Back to Journals » Clinical Ophthalmology » Volume 19
Strabismus Surgery in Orthophoric Patients with Abduction Limitation
Authors Phanphruk W ![]() , Hennein L, Hunter DG
, Hennein L, Hunter DG ![]()
Received 22 July 2025
Accepted for publication 23 September 2025
Published 29 October 2025 Volume 2025:19 Pages 3991—3999
DOI https://doi.org/10.2147/OPTH.S543647
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Warachaya Phanphruk,1– 3 Lauren Hennein,1,2,4,5 David G Hunter1,2
1Department of Ophthalmology, Boston Children’s Hospital, Boston, MA, USA; 2Department of Ophthalmology, Harvard Medical School, Boston, MA, USA; 3Department of Ophthalmology, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand; 4Viterbi Family Department of Ophthalmology, University of California San Diego, San Diego, CA, USA; 5Division of Ophthalmology, Rady Children’s Hospital - San Diego, San Diego, CA, USA
Correspondence: David G Hunter, Department of Ophthalmology, Boston Children’s Hospital, 300 Longwood Ave, Fegan 4, Boston, MA, 02115, USA, Tel +1 617 355 6766, Fax +1 617 249 0615, Email [email protected]
Background: Patients with symptomatic esotropia in lateral gaze after lateral rectus recession may not be offered surgery if they are orthophoric in primary gaze due to concern of creating diplopia in primary gaze. There are currently no reports of the surgical management of these cases. The purpose of this study was to report our experience and describe the surgical outcomes for these rare patients.
Methods: A comprehensive, retrospective review of all patients undergoing strabismus surgery at Boston Children’s Hospital over an 11-year period identified all cases of orthophoric patients operated on for diplopia in lateral gaze following lateral rectus recession(s). Surgical approach, pre- and post-operative measurements in diagnostic gaze positions, and surgical outcomes were assessed. We developed a new lateral incomitance (LI) score to characterize patient disability before and after surgery. Main outcome measures were improvement in LI score and lateral gaze diplopia, lack of new-onset diplopia in primary gaze, and patient/surgeon satisfaction.
Results: In all cases, previously recessed lateral rectus muscles were advanced 2– 3 mm with an adjustable suture technique despite anticipated exotropia in primary gaze. Early, large-angle, transient sequential exotropia with diplopia was common. All patients had resolution of lateral-gaze diplopia with improvement in LI score by 8– 18 PD, and none experienced persistent new-onset diplopia in primary gaze (median follow-up 16 months; range, 8.5– 83 months). One patient with a history of surgery for convergence insufficiency developed a well-controlled intermittent exotropia; no other patient had exotropia in primary gaze.
Conclusion: Small, adjustable advancements of the lateral rectus muscles provided excellent results in our series of patients with lateral gaze esotropia caused by previous lateral rectus recessions. Despite large, early overcorrections, LI scores improved in all cases, and no patient had recurrence of symptomatic exotropia. The results will support surgical decision-making in the management of these challenging cases.
Plain Language Summary: Patients with symptomatic esotropia in lateral gaze after lateral rectus recession may not be offered surgery if they are orthophoric in primary gaze due to concern of creating diplopia in primary gaze.In this comprehensive retrospective review, we identified several rare cases meeting strict enrollment criteria of orthophoria in primary gaze but esotropia and diplopia in lateral gaze following lateral rectus recession(s).We found that lateral rectus muscle advancement eliminated lateral gaze diplopia in all cases. Although large, early overcorrections were common, they resolved spontaneously.While there are currently no reports of successful surgical management of these cases, this study demonstrates that orthophoric patients can benefit from surgical intervention for lateral gaze esotropia.
Keywords: strabismus surgery, consecutive esotropia, lateral gaze incomitance, consecutive exotropia, microstrabismus
Introduction
Asymmetric strabismus surgery is known to cause lateral gaze incomitance,1–3 but it may be less recognized that large amounts of symmetric horizontal surgery may cause symptomatic deficits in lateral gaze. In particular, lateral rectus muscle recessions for exotropia may cause esotropia in right and left gaze despite the achievement of orthotropia in primary gaze. While this may be tolerable for many patients, lateral gaze incomitance can produce symptomatic diplopia, causing functional and social deficits that warrant additional intervention.1,4
The management of postoperative diplopia caused by lateral gaze incomitance in orthophoric patients can be challenging due to the potential for causing recurrence of symptomatic exotropia in primary gaze. To our knowledge, the results of intervention in these patients has not previously been published. Our practice has been to perform small, adjustable resection/advancement of the affected lateral rectus muscle(s) when patients seek symptomatic relief. In this study, we report the outcomes of this surgical strategy in orthophoric patients treated for symptomatic, lateral-gaze esotropia. To do so required the development of a new assessment of lateral incomitance that we call the lateral incomitance (LI) score.
Methods
This retrospective study was approved by the Boston Children’s Hospital Institutional Review Board with a waiver of patient informed consent under the Code of Federal Legislation 45 CFR 46.104 (d). This study was conducted in compliance with the Declaration of Helsinki and the Health Insurance Portability and Accountability Act. We retrospectively reviewed the medical records of all patients who underwent strabismus surgery by a single surgeon (DGH) at Boston Children’s Hospital from 7/1/2010 to 5/7/2021. From this search, we identified patients who were orthophoric in primary gaze but who underwent strabismus surgery. Exclusion criteria included Brown syndrome, nystagmus, and superior oblique myokymia. We then further narrowed the cohort to include only those who had an esodeviation in lateral gaze following prior lateral rectus recessions. Minimum follow-up was 6 weeks, and all patients were required to have pre- and post-operative measurements in lateral gaze for inclusion.
The rationale for surgery was to advance the affected lateral rectus muscle to enhance the ability of the eye to abduct, understanding this carried with it a risk of creating an exotropia in primary gaze. While the goal was to advance the muscles, some degree of resection is unavoidable in these cases, and so we refer to the procedure as resection/advancement. The short-tag sliding knot approach5–9 was used to allow for adjustment up to 1 week after surgery in case of under- or over-correction, though early overcorrection (sometimes large) was anticipated and therefore the target that evolved over time was to adjust for any undercorrection but to perform no adjustment for overcorrection unless the exotropia exceeded 20 PD more than 5 days after the procedure. The short-tag adjustable approach is used in all of these cases. In our experience, the muscle position can be adjusted up to 1 week after surgery, after which the muscle adherence to the globe is too strong and there would be in increased risk of suture breakage.7
Surgical Outcome Measures
While most studies of strabismus surgery rely on primary gaze deviation as a main outcome measure, in these cases primary gaze deviation was “orthophoria” before intervention by design. We therefore developed a new objective analysis to characterize the change in lateral comitance by determining the difference in deviation from primary gaze to right gaze and from primary gaze to left gaze, then adding the absolute value of right gaze incomitance + left gaze incomitance (Figure 1). We called this the lateral incomitance (LI) score.
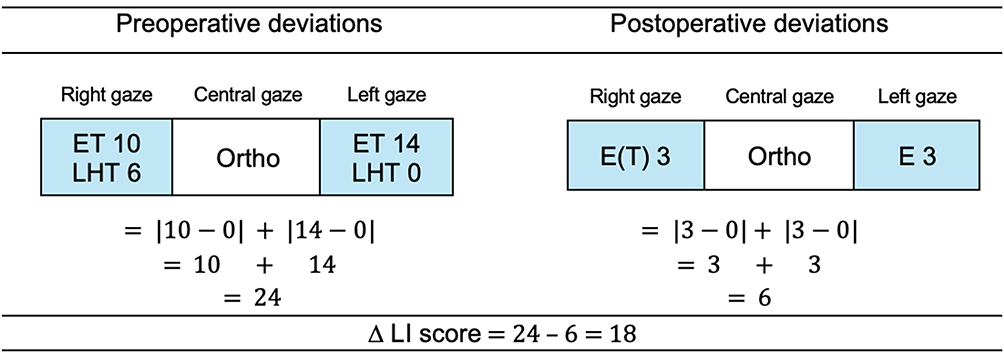 |
Figure 1 Calculation of lateral incomitance (LI) score for Case 1. Vertical deviations are ignored for the calculation. Final Δ LI score for this case is 24–6 = 18. All measurements are in prism diopters. Abbreviations: ET, esotropia; LHT, left hypertropia; Ortho, orthophoria. |
Pre- and post-operative measurements in at least five gaze directions at distance and in primary gaze at near (1/3 m), as well as near stereopsis, were recorded for all patients. Ductions were documented on a grading scale from −4 to +4. Presence of an abnormal head posture, surgery performed, and need for additional surgery were evaluated. Reasons for surgery were documented. Surgical outcomes were assessed at the scheduled 2-month follow-up visit and at the most recent available examination (final follow-up).
In addition to post-operative measurements, surgeon assessment of alignment and patient satisfaction were reviewed. In our practice, post-operative patients often (but not always) receive a satisfaction survey at the 2-month post-operative visit. This survey asks the patient to categorize their satisfaction on a Likert scale ranging from “very satisfied” to “very dissatisfied.” Results of this survey were recorded if available, otherwise patient satisfaction was obtained from review of comments recorded in the clinic note.
Study data were collected and managed using REDCap (Research Electronic Data Capture)10,11 tools hosted at Boston Children’s Hospital, with statistical analysis consisting of mean and median calculations only.
Results
The record review identified 44 surgical patients with minimal pre-operative primary gaze strabismus who met exclusion criteria and follow-up requirements, of whom four had orthotropia in primary gaze with esotropia and symptomatic diplopia in lateral gaze following lateral rectus muscle recession(s) (Table 1). All patients were female, with a median age of 21.5 years at surgery (range, 7–58 years). All four patients had previous strabismus surgery, including two also treated with botulinum toxin in an unsuccessful effort to manage the post-operative diplopia. None had diplopia in primary position, and all had high-grade stereopsis (20–40 arcsec). Esotropia ranged from 6 PD to 18 PD in a single lateral gaze direction, with the total targeted correction ranging from 12 PD (ET 6 in right gaze and left gaze) to 26 PD (ET 8 in right gaze and 18 in left gaze) (Figure 2). The average preoperative LI score was 20 PD (range 12–26 PD). Two patients had a V-pattern and reported diplopia in downgaze. (Table 2).
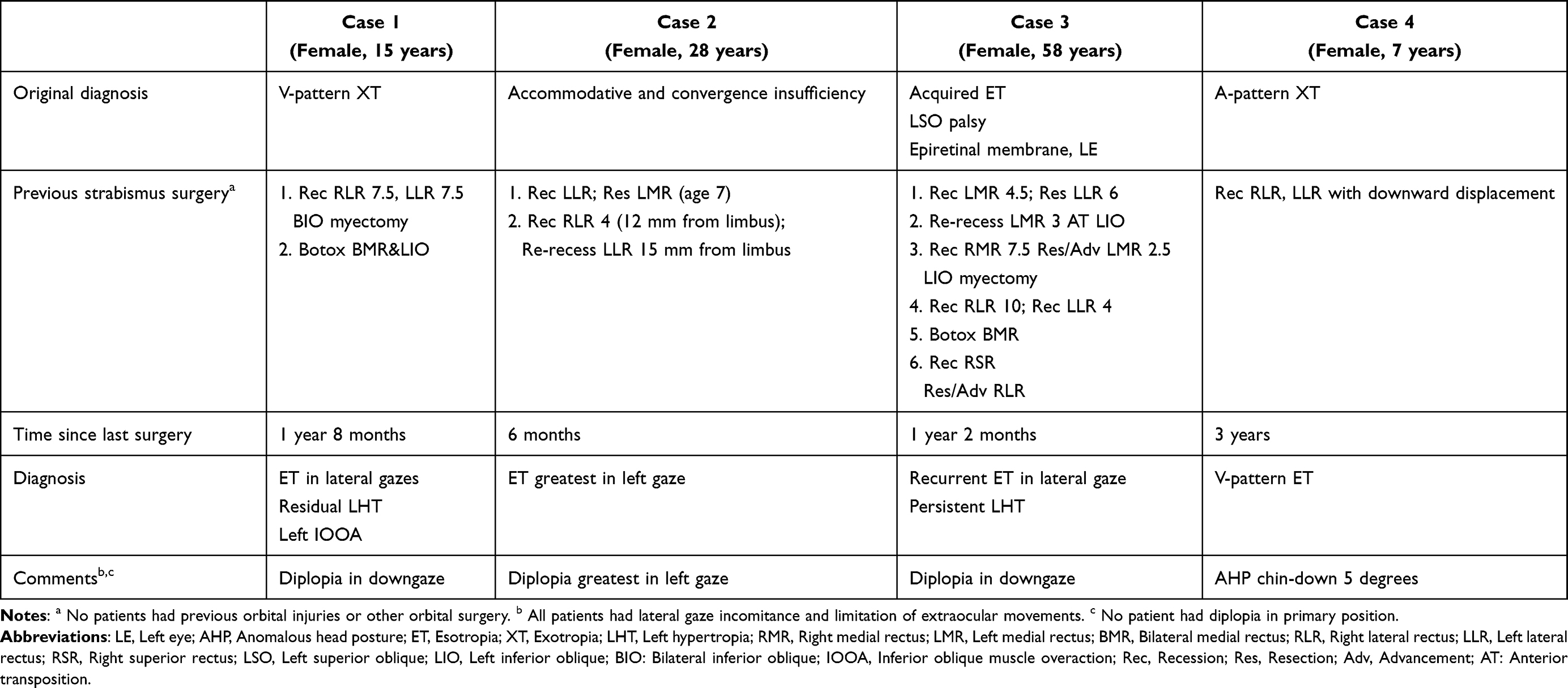 |
Table 1 Patient Profiles |
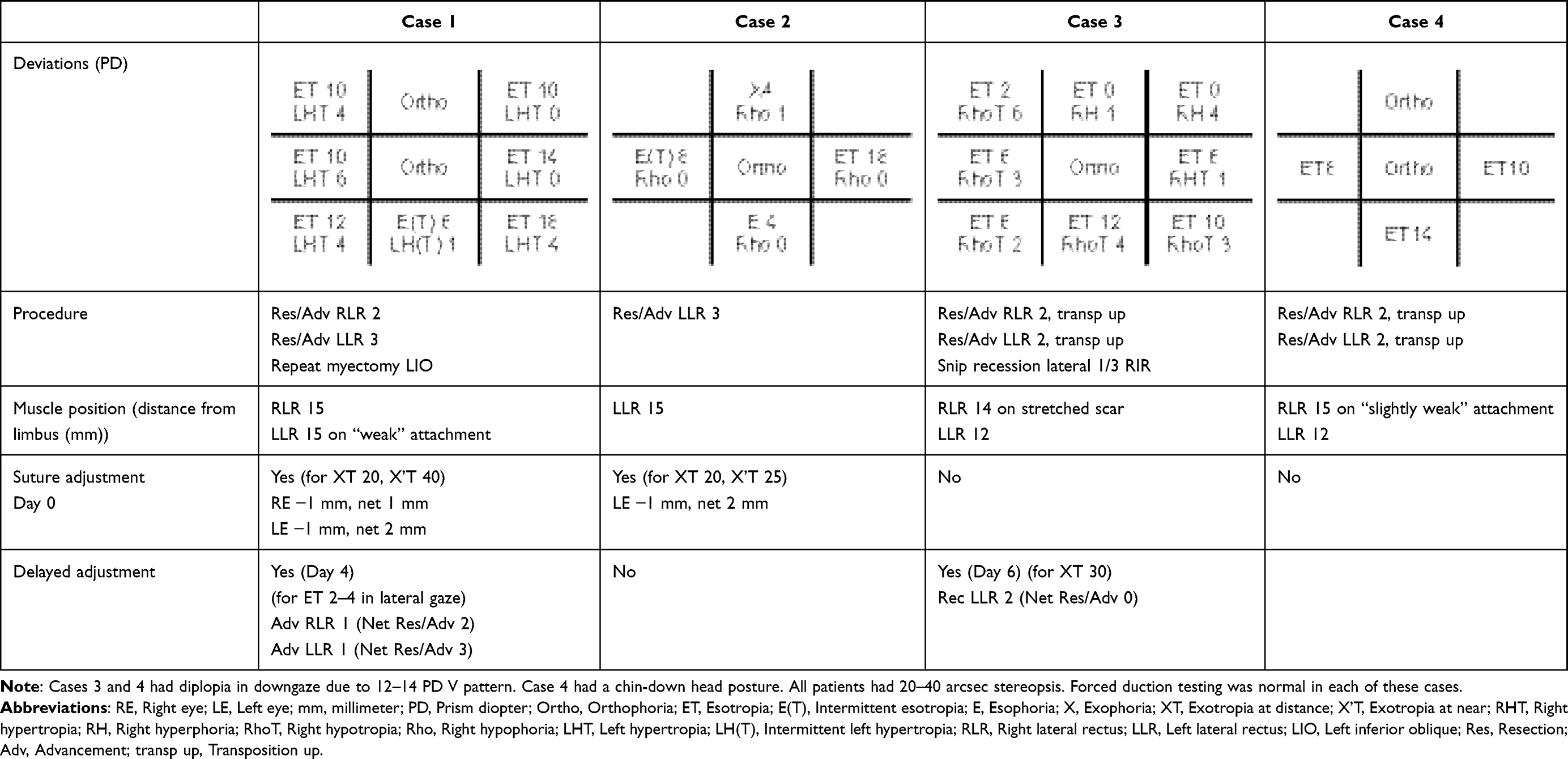 |
Table 2 Preoperative Measurements |
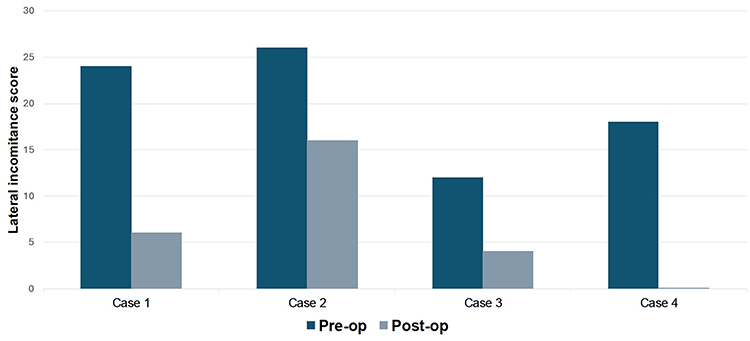 |
Figure 2 Lateral incomitance (LI) score. Results for all patients shown. See Figure 1 for how the LI score is calculated. Patient 4 post-op LI score was 0 as indicated by a small non-negative bar. |
All patients underwent adjustable resection/advancement of one or both lateral rectus muscles to treat lateral gaze esotropia (Table 2)., ranging from a left lateral rectus resection of 3 mm in Case 2 (unilateral) to bilateral lateral resections of 2–3 mm. Suture adjustment was performed on the day of surgery in cases 1 and 2 for overcorrections of XT 20 PD at distance, XT 40 PD at near (case 1) and XT 20 PD at distance, XT 25 PD at near (case 2). However, case 1 was then undercorrected at post-op day 4 and so was re-adjusted to again increase the surgical dosage. Case 3 had a very large overcorrection (XT 30) on the day of surgery but, based on the experience of cases 1 and 2, no adjustment was performed. By post-op day 6 she remained overcorrected despite the small amount of surgery, with XT 30 PD at distance, 45 PD at near, with diplopia. The left lateral rectus muscle was therefore recessed 2 mm to decrease the XT to 20 PD at distance and near for net surgery of right lateral rectus resection/advancement of 2 mm.
Surgical Outcomes
Median follow-up was 16 months (range, 8.5–83 months). Esotropia was reduced or eliminated in lateral gaze and LI Scores improved 8–18 PD in all patients (Figure 3), with no patient reporting diplopia either in primary gaze or lateral gaze by the time of the 2-month follow-up visit (Table 3).
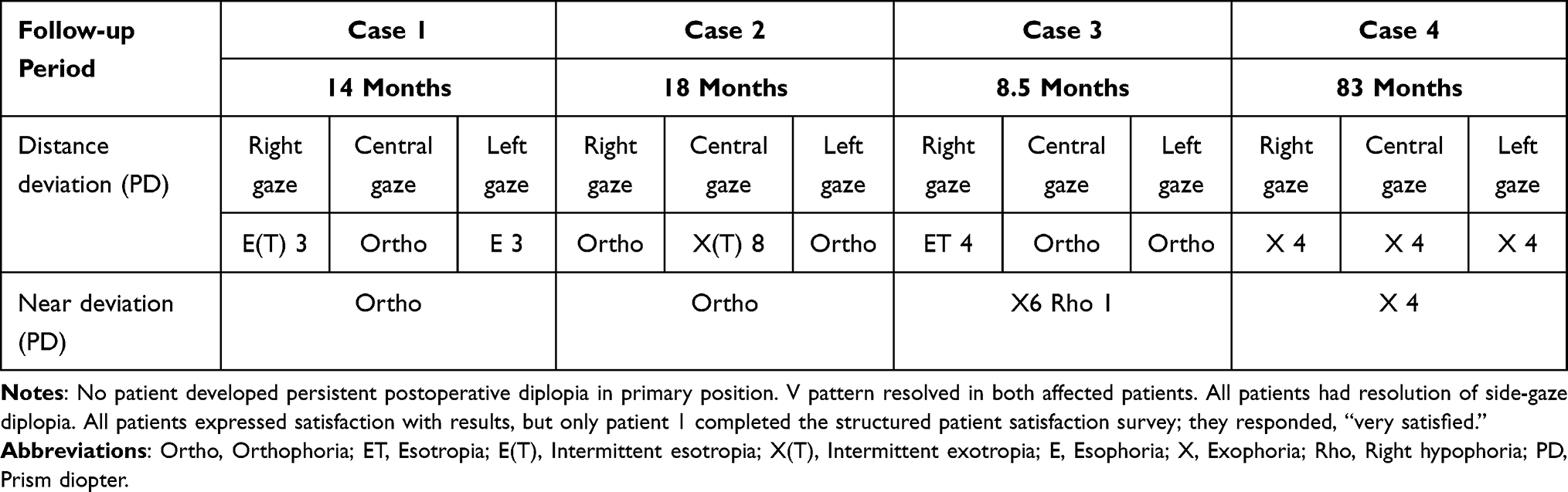 |
Table 3 Postoperative Measurements at Last Visit |
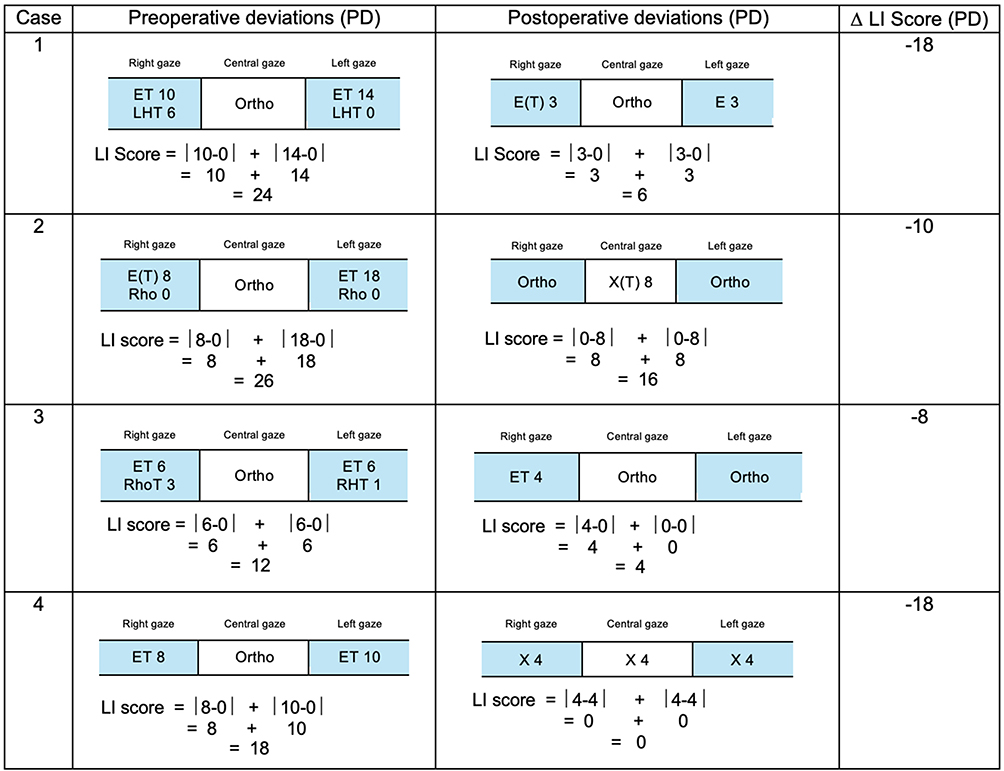 |
Figure 3 Lateral incomitance (LI) score improvement. The figure demonstrates the LI scoring before and after surgery for every case. Abbreviations: LI Score, Lateral incomitance score; Δ LI Score, The difference of preoperative and postoperative LI Scores; PD, Prism diopter. |
All patients recovered full abduction except Case 3 who had a symmetric, −1 residual abduction deficit that was asymptomatic. One patient (case 2) had a recurrence of small-angle, well-controlled intermittent exotropia in primary gaze. This patient had a history of multiple procedures for convergence insufficiency. She was comfortable managing her post-operative intermittent exotropia of 8 PD and did not require further intervention.
Stereopsis remained within the range of 20–50 arcsec before and after surgery, with two patients showing mild improvement and one decreasing from 20 to 50 arcsec. That highly myopic patient had developed an epiretinal membrane, with distortion on Amsler grid testing, and was referred to a retina specialist. One patient (case 4) with a V pattern and chin-down head posture had resolution of the head posture when the V pattern was eliminated by upward transposition of the lateral rectus muscles at the time of advancement.
All patients reported satisfaction with the postoperative outcome. No patients required additional surgery. Surgeon assessment of post-operative alignment was recorded as “excellent” in all cases.
Discussion
While overcorrection is a risk after any surgery for exotropia, most such overcorrections also produce an esotropia in primary gaze, making subsequent surgical planning relatively straightforward. In rare cases, alignment is satisfactory in primary gaze, but an overcorrection in lateral gaze can cause disabling diplopia. Such cases are a challenge for strabismus surgeons, out of concern that treating the lateral gaze esotropia will cause recurrence of the original problem – symptomatic exotropia in primary gaze.
Three of the 4 patients in our series had relatively symmetric, symptomatic esotropia in lateral gaze and were orthophoric in primary gaze. Of note, despite performing 2–3 mm resection/advancement of both lateral rectus muscles in these patients, and with the successful elimination of diplopia in lateral gaze, they did not develop an exotropia in primary gaze. The reasons for this are a matter of speculation. Perhaps the patients (all of whom had high-grade stereopsis) had strong fusional divergence in primary gaze and had a pre-operative, primary gaze esotropia that could not be detected on cover testing. However, we believe that these patients were truly orthophoric in primary gaze, but the resection/advancement gave better mechanical advantage to the lateral rectus muscles or placed them in a different place on the length-tension curve without changing primary gaze alignment, improving abduction – essentially the reverse of a posterior fixation suture. While theoretically a resection might compromise adduction, in these cases the muscles are being advanced closer to their original physiologic insertion. While there may have been short-term motility restriction, we did not observe any significant post-operative restriction after either bilateral or unilateral surgery.
An alternative approach to consider in these cases might have been a mini-tenotomy12 or mini-recession of the medial rectus muscles.13 However, we do not believe this procedure would have been able to correct as much as 26 PD of lateral gaze incomitance as was achieved in these cases. If mini-tenotomy failed, it might have then made it more difficult to subsequently advance the lateral rectus muscles to restore their abducting ability without creating a symptomatic exotropia in primary gaze.
We developed the LI score as a means of quantitatively characterizing lateral gaze incomitance in these patients. Previous studies have measured lateral incomitance by subtracting the right gaze deviation from the left gaze deviation.1 However, since many of our patients had the same esodeviation in right and left gaze (for example, ET 12 in right and left gaze but orthophoric in primary gaze), the measured lateral incomitance would have been 0 PD. The disadvantage of our LI score is demonstrated in case 2, where the post-op esotropia was 0 in right and left gaze, but X(T) 8 PD in primary gaze. In that setting, 8 PD is counted for both right (8–0) and left (8–0) gaze and the lateral incomitance score was 16 when, intuitively, a score of 8 would have seemed to be more appropriate.
No patients experienced new-onset diplopia in primary gaze by the 2-month follow-up visit, and no patients required additional surgery. All patients reported improved diplopia and demonstrated improvement in lateral gaze at the final visit, with corresponding improvement in the LI score. Patient satisfaction and surgeon assessment of postoperative alignment were generally high.
We have described the surgical management of orthophoric patients with more complex, incomitant horizontal and vertical deviations elsewhere.14 In those cases and in the present series, the use of adjustable sutures was key to assuring that the post-operative alignment would be within the targeted range. It is remarkable that 3 of the patients had large overcorrections (XT 20 PD or greater) at post-operative assessment on the day of surgery. Informed by case 1, where we reduced the advancements, only to find recurrence of the esotropia 4 days later (necessitating a second adjustment to restore the original surgical dosage), we now accept large amounts of exotropia in the early post-operative period, adjusting by a small amount only if the overcorrection remains large after 5–6 days, and definitely adjusting to increase the surgical dosage for persistent esotropia in lateral gaze. Considering the risk of persistent overcorrection if a large exotropia is allowed to remain on post-op day 1 without adjustment, we feel that the short-tag sliding knot approach5–9 is an essential element of care in these cases. While patients may experience some discomfort during a delayed adjustment, we and others15 have been able to successfully carry out these delayed adjustments in the office in adult patients without difficulty in most cases.
This is a limited study, with all of the confounders of retrospective case series applicable. The series includes only a small number of participants. This limits the generalizability and strength of the conclusions, particularly regarding the consistency of lateral incomitance correction. Field of binocular single vision, a valuable objective indicator of improved function, was not routinely mapped in our patients. Surgeon and patient bias may have overstated the degree of subjective improvement following surgery. The patch test was not performed pre-operatively, meaning that some patients may not have been truly orthophoric at the pre-operative visit. Despite these limitations, our goal is to provide surgeons facing orthophoria with symptomatic lateral incomitance following lateral rectus recessions with a surgical approach that was successful in all four of our patients.
In conclusion, small, adjustable advancements of the lateral rectus muscles provided excellent results in our series of patients with lateral gaze esotropia caused by previous lateral rectus recessions. Despite large, early overcorrections, LI scores improved in all cases, and no patient had recurrence of symptomatic exotropia. With the option of delayed suture adjustment an essential part of the approach considering the early overcorrection sometimes observed, the observed outcomes in this small case series will support surgical decision-making in the management of these challenging cases.
Ethics Statement
This retrospective study was approved by the Boston Children’s Hospital Institutional Review Board.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Children’s Hospital Ophthalmology Foundation, Inc.
Disclosure
Presented at the American Association for Pediatric Ophthalmology and Strabismus annual meeting, Scottsdale, Arizona, March 26th, 2022. The authors declare that they have no relevant conflict of interest to report.
References
1. Graeber CP, Hunter DG. Changes in lateral comitance after asymmetric horizontal strabismus surgery. JAMA Ophthalmol. 2015;133(11):1241–1246. doi:10.1001/jamaophthalmol.2015.2721
2. Yoon CH, Kim SJ. Lateral incomitancy and surgical results in intermittent exotropia. Br J Ophthalmol. 2014;98(10):1404–1408. doi:10.1136/bjophthalmol-2014-305132
3. Deacon BS, Fray KJ, Grigorian AP, et al. Unilateral strabismus surgery in patients with exotropia results in postoperative lateral incomitance. J AAPOS. 2014;18(6):572–575. doi:10.1016/j.jaapos.2014.08.010
4. Sharma M, Hunter DG. Diplopia after strabismus surgery. Semin Ophthalmol. 2018;33(1):102–107. doi:10.1080/08820538.2017.1353827
5. Nihalani BR, Hunter DG. Adjustable suture strabismus surgery. Eye. 2011;25(10):1262–1276. doi:10.1038/eye.2011.167
6. Engel JM, Guyton DL, Hunter DG. Adjustable sutures in children. J AAPOS. 2014;18(3):278–284. doi:10.1016/j.jaapos.2013.12.015
7. Nihalani BR, Whitman MC, Salgado CM, Loudon SE, Hunter DG. Short tag noose technique for optional and late suture adjustment in strabismus surgery. Arch Ophthalmol. 2009;127(12):1584–1590.
8. Heidary G, Aakalu VK, Binenbaum G, et al. Adjustable sutures in the treatment of strabismus: a report by the American Academy of Ophthalmology. Ophthalmology. 2022;129(1):100–109. doi:10.1016/j.ophtha.2021.07.026
9. Phanphruk W, Alkharashi M, Bilge A, Hunter DG. Sedated suture adjustment in children undergoing adjustable suture strabismus surgery. J AAPOS. 2017;21(3):196–200. doi:10.1016/j.jaapos.2017.05.010
10. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010
11. Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019;95:103208. doi:10.1016/j.jbi.2019.103208
12. Wright KW. Mini-tenotomy procedure to correct diplopia associated with small-angle strabismus. Trans Am Ophthalmol Soc. 2009;107:97–102.
13. Gurland J, Vagge A, Nelson LB. One-muscle strabismus surgery: a review. J Pediatr Ophthalmol Strabismus. 2018;55(5):288–292. doi:10.3928/01913913-20180327-03
14. Phanphruk W, Hennein L, Hunter DG. Strabismus surgery in orthophoric patients with symptomatic, asymmetric vertical or horizontal incomitance. Am J Ophthalmol. 2023;249:29–38. doi:10.1016/j.ajo.2022.12.019
15. Robbins SL, Granet DB, Burns C, et al. Delayed adjustable sutures: a multicentred clinical review. Br J Ophthalmol. 2010;94(9):1169–1173. doi:10.1136/bjo.2009.169987
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.