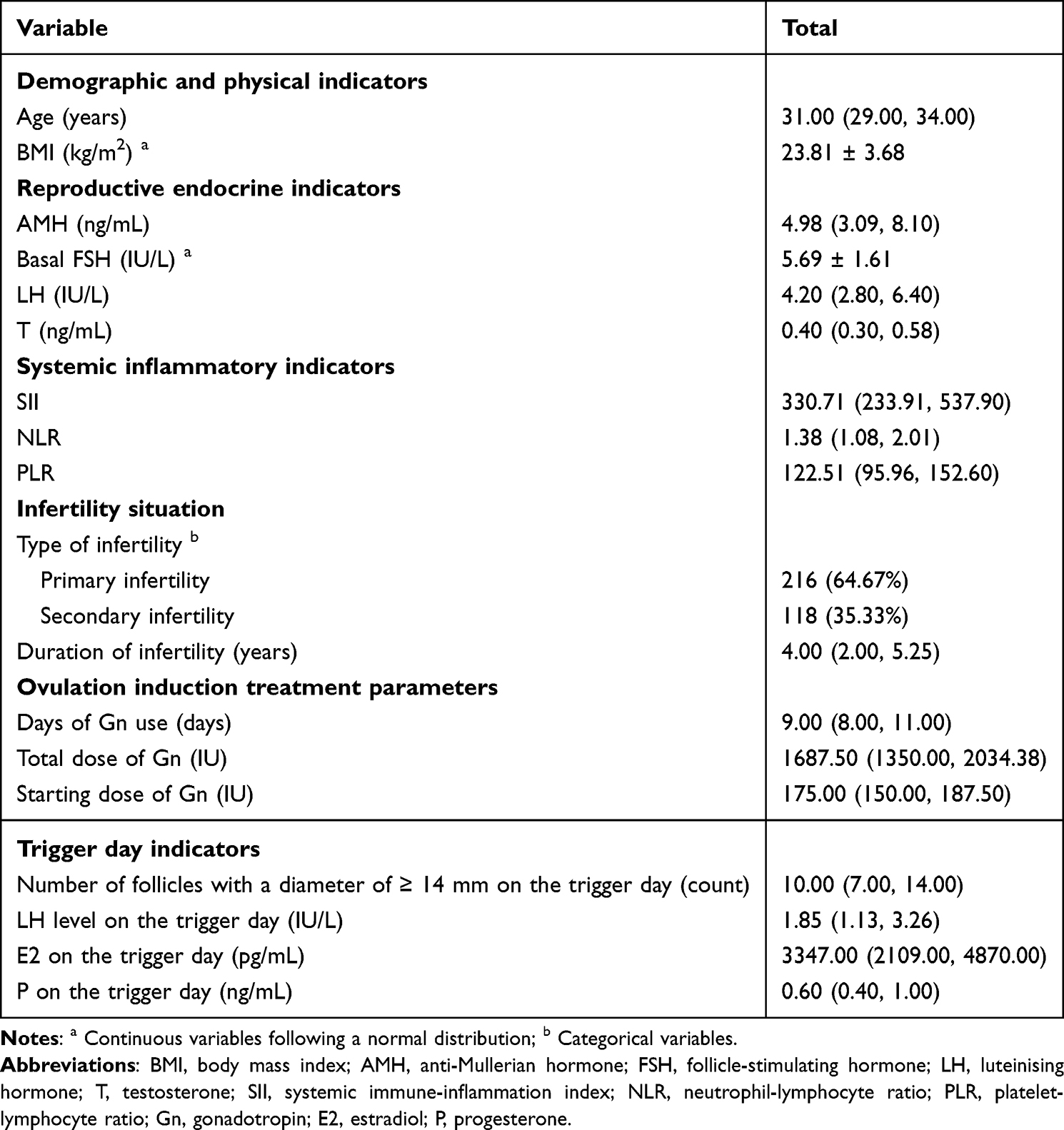 |
Table 1 Characteristics of participants (N=334) |
Univariate Analysis of the Associated Factors of PCOS
The univariate analysis showed that there were significant differences between PCOS and non-PCOS in terms of age, BMI, AMH, basal FSH, LH, T, SII, NLR, total dose of Gn, starting dose of Gn, number of follicles with a diameter of ≥14 mm on the trigger day, LH level on the trigger day, and E2 on the trigger day (P<0.05) (Table 2).
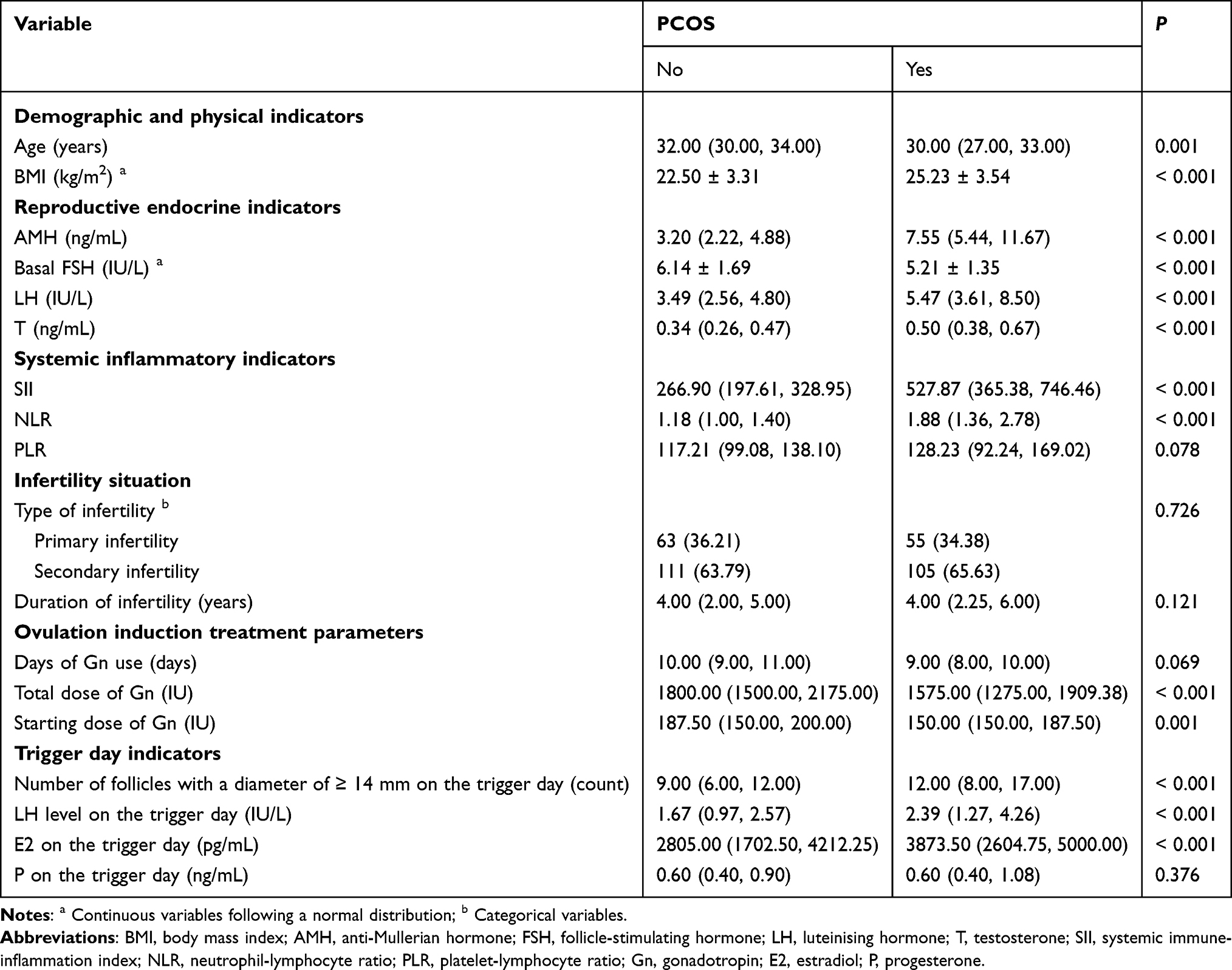 |
Table 2 Univariate Analysis of the Associated Factors of PCOS |
Multivariate Analysis of the Associated Factors of PCOS
The results of the multivariate analysis found that AMH (OR=1.437, 95% CI: 1.222–1.690, P<0.001), basal FSH (OR=0.718, 95% CI: 0.519–0.993, P=0.046), LH (OR=1.293, 95% CI: 1.100–1.519, P=0.002), T (OR=14.533, 95% CI: 2.162–97.677, P=0.006), SII (OR=2.030, 95% CI: 1.079–3.819, P=0.028), and LH level on the trigger day (OR=1.284, 95% CI: 1.061–1.554, P=0.010) were independently associated with PCOS (Table 3).
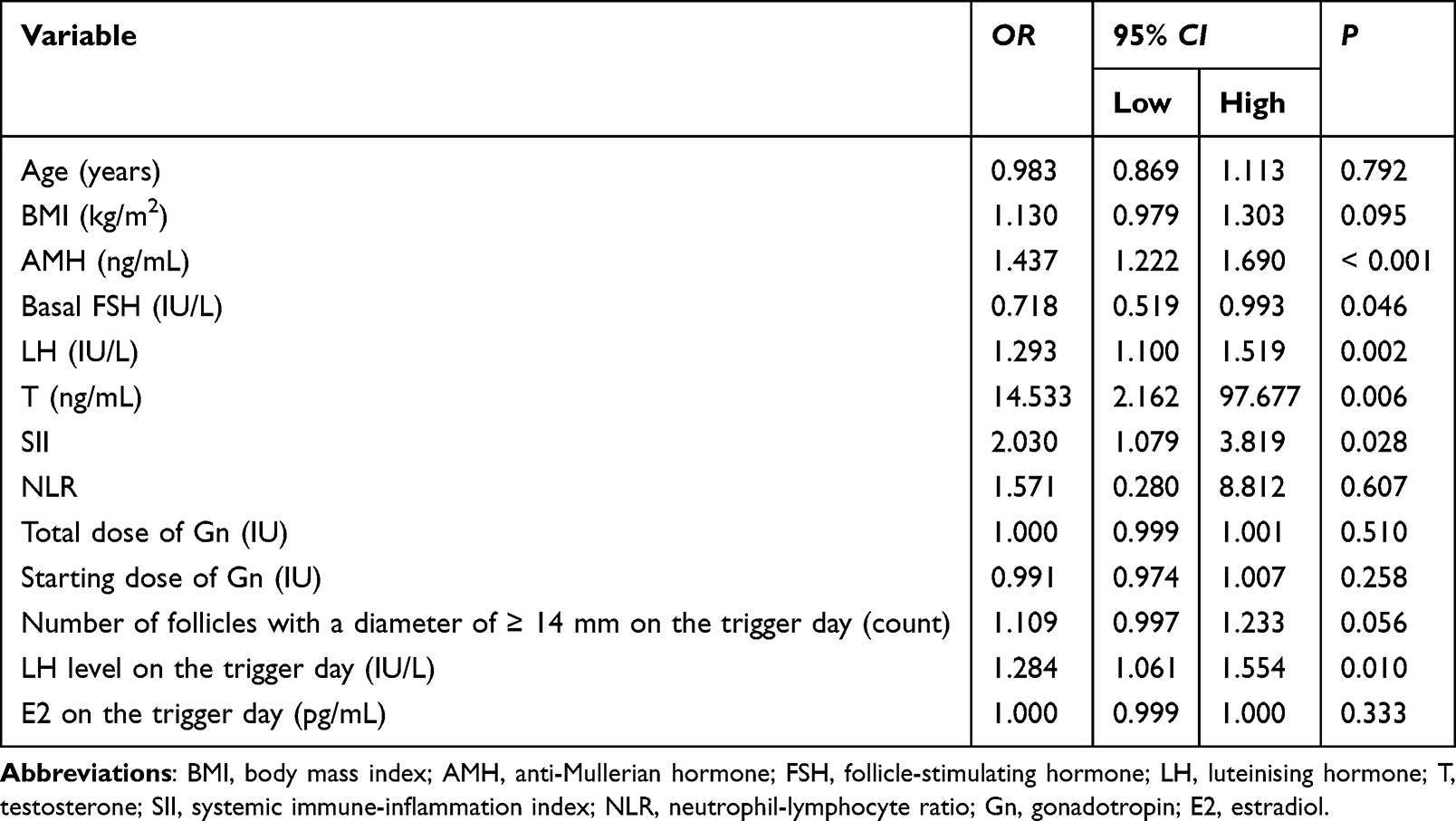 |
Table 3 Multivariate Analysis of the Associated Factors of PCOS |
ROC Curve for SII
The ROC curve analysis demonstrated that the AUC was 0.837 (95% CI: 0.792–0.882, P<0.001), indicating that SII could effectively distinguish between the PCOS and non-PCOS groups. The sensitivity and specificity were 0.756 and 0.845, respectively (Figure 2).
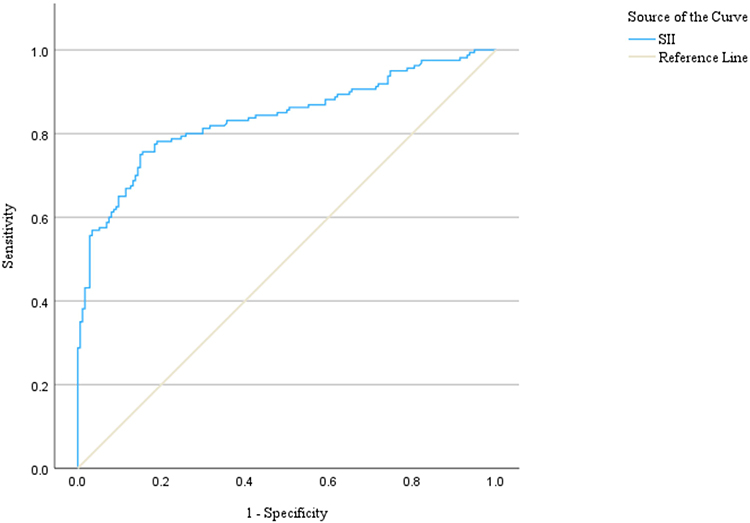 |
Figure 2 ROC curve for SII. Abbreviation: SII, systemic immune-inflammation index. |
Discussion
The complex pathophysiological mechanism of PCOS and the lack of reliable biomarkers continue to pose challenges to its clinical management.29 Chronic low-level inflammation is the core factor driving metabolic and reproductive disorders. The current study evaluated the association between SII and PCOS in a homogeneous group of women who received the first IVF treatment with a GnRH antagonist protocol. The study found that even after controlling for the effects of infertility itself and different stimulation protocols, the SII levels of patients with PCOS were still significantly higher than those in the UI group, and SII was independently associated with PCOS. This discovery provided more direct and specific evidence for the central role of inflammation in PCOS.
The univariate analysis revealed significant differences in SII between patients with PCOS and UI patients. Previous studies have also shown that SII is elevated in PCOS.30 The core contribution of this study lay in its relatively rigorous design. In this study, UI patients were selected as the control group, and the research subjects were limited to those who received the GnRH antagonist protocol that was more in line with physiological hormone feedback. These aimed to minimize the influence of the two major confounding factors, namely “infertility background” and “excessive physiological ovarian stimulation”.18,31 The heterogeneity of the previous research results might be partly attributed to these biases that have not been adequately controlled. For instance, the profound pituitary suppression and the hyperphysiological hormonal environment resulting from the traditional GnRH agonist protocol have been demonstrated to independently affect the overall immune and inflammatory status of the body.19,20 This might confuse the observation of the inherent inflammatory characteristics of PCOS. This study selected the GnRH antagonist protocol that has become the preferred treatment option for ART in patients with PCOS,22–24 ensuring that the observed inflammatory differences were more likely to be attributed to the pathological physiological changes of PCOS itself rather than the interference of the treatment intervention.
More importantly, the multivariate analysis revealed that SII was independently associated with PCOS, while NLR and PLR did not show independent association. This highlighted the potential advantages of SII. SII integrates the three key immune-inflammatory pathways of neutrophils, lymphocytes, and platelets, and is considered to be able to more systematically and stably reflect the immune balance state of the body compared to a single ratio.11,12 The superiority of SII in this study might have specific pathological and physiological bases. The platelet components in SII demonstrate the synergistic effect of endothelial dysfunction and platelet activation. In the context of chronic low-grade inflammation in patients with PCOS, this synergy occurs through two parallel pathways. On the one hand, pro-inflammatory cytokines (such as interleukin-6 (IL-6)) activate the nuclear factor κB (NF-κB) pathway in endothelial cells, upregulate the expression of adhesion molecules, thereby inducing endothelial dysfunction. The clinical manifestations include increased microvascular permeability and impaired vascular dilation function.32–34 On the other hand, activated platelets not only release pro-inflammatory mediators, further exacerbating endothelial damage, but also form platelet-leukocyte aggregates through interactions with endothelial cells and white blood cells, thereby continuously driving the local inflammatory microenvironment.35,36 In summary, this vicious cycle involving “inflammation-endothelium-platelets” constitutes an important pathological basis for the elevated cardiovascular metabolic risk in patients with PCOS.30 SII may not only reflect the imbalance between innate immunity (neutrophils) and adaptive immunity (lymphocytes),37,38 but also indirectly capture the inflammatory-vessel interaction involving platelets in PCOS. This might be a dimension that neither NLR nor PLR has fully captured. The current research findings were highly consistent with the vicious cycle model of chronic low-level inflammation interacting with insulin resistance and hyperandrogenemia in PCOS.7,8 It was worth noting that the univariate analysis showed that the BMI of the PCOS group was significantly higher than that of the UI group. However, after eliminating confounding factors through regression analysis, no independent correlation between BMI and PCOS was found. The higher BMI in the PCOS group might not be a direct inflammatory inducer, but rather an external manifestation of underlying metabolic disorders.39 Previous studies have shown that an elevated BMI can indirectly amplify the inherent chronic inflammatory state of PCOS through disorders in the secretion of fat factors.40
Furthermore, multivariate analysis also revealed that AMH, basal FSH, LH, T, and LH level on the trigger day were associated with PCOS. This strongly supported the notion that chronic low-grade inflammation was not an isolated phenomenon in PCOS, but rather deeply embedded within the core components of its hypothalamic-pituitary-ovarian axis dysfunction, arrested follicular development, and hyperandrogenemia.7,41 In terms of mechanism, when inflammatory factors bind to cell surface receptors, they can activate downstream signaling pathways such as NF-κB and mitogen-activated protein kinase (MAPK).42,43 These pathways, on the one hand, directly regulate the expression of various pro-inflammatory genes, thereby amplifying the inflammatory cascade reactions both locally and systemically. On the other hand, they can also interact with other metabolic signaling pathways through cross-talk.44 Inflammatory factors could interfere with the insulin signaling pathway, exacerbating insulin resistance and hyperinsulinemia, and subsequently stimulating the synthesis of androgens in the ovaries and adrenal glands.45,46 Conversely, androgens could also promote inflammatory responses through multiple pathways.47
From a clinical perspective, this study’s findings had significant implications. Firstly, SII was derived from basic blood routine tests, which were readily available and cost-effective. This indicator may be helpful for the auxiliary diagnosis and risk stratification of PCOS patients when they undergo assisted reproductive technology for conception. However, the predictive efficacy and the value of individualized management of this method still need to be confirmed through large-scale prospective studies and external validation. Secondly, the study observed that although the total dose of Gn and the starting dose of Gn were lower in patients with PCOS, they still achieved a greater number of follicles and higher estradiol levels on the trigger day. Specifically, inflammatory factors can activate signaling pathways such as NF-κB, down-regulate the expression of FSH receptors on granulosa cells, and inhibit the efficiency of downstream signal transduction of FSH receptors.48,49 These two aspects of effects ultimately lead to a decrease in the sensitivity of granule cells to FSH. Furthermore, the inflammatory environment may also increase the expression of LH receptors or enhance their sensitivity,50 thereby causing the granulosa cells to undergo premature pigmentation. Under the combined influence of these factors, even with a lower dose of exogenous Gn, there is a tendency for excessive follicular recruitment and high secretion of estradiol. This gives rise to a hypothesis that is worthy of further in-depth study and thought in the future: Is the inherent chronic inflammatory state of patients with PCOS caused by altering the local microenvironment of the ovaries or the sensitivity of granulosa cells to Gn, thereby leading to this “high response-low demand” ovulation-promoting pattern? This study provided a possible entry point for subsequent research. Future studies that verify this hypothesis may provide new ideas for developing more individualized and low-risk ovulation induction strategies for PCOS.
Limitations
This study had some limitations. Firstly, this study employed relatively strict exclusion criteria. This design helped to enhance the homogeneity of the research population, thereby enabling a more reliable comparison of key indicators between women with PCOS and those with UI undergoing their first IVF treatment. However, this strict screening process also introduced potential selection bias. Future studies can minimize this bias by adopting broader inclusion criteria. Secondly, as a single-center study, the generalizability of the conclusion needs to be verified in multi-center studies. Thirdly, this study only compared the baseline inflammatory status and ovulation induction treatment parameters of the two groups of patients. It did not further assess whether the inflammatory indicators (such as SII) were associated with key outcomes such as the number of retrieved eggs, embryo quality, clinical pregnancy rate, or live birth rate. Future studies can delve deeper into the correlation between SII and ART outcomes in order to determine whether SII can predict ovarian responsiveness or pregnancy success rates of patients with PCOS, thereby providing more direct evidence for clinical decision-making. Finally, although most of the known confounding factors were strictly controlled through strict exclusion criteria, it was impossible to completely rule out the potential influence of unmeasured lifestyle factors such as dietary patterns, physical activity levels, and psychological stress. Future studies can further elucidate the role of lifestyle factors in the inflammatory manifestations of PCOS by incorporating standardized lifestyle questionnaires, biomarkers, or an intervention-based research design.
Conclusion
In conclusion, through the relatively strict setting and homogenized treatment plans, this study found that SII has an independent association with PCOS in women undergoing their first IVF treatment with a GnRH antagonist protocol. This discovery reinforced the crucial role of chronic low-grade inflammation in the pathophysiology of PCOS. In the future, it is necessary to conduct a systematic evaluation of its predictive performance through large-scale prospective studies and external validation. Furthermore, a more in-depth exploration of the potential value of SII in guiding the individualized clinical management of PCOS patients and predicting the outcome of ART is warranted. However, before thorough verification is conducted, SII should not be regarded as an independent clinical decision-making tool.
Abbreviations
PCOS, polycystic ovary syndrome; SII, systemic immune-inflammation index; IVF, in vitro fertilization; GnRH, gonadotropin-releasing hormone; AMH, anti-Mullerian hormone; FSH, follicle-stimulating hormone; LH, luteinising hormone; T, testosterone; CRP, C-reactive protein; NLR, neutrophil-lymphocyte ratio; PLR, platelet-lymphocyte ratio; ART, assisted reproductive technology; OHSS, ovarian hyperstimulation syndrome; UI, unexplained infertility; E2, estradiol; P, progesterone; Gn, gonadotropin; ESHRE, the European Society of Human Reproduction and Embryology; BMI, body mass index; AFC, antral follicle count; SDs, standard deviations; OR, odds ratio; CI, confidence interval; TNF-alpha, tumor necrosis factor-alpha; IL-6, interleukin-6; IL-1β, interleukin-1β; NF-κB, nuclear factor κB; MAPK, mitogen-activated protein kinases.
Acknowledgments
We would like to express our gratitude to all those who have contributed to this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study had no funding support.
Disclosure
The authors declare no competing interests in this work.
References
1. Helvaci N, Yildiz BO. Polycystic ovary syndrome as a metabolic disease. Nat Rev Endocrinol. 2025;21(4):230–12. doi:10.1038/s41574-024-01057-w
2. Joham AE, Rees DA, Shinkai K, Forslund M, Tay CT, Teede HJ. Polycystic ovary syndrome: origins and implications: epidemiological aspects of polycystic ovary syndrome. Reproduction. 2025;170(2). doi:10.1530/REP-25-0121
3. Stener-Victorin E, Teede H, Norman RJ, et al. Polycystic ovary syndrome. Nat Rev Dis Primers. 2024;10(1):27. doi:10.1038/s41572-024-00511-3
4. Khan MJ, Ullah A, Basit S. Genetic basis of Polycystic Ovary Syndrome (PCOS): current Perspectives. Appl Clin Genet. 2019;12:249–260. doi:10.2147/TACG.S200341
5. Carter FE, Jarrett BY, Oldfield AL, Vanden Brink H, Kim JY, Lujan ME. Impact of hypocaloric dietary intervention on phenotypic presentations of Polycystic Ovary Syndrome (PCOS). Nutrients. 2025;17(13):2223. doi:10.3390/nu17132223
6. Louwers YV, Laven JSE. Characteristics of polycystic ovary syndrome throughout life. Ther Adv Reprod Health. 2020;14:2633494120911038. doi:10.1177/2633494120911038
7. Luan YY, Zhang L, Peng YQ, Li YY, Liu RX, Yin CH. Immune regulation in polycystic ovary syndrome. Clin Chim Acta. 2022;531:265–272. doi:10.1016/j.cca.2022.04.234
8. Wegrzynowicz AK, Dudley CM, Cooney LG, Stanic AK. Polycystic ovary syndrome: origins and implications: maternal complications of pregnancy in polycystic ovary syndrome. Reproduction. 2025;170(6). doi:10.1530/REP-25-0108
9. Huffman AM, Rezq S, Basnet J, Romero DG. Biomarkers in polycystic ovary syndrome. Curr Opin Physiol. 2023;36:421–431.
10. Sun H, Li D, Jiao J, Liu Q, Bian J, Wang X. A potential link between polycystic ovary syndrome and asthma: a meta-analysis. Reprod Sci. 2022;29(1):312–319. doi:10.1007/s43032-021-00662-8
11. Guo P, Kang R, Zhao X. Associations between systemic immune-inflammation index and iron deficiency. Sci Rep. 2025;15(1):36182. doi:10.1038/s41598-025-19975-8
12. Ma R, Cui L, Cai J, et al. Association between systemic immune inflammation index, systemic inflammation response index and adult psoriasis: evidence from NHANES. Front Immunol. 2024;15:1323174. doi:10.3389/fimmu.2024.1323174
13. Dai M, Hong L, Yin T, Liu S. Disturbed follicular microenvironment in polycystic ovary syndrome: relationship to oocyte quality and infertility. Endocrinology. 2024;165. doi:10.1210/endocr/bqae023
14. Zhou X, Tian Y, Zhang X. Correlation and predictive value of systemic immune-inflammation index for dyslipidemia in patients with polycystic ovary syndrome. BMC Womens Health. 2024;24(1):564. doi:10.1186/s12905-024-03405-4
15. Cognasse F, Duchez AC, Audoux E, et al. Platelets as key factors in inflammation: focus on CD40L/CD40. Front Immunol. 2022;13:825892. doi:10.3389/fimmu.2022.825892
16. Alwan SH, Al-Saeed MH. Silver nanoparticles biofabricated from Cinnamomum zeylanicum Reduce IL-6, IL-18, and TNF-ɑ in female rats with polycystic ovarian syndrome. Int J Fertil Steril. 2023;17(1):80–84. doi:10.22074/ijfs.2022.539396.1189
17. Gao N, Yuan P, Tang ZM, et al. Monomeric C-reactive protein is associated with severity and prognosis of decompensated hepatitis B cirrhosis. Front Immunol. 2024;15:1407768. doi:10.3389/fimmu.2024.1407768
18. Qi S, Yu H, Yang X, Shi Q, Yang L, Wang K. Progestin-primed ovarian stimulation protocol in patients undergoing assisted reproductive technology. Front Reprod Health. 2025;7:1719930. doi:10.3389/frph.2025.1719930
19. Siristatidis CS, Yong LN, Maheshwari A, Ray Chaudhuri Bhatta S. Gonadotropin-releasing hormone agonist protocols for pituitary suppression in assisted reproduction. Cochrane Database Syst Rev. 2025;1:Cd006919. doi:10.1002/14651858.CD006919.pub5
20. Huang H, Gao H, Shi Y, et al. Can AMH levels predict the need to step up FSH dose for controlled ovarian stimulation following a long GnRH agonist protocol in PCOS women? Reprod Biol Endocrinol. 2023;21(1):121. doi:10.1186/s12958-023-01173-8
21. Hoseini FS, Noori Mugahi SM, Akbari-Asbagh F, et al. A randomized controlled trial of gonadotropin-releasing hormone agonist versus gonadotropin-releasing hormone antagonist in Iranian infertile couples: oocyte gene expression. Daru. 2014;22:67. doi:10.1186/s40199-014-0067-4
22. Liu C, Tian T, Lou Y, et al. Live birth rate of gonadotropin-releasing hormone antagonist versus luteal phase gonadotropin-releasing hormone agonist protocol in IVF/ICSI: a systematic review and meta-analysis. Expert Rev Mol Med. 2023;1–30.
23. Al-Inany HG, Youssef MA, Ayeleke RO, Brown J, Lam WS, Broekmans FJ. Gonadotrophin-releasing hormone antagonists for assisted reproductive technology. Cochrane Database Syst Rev. 2016;4(4):Cd001750. doi:10.1002/14651858.CD001750.pub4
24. Griesinger G, Diedrich K, Tarlatzis BC, Kolibianakis EM. GnRH-antagonists in ovarian stimulation for IVF in patients with poor response to gonadotrophins, polycystic ovary syndrome, and risk of ovarian hyperstimulation: a meta-analysis. Reprod Biomed Online. 2006;13(5):628–638. doi:10.1016/S1472-6483(10)60652-9
25. Rotterdam ESHRE/ASRM-Sponsored PCOS consensus workshop group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum Reprod. 2004;19(1):41–47. doi:10.1093/humrep/deh098
26. Romualdi D, Ata B, Bhattacharya S, et al. Evidence-based guideline: unexplained infertility†. Hum Reprod. 2023;38(10):1881–1890. doi:10.1093/humrep/dead150
27. Yorulmaz A, Hayran Y, Akpinar U, Yalcin B. Systemic Immune-Inflammation Index (SII) predicts increased severity in psoriasis and psoriatic arthritis. Curr Health Sci J. 2020;46(4):352–357. doi:10.12865/CHSJ.46.04.05
28. Zegers-Hochschild F, Adamson GD, Dyer S, et al. The International Glossary on Infertility and Fertility Care, 2017. Fertil Steril. 2017;108(3):393–406. doi:10.1016/j.fertnstert.2017.06.005
29. Luo M, Yang X, Li L, et al. Integrated transcriptomic and co-expression network analysis identifies immune-metabolic biomarkers of polycystic ovary syndrome in granulosa cells. J Ovarian Res. 2025;18(1):248. doi:10.1186/s13048-025-01835-8
30. Zhang X, Lin L, Ge H. Mediating role of the systemic immune-inflammation index in obesity-induced glycolipid dysmetabolism and compromised IVF/ICSI outcomes in polycystic ovary syndrome: a retrospective cohort study. Medicine. 2026;105(12):e48005. doi:10.1097/MD.0000000000048005
31. Robertson SA, Sharkey DJ. Seminal fluid cytokines in reproductive health and fertility of men. Fertil Steril. 2026;125:757–769. doi:10.1016/j.fertnstert.2026.03.017
32. Kiatsoonthon K, Phimthong N, Potikanond S, Wikan N, Nimlamool W. Panduratin A inhibits TNF alpha-stimulated endothelial cell activation through suppressing the NF-κB pathway. Biomolecules. 2024;15(1):34. doi:10.3390/biom15010034
33. Kang S, Kishimoto T. Interplay between interleukin-6 signaling and the vascular endothelium in cytokine storms. Exp Mol Med. 2021;53(7):1116–1123. doi:10.1038/s12276-021-00649-0
34. Mroueh A, Fakih W, Carmona A, et al. COVID-19 promotes endothelial dysfunction and thrombogenicity: role of proinflammatory cytokines/SGLT2 prooxidant pathway. J Thromb Haemost. 2024;22(1):286–299. doi:10.1016/j.jtha.2023.09.022
35. Chen R, Huang E, Wu X, et al. Prorenin in hepatic stellate cell extracellular vesicles induces platelet-dependent thrombin formation and release of profibrotic TGF-β. FASEB j. 2025;39(20):e71125. doi:10.1096/fj.202501902R
36. Moghaddasnejad MR, Saki N. “Targeting platelets in breast cancer: insights into pathophysiology and therapeutic strategies”. Crit Rev Oncol Hematol. 2026;223:105266. doi:10.1016/j.critrevonc.2026.105266
37. Huang H, Wang W, Ma Q, Cao K. Systemic inflammation-based hematological indices and 90-day functional outcomes after intravenous thrombolysis in acute ischemic stroke: a systematic review. Front Neurol. 2025;16:1699939. doi:10.3389/fneur.2025.1699939
38. Gao L, Liu C, Ye G, Gao Y, Wang H. Advancing gouty arthritis research: the clinical value of complete blood cell count ratios and immune-inflammatory interactions. J Inflamm Res. 2025;18:16597–16610. doi:10.2147/JIR.S556837
39. Shaaban Z, Khoradmehr A, Amiri-Yekta A, Jafarzadeh Shirazi MR, Tamadon A. Pathophysiologic mechanisms of obesity- and chronic inflammation-related genes in etiology of polycystic ovary syndrome. Iran J Basic Med Sci. 2019;22(12):1378–1386. doi:10.22038/IJBMS.2019.14029
40. Dilbaz B. Are women with polycystic ovary syndrome more vulnerable to COVID-19 infection? Turk J Obstet Gynecol. 2021;18(3):221–223. doi:10.4274/tjod.galenos.2021.05014
41. Kından A, Kından G, Soysal Ç, Turan V. PCOS phenotypes and hematological immune-inflammatory indices: a comparative evaluation. J Reprod Immunol. 2025;173:104823. doi:10.1016/j.jri.2025.104823
42. Silva AD, Hwang J, Marciel MP, Bellis SL. The pro-inflammatory cytokines IL-1β and IL-6 promote upregulation of the ST6GAL1 sialyltransferase in pancreatic cancer cells. J Biol Chem. 2024;300:107752. doi:10.1016/j.jbc.2024.107752
43. Saeedi TA, Hakem FT, Helal MA, et al. Molecular docking and experimental validation for the protective effect of betanin against capecitabine-induced myocardial injury: binding to TLR4 and downregulation of MyD88/NFκB signaling. Tissue Cell. 2026;101:103475. doi:10.1016/j.tice.2026.103475
44. Li J, Lei X, Yang X. The cross-talk of non-coding RNAs and inflammation in human cancer. Curr Pharm Biotechnol. 2024.
45. Ozkan HD, Ayas Ozkan M, Dayanan R, Duygulu Bulan D, Filiz AA, Engin-Ustun Y. Inflammatory status and clinical phenotypes of PCOS: the role of NLR, SII, SIRI, and AISI. BMC Womens Health. 2025;25(1):463. doi:10.1186/s12905-025-04033-2
46. Cakir I, Çakir N. Immune-inflammation markers are related to hormone levels in polycystic ovary syndrome: a case-control study: immune-inflammatory markers in PCOS. BMC Endocr Disord. 2025;25(1):274. doi:10.1186/s12902-025-02094-w
47. Zorlu U, Turgay B, Yılmazer-Zorlu SN, Halilzade M, Halilzade İ, Yalçın HR. Investigation of the relationship between clinical features and the sonographic appearance of the ovaries with the delta neutrophil index in polycystic ovary syndrome. JBRA Assist Reprod. 2025;1–5. doi:10.5935/1518-0557.20250014
48. Tabandeh MR, Jozaie S, Ghotbedin Z, Gorani S. Dimethyl itaconic acid improves viability and steroidogenesis and suppresses cytokine production in LPS-treated bovine ovarian granulosa cells by regulating TLR4/nfkβ, NLRP3, JNK signaling pathways. Res Vet Sci. 2022;152:89–98. doi:10.1016/j.rvsc.2022.07.024
49. Jin S, Wang YS, Huang JC, et al. Osthole exhibits the remedial potential for polycystic ovary syndrome mice through Nrf2-Foxo1-GSH-NF-κB pathway. Cell Biol Int. 2024;48:1111–1123. doi:10.1002/cbin.12170
50. Li P, Zhang Z, Liu J, Xue H. LIPUS can promote osteogenesis of hPDLCs and inhibit the periodontal inflammatory response via TLR5. Oral Dis. 2024;30(5):3386–3399. doi:10.1111/odi.14807
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.