Back to Journals » Psychology Research and Behavior Management » Volume 19
Stress Coping and Psychological Resilience Development in Newly Licensed Registered Nurses During the Transition to Independent ICU Practice: A Descriptive Qualitative Study
Authors Wu L, Hong X ![]() , Liang Y, Yan X, Gong H
, Liang Y, Yan X, Gong H
Received 9 October 2025
Accepted for publication 31 December 2025
Published 9 January 2026 Volume 2026:19 569101
DOI https://doi.org/10.2147/PRBM.S569101
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gabriela Topa
Luqing Wu, Xuepei Hong, Yufeng Liang, Xiaoling Yan, Huafeng Gong
Department of Critical Care Medicine, The First Affiliated Hospital of Xiamen University, School of Medicine, Xiamen University, Xiamen, People’s Republic of China
Correspondence: Xuepei Hong, Department of Critical Care Medicine, The First Affiliated Hospital of Xiamen University, School of Medicine, Xiamen University, Xiamen, People’s Republic of China, Email [email protected]
Background: The transition from the intensive care unit (ICU) to independent practice is highly stressful for newly licensed registered nurses (NLRNs), who need to navigate complex clinical demands while growing professionally under high-risk conditions. Although psychological resilience is acknowledged as a critical factor for successful adaptation, the specific processes through which NLRNs cope with transitional stressors and develop such resilience are still inadequately understood.
Objective: This study aimed to explore the stress coping mechanisms and psychological resilience experiences of NLRNs during their transition to independent practice in ICU.
Methods: Descriptive qualitative study was conducted using purposive sampling. Between April and September 2024, 22 NLRNs were selected from the First Affiliated Hospital of Xiamen University in Xiamen. NVivo 12 was employed to systematically organize and code the interview data. The data were analyzed and thematically condensed through the application of content analysis methods.
Results: Five themes and fifteen sub-themes emerged from the analysis: 1) deconstruction and reconstruction of identity, 2) the gap between know and do, 3) ethical dilemmas and emotional labor, 4) organizational socialization, and 5) turning point and “metamorphosis”.
Conclusion: The process of stress coping and resilience development among NLRNs transitioning to the ICU could be characterized as a “challenge-adaptation-growth” framework. By actively engaging with various stressors, NLRNs were able to cultivate resilience, which was marked by emotional adaptability, cognitive flexibility, and social connectedness. This development not only aided in their personal growth but also enhanced their professional value.
Keywords: nurse, stress, psychological resilience, ICU, qualitative
A Letter to the Editor has been published for this article.
Key Points
- This study proposed a novel “challenge-adaptation-growth” framework that reconceptualized the ICU transition as a dynamic process of professional transformation.
- This study identified emotional adaptability, cognitive flexibility, and social connectedness as core, developable dimensions of resilience, tracing their origins to nurses’ active coping with specific clinical and social stressors.
Introduction
The transition from nursing education to independent clinical practice represented a highly challenging period for NLRNs.1 This phase, commonly referred to as “transition shock”, was characterized by the daunting task of applying theoretical knowledge to complex and unpredictable patient care scenarios.2 These challenges were particularly pronounced in ICU, where the work environment was marked by high acuity, technical complexity, rapid decision-making, and emotional intensity.3 In the ICU, NLRNs found themselves suddenly immersed in an environment where they must manage critically ill patients, operate sophisticated life-support equipment, and provide comfort to anxious family members, all while navigating their emerging professional identities.4
The inherent challenges of working in the ICU, including the severity of patient conditions, high mortality rates, ethical dilemmas, and the pressures of emergent care, resulted in ICU nurses experiencing higher stress levels compared to their counterparts in general departments.5 For NLRNs, the pressure to achieve independent practice within a short time frame in such an environment could be overwhelming.6 Due to China’s large population, there has been a shortage of nursing staff, a phenomenon that was even more pronounced in the ICU.7 Consequently, ICU managers expected NLRNs to quickly attain the qualifications necessary for independent practice. However, there existed a significant gap between the preparation of NLRNs prior to their employment and the reality of independent practice once they commence work, leading to feelings of inadequacy, anxiety, and burnout. Without adequate support, these challenges would persistently exacerbate the work pressure and psychological strain on NLRNs, jeopardizing not only their well-being but also patient safety and nurse turnover rates.8
Existing research has accumulated substantial evidence through quantitative methods, revealing stressors, burnout rates, and organizational-level influencing factors among NLRNs in the ICU.9–12 Additionally, these studies have attempted to enhance psychological resilience through structured interventions.13,14 However, they predominantly focus on statistical relationships between variables, making it challenging to capture the dynamic psychological processes and meaning-making mechanisms that NLRNs employ while coping with stress during their transition to independent practice.15 Specifically, two critical gaps persist in the literature: First, at the cognitive-behavioral level, there is a lack of systematic understanding of how NLRNs proactively identify stress, adjust their strategies, and form personalized coping patterns. Second, at the psychological construction level, there is insufficient exploration of how their psychological resilience gradually develops in practical contexts. This includes the process from initial stress adaptation to eventual professional growth, which is a key factor in nurse retention and well-being.16 Thus, firsthand experience-based exploration of how resilience develops among NLRNs during their transition period remains lacking.
Qualitative research is not only necessary but also pivotal in addressing this gap. As a methodological approach, qualitative investigation facilitates a comprehensive and in-depth understanding of social phenomena and human experiences, making it particularly suitable for exploring complex and contextually embedded processes.17 Through detailed interviews with NLRNs, this study captures first-hand accounts of their coping strategies for stress during the transition to independent practice. This provides an appropriate research pathway for delving into the intricate and highly contextualized experiences of this transitional period. In contrast to quantitative studies that struggle to capture the dynamic psychological processes of novice nurses during their transition to independent practice—such as the evolution of coping strategies, the formation of professional identity, and fluctuations in self-efficacy—qualitative investigations, through in-depth interviews, systematically reveal their meaning-making and coping logic during this critical phase.18 This approach helps identify gaps in existing research regarding the influencing factors and intrinsic mechanisms of resilience development. Furthermore, it enables the identification of key facilitators and barriers affecting resilience development while elucidating the meanings participants ascribe to their transitional experiences. Such insights are crucial for developing conceptually sound and empirically grounded interventions.
This study aimed to employed a descriptive qualitative to explore the stress coping mechanisms and psychological resilience experiences of NLRNs during their transition to independent practice in the ICU. The specific research objectives were as follows:
- To identify the core stressors encountered during the transition period and the primary emotional experiences associated with them;
- To describe the key response strategies and adjustment behaviors developed or adopted by NLRNs to facilitate their adaptation to independent practice.
Methods
Design
This study utilized a descriptive qualitative design, as conceptualized by Sandelowski,19 which was particularly effective in providing a clear and rich summary of participants’ experiences articulated in their own words. This methodology aligned with the research objective of directly describing the coping strategies and resilience development processes of NLRNs, without imposing extensive theoretical interpretations. Purposive sampling was employed to select participants. Data were collected through semi-structured, in-depth interviews guided by an open-ended interview protocol. This approach enabled participants to freely share their experiences while ensuring that all pertinent topics were addressed. This study was consistent with the unified standard of qualitative survey.20
Participants
The participants in this study were NLRNs employed as full-time staff members at the ICU of the First Affiliated Hospital of Xiamen University. This hospital, recognized as a prestigious Grade III, Class A institution in South China, had demonstrated advanced capabilities in the development of critical care medicine and the establishment of nursing teams. It had also accumulated extensive experience in training ICU specialist nurses. This study were conducted between April and September 2025. All participants were interviewed in accordance with the principles of informed consent and voluntary participation. Demographic information included age, educational attainment, etc. The sample size was determined according to the principle of data saturation, whereby interviews were terminated after at least 10 sessions, when no new information emerged during three consecutive interviews.21
Data Collection
Based on the research objectives, the research team developed a semi-structured interview guide covering three main domains: demographic information, work-related stress, and coping strategies. This guide was designed to explore participants’ experiences during their independent shifts in the ICU. To ensure content validity, the guide was reviewed by two clinical nursing experts, and two pilot interviews were conducted (Data from these pilot interviews were not included in the final analysis). The final version of the interview guide was presented in Table 1.
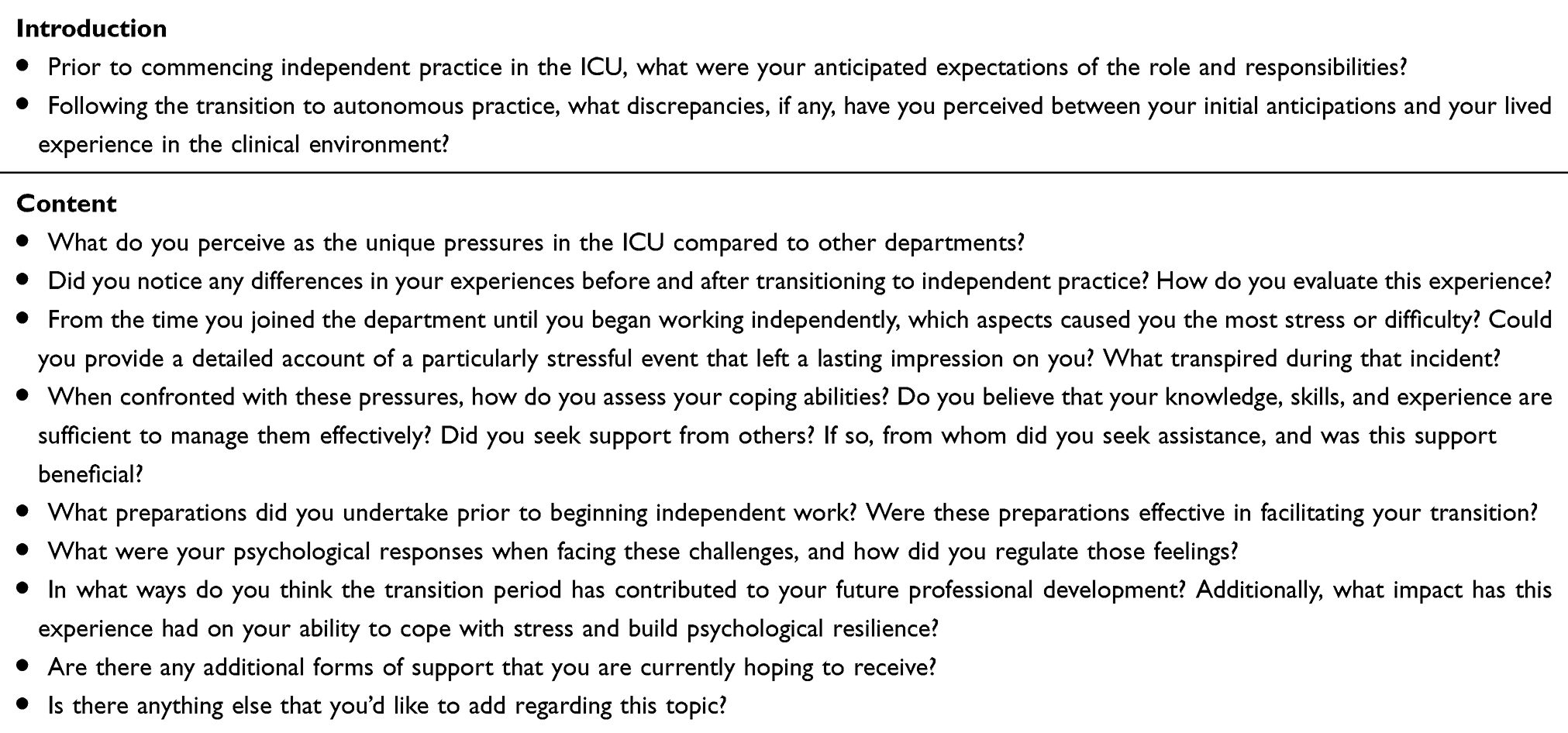 |
Table 1 Interview List |
Before the interview commenced, the researchers explained the purpose and significance of the study to the participants. Since both the researchers and the participants were ICU staff, a strong trust relationship existed between them, which laid the foundation for the smooth conduct of the interview. The researchers had participated in multiple qualitative studies and possessed the necessary professional qualifications to conduct this research.
The interview location was chosen to prioritize privacy and quietness, with timing selected by the participants. Each interview was conducted in a one-on-one, face-to-face format. Before the interviews commenced, participants were informed about the purpose, content, and specific requirements (eg interviews were audio-recorded). The researcher documented participants’ body language and emotional expressions—such as laughter, crying, or frowning—to better assess their authentic thoughts. Each interview lasted approximately 30 to 40 minutes. The process concluded after 22 interviews, as three consecutive interviews following the 19th yielded no new themes or substantive information, indicating data redundancy and thematic saturation. It was concluded that further interviews were unnecessary, given that the data provided a comprehensive and rich account of the nurses’ experiences.
Data Analysis
The qualitative data in this study were analyzed using the content analysis method described by Graneheim and Lundman.22 The analytical process was systematically conducted in three main steps, a) Identifying Meaning Units and Condensation: After a thorough review of the interview transcripts to achieve a comprehensive understanding, the text was segmented into meaning units—sentences or paragraphs that encapsulate elements pertinent to the research phenomenon. These meaning units were subsequently condensed to reduce the text length while maintaining the core content relevant to stress coping and resilience development. b) Developing Codes: The condensed meaning units were abstracted and assigned codes that succinctly encapsulated the essential concepts of each data segment. This process effectively transformed the participants’ raw experiences into a structured set of codes. c) Forming Categories and Themes: The codes were systematically compared and grouped based on their similarities and differences. Through this iterative process, related codes were synthesized into sub-categories and broader categories, which were further refined into the main themes that articulate the typical experiential features and patterns observed among the participants. NVivo 12 software was utilized for data management, aiding in the systematic organization of transcripts, the consistent application of codes across the entire dataset, and the efficient retrieval of data segments during the thematic synthesis process.
Rigour
To minimize potential biases, this study ensured that no prior relationships existed between the principal investigators and participants. The research team maintained a neutral stance throughout the data collection and analysis process. Two principal investigators independently conducted the data analysis, and in cases of disputed findings, a third senior investigator was invited for evaluation, with results determined through consensus. To ensure the reproducibility of the research outcomes, we meticulously documented all procedures, including interview guides, data transcription, and analytical steps. Through regular team discussions and reflective practices, such as documenting potential biases, we enhanced the credibility and reliability of the research findings.
Ethics
The study received approval from the Ethics Committee of the First Affiliated Hospital of Xiamen University (No. XMFHIIT-2025SL166), and the research protocol was in accordance with the Declaration of Helsinki. Prior to the study, all participants were thoroughly informed about the research objectives, content, and other pertinent information. They voluntarily consented to participate in the study. Additionally, they were provided with written assurances, including: a) the right to withdraw from the study at any time; b) personal information will be utilized solely for the purposes of this research, with any published results presented in a coded format to safeguard participants’ identities; c) potential benefits of participation, such as relevant support for the participants’ work. All participants consented to the use of their anonymized responses and direct quotes in scientific publications.
Results
A total of 22 patients (18 females and 4 males) were interviewed for this study. The age of the participants ranged from 23 to 27 years, with independent practice durations varying from 1 week to 12 weeks, as shown in Table 2. The study identified five themes and fifteen sub-themes, illustrating that NLRNs experienced a complex, multi-stage process of adaptation and growth. This process commenced with the reconstruction of personal identity, wherein they confronted core challenges, including the substantial gap between theoretical knowledge and practical application, ethical dilemmas, and emotional labor. These challenges necessitated the pursuit of resource support within intricate social organizations. By successfully navigating these obstacles, NLRNs underwent a pivotal transformation in their personal capabilities and professional values. Figure 1 illustrates the conceptual relationships among these themes.
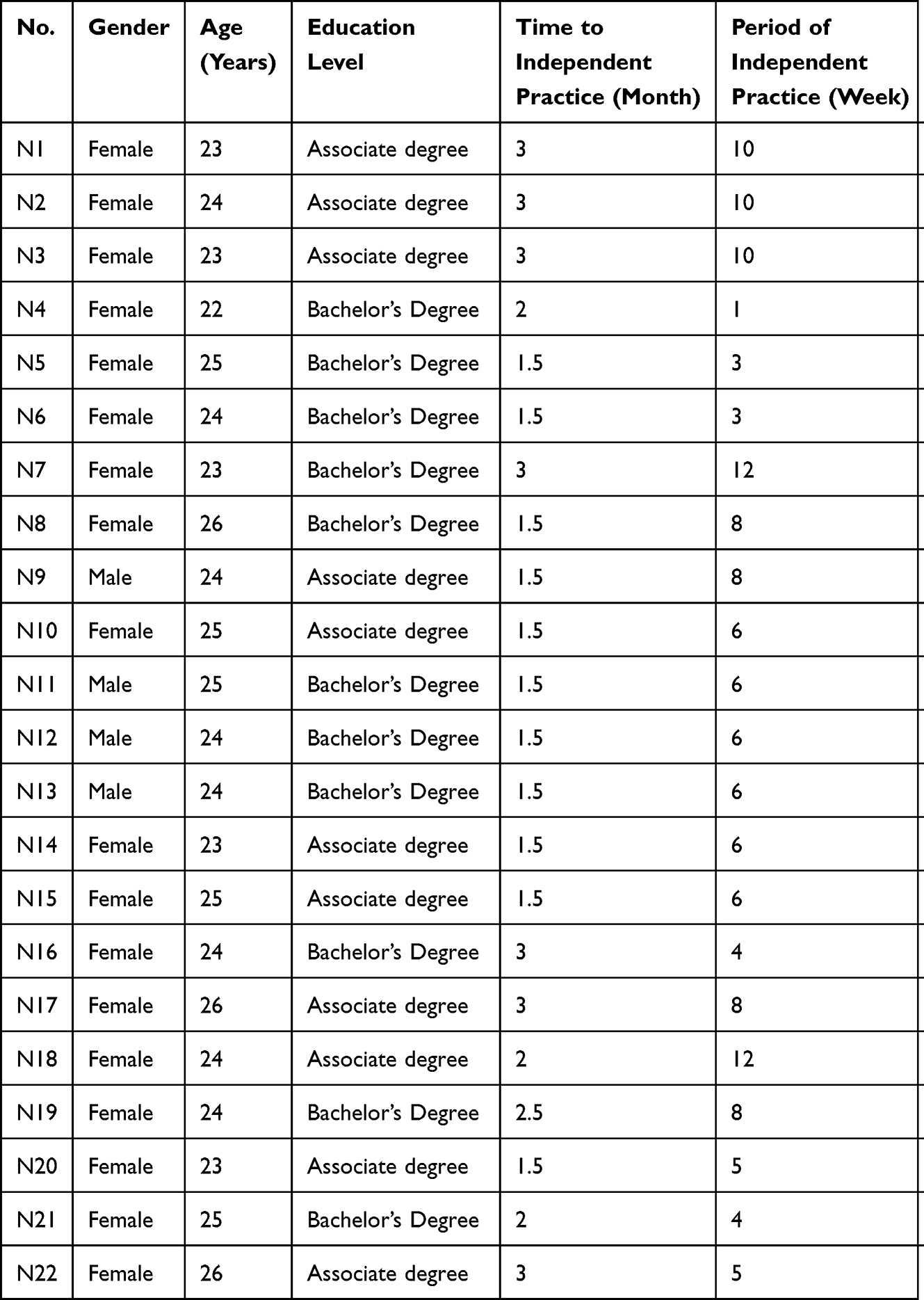 |
Table 2 Interviewer Demographic Information |
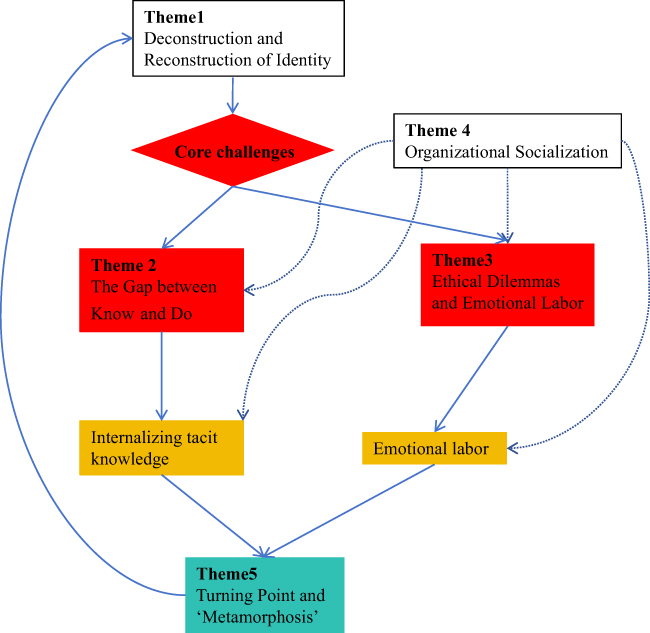 |
Figure 1 A Dynamic Model of Stress Coping and Resilience Development in ICU NLRNs. Notes: Red Boxes indicate the core stressors (challenges). Yellow Boxes correspond to the active coping strategies and mechanisms (adaptation). Green Boxes represent the positive outcomes and developmental stages (growth). Solid arrows (→) depict the primary sequential flow of the process. Dashed arrow (- - →) signifies a supporting or reinforcing relationship. |
Theme 1: Deconstruction and Reconstruction of Identity
Sub-Theme 1.1 Initial Phase of Deconstruction: Experiences of Legitimate Peripheral Participation
The pre-independent phase for NLRNs was characterized by internal feelings of illegitimacy and marginalization. This occurred despite their formal qualifications and was evident in the lack of acknowledgment from the healthcare team and from their own professional self-perception.
Although I wear a “Registered Nurse” badge, I often feel as though I am merely acting in the role of a nurse. (N3)
Despite holding a valid license, I sometimes perceive myself as an ‘illegal practitioner,’ primarily because my mentor consistently accompanies me, resembling a ‘supervisor.’ (N17)
Sub-Theme 1.2 Cognitive Grounding for Reconstruction: Understanding the Essential Transitional Period
The transition to independent practice was characterized by three distinct attitudes among NLRNs: excitement (anticipation of new responsibilities), anxiety (apprehension about clinical competence), and indifference (perception of the transition as a mandatory task).
This period is undoubtedly challenging; however, upon its completion, I will be capable of working independently, just like my experienced colleagues. (N1)
I am concerned about my performance during this extended process. (N6)
Nevertheless, as these tasks are mandatory assignments from the hospital, they must be completed—refusal is not an option. (N13)
Sub-Theme 1.3 Action in Reconstruction: The Transition From a Mimic to a Critical Thinker
Working independently necessitated that NLRNs cultivated their own mindset, values, and approach to work within ICU.
I aim to develop my own methods at work, drawing on the experiences of my predecessors. Working independently is essential; without it, I would miss the opportunity to make my own decisions when confronted with challenges, which presents both a challenge and an opportunity. (N10)
If I fail to clearly explain every detail and potential risk to the next shift during the handover, I find it difficult to sleep when I return home. This sense of ‘crisis’ has become an integral part of my existence. (N19)
Theme 2: The Gap Between Know and Do
Translating theoretical knowledge into practice required NLRNs to navigate technical deficits, informational overload, and complex decision-making.
Sub-Theme 2.1 Ineffective Coping Skills
Deficiencies persisted in NLRNs’ ability to manage complex responsibilities, including work efficiency, risk anticipation, psychological stress, and role-specific comprehension, during their transition to autonomous ICU practice.
When the patient’s condition is relatively serious, I often find it difficult to fall asleep before my night shift. (N1)
Her condition was critical, and the doctor’s orders were complex, leaving me uncertain about how to proceed at that time. (N7)
There are an excessive number of assessment forms in the nursing records. (N3)
It is essential to know how to adjust a decimal point in the parameters of a ventilator, predict potential changes in a patient’s condition in the immediate future, and communicate effectively with a physician who has a specific personality. (N13)
Sub-Theme 2.2 Information Overload & Decision Paralysis
NLRNs encountered substantial challenges in prioritizing tasks due to the vast, continuous, and multidimensional information generated within the ICU environment. This difficulty stemmed from their underdeveloped skills in information filtering and pattern recognition, which ultimately hampered their decision-making efficiency.
The most alarming situation occurs when multiple alarms activate simultaneously. For certain patients requiring external examinations while undergoing endotracheal intubation, the presence of numerous tubes can be overwhelming. (N7, N8)
When confronted with unfamiliar tubes or devices, or when faced with an excessive number of them, anxiety may arise. (N6, N8)
During quality control observations of our shift handover, the evaluators pose intricate questions regarding the patients’ conditions and circumstances. Due to my limited familiarity with these details, I often experience heightened nervousness and a significant amount of pressure. (N1)
Sub-Theme 2.3: Internalizing Tacit Knowledge: The Bridge to Practice
Confronted with the limitations of textbook knowledge, NLRNs turned to the internalization of tacit knowledge—the unspoken, context-dependent wisdom of clinical practice. This knowledge, essential for effective skill application and information prioritization, was not directly transferable. It required an iterative process of learning-by-doing and thoughtful observation of peers. Successfully internalizing this knowledge allowed NLRNs to develop an embodied understanding of their work, moving beyond mimicry to informed independent practice.
A quintessential example is engaging in conversation with family members. The theories presented in literature regarding ‘showing empathy’ and ‘effective communication’ seem particularly inadequate when confronted with a family member who is emotionally distressed and persistently questioning the deterioration of a loved one’s condition. (N17)
Her condition was severe, and the medical directives were exceedingly complex. At that moment, I felt lost and uncertain about the necessary procedures during the handover of a critically ill patient for surgery. (N21)
Theme 3 Ethical Dilemmas and Emotional Labor
Two principal, intertwined challenges characterized the independent practice of ICU NLRNs: ethical conflicts at the cognitive level, and the burden of emotional labor. These arose from the complex interplay between adapting technical knowledge and upholding professional values, moral identity, and emotional well-being.
Subthemes 3.1 Ethical Dilemmas
NLRNs in the ICU environment, characterized by limited resources, critical conditions, and uncertain information, experienced psychological indecision when faced with conflicting ethical principles, values, or responsibilities.
The patient exhibited clear signs of volume depletion, with blood pressure barely maintained despite the administration of high doses of vasopressors. I communicated this concern to the attending physician, who merely instructed me to ‘keep an eye on it.’ Consequently, I felt powerless as the patient’s blood pressure continued to decline. (N17)
In some cases, patients experience such profound agony that they seem to possess little desire to live, as even therapeutic interventions provoke feelings of aversion in them. (N19)
Subtheme 3.2 Emotional Labor and Coping Strategies
Emotion management represented a continuous and demanding aspect of ICU practice. NLRNs articulated the prolonged stress associated with the necessity of appearing calm and competent to conceal their internal panic. They also described a range of strategies they have developed to cope with this stress.
Surface acting referred to the practice of concealing one’s true feelings while exhibiting emotions that align with professional expectations.
When a family member, overwhelmed with emotion, pointed at my nose and scolded me, I felt a sense of injustice and a desire to cry. However, I had to suppress all my anger and grievances, striving to maintain a calm voice and explain the situation with a smile. (N9)
Deep acting meant not only control expressions, but also actively try to understand the other person from the bottom of one’s heart, stimulating true empathy to achieve more sincere communication.
Facing a mother who has lost her child, I would force myself to think, If this were my family. Let that genuine sadness come out, then hold her hand and sit with her for a while. (N13)
Internalization and self-regulation of emotional rules: learning and adhering to the “emotional rules” in the ICU (such as “must remain calm” and “must be strong”) and developing personal coping strategies (such as “numbing” and “dark humor”).
For instance, we often joke about ‘going fishing again’—a euphemism referring to unsuccessful rescues. While this may sound cold-blooded, it serves as a vital outlet for stress relief. (N22)
Theme 4 Organizational Socialization
The most enduring challenge for nurses was achieving full integration into the team and gaining recognition for their contributions. This process necessitates skillful management of interactions with a variety of roles and the consistent demonstration of initiative in collaborative endeavors.
Subtheme 4.1 Role-Specific Interaction
Role interactions primarily involved three key aspects: 1) engaging with senior nurses to seek protection, guidance, and recognition, 2) collaborating with physicians to learn efficient methods for reporting patient conditions and making recommendations, and 3) communicating with nursing managers to bridge the gap between management expectations and clinical realities, while also participating in “measured communication”.
When I encounter uncertainties, I often seek guidance from my team leader or the quality control supervisor on duty. (N1-N10)
I have received considerable support from nearly every teacher, who have been patient and willing to assist me. Additionally, the doctors have taken the time to explain medication-related knowledge in detail. (N4, N5)
Regarding the shift handover, the leader will evaluate our performance to ensure it is conducted properly, and they will provide us with some reassurance. (N1, N3)
Subtheme 4.2 To Break into the Inner Circle
NLRNs acquired legitimacy and recognition within their teams by understanding the implicit social structure, which encompassed specialized language, humor, and informal rules.
I need to participate in more gatherings to build better relationships with my colleagues. (N19)
It’s important to learn the different names people use for equipment, supplies, and even medications—they have their own unique naming habits. (N20)
If you can coordinate with them efficiently and pull your own weight, it’s easier to gain recognition. (N16)
Subtheme 4.3 Taking Initiative
Working independently encouraged NLRNs to demonstrate initiative, take on additional responsibilities, and utilize personal charm and various strategies. This proactive approach actively fostered more favorable team dynamics and created enhanced learning opportunities for themselves.
If I were to work independently, I would first outline my workflow to ensure efficiency and clarity. (N6)
Upon encountering a new machine, my initial step would be to consult my teacher regarding the general operational process. (N7)
Subtheme 4.4 Navigating Formal and Informal Support Systems
In addition to informal team integration, NLRNs actively sought and utilized formal support resources provided by the hospital to manage the stress associated with independent practice. These resources included mentorship programs, clinical educators, and employee assistance programs.
I will confide in my mentor when I experience excessive pressure. (N11)
The psychological care specialist team at the hospital can provide support and assistance, provided that you take the initiative to seek consultation. (N20)
Theme 5 Turning Point and “Metamorphosis”
By addressing the identity crisis, the gap between knowledge and practice, social pressures, and ethical-emotional challenges, NLRNs experienced a pivotal moment in their personal and professional development. This signified their transformation from stressed novices to resilient and confident practitioners who derived meaning from their practice.
Subtheme 5.1 Experiences Near the Tipping Point
Independent practice consolidated the knowledge and cognitive skills of NLRNs, leading to the internalization of clinical concepts that demonstrated considerable retention.
Technical improvement: I have learned how to perform hemoperfusion, or at least how to execute the procedure effectively. (N9)
For instance, the concepts of caring for a patient and looking after a patient are distinct. (N9)
My communication and collaboration skills with doctors and family members have significantly improved. (N9)
Subtheme 5.2 The Maturation of Resilience
The psychological resilience fostered through independent practice was conceptualized not as mere stress resistance, but as a dynamic, cultivable professional capability. This capacity was defined by three core attributes: emotional adaptability, cognitive flexibility, and purposeful social connectivity.
It might be easier now. I have encountered such patients before and feel more equipped to handle these situations. (N9)
While I still experience anxiety, I am significantly stronger than I was in the past. (N10)
Initially, I was quite reserved, constantly fearing that I might make mistakes. (N17)
Now, I prepare by rehearsing plans in my mind and creating a work plan for the following day. (N20)
Subtheme 5.3 Deepening of Work Values
The experience of working independently served as a catalyst for NLRNs, prompting a reconceptualization of their role from a mere profession to a mission-driven career. This shift enhanced their sense of accomplishment and fosters professional autonomy.
This experience has been profoundly meaningful to me. For instance, I have identified several concerning signals from patients and addressed them promptly. (N2)
It is immensely rewarding to provide comprehensive care for a patient upon their departure from the department, which enhances my job satisfaction significantly. (N14)
Discussion
This study systematically explored the stress coping and the development of psychological resilience among NLRNs during their transition to independent practice in the ICU through qualitative analysis methods. The research primarily identified that NLRNs underwent a series of critical transitional processes during this phase, including deconstruction and reconstruction of identity, the gap between know and do, ethical dilemmas and emotional labor, organizational socialization, turning point and “metamorphosis”. The development of psychological resilience and the consolidation of professional values signify critical milestones in NLRNs’ successful transition to independent practice.23 This transformation manifests through four interconnected dimensions: cognitively, through the reconstruction from knowledge application to clinical judgment; technically, through the sublimation from mechanical imitation to tacit knowledge internalization; professionally, through the identity shift from peripheral observer to community member; and emotionally, through the maturation from natural reactions to strategic emotional management. Based on these findings, this study constructs a “Challenge-Transformation-Growth” model of resilience development, offering a novel theoretical perspective and practical framework for comprehensively understanding and effectively intervening in the professional adaptation process of novice nurses.
This study revealed that despite holding formal nursing licenses, NLRNs in the ICU frequently experienced a contradictory sense of “illegitimacy”, manifesting as self-perceptions of being “acting nurses” or even “illegal practitioners”. This phenomenon aligned with Legitimate Peripheral Participation theory,24 which posited that novices occupy marginal roles within a community of practice before attaining full membership. The marginalization of NLRNs was shaped by a dual cognition: externally, by a lack of team affirmation, and internally, by self-doubt. This dynamic was readily amplified within the distinct culture of the ICU—an environment that placed a high premium on advanced technical skills and rapid decision-making.25 Given the critical condition of patients and the complexity of treatments, clinical teams exhibited considerable reluctance to fully delegate primary responsibilities to novices. Consequently, although the supervision by mentors was intended as support, it paradoxically reinforced the NLRN’s perception of being an inadequately prepared outsider.26 Furthermore, the three distinct attitudes toward the transition period (excitement, anxiety, and indifference) highlighted individuals’ divergent appraisals of this professional challenge, which subsequently influenced their level of engagement in the identity reconstruction process. While previous studies confirmed that emotional fluctuations during this adaptation phase are inevitable,27 our findings demonstrated that such variability did not preclude the ultimate accomplishment of the critical transition from imitation to cultivated critical thinking. Crucially, this evolution represented more than mere technical proficiency; it constituted a fundamental reconstruction of professional identity, through which NLRNs began to establish their own work values, clinical judgment, and sense of responsibility. This study contends that this profound cognitive shift served as the foundational element for reducing workplace anxiety and building long-term adaptive capacity. The development of critical thinking proved particularly vital in the ICU environment, where nurses frequently confronted information overload, clinical uncertainty, and life-and-death decisions.28 Without the ability to critically analyze situations, prioritize actions, and exercise autonomous judgment, NLRNs remained dependent on external guidance, thereby perpetuating feelings of anxiety and incompetence.29 Therefore, by explicitly valuing and fostering critical thinking in novices as the cornerstone of professional identity reconstruction, transition-related anxiety could be more effectively mitigated.
The findings of this study indicated that the transition to independent practice placed NLRNs at risk of adopting ineffective coping strategies, experiencing information overload, and facing difficulties in clinical decision-making. It was consistent with the results of previous studies that NLRNs frequently encounter decision-making hesitation due to a disconnect between theoretical knowledge and practical application.30 Zhou et al also reported similar issues, including information overload and ineffective coping.31 These challenges were particularly pronounced in the high-risk, high-complexity environment of ICU. The underlying causes were not solely attributed to new nurses’ lack of practical experience; rather, they also stemmed from the structural limitations of classroom education. While traditional nursing education effectively provided systematic “know-what” knowledge, it failed to adequately convey the clinically essential “know-how”, “know-when”, and “know-why” components of practice. The ICU setting was highly intricate, necessitating that nurses not only mastered multidisciplinary foundational skills—such as ventilator operation and blood purification equipment handling—but also processed vast streams of patient data and managed family communications.32 This combination led to systemic cognitive overload for new nurses who were still in the process of skill integration. Such knowledge could not be directly taught; it must be constructed through hands-on experience and reflective learning.33 In this study, NLRNs actively engaged in observational learning, reflection, and the accumulation of personal experience. Through these processes, they began to internalize the tacit rules and unspoken understandings of expert practice, achieving a fundamental shift from passive knowledge acquisition to active knowledge construction. This self-directed internalization of implicit cognition and practical skills enabled them to transform overwhelming explicit information into actionable clinical intuition, thereby converting ineffective coping strategies into strategic actions and fostering greater psychological resilience.34
This study indicated that ethical dilemma served as the primary stressor for unlicensed NLRNs during transitional periods, while emotional labor represented its main manifestation.35,36 Consistent with previous research,35 ethical dilemma was identified as a key psychological stressor for ICU nurses that impaired mental health. The root cause of ethical dilemmas encountered by novice NLRNs stemmed from the imbalance between their role competence and ethical responsibilities. On one hand, they had acquired the statutory duties of registered nurses and a preliminary ethical awareness, which enabled them to perceive patients’ best interests and their own professional judgments.37 On the other hand, limited clinical experience and insufficient understanding of complex treatment plans left them lacking the necessary knowledge, operational authority, or communication credibility to implement these judgments effectively.38 The inherent conflicts and tensions arising from such ethical dilemmas directly influenced and shaped the emotional labor of NLRNs. To fulfill their professional roles, they must manage the frustration, anxiety, compassion, and sense of powerlessness triggered by these ethical dilemma while demonstrating the expected qualities of “calmness” and “professionalism”.39 Research suggested that moderate emotional labor, particularly deep acting and internalization of rules, helped maintain their professional functioning, gain team acceptance, and protect them from immediate emotional exhaustion, serving as a preliminary manifestation of resilience.40 However, excessive reliance on surface acting without adequate coping mechanisms, or prolonged exposure to ethical dilemmas without institutional support, might lead to emotional detachment, moral numbness, or occupational burnout due to sustained emotional labor.41 The coping process of NLRNs, both at ethical and emotional levels, represented a critical journey in learning to balance professional demands with self-preservation, while also developing an adaptive professional identity in high-pressure environments. Therefore, supporting NLRNs in cultivating more adaptive emotional strategies and enhancing their ethical decision-making abilities was essential for achieving sustainable professional growth and psychological resilience.
This study found that NLRNs successfully internalized technical competencies and cognitive skills, matured their psychological resilience, and sublimated their work values after engaging in independent clinical practice. Although previous studies documented improvements in skills and confidence among NLRNs following their adaptation period,42 the transformation of NLRNs represented a comprehensive identity reconstruction encompassing cognitive, emotional, and value systems. Independent clinical practice compelled NLRNs to actively integrate and transform previously fragmented and passively acquired knowledge, skills, and social support. Repeated exposure to complex clinical situations sharpened their emotional regulation and cognitive strategies, while the positive feedback gained from effectively managing clinical challenges enhances their sense of professional worth.43 For NLRNs, independent practice signified a more robust professional identity, improved capacity for coping with adversity, and increased career autonomy, collectively laying the foundation for their long-term occupational mental health.31 For healthcare organizations and the nursing profession, NLRNs were not only qualified clinical human resources but also a core force driving the advancement of nursing.44 Consequently, the focus on nurses’ transition to independent practice should shift from merely “reducing transitional stress” to systematically “facilitating transformation”. This involved designing supportive frameworks for independent practice, providing timely reflective guidance, and recognizing competency development to accelerate this process, thereby nurturing nursing professionals with enhanced resilience and professional conviction.
Strengths and Limitation
To the best of our knowledge, this was the first qualitative study in China that explored the stress coping mechanisms and psychological resilience of NLRNs during their transition to independent practice. This study identified the challenges that NLRNs addressed in the long term during this critical period and innovatively revealed specific strategies for achieving transformation throughout the transition. The findings of this study were essential for guiding the development of targeted, evidence-based supportive interventions—such as tailored mentoring programs, mentorship initiatives, and resilience-building workshops—that effectively responded to the needs of NLRNs.
However, this study was not without its limitations: 1) All participants had completed the transition period, and the interviews relied on their recollections, which may introduce bias. Future research should employ a longitudinal qualitative design that tracks the practical experiences of NLRNs from their initial entry into the department through various stages. 2) Variations in training and mentoring methods for NLRNs during the independent practice transition period across different regions may result in bias in the interview data provided by respondents. Therefore, it is essential to investigate the experiences of NLRNs under different mentoring models. 3) Different roles, such as department managers and mentors, possessed unique perspectives on the performance and expectations of NLRNs during the independent practice transition period, which were crucial for understanding the psychological development of NLRNs. However, this study did not include interviews with these groups. Future research should examine the stress and development of psychological resilience among newly hired nurses from diverse perspectives. 4) The reference and application of research findings should fully account for differences in health policies across countries or regions, particularly regarding variations in training and support for new staff, as well as the influence of distinct regional cultures.
Conclusion
This study explored the stress coping mechanisms and the development of psychological resilience among NLRNs during their transition period in ICU, revealing a professional transformation process centered on “challenge-adaptation-growth”. The findings indicated that by actively coping with multiple stressors—including identity formation, theory-practice gaps, ethical dilemmas, and team integration—NLRNs gradually develop psychological resilience characterized by emotional adaptability, cognitive flexibility, and social connectedness, ultimately leading to an enhancement in their work values. These findings not only provided a procedural theoretical framework for understanding the dynamic construction of resilience but also offered clear guidance for nursing management practices. Future transitional support should extend beyond traditional pre-job training and instead systematically design and implement intervention systems that promote reflective practice, provide ethical emotional support, and encourage proactive socialization. These findings underscore the need for longitudinal and intervention studies to validate the proposed “challenge-adaptation-growth” framework. Additionally, they urge healthcare policymakers to incorporate structured resilience support into training programs during the independent practice period, thereby fostering psychological resilience and stress-coping abilities among newly employed nurses.
Acknowledgments
The authors sincerely thank all respondents who participated in this study, as well as the medical staff of the ICU at the First Affiliated Hospital of Xiamen University for their invaluable support during this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
All author affirm that there is no conflict of interest in this study.
References
1. Hampton KB, Smeltzer SC, Ross JG. The transition from nursing student to practicing nurse: an integrative review of transition to practice programs. Nurse Educ Pract. 2021;52:103031. doi:10.1016/j.nepr.2021.103031
2. Xin D, Li W, Zhu W, et al. Relationship between transition shock, resilience, career calling, and retention intention among new nurses: a moderated mediation model. BMC Nurs. 2024;23(1):873. doi:10.1186/s12912-024-02555-y
3. Bai J, Zhang Q, Wang Y, et al. Work environment for Chinese nurses in different types of ICUs: a multisite cross-sectional survey. J Nurs Manag. 2015;23(4):498–15. doi:10.1111/jonm.12163
4. Stewart C. Understanding new nurses’ learning experiences in intensive care. Intensive Crit Care Nurs. 2021;67:103094. doi:10.1016/j.iccn.2021.103094
5. Mealer M, Moss M. Moral distress in ICU nurses. Intensive Care Med. 2016;42(10):1615–1617. doi:10.1007/s00134-016-4441-1
6. Liu C, Yang Y, Zhang Q, Ma Y. Informal learning of ICU new graduate registered nurses: an interpretive phenomenological analysis. Nurse Educ Today. 2025;147:106588. doi:10.1016/j.nedt.2025.106588
7. Chen X, Tao Z, Tang Y, Yan X. Status and associations of nursing practice environments in intensive care units: a cross-sectional study in China. J Nurs Manag. 2022;30(7):2897–2905. doi:10.1111/jonm.13616
8. Labrague LJ, De Los Santos JAA. Transition shock and newly graduated nurses’ job outcomes and select patient outcomes: a cross-sectional study. J Nurs Manag. 2020;28(5):1070–1079. doi:10.1111/jonm.13033
9. Quesada-Puga C, Izquierdo-Espin FJ, Membrive-Jiménez MJ, et al. Job satisfaction and burnout syndrome among intensive-care unit nurses: a systematic review and meta-analysis. Intensive Crit Care Nurs. 2024;82:103660. doi:10.1016/j.iccn.2024.103660
10. Shen X, Zou X, Zhong X, Yan J, Li L. Psychological stress of ICU nurses in the time of COVID-19. Crit Care. 2020;24(1):200. doi:10.1186/s13054-020-02926-2
11. Hu M, Wang Y, Zhang H, et al. The relationship between spiritual climate and secondary traumatic stress in ICU nurses: the mediating role of moral resilience. Intensive Crit Care Nurs. 2025;87:103815. doi:10.1016/j.iccn.2024.103815
12. Alharbi BAA, McKenna N. A systematic review of mindfulness-based interventions to reduce ICU nurse burnout: global evidence and thematic synthesis. BMC Nurs. 2025;24(1):927. doi:10.1186/s12912-025-03507-w
13. Li X, Tian Y, Yang J, et al. Network of job demands-resources and depressive symptoms in critical care nurses: a nationwide cross-sectional study. Crit Care. 2025;29(1):39. doi:10.1186/s13054-025-05282-1
14. Liu X, Cheng F, Jin Y, Chien CW, Chuang YC, Yang WY. Psychological resilience factors in intensive care nursing: a hybrid multi-criteria decision-making model. BMC Nurs. 2024;23(1):566. doi:10.1186/s12912-024-02229-9
15. Parizad N, Lopez V, Jasemi M, Gharaaghaji Asl R, Taylor A, Taghinejad R. Job stress and its relationship with nurses’ autonomy and nurse-physician collaboration in intensive care unit. J Nurs Manag. 2021;29(7):2084–2091. doi:10.1111/jonm.13343
16. Grabbe L, Higgins MK, Baird M, Craven PA, San Fratello S. The community resiliency model® to promote nurse well-being. Nurs Outlook. 2020;68(3):324–336. doi:10.1016/j.outlook.2019.11.002
17. Denzin NK, Lincoln YS. Introduction: the discipline and practice of qualitative research. 2008.
18. See ECW, Koh SSL, Baladram S, Shorey S. Role transition of newly graduated nurses from nursing students to registered nurses: a qualitative systematic review. Nurse Educ Today. 2023;121:105702. doi:10.1016/j.nedt.2022.105702
19. Sandelowski M. Whatever happened to qualitative description? Res Nurs Health. 2000;23(4):334–340. doi:10.1002/1098-240x(200008)23:4<334::aid-nur9>3.0.co;2-g
20. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
21. Zhou H, Wang X, Yu D, et al. Adherence to oral targeted anti-lung cancer therapy: a qualitative interview study. Patient Preference Adherence. 2022;16:995–1004. doi:10.2147/PPA.S341966
22. Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112. doi:10.1016/j.nedt.2003.10.001
23. Cooper AL, Brown JA, Leslie GD. Nurse resilience for clinical practice: an integrative review. J Adv Nurs. 2021;77(6):2623–2640. doi:10.1111/jan.14763
24. Orsmond P, McMillan H, Zvauya R. It’s how we practice that matters: professional identity formation and legitimate peripheral participation in medical students: a qualitative study. BMC Med Educ. 2022;22(1):91. doi:10.1186/s12909-022-03107-1
25. Weatherburn C, Greenwood M. The role of the intensive care nurse in the medical emergency team: a constructivist grounded theory study. Aust Crit Care. 2023;36(1):119–126. doi:10.1016/j.aucc.2022.12.003
26. Taylor C, Foster J. The experiences of new graduate nurses working in a pediatric setting: a qualitative systematic review. J Pediatr Nurs. 2022;67:e234–e248. doi:10.1016/j.pedn.2022.07.005
27. Han P, Duan X, Wang L, Zhu X, Jiang J. Stress and coping experience in nurse residency programs for new graduate nurses: a qualitative meta-synthesis. Front Public Health. 2022;10:979626. doi:10.3389/fpubh.2022.979626
28. Bergauer L, Braun J, Roche TR, et al. Avatar-based patient monitoring improves information transfer, diagnostic confidence and reduces perceived workload in intensive care units: computer-based, multicentre comparison study. Sci Rep. 2023;13(1):5908. doi:10.1038/s41598-023-33027-z
29. Spiva L, Hart PL, Pruner L, et al. Hearing the voices of newly licensed RNs: the transition to practice: a qualitative study suggests that new nurses need more guidance and support than they’re getting. Am J Nurs. 2013;113(11):24–32. doi:10.1097/01.NAJ.0000437108.76232.20
30. Hsiao P, Lin C, Han C, Chen L, Wang L, Su C. Role transition of newly graduated nurses: a qualitative study. Contemp Nurse. 2021;57(6):450–461. doi:10.1080/10376178.2022.2029519
31. Zhou H, Wang X, Du R, et al. The work experience of newly recruited male nurses during COVID-19: a qualitative study. Asian Nurs Res. 2021;15(3):203–209. doi:10.1016/j.anr.2021.05.001
32. Bosco V, Mercuri C, Giordano V, et al. Enhancing ICU care with nurse-written diaries. Nurs Crit Care. 2024;29(6):1355–1362. doi:10.1111/nicc.13161
33. Edwards D, Hawker C, Carrier J, Rees C. The effectiveness of strategies and interventions that aim to assist the transition from student to newly qualified nurse. JBI Libr Syst Rev. 2011;9(53):2215–2323. doi:10.11124/01938924-201109530-00001
34. Lin CC, Thorberg FA, Huang YL, Han CY, Su CC, Chen LC. An exploration of psychological resilience among undergraduate nursing students undertaking an adult nursing virtual practicum during the coronavirus pandemic in Taiwan: a qualitative study. Int J Environ Res Public Health. 2023;20(2):1264. doi:10.3390/ijerph20021264
35. Asadi N, Royani Z, Maazallahi M, Salmani F. Being torn by inevitable moral dilemma: experiences of ICU nurses. BMC Med Ethics. 2021;22(1):159. doi:10.1186/s12910-021-00727-y
36. Kvande ME, Delmar C, Lauritzen J, Damsgaard JB. Ethical dilemmas embedded in performing fieldwork with nurses in the ICU. Nurs Ethics. 2021;28(7–8):1329–1336. doi:10.1177/0969733021996025
37. Hazelwood T, Murray CM, Baker A, Stanley M. Ethical tensions: a qualitative systematic review of new graduate perceptions. Nurs Ethics. 2019;26(3):884–902. doi:10.1177/0969733017727154
38. Dunn H. Ethical decision-making: exploring the four main principles in nursing. Nurs Stand. 2024;39(8):53–57. doi:10.7748/ns.2024.e12346
39. Haahr A, Norlyk A, Martinsen B, Dreyer P. Nurses experiences of ethical dilemmas: a review. Nurs Ethics. 2020;27(1):258–272. doi:10.1177/0969733019832941
40. Feng H, Zhang M, Li X, Shen Y, Li X. The level and outcomes of emotional labor in nurses: a scoping review. J Nurs Manag. 2024;2024(1):5317359. doi:10.1155/2024/5317359
41. Kelly LA, Gee PM, Butler RJ. Impact of nurse burnout on organizational and position turnover. Nurs Outlook. 2021;69(1):96–102. doi:10.1016/j.outlook.2020.06.008
42. Aldosari N, Pryjmachuk S, Cooke H. Newly qualified nurses’ transition from learning to doing: a scoping review. Int J Nurs Stud. 2021;113:103792. doi:10.1016/j.ijnurstu.2020.103792
43. Chen C, Sun X, Zhang Y, Liu Z, Jiao M, Hu Y. Mediating effect of perceived professional benefit on the relationship between spiritual health and spiritual care competence among new nurses: a cross-sectional study. J Nurs Manag. 2025;2025(1):8832454. doi:10.1155/jonm/8832454
44. Regan S, Wong C, Laschinger HK, et al. Starting Out: qualitative perspectives of new graduate nurses and nurse leaders on transition to practice. J Nurs Manag. 2017;25(4):246–255. doi:10.1111/jonm.12456
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.