Back to Journals » OncoTargets and Therapy » Volume 11
Stereotactic body radiotherapy using the CyberKnife® system in the treatment of patients with liver metastases: state of the art
Authors Ihnát P ![]() , Skácelíková E, Tesař M, Penka I
, Skácelíková E, Tesař M, Penka I
Received 19 February 2018
Accepted for publication 4 June 2018
Published 10 August 2018 Volume 2018:11 Pages 4685—4691
DOI https://doi.org/10.2147/OTT.S165878
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jianmin Xu
Peter Ihnát,1,2 Eva Skácelíková,3 Milan Tesař,1,2 Igor Penka1,2
1Department of Surgery, University Hospital Ostrava, Ostrava, Czech Republic; 2Department of Surgical Studies, Faculty of Medicine, University of Ostrava, Ostrava, Czech Republic; 3Department of Oncology, Faculty of Medicine, University of Ostrava, Ostrava, Czech Republic
Background: The management of patients with liver metastases presents a challenging problem in clinical oncology. Patients with limited involvement of the liver may be suitable for surgical resection or local ablative techniques. Stereotactic body radiotherapy (SBRT) presents an emerging new technology that has shown high efficacy in ablating tumors at various disease sites.
Methods: A comprehensive literature search was performed to identify articles in regard to the SBRT in the treatment of patients with liver metastases.
Results: SBRT allows for the delivery of high-dose radiation in few fractions to the tumor with extreme accuracy, while minimizing the damage to normal surrounding tissue. The CyberKnife® system is an image-guided robotic system that delivers SBRT, tracks tumors during respiration, and automatically adjusts treatment for any patient movement. The most frequently used indications for CyberKnife® therapy are ≤5 liver metastases with maximum tumor sizes of 6 cm, no extrahepatic disease, good performance status, and adequate hepatic functions. Local control rates range from 70%–100% at 1 year and from 60%–90% at 2 years. Severe toxicity related to SBRT is uncommon – grade three side effects occur in less than 5% of cases. Despite excellent local control rates, out-of-field metastatic progression (out-of-field hepatic metastases and extrahepatic metastases) develops in a substantial proportion of patients after SBRT. Therefore, it seems essential to improve the selection of patients with liver metastases for SBRT.
Conclusion: The CyberKnife® system presents an effective minimally invasive treatment modality for patients with hepatic oligometastases who are not suitable candidates for radical liver resection. The available data suggest that liver metastases can be treated by CyberKnife therapy with very low toxicity and excellent local control rates.
Keywords: CyberKnife, liver metastases, stereotactic body radiotherapy, indications, clinical outcomes, toxicity
Introduction
The management of patients with liver metastases presents a challenging problem in clinical oncology. Without treatment, the 3-year survival rates remain dismal at 3%.1,2 Systemic treatment given with palliative intent is the only available therapy for the vast majority of patients.3,4 Patients with limited involvement of the liver may be suitable for surgical resection or local ablative techniques.
Despite significant advancements in surgical techniques during the last decades, only a small proportion of patients (20%–30%) are eligible for surgical resection because of tumor location, multifocality, proximity of tumor to vessels, or inadequate functional hepatic reserve.3,4 In an effort to provide treatment for patients who are not candidates for surgery, novel treatment approaches to control and potentially cure liver oligometastases are being explored (such as chemoembolization, thermal ablation, radiotherapy).5–7
Stereotactic body radiotherapy (SBRT) presents an emerging new technology that has shown high efficacy in ablating tumors at various disease sites. SBRT allows for the delivery of high-dose radiation in few fractions to the tumor with extreme accuracy, while minimizing the damage to normal surrounding tissue.6,8,9 The CyberKnife® system (Accuray Incorporated, Sunnyvale, CA, USA) is an image-guided robotic system that delivers SBRT, tracks tumors during respiration, and automatically adjusts treatment for any patient movement.10,11
The aim of the present paper is to offer an up-to-date review of current available data on the rationale, feasibility, safety, and outcomes of SBRT using the CyberKnife system in the treatment of patients with liver metastases.
Materials and methods
A comprehensive literature search was performed to identify articles in regard to the SBRT in the treatment of patients with liver metastases. The search combined the following terms: SBRT, CyberKnife, robotic radiotherapy, and liver metastases. Sources were Medline, PubMed, and Google Scholar database. The Medline search was combined with back tracking based on published reference lists.
Results
Stereotactic body radiotherapy (SBRT)
The concept of stereotactic radiosurgery for intracranial tumors treatment was first proposed by Lars Leksell in 1951.12 During the following decades, several systems of linear accelerators have been developed with an aim to deliver high, ablative radiation doses with maximal dose fall-off outside the treatment volume.6,13 However, the use of stereotactic radiosurgery for extracranial tumor treatment has been limited because of movement caused by the respiratory cycle.14
SBRT originated from the principles of a frame-based stereotacic targeting system used in neurosurgery. SBRT is defined as the external beam radiotherapy used to deliver larger doses of highly conformal radiation with steep dose gradients toward the surrounding normal tissue over a limited number of fractions to an extracranial target within the body.15 An image-guided targeting system (resulting from advancements in image guidance and radiation delivery technology) allows the SBRT to be used for whole-body radiosurgery.7,9
In 1997, Adler et al introduced the CyberKnife® Robotic System (Accuray Incorporated) – a new frameless robotic system for radiosurgery.16 CyberKnife consists of a linear accelerator mounted on an industrial robotized arm, which allows 6 df, allowing up to 1,320 different treatment positions with sub-millimetric accuracy.13,17
CyberKnife was the first robotic device in which a human was permitted to be present within a robot workspace. As safety precautions, regulations limit the speed of motion of the robot and require its travel only along a set of pre-defined paths, stopping at treatment “nodes.” At each stopping position, the robot can change the beam angle within limits to create 12 beam directions at each node.6
The principal components of the CyberKnife Robotic System (robotized arm, linear accelerator, collimator, X-ray imaging, etc.) are presented in Figure 1. The fundamental design advantage of the CyberKnife Robotic System is its method of active image guidance during treatment. Tracking system software monitors respiratory movements through LED’s applied to the patient’s chest and correlates the data with movements of a fiducial-marked target lesion. The sophisticated system allows increasing the dose per session beyond 8 Gy with a high degree of spatial accuracy. Although the system is capable of imaging before every treatment beam, imaging every third to fifth beam (or every 20–60 seconds) is sufficient. The treatment course usually consists of 1–5 sessions, with each session lasting ~20–30 minutes.6,13
 | Figure 1 Cyberknife® Robotic System and its components. 1. Robotized arm, 2. linear accelerator, 3. X-ray imaging, 4. X-ray detectors, 5. Robocouch™ table. |
Treatment options for patients with liver metastases
Surgical resection is considered to be the optimal treatment modality with a curative effect offering long-term survival to the subgroup of patients with limited metastatic disease in the liver. Nonrandomized studies have shown that patients undergoing radical resection have 5-year survivals of 30%–58%.2,18,19 However, resection is possible only in 10%–25% of patients with liver metastases at the time they are first detected. Patients with liver oligometastases unsuitable for radical surgical resection (due to technical or medical reasons) may be treated by local ablative techniques such as radiofrequency ablation (RFA), cryotherapy, radioembolization, laser-induced thermotherapy, or SBRT.9
RFA has become the most widely used ablative technique, which is based on the local application of radiofrequency energy producing thermal destruction of the tumor. Radiofrequency energy is applied through a needle electrode placed directly into the tumor.5,20 When optimal conditions are reached, effective ablation of hepatic lesions with diameters of 5–7 cm is possible.5,20,21 There are several limitations of RFA application, especially in regard to lesion’s location and size, proximity to great vessels, or subcapsular position. Local recurrence after RFA is reported in up to 40% of patients; the tumor size and proximity to great vessels are associated with higher risk of local recurrences.3,20,22
SBRT presents a novel, locally ablative technique with excellent local control rates. With respect to the aforementioned limitations of RFA, SBRT seems to be superior in the local ablation of liver metastases because of higher local control rates, low toxicity, and significantly less technical limitations.8–10,17 During multidisciplinary team meetings, SBRT of unresectable liver metastases should, therefore, be preferred (provided the CyberKnife system is available).
There is a significant heterogeneity regarding the indication criteria and parameters concerning SBRT of liver metastases (colorectal carcinoma vs other primary subtypes, different tumor volumes, various total doses/doses per fraction, dosimetric planning criteria, etc.) in the available literature.9,17 The most frequently used indications for CyberKnife therapy are ≤5 liver metastases with maximum tumor sizes of 6 cm, no extrahepatic disease, good performance status, and adequate hepatic functions.8–11,17,23–25 In our center (Ostrava, Czech Republic), the following indication criteria for CyberKnife therapy of liver metastases are employed:
- ≤5 liver metastases;
- diameter of the lesions to be treated ≤6 cm;
- cancer controlled outside the liver;
- volume of healthy liver >700 cm3;
- good performance status (Karnofsky performance score ≥70);
- life expectancy of more than 3 months; and
- adequate liver function (aspartate aminotransferase and alanine aminotransferase ≤5×upper limit of normal [ULN]).
All substantive limitations of the SBRT therapy of liver metastases can be deduced from the indication criteria for SBRT. The relative limitation of CyberKnife therapy is the proximity of adjacent critical structures (lung, esophagus, heart, stomach, etc.). That is why CyberKnife treatment planning has to be adjusted with respect to the proximity of these critical structures.
The main disadvantage of the SBRT therapy is its limited availability to patients because of the restricted number of CyberKnife devices worldwide. CyberKnife therapy requires specialized therapeutic teams, availability of technical facilities, and decisions made at multidisciplinary consultative meetings.
SBRT planning and doses
In patients who are candidates for CyberKnife therapy, radio-opaque fiducial markers are inserted within and around the tumor to enable tracking. Radio-opaque 3-mm long gold fiducials are placed percutaneously under CT guidance by an interventional radiologist. A treatment planning CT scan with intravenous contrast to highlight the tumor lesion(s) is performed at least 1 week after fiducial placement to avoid marker migration between the simulation and the start of the treatment.17,23,24
A gross tumor volume (GTV) is delineated on the CT scans. Typically, a margin of 3–5 mm is added to the GTV to form the planning target volume (PTV).24 The adjacent critical structures (lung, esophagus, heart, thoracic wall or ribs, kidneys, intestinal structures, stomach, spinal canal, and a 4-mm skin area) are delineated during the treatment planning. Presently, SBRT is usually performed by the CyberKnife system (Accuray Incorporated) and planned using Multiplan treatment planning software. The Synchrony Respiratory Tracking System is used to continuously tract fiducial position and synchronize beam delivery with respiratory motion.6,8,10
The SBRT prescription doses for the ablation of liver metastases vary in published literature. The authors of a multicenter study reported that local control rates may be a function of dose per fraction, total dose, and biologically equivalent dose. The authors, therefore, recommend a dose of at least 48 Gy in three fractions in the treatment of liver metastases.24 Most SBRT studies used doses ranging from 30–60 Gy in one-to-six fractions.25 According to available data, a minimal dose of 40 Gy in three fractions seems to be necessary to obtain good local control.17,24–26
In a prospective dose-escalation study, different doses (30 Gy in three fractions, 50 Gy in five fractions, and 60 Gy in six fractions) have been compared in the SBRT treatment of liver metastases. The rates of complete and partial responses (at 6 and 12 months) were significantly higher in the 60 Gy group in comparison with the 50 Gy and 30 Gy groups. However, the local control rate at 12 months was only significantly different between the 60 Gy and 30 Gy groups. There was no difference in overall survival at 1 and 2 years.25 In France and Belgium, a dose of 45 Gy in three fractions is recommended currently for the treatment of colorectal liver metastases.10,17 In an effort to maximize effectiveness of SBRT and with respect to the fact that SBRT is well tolerated (side effects and toxicity see below), we prescribe a dose of 50–60 Gy in five fractions in our center.
Clinical outcomes and side effects
The effectiveness of CyberKnife therapy is measured by the rates of local control achieved; the main goal is to improve the time to progression and overall survival of patients. In general, excellent local control of liver metastases treated by CyberKnife has been reported. Local control rates range from 70%–100% at 1 year and from 60%–90% at 2 years.17,24–33 The differences between published studies depend on the tumor volume and histopathology, prior therapy, radiotherapy (RT) dose, and fractionation regimens that have been used. Table 1 shows an overview of the most pertinent studies focused on SBRT of liver metastases within the last 10 years (data regarding number of patients/number of lesions, tumor volume, RT dose, and clinical outcomes are presented).
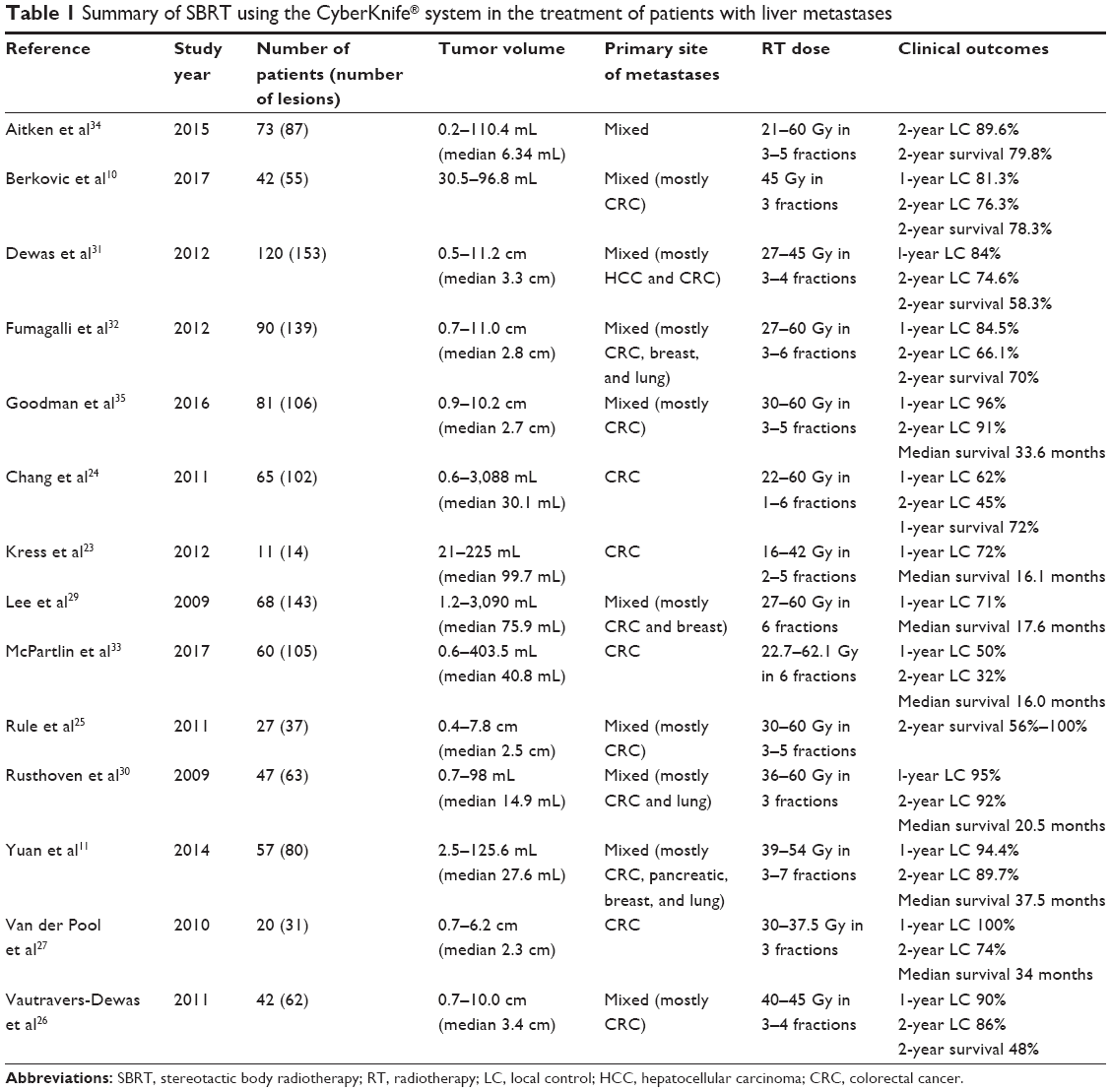 | Table 1 Summary of SBRT using the CyberKnife® system in the treatment of patients with liver metastases |
In 2012, Høyer et al9 reviewed the available evidence, and concluded that the median overall survival after CyberKnife® therapy ranges from 10–34 months; 2-year overall survival rates were reported in 30%–83% of patients, with occasional long-term survivors.27 Within the last years, clinical outcomes of liver metastases treated by CyberKnife® further improved due to increasing knowledge, technology enhancements, standard dose recommendations, and organ-at-risk constraints. The authors of the most recent studies report local control rates at 2 years of more than 76.3%; 1-year survival rates of more than 84.5% and 2-year survival rates of more than 72.3%.10,11,34,35
The prognostic factors that favor achievement of local control after CyberKnife® therapy are: tumor size ≤6 cm, ≤3 lesions, metachronous metastases, no prior chemotherapy, and non-colorectal liver metastases.17 The worst outcomes of colorectal metastases treated by the CyberKnife system are probably caused by the fact that most of these patients have been heavily pretreated with other local and systemic treatment modalities before being referred for CyberKnife®.9,17,36
In regard to the aforementioned data, SBRT seems to be more effective in the local ablation of liver metastases in comparison with RFA (local control rates after RFA range from 40%–96%). Moreover, there are many more technical limitations of RFA application.3,20,22,37 To the best of our knowledge, there is only one study focused on the comparison of SBRT and RFA. The local control rates at 1 and 2 years favored SBRT (85% vs 65% and 80% vs 61%, respectively), but the differences were not statistically significant. Local disease-free survival was significantly longer in patients treated with SBRT in comparison with RFA (34.4 months vs 6.0 months).37
SBRT of liver metastases is a very well-tolerated minimally invasive treatment modality. Acute side effects grade 1–2 (nausea, vomiting, abdominal pain, and peptic ulcers) are the most frequent side effects, which are encountered amongst 10%–30% of patients. Currently, nausea and vomiting are usually prevented by the prophylactic administration of antiemetics; peptic ulcers are prevented by proton pump inhibitors.8,9,17
Severe toxicity related to SBRT is uncommon – grade 3 side effects occur in less than 5% of cases: mostly elevated liver enzymes or gastroduodenal ulceration in patients with lesions situated close to the digestive structures.17 Radiation-induced liver disease (RILD) is an acute reaction occurring between 2 weeks and 4 months after radiotherapy in patients who received a dose of at least 30 Gy to the whole liver.9,38 Méndez Romero et al28 reported two cases of RILD after SBRT. However, no cases of RILS have been described in the vast majority of studies focused on SBRT of liver metastases.10,11,25,29,30 Very low RILD incidence is probably the consequence of extreme accuracy of radiation delivery on PTV during CyberKnife® therapy.
According to the outcomes of dose-escalation studies, toxicity did not differ, regardless of the prescribed dose during SBRT; no threshold dose has been defined yet. Toxicity is more likely to develop in patients receiving a high radiation dose to adjacent organs at risk or in patients receiving radiation to large volumes of the liver.
Oligometastatic disease
Despite excellent local control rates, out-of-field metastatic progression (out-of-field hepatic metastases and extrahepatic metastases) develops in a substantial proportion of patients after SBRT.8,9,39 Currently, the selection of patients for SBRT is based on clinical criteria only. Therefore, it seems essential to improve the selection of patients with liver metastases for SBRT.
It has been suggested that cancer progression has a multistep nature, with a state of oligometastases between the stages of purely localized and widely metastatic disease. The concept of oligometastatic disease was first introduced by Hellman and Weichselbaum40 in 1995. In an early stage of disease progression, tumors may have metastases limited in number and location because the tumors’ ability for metastatic growth has not been fully developed yet. If oligometastatic disease is eradicated using local ablative procedures, patients may be cured.39 This hypothesis has been supported by studies reporting that patients with oligometastatic disease after radical surgical resection have 5-year survival rates of 30%–50%.2,18,19
Acceptance of the oligometastatic disease paradigm requires the use of the most sophisticated diagnostic techniques in an effort to objectively categorize patients. Localized tumors, oligometastatic disease, and widely metastatic tumors are likely to require different strategies. The methods (biomarkers) that objectively and unequivocally identify patients with oligometastatic disease are needed.39,41 Subsequently, a group of oligometastatic patients could be offered a curative treatment such as radical surgical resection or CyberKnife therapy.
Conclusion
SBRT presents an effective minimally invasive treatment modality for patients with hepatic oligometastases who are not suitable candidates for radical liver resection. The CyberKnife® system allows for the delivery of high-dose radiation in a few fractions to the tumor with millimetric precision. The available data suggest that liver metastases can be treated by CyberKnife® therapy with very low toxicity and excellent local control rates ranging from 70%–100% at 1–2 years. In patients with oligometastatic disease, CyberKnife® therapy may lead to a complete remission and cure. The ability to identify patients at the oligometastatic stage of the disease presents the current challenge in oncology.
Disclosure
The authors report no conflicts of interest in this work.
References
Siegel R, Ward E, Brawley O, Jemal A, Cancer statistics, 2011: the impact of eliminating socioeconomic and racial disparities on premature deaths. CA Cancer J Clin. 2011;61(4):212–236. | ||
Choti MA, Sitzmann JV, Tiburi MF, et al. Trends in long-term survival following liver resection for hepatic colorectal metastases. Ann Surg. 2002;235(6):759–766. | ||
Khan K, Wale A, Brown G, Chau I. Colorectal cancer with liver metastases: neoadjuvant chemotherapy, surgical resection first of palliation alone? World J Gastroenterol. 2014;20(35):12391–12406. | ||
Grundmann RT. Current state of surgical treatment of liver metastases from colorectal cancer. World J Gastrointest Surg. 2011;3(12):183–196. | ||
Ihnát P, Ihnát Rudinská L, Zonča P. Radiofrequency energy in surgery: state of the art. Surg Today. 2014;44(6):985–991. | ||
Dieterich S, Gibbs IC. The CyberKnife in clinical use: current roles, future expectations. Front Radiat Ther Oncol. 2011;43:181–194. | ||
Ihnát P, Vávra P, Zonča P. Treatment strategies for colorectal carcinoma with synchronous liver metastases: which way to go? World J Gastroenterol. 2015;21(22):7014–7021. | ||
Tree AC, Khoo VS, Eeles RA, et al. Stereotactic body radiotherapy for oligometastases. Lancet Oncol. 2013;14(1):e28–e37. | ||
Høyer M, Swaminath A, Bydder S, et al. Radiotherapy for liver metastases: a review of evidence. Int J Radiat Oncol Biol Phys. 2012;82(3):1047–1057. | ||
Berkovic P, Gulyban A, Nguyen PV, et al. Stereotactic robotic body radiotherapy for patients with unresectable hepatic oligorecurrence. Clin Colorectal Cancer. 2017;16(4):349–357. | ||
Yuan ZY, Meng MB, Liu CL, et al. Stereotactic body radiation therapy using the CyberKnife(®) system for patients with liver metastases. Onco Targets Ther. 2014;7:915–923. | ||
Leksell L. The stereotaxic method and radiosurgery of the brain. Acta Chir Scand. 1951;102(4):316–319. | ||
Wowra B, Muacevic A, Tonn JC. CyberKnife radiosurgery for brain metastases. Prog Neurol Surg. 2012;25:201–209. | ||
Kato H, Yoshida H, Taniguch H, et al. Cyberknife treatment for advanced or terminal stage hepatocellular carcinoma. World J Gastroenterol. 2015;21(46):13101–13112. | ||
Potters L, Kavanagh B, Galvin JM, et al. American Society for Therapeutic Radiology and Oncology (ASTRO) and American College of Radiology (ACR) practice guideline for the performance of stereotactic body radiation therapy. Int J Radiat Oncol Biol Phys. 2010;76(2):326–332. | ||
Adler JR, Chang SD, Murphy MJ, Doty J, Geis P, Hancock SL. The Cyberknife: a frameless robotic system for radiosurgery. Stereotact Funct Neurosurg. 1997;69(1–4 Pt 2):124–128. | ||
Peiffert D, Baumann AS, Marchesi V. Treatment of hepatic metastases of colorectal cancer by robotic stereotactic radiation (Cyberknife®). J Visc Surg. 2014;151(Suppl 1):S45–S49. | ||
Lemke J, Cammerer G, Ganser J, et al. Survival and prognostic factors of colorectal liver metastases after surgical and nonsurgical treatment. Clin Colorectal Cancer. 2016;15(4):e183–e192. | ||
Kanas GP, Taylor A, Primrose JN, et al. Survival after liver resection in metastatic colorectal cancer: review and meta-analysis of prognostic factors. Clin Epidemiol. 2012;4:283–301. | ||
Pereira PL. Actual role of radiofrequency ablation of liver metastases. Eur Radiol. 2007;17(8):2062–2070. | ||
Nikfarjam M, Muralidharan V, Christophi C. Mechanisms of focal heat destruction of liver tumors. J Surg Res. 2005;127(2):208–223. | ||
Pawlik TM, Izzo F, Cohen DS, Morris JS, Curley SA. Combined resection and radiofrequency ablation for advanced hepatic malignancies: results in 172 patients. Ann Surg Oncol. 2003;10(9):1059–1069. | ||
Kress MS, Collins BT, Collins SP, Dritschilo A, Gagnon G, Unger K. Stereotactic body radiation therapy for liver metastases from colorectal cancer: analysis of safety, feasibility, and early outcomes. Front Oncol. 2012;2:8. | ||
Chang DT, Swaminath A, Kozak M, et al. Stereotactic body radiotherapy for colorectal liver metastases: a pooled analysis. Cancer. 2011;117(17):4060–4069. | ||
Rule W, Timmerman R, Tong L, et al. Phase I dose-escalation study of stereotactic body radiotherapy in patients with hepatic metastases. Ann Surg Oncol. 2011;18(4):1081–1087. | ||
Vautravers-Dewas C, Dewas S, Bonodeau F, et al. Image-guided robotic stereotactic body radiation therapy for liver metastases: is there a dose response relationship? Int J Radiat Oncol Biol Phys. 2011;81(3):e39–e47. | ||
van der Pool AE, Méndez Romero A, Wunderink W, et al. Stereotactic body radiation therapy for colorectal liver metastases. Br J Surg. 2010;97(3):377–382. | ||
Méndez Romero A, Wunderink W, Hussain SM, et al. Stereotactic body radiation therapy for primary and metastatic liver tumors: A single institution phase i-ii study. Acta Oncol. 2006;45(7):831–837. | ||
Lee MT, Kim JJ, Dinniwell R, et al. Phase I study of individualized stereotactic body radiotherapy of liver metastases. J Clin Oncol. 2009;27(10):1585–1591. | ||
Rusthoven KE, Kavanagh BD, Cardenes H, et al. Multi-institutional phase I/II trial of stereotactic body radiation therapy for liver metastases. J Clin Oncol. 2009;27(10):1572–1578. | ||
Dewas S, Bibault JE, Mirabel X, et al. Prognostic factors affecting local control of hepatic tumors treated by stereotactic body radiation therapy. Radiat Oncol. 2012;7:166. | ||
Fumagalli I, Bibault JE, Dewas S, et al. A single-institution study of stereotactic body radiotherapy for patients with unresectable visceral pulmonary or hepatic oligometastases. Radiat Oncol. 2012;7:164. | ||
McPartlin A, Swaminath A, Wang R, et al. Long-term outcomes of phase 1 and 2 studies of SBRT for hepatic colorectal metastases. Int J Radiat Oncol Biol Phys. 2017;99(2):388–395. | ||
Aitken K, Tree A, Thomas K, et al. Initial UK experience of stereotactic body radiotherapy for extracranial oligometastases: can we change the therapeutic paradigm? Clin Oncol. 2015;27(7):411–419. | ||
Goodman BD, Mannina EM, Althouse SK, Maluccio MA, Cárdenes HR. Long-term safety and efficacy of stereotactic body radiation therapy for hepatic oligometastases. Pract Radiat Oncol. 2016;6(2):86–95. | ||
Milano MT, Katz AW, Schell MC, Philip A, Okunieff P. Descriptive analysis of oligometastatic lesions treated with curative-intent stereotactic body radiotherapy. Int J Radiat Oncol Biol Phys. 2008;72(5):1516–1522. | ||
Stintzing S, Grothe A, Hendrich S, et al. Percutaneous radiofrequency ablation (RFA) or robotic radiosurgery (RRS) for salvage treatment of colorectal liver metastases. Acta Oncol. 2013;52(5):971–977. | ||
Hoyer M, Roed H, Traberg Hansen A, et al. Phase II study on stereotactic body radiotherapy of colorectal metastases. Acta Oncol. 2006;45(7):823–830. | ||
Palacios-Eito A, Garcia-Cabezas S. Oligometastatic disease, the curative challenge in radiation oncology. World J Clin Oncol. 2015;6(4):30–34. | ||
Hellman S, Weichselbaum RR. Oligometastases. J Clin Oncol. 1995;13(1):8–10. | ||
Niibe Y, Hayakawa K. Oligometastases and oligo-recurrence: the new era of cancer therapy. Jpn J Clin Oncol. 2010;40(2):107–111. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.