Back to Archived Journals » Reports in Medical Imaging » Volume 11
Stereology volume analysis to evaluate teeth’s root using CBCT images
Authors Fadili A, Halimi A, Benyahia H, Zaoui F
Received 3 October 2017
Accepted for publication 27 December 2017
Published 9 November 2018 Volume 2018:11 Pages 31—39
DOI https://doi.org/10.2147/RMI.S153169
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Tarik Massoud
Ahmed Fadili, Abdelali Halimi, Hicham Benyahia, Fatima Zaoui
Department of Orthodontics and Dentofacial Orthopedics, Faculty of Dental Medicine, Mohammed V University, Rabat, Morocco
Purpose: The purpose of the present study was to evaluate a semiautomated segmentation tool designated for the volume measurements of teeth root; this method is based on three-dimensional and focused to follow-up the root’s volume when an orthodontic treatment occurred.
Materials and methods: In order to evaluate a semiautomated segmentation tool, a cone beam computed tomography (CBCT) was selected with 20 intact teeth (10 maxillary and 10 mandibular teeth), CBCT images were imported into the ImageJ software, and the root volumes were measured using two methods (the semiautomated segmentation and the manual segmentation). Both segmentations are carried out by two experts; the manual segmentation served as a reference method and considered as the “gold standard”. The data were analyzed using the Bland–Altman analysis to compare the agreement between methods, and the intraclass correlation coefficient (ICC) was used to assess the interobserver reliability.
Results: The Bland–Altman analysis revealed the agreement between measurements on semiautomated segmentation and manual segmentation, with a mean bias of –2.09 mm3 and the 95% limits of agreement of –11.38 to 7.21 mm3. The ICC was 0.999 for semiautomated segmentation method and 0.999 for manual segmentation method.
Conclusion: The use of stereology employing the ImageJ software and CBCT images provide an accurate and reliable semiautomated segmentation, leading to an approach of volume quantitative analysis to evaluate and follow-up the root’s volume when orthodontic treatment occurred. Further clinical studies are necessary to explore this method.
Keywords: three-dimensional imaging, segmentation, accuracy, orthodontic treatment, ImageJ software, root resorption
Introduction
Root resorption occurs when the periodontal ligament on the root surface is either damaged or removed. It is well recognized from the orthodontic literature that apical root resorption can be seen after orthodontic treatment. It has been recommended that follow-up radiographs should be obtained after 6 months treatment with fixed appliance.1 Root resorption combined with orthodontic treatment is a complex and multifactorial phenomenon that most likely results from individual physiological and genetic risk factors.2–12
Two-dimensional imaging techniques are not satisfactory in quantitative evaluation because of lack of information in the three-dimensional space.13 It has been concluded that volumetric measurement of teeth using cone beam computed tomography (CBCT) is a reliable, reproducible, and valid method.14–16 Therefore, an accurate detection and accurate evaluation of root resorption is crucial for monitoring and follow-up an appropriate orthodontic treatment. Many studies are conducted about root resorption employing methods based on 2D images such as panoramic, periapical, and lateral cephalographic radiographs. However, compared to CBCT images, 2D images present some limitations, such as the superimposition and lack of definition of the anatomical structures.17
Although paralleling techniques can diminish projection and procedural errors, ideal film, X-ray tube, and head orientations can still be difficult to achieve, leading to image distortions.18 Previous studies have demonstrated that conventional radiographic techniques are inadequate for a consistent accurate diagnosis of root resorption.19
CBCT has made it possible to overcome these limitations and provides anatomically accurate three-dimensional images, Moreover, compared to multislice computerized tomography, CBCT images are considered as a noninvasive method, with low cost, conferring secure radiation and easy accessibility. There are many dental radiation dosimetry studies in the literature comparing traditional 2D dental radiographs and CBCT. Effective dose of a 2D panoramic radiograph ranges from 0.004 to 0.030 mSv (4.0–30 μSv); a full mouth radiographic series utilizing D speed film and round collimation produces an effective dose level between 0.0349 and 0.388 mSv (34.9–388 μSv).20 Using Monte Carlo simulations and the International Commission on Radiological Protection, effective doses (in an i-CAT CBCT) were calculated and were in the range of 25–66 and 46 μSv for full head.21
Therefore, for the doses that approximating the conventional 2D radiology, CBCT tends to become the diagnostic standard to use routinely and allow better visualization. The aim of this study was to evaluate a semiautomated segmentation tool designated for the volume measurements of teeth root; the measurements of the accuracy, agreement, and reliability were performed in comparison with the manual segmentation; this method will be suitable for a perspective to measure volume root at different time points when orthodontic treatments occurred.
Materials and methods
In this study, we used two segmentation methods to assess the root’s volume that allows us to follow-up and quantify any changes in root’s volume, which can be useful for further studies focusing on root’s volume measurements.
In this study, we used CBCT images of an anonymous patient of which teeth criteria are defined as follows: 20 undamaged roots’ structure (10 maxillary [two central incisors, two lateral incisors, two canines, two first premolars, and two second premolars] and 10 mandibular teeth [two central incisors, two lateral incisors, two canines, two first premolars, and two second premolars]), ordinary shape, without any orthodontic treatment, and without any artifacts. CBCT images were taken with Sirona, SIDEXIS study, resolution 6,250 pixels/mm, at 85 kV, 5 mA, voxel size 0.16×0.16×0.16 mm3, and slice thickness 0.16 mm. The images were generated in the DICOM format and imported into the ImageJ software (v 1.50 Java 1.6.0_20 64 bits),22 and the volume measurements were based on two kinds of segmentation, which integrated into ImageJ platform tools.
Ethics and informed consent
As CBCT data were anonymously available and collected from an earlier research study, ethics approval and written informed consent were not required for this study.
Segmentation
To assess the volume of teeth root; the segmentations were performed by two observers who use Segmentation Editor procedure developed by Johannes Schindelin, Francois Kusztos, and Benjamin Schmid (http://132.187.25.13/home/?category=Download&page=SegmentationEditor).
Two different segmentation methods were used to assess the root volumes after importing the DICOM files. The Segmentation Editor was already applied on Virtual Insect Brain by the authors cited earlier. In our study, we focus on the application of Segmentation Editor on human skull using CBCT images.
Manual segmentation
The manual segmentation was performed using a polygon selection tool that creates irregularly shaped selections defined by a series of line segments, and polygon selection was developed in-house with ImageJ (Figure 1), and we use duplication segmentation and manual adjustment to refine and save time. Polygon selection tool is included with ImageJ.
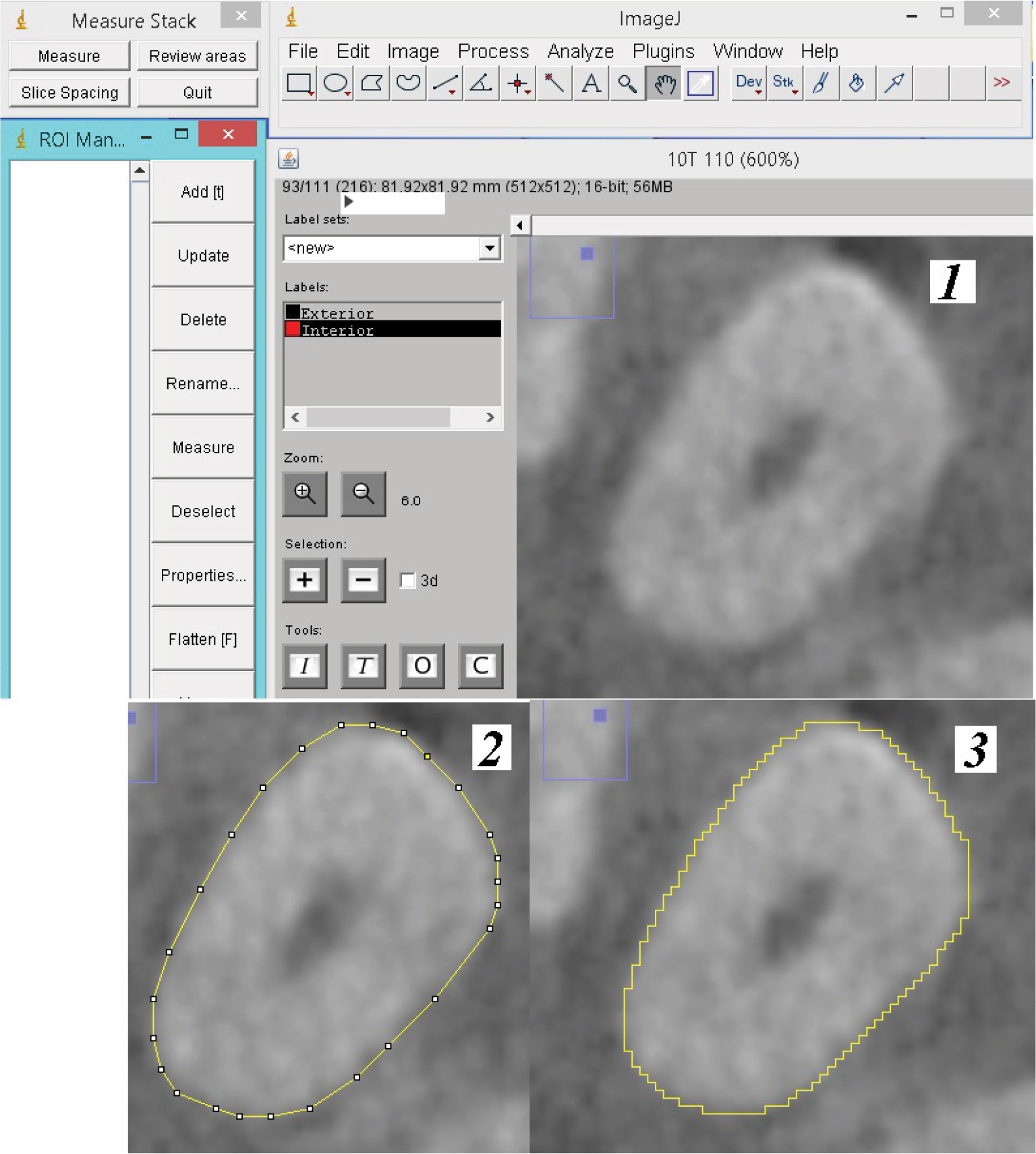 | Figure 1 Steps followed to create ROI of root tooth employing manual segmentation on axial slice. Notes: (1) Original image (2) drawing up the ROI manually (3) Execution of the manual segmentation to delimit ROI. Abbreviation: ROI, region of interest. |
Semiautomated segmentation
We used the Brush Selection tool to draw an outline around the region of interest (ROI), we use the threshold (T button) to refine the selected area based on a locally adjusted threshold, using O (open) and C (close) buttons, which apply the corresponding morphological kernels to selection for smoothing the outline. The ROI exists on a range of consecutive slices. The observers create the ROI on key slices (Figure 2). The plugin interpolates the ROI for the slices in between the key slices to be faster and save time. Linear interpolation is used.
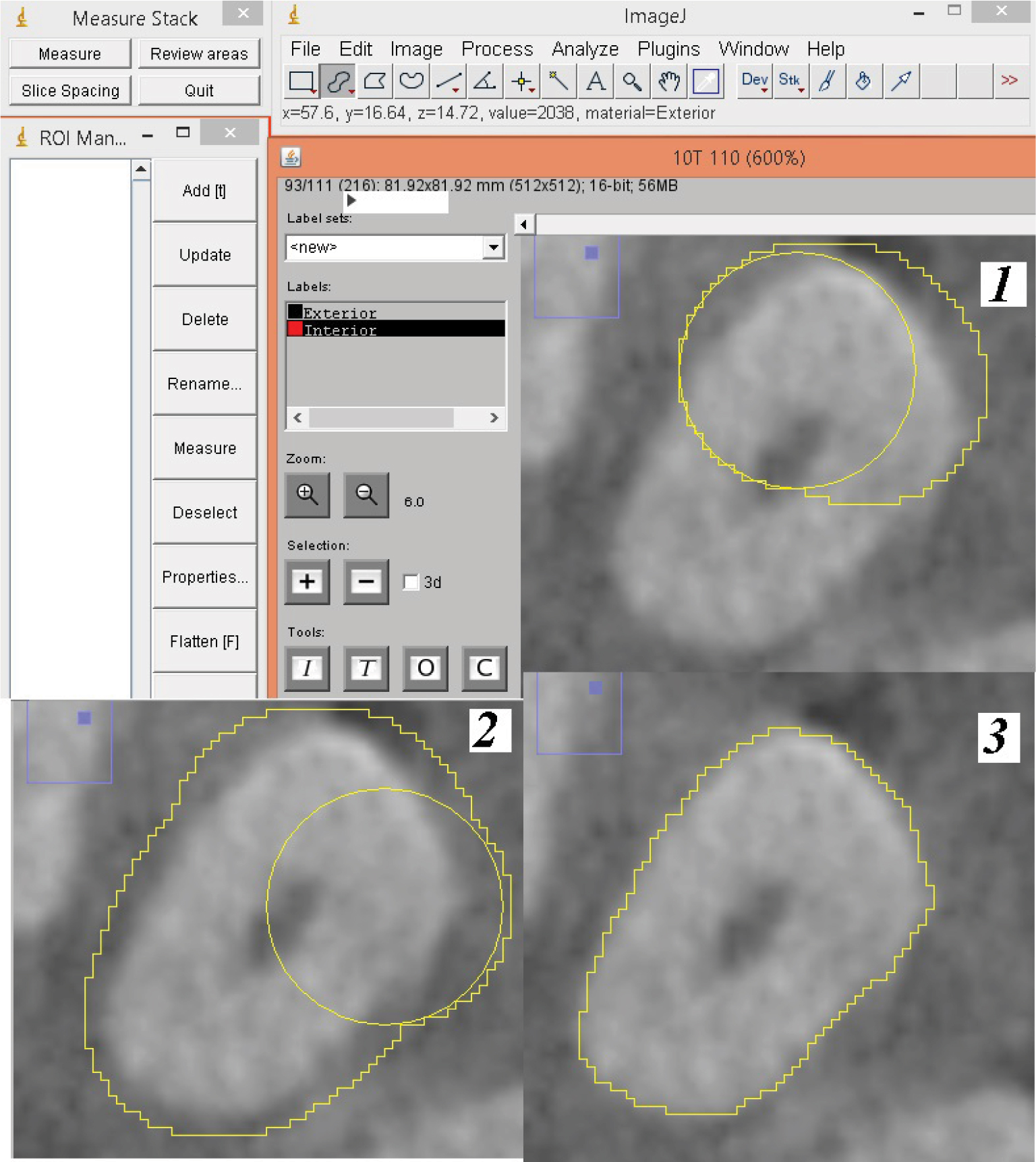 | Figure 2 Steps followed to create ROI of root tooth employing semiautomated segmentation on axial slice. (1) Original image (2) Drawing up the ROI using Brush Selection (3) Execution of the semiautomated to delimit ROI. Abbreviation: ROI, region of interest. |
Calculation of teeth roots volumes
Downloading ImageJ
ImageJ (v 1.50 java 1.6.0_20 64 bits) is a multiplatform software, open source, image processing and analysis developed by the National Institutes of Health (http://rsb.info.nih.gov/ij/download.html).
Calculating volume
Both for manual and semiautomated segmentations, stereological volume measurements were performed using the Measure Stack, Reference Software Version 0, December 6, 2002, which was developed by B Dougherty (http://www.optinav.com/MeasureStack.htm). Figure 3 displays schematic illustrations of reference planes and line used in this study to define slices between apex and cementoenamel junction (CEJ).
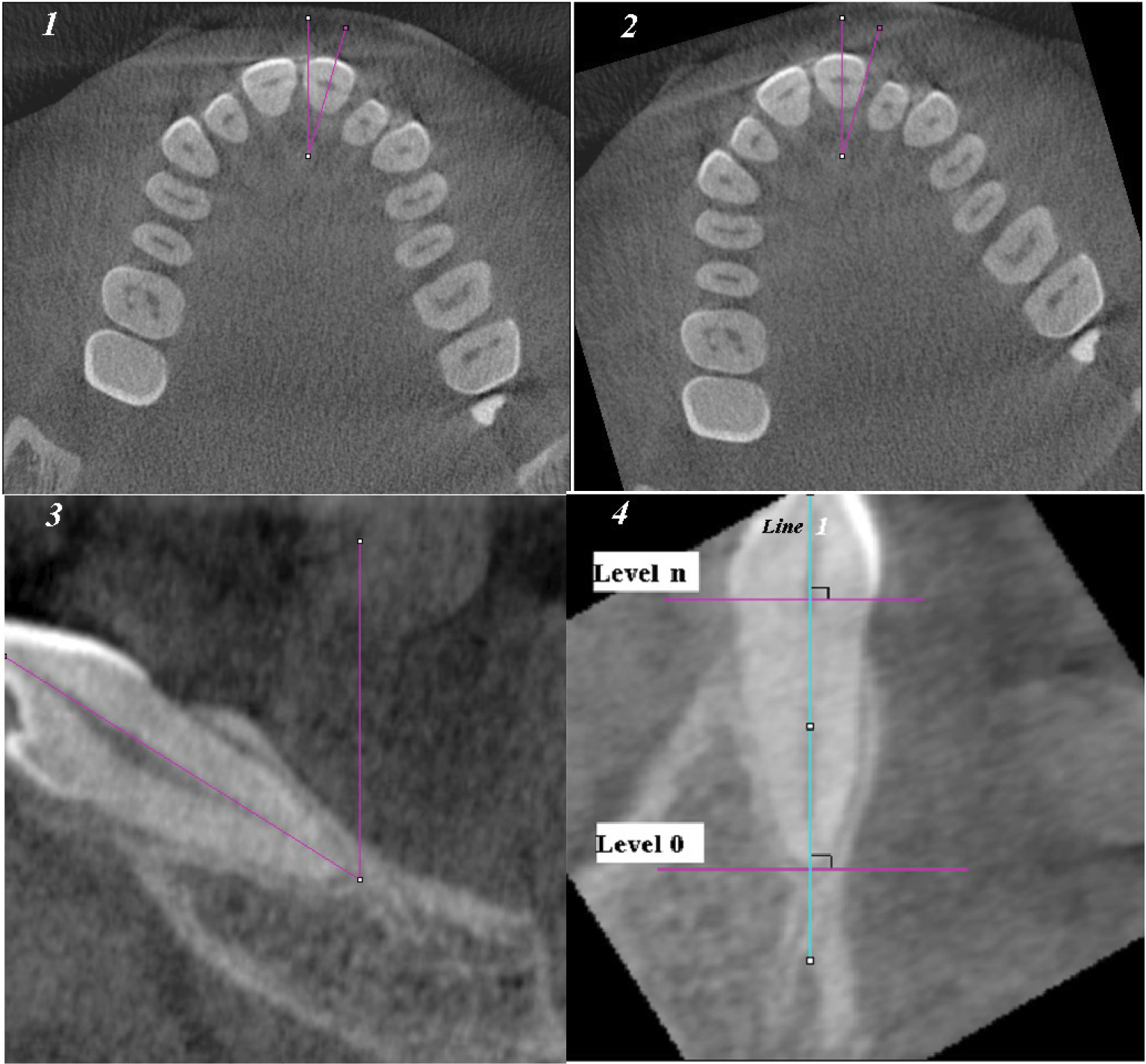 | Figure 3 Schematic illustrations of reference planes and line used in this study to define slices between apex and CEJ: (Line 1) root axis, (Level 0) perpendicular plane to root axis on the root, apex (Level n) perpendicular plane to root axis on the CEJ. Notes: (1) measuring the angle between the sagittal plane and the plane crossing the middle of tooth, (2) rotation with the angle measured in the way to superimpose the plane crossing middle tooth with sagittal plane, (3) reslice and rotation with 90° starting at left, (4) by this way we can easily define axial slices between apex and CEJ. Abbreviation: CEJ, cementoenamel junction. |
The following steps were followed to define accurate slices between Level 0 and Level n: 1) we handle angle tool to measure the angle between the sagittal plane and the plane crossing the middle of tooth as shown in this image, 2) rotation with the angle measured in the way to superimpose the plane crossing middle tooth with sagittal plane, 3) reslice and rotation with 90° starting at left, and 4) by this way, we can easily define slices between apex and CEJ Figure 3.
Visualization
The ImageJ 3D Viewer plugin (Volume_Viewer) is included with ImageJ in the (ImageJ/plugins/3D) folder, developed by Kai Uwe Barthel: (http://rsb.info.nih.gov/ij/plugins/volume-viewer.html/), and the 3D Viewer uses Java 3D to provide hardware-accelerated 3D visualization of image stacks as volumes, surfaces, and orthogonal view (Figures 4 and 5).
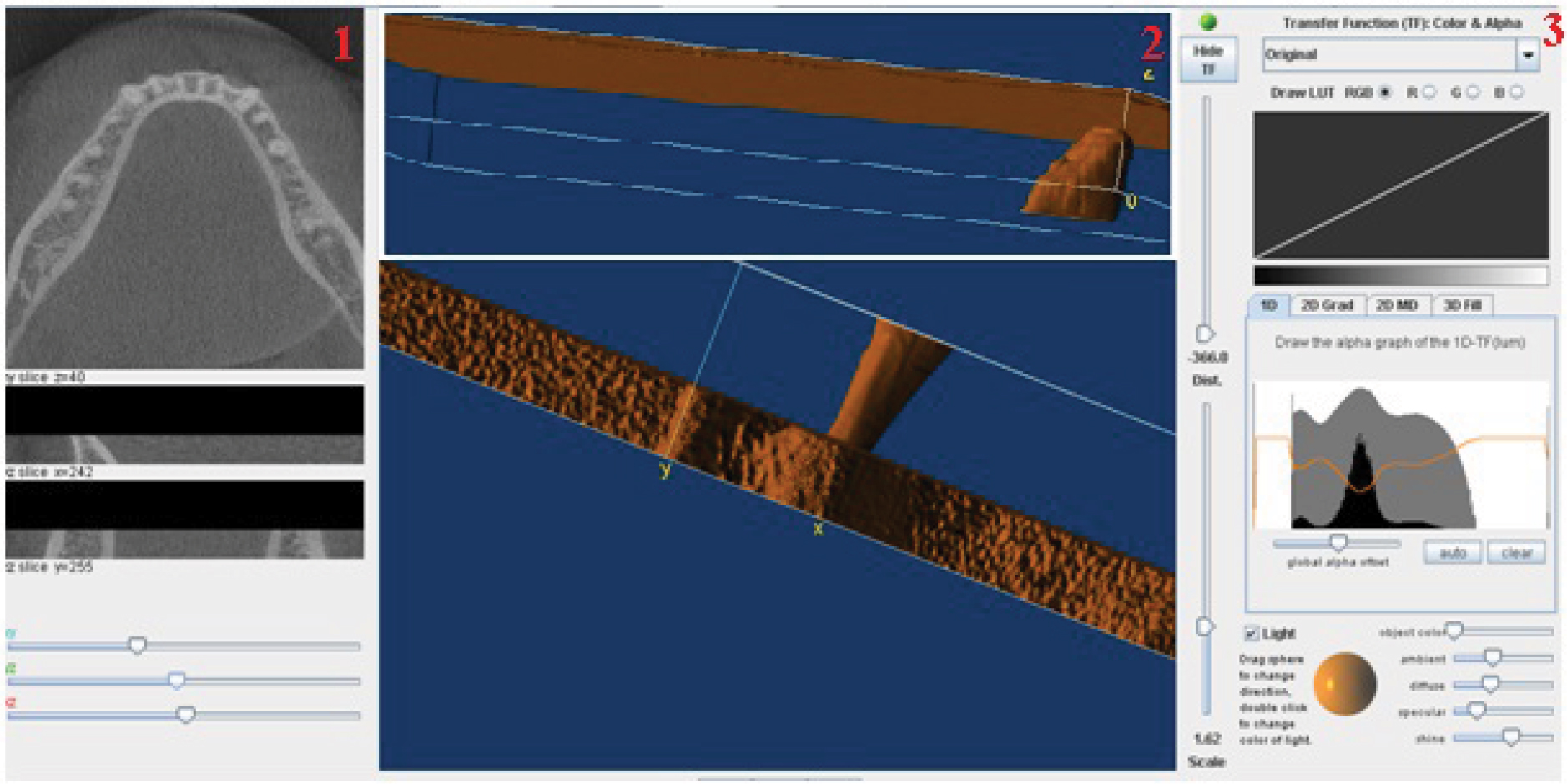 | Figure 4 Screenshot of 3D reconstruction: (1) orthogonal view, (2) surface visualizations of the root and crown mandibular, and (3) input parameters used for visualization. |
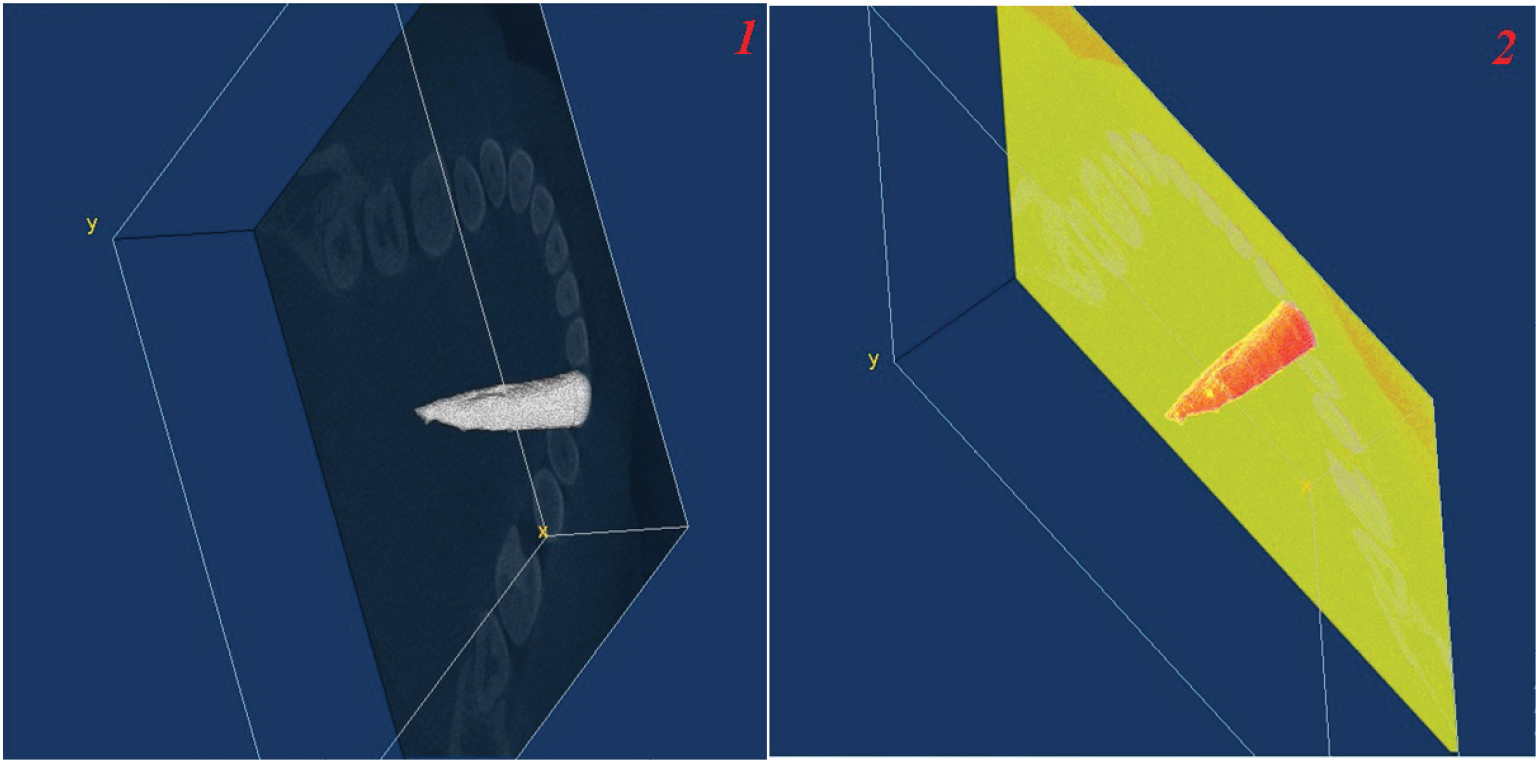 | Figure 5 Screenshot of 3D visualization: (1) using original parameters and (2) using spectrum LUT parameters. Abbreviation: LUT, lookup table. |
Statistics
The volume measurements were compared between the manual segmentation and semiautomated segmentation, and all the data were tested for normality using the Shapiro–Wilk test. The data were analyzed using Bland–Altman analysis to compare the agreement between methods, and the intraclass correlation coefficient was used to assess interobserver reliability. All statistical calculations were done using the computer programs Microsoft Excel 2013 (Microsoft Corporation, Redmond, WA, USA) and SPSS software (Version 21; IBM Corporation, Armonk, NY, USA).
Results
The results of the root’s volume measured by the stereology method using the semiautomated segmentation and the manual segmentation were carried out by two observers are shown in Table 1. Interobserver reliability is presented as intraclass correlation coefficient (ICC) for the manual segmentation and semiautomated segmentation measurements. Interobserver reliability is considered high when ICC is more or equal to ≥0.90. in our case ICC=0.999; these results suggest that the methods are not examiner dependent (Tables 2 and 3).
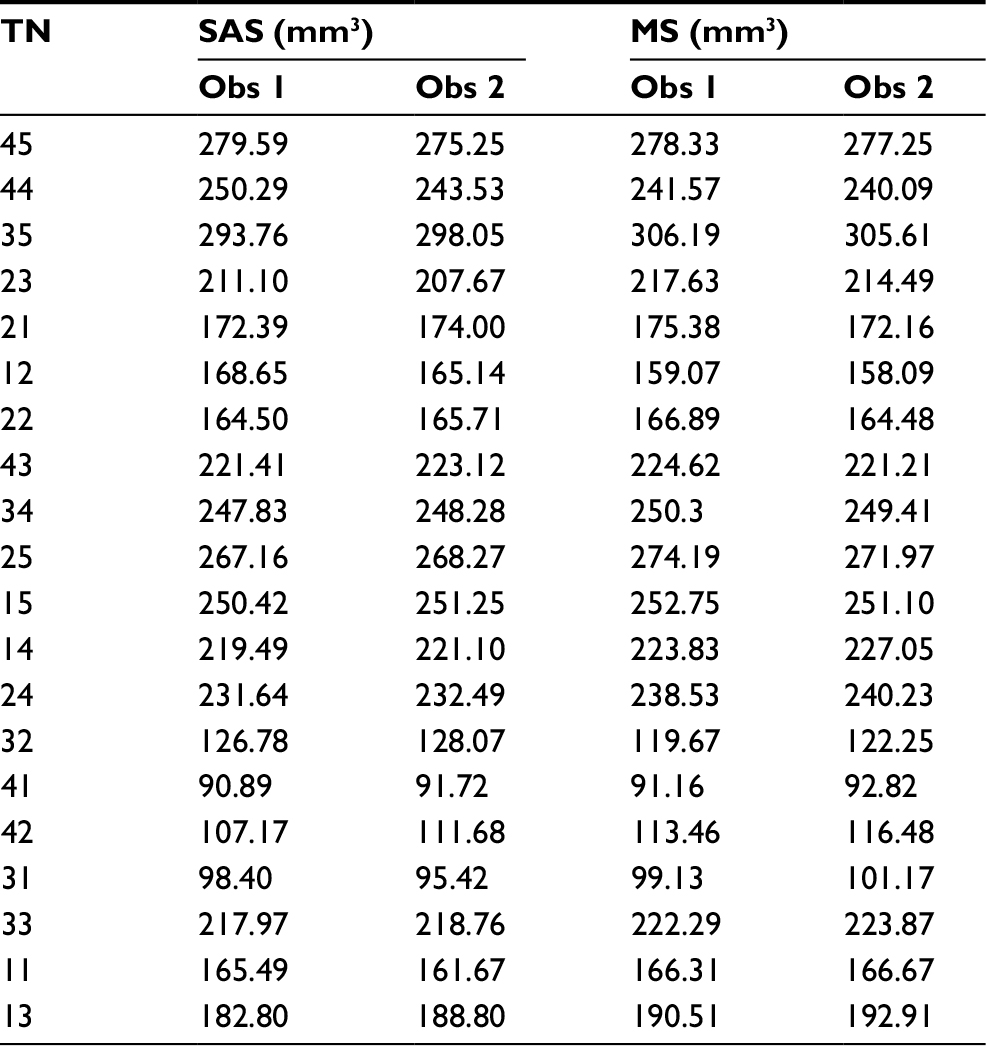 | Table 1 The root’s volume measurements assessed using two methods and carried out by two observers Note: TN, TN according to the FDI numbering system. Abbreviations: MS, manual segmentation; Obs, observer; SAS, semiautomated segmentation; TN, teeth numbered. |
 | Table 2 Comparison measurements made between observer 1 and observer 2 using semiautomated segmentation Abbreviation: ICC, intraclass correlation coefficient. |
 | Table 3 Comparison measurements made between observer 1 and observer 2 using manual segmentation Abbreviation: ICC, intraclass correlation coefficient. |
The dental pulp chamber and canals were included in the volume measurements with either manual segmentation or semiautomated segmentation of the root’s volume. Surface visualizations are generated (Figures 4 and 5); we can also use orthogonal view visualization. The mean time of one root required for measurement by stereology using the semiautomated segmentation was 175.8 seconds, and that using the manual segmentation was 1,810.4 seconds.
Discussion
In this article, we describe a semiautomated approach using CBCT images and ImageJ software to assess the volumes of the teeth roots. 1) The semiautomated approach is able to segment thoroughly teeth’s root and 2) provide 3D visualization by means 3D viewer plugin. 3) This approach provides interpolation between slices and detects the margins for saving time. 4) The measurement of the teeth roots will be useful for any perspective that focuses to evaluate root resorption after orthodontic treatment for a large specimen size of scans. In addition, the user can visually check the segmentation performance using 3D surface representations and orthogonal view visualization. Ahlowalia et al23 created the cavities in the bone bovine while varying shapes and sizes simulating periapical pathosis, and then, the physical volume of the cavities was determined by using the silicone impression of Aquasil™; this method involves weighing the impression and dividing the mass of each sample by the known density of Aquasil™. Ahlowalia et al23 concluded that CBCT may provide a valuable tool for monitoring the healing rate of apical periodontitis.
The results of Ponder et al24 demonstrated that, compared with measurements from microCT images, high-resolution CBCT scans can be used for an accurate volumetric quantifications of simulated lateral and apical root resorption defects than do low-resolution scans and both high- and low-resolution CBCT scans can also be used to more accurately measure external apical root resorption defects than periapical radiographs. Manual segmentation analysis is a better alternative but is very labor intensive and taking considerable time. A semiautomated method for CBCT images has several advantages over manual analysis; the risk of nonobjectivity and interobserver variability is greatly reduced by minimizing the active manual input of the user. Semiautomated approach can be purely objective and handle every dataset in exactly the same manner. Additionally, a semiautomated analysis method is much faster than any manual procedure. Thus, by the semiautomated method, the analysis of larger number of scans can be evaluated compared to a manual segmentation. To enable the researcher to check every step along the way, the semiautomated method generates visualizations of the segmented volume. These visualizations can be evaluated after the analysis is complete. The Bland–Altman analysis revealed the agreement between measurements on semiautomated segmentation and manual segmentation, with a mean bias of –2.09 mm3 and the 95% limits of agreement of –11.38 to 7.21 mm3 (Figure 6). Further clinical studies are necessary to explore this method with predefined clinical margin. Interobserver reliability is presented as ICC showing that both the manual and the software methods (using DICOM images of CBCT) were high for all measurements, as indicated by ICC (≥0.90); these results suggest that the methods are not examiner dependent. Manual analysis to evaluate apical root resorption panoramic and lateral cephalometric radiographs can be used before and after orthodontic treatment, based on 2D measurement where the length from the incisal edge to the root apex was calculated.25 However, as the apical resorption occurred in different directions around the root, 3D measurement will be more relevant to evaluate root resorption. In addition, when orthodontic treatment was performed, CBCT is a powerful tool to detect apical root resorption compared with panoramic radiography and a useful tool to put it in use when determining whether to continue or modify orthodontic treatment.26 The presented segmentation method is not restricted to the mandibular and maxillary teeth but can be applied to any bone, or any tooth’s root. It was reliable for 2D and 3D segmentations of cells and cell nuclei useful for the segmentation and visualization of a neuron in the housefly’s visual system.27,28 However, when we use the semiautomated method or manual method, may be some slices will not well segmented where the interpolation was performed; in this case, 3D visualization will show irregularity of the volume constructed in the 3D viewer and we can remedy this mistake by rectifying and refining the segmentation (on the slice affected). In our study, we excluded all source artifacts such as rolling (caused by involuntary movements) considered as the type of movement that most severely affects the image diagnostic value.29 We excluded the artifacts caused by root canal fillings that affected the accuracy assessment30 and also excluded all sorts of metal artifacts for the reason that the CBCT user has very limited possibilities to reduce metal artifacts by the lack of algorithms implementing metal artifact reduction.31 A few studies were conducted about volumetric root resorption; The segmentation and volumetric measurement of teeth were carried out using the Mimics software V 16.0 (Materialise NV, Leuven, Belgium) after rapid maxillary expansion between tooth-borne and tissue-borne appliances using CBCT, which was considered as the most relevant; tooth volume loss and its percentage were measured.32 The percentage of root volume loss was calculated by subtracting the postexpansion root volume from the pre-expansion volume. However, the segmentation and volumetric measurement of all teeth (root and crown) were measured.32 In our study to calculate the root’s volume, we used the CEJ as a reference to separate root (as ROI) from tooth crown. Our study is based on a previously published approach related to the assessment of the volume-of-interest accuracy using CBCT.33 Our study offers promising prospects for assessments of all kinds of teeth roots, and we used two segmentation methods allowing us to follow-up and quantify any change in the root’s volume occurred when orthodontic treatment performed. Therefore, we eliminate the effects of artifacts induced by discrepancies between the mathematical modeling and the actual physical imaging process.34 This method will be useful for any perspective that focuses to evaluate root resorption after orthodontic treatment for a large specimen size of scans.
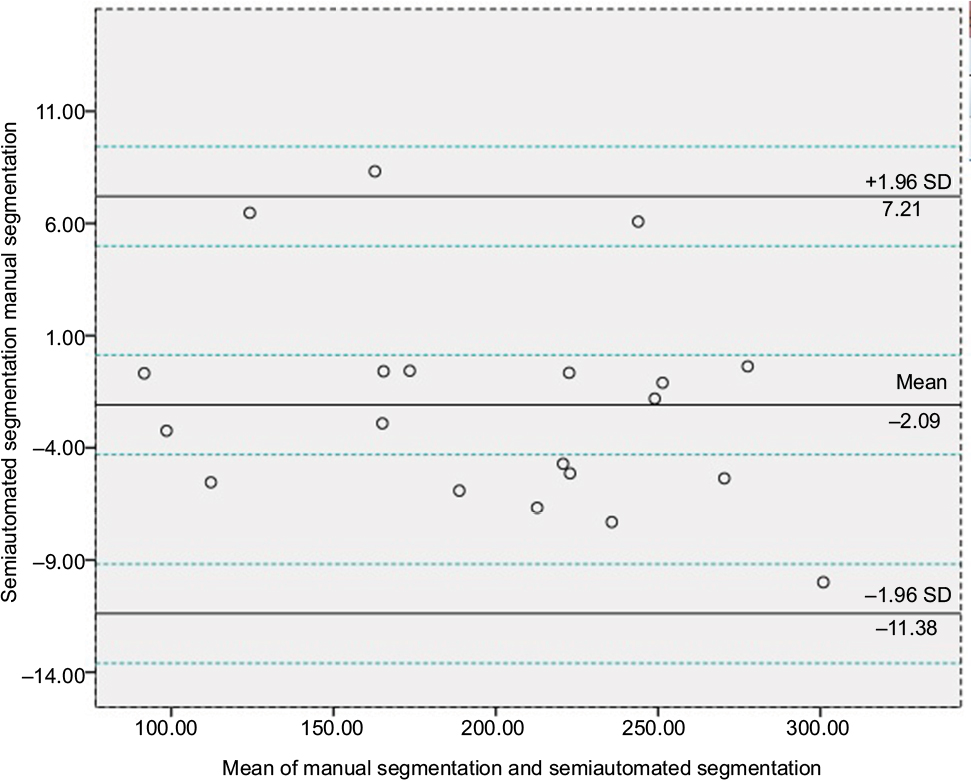 | Figure 6 Bland and Altman plot with the representation of the limits of agreement from –1.96 to +1.96 seconds and representation of CI limits for mean and agreement limits (between the blue dotted lines). |
Conclusion
The use of stereology employing the ImageJ software (on a personal computer) and CBCT images provide an accurate and reliable semiautomated approach for volume quantitative analysis leading to evaluate and follow-up the root’s volume when any orthodontic treatment occurred; it provides a valuable tool for research monitoring and provides a good 3D visualization with less complexity.
Disclosure
The authors report no conflicts of interest in this work.
References
Levander E, Malmgren O, Eliasson S. Evaluation of root resorption in relation to two orthodontic treatment regimes. A clinical experimental study. Eur J Orthod. 1994;16(3):223–228. | ||
Linge L, Linge BO. Patient characteristics and treatment variables associated with apical root resorption during orthodontic treatment. Am J Orthod Dentofacial Orthop. 1991;99(1):35–43. | ||
Weiland F. Constant versus dissipating forces in orthodontics: the effect on initial tooth movement and root resorption. Eur J Orthod. 2003;25(4):335–342. | ||
Gonzales C, Hotokezaka H, Yoshimatsu M, Yozgatian JH, Darendeliler MA, Yoshida N. Force magnitude and duration effects on amount of tooth movement and root resorption in the rat molar. Angle Orthod. 2008;78(3):502–509. | ||
Ren Y, Maltha JC, Liem RS, Stokroos I, Kuijpers-Jagtman AM. Age-dependent external root resorption during tooth movement in rats. Acta Odontol Scand. 2008;66(2):93–98. | ||
Al-Qawasmi RA, Hartsfield JK, Everett ET, et al. Root resorption associated with orthodontic force in inbred mice: genetic contributions. Eur J Orthod. 2006;28(1):13–19. | ||
Al-Qawasmi RA, Hartsfield JK, Everett ET, et al. Genetic predisposition to external apical root resorption. Am J Orthod Dentofacial Orthop. 2003;123(3):242–252. | ||
Nishioka M, Ioi H, Nakata S, Nakasima A, Counts A. Root resorption and immune system factors in the Japanese. Angle Orthod. 2006;76(1):103–108. | ||
Mcnab S, Battistutta D, Taverne A, Symons AL. External apical root resorption of posterior teeth in asthmatics after orthodontic treatment. Am J Orthod Dentofacial Orthop. 1999;116(5):545–551. | ||
Parker RJ, Harris EF. Directions of orthodontic tooth movements associated with external apical root resorption of the maxillary central incisor. Am J Orthod Dentofacial Orthop. 1998;114(6):677–683. | ||
Sameshima GT, Sinclair PM. Predicting and preventing root resorption: Part I. Diagnostic factors. Am J Orthod Dentofacial Orthop. 2001;119(5):505–510. | ||
Sameshima GT, Sinclair PM. Predicting and preventing root resorption: Part II. Treatment factors. Am J Orthod Dentofacial Orthop. 2001;119(5):511–515. | ||
Chan EK, Darendeliler MA. Exploring the third dimension in root resorption. Orthod Craniofac Res. 2004;7(2):64–70. | ||
Ye N, Jian F, Lai W. Effect of voxel size and partial volume effect on accuracy of tooth volumetric measurements with cone beam CT. Dentomaxillofac Radiol. 20132013;42(5):0070. | ||
Wang Y, He S, Yu L, Li J, Chen S. Accuracy of volumetric measurement of teeth in vivo based on cone beam computer tomography. Orthod Craniofac Res. 2011;14(4):206–212. | ||
Li W, Chen F, Zhang F, et al. Volumetric measurement of root resorption following molar mini-screw implant intrusion using cone beam computed tomography. PLoS One. 2013;8(4):e60962. | ||
Reddy MS. Radiographic methods in the evaluation of periodontal therapy. J Periodontol. 1992;63(12s):1078–1084. | ||
Brezniak N, Goren S, Zoizner R, et al. A comparison of three methods to accurately measure root length. Angle Orthod. 2004;74(6):786–791. | ||
Sameshima GT, Asgarifar KO. Assessment of root resorption and root shape: periapical vs panoramic films. Angle Orthod. 2001;71(3):185–189. | ||
Lee CY, Koval TM, Suzuki JB. Low-dose radiation risks of computerized tomography and cone beam computerized tomography: reducing the fear and controversy. J Oral Implantol. 2015;41(5):e223–e230. | ||
Morant JJ, Salvadó M, Hernández-Girón I, Casanovas R, Ortega R, Calzado A. Dosimetry of a cone beam CT device for oral and maxillofacial radiology using Monte Carlo techniques and ICRP adult reference computational phantoms. Dentomaxillofac Radiol. 2013;42(3):92555893. | ||
Farman AG. Applying DICOM to dentistry. J Digit Imaging. 2005;18(1):23–27. | ||
Ahlowalia MS, Patel S, Anwar HM, et al. Accuracy of CBCT for volumetric measurement of simulated periapical lesions. Int Endod J. 2013;46(6):538–546. | ||
Ponder SN, Benavides E, Kapila S, Hatch NE. Quantification of external root resorption by low- vs high-resolution cone-beam computed tomography and periapical radiography: A volumetric and linear analysis. Am J Orthod Dentofacial Orthop. 2013;143(1):77–91. | ||
Savoldi F, Bonetti S, Dalessandri D, Mandelli G, Paganelli C. Incisal Apical Root Resorption Evaluation after Low-Friction Orthodontic Treatment Using Two-Dimensional Radiographic Imaging and Trigonometric Correction. J Clin Diagn Res. 2015;9(11):ZC70–ZC74. | ||
Dudic A, Giannopoulou C, Leuzinger M, Kiliaridis S. Detection of apical root resorption after orthodontic treatment by using panoramic radiography and cone-beam computed tomography of super-high resolution. Am J Orthod Dentofacial Orthop. 2009;135(4):434–437. | ||
Nandy K, Kim J, Mccullough DP, et al. Segmentation and quantitative analysis of individual cells in developmental tissues. Methods Mol Biol. 2013;1092:235–253. | ||
Anderson JR, Barrett SF, Wilcox MJ. The segmentation and visualization of a neuron in the housefly’s visual system. Biomed Sci Instrum. 2005;41:235–240. | ||
Nardi C, Molteni R, Lorini C, et al. Motion artefacts in cone beam CT: an in vitro study about the effects on the images. Br J Radiol. 2016;89(1058):20150687. | ||
Camilo CC, Brito-Júnior M, Faria-E-Silva AL, et al. Artefacts in Cone Beam CT Mimicking an Extrapalatal Canal of Root-Filled Maxillary Molar. Case Rep Dent. 2013;2013:1–5. | ||
Pauwels R, Stamatakis H, Bosmans H, et al. Quantification of metal artifacts on cone beam computed tomography images. Clin Oral Implants Res. 2013;24 Suppl A100:94–99. | ||
Dindaroğlu F, Doğan S. Evaluation and comparison of root resorption between tooth-borne and tooth-tissue borne rapid maxillary expansion appliances: A CBCT study. Angle Orthod. 2016;86(1):46–52. | ||
Fadili A, Alehyane N, Halimi A, Zaoui F. An Alternative Approach to Assessing Volume-of-Interest Accuracy Using CBCT and ImageJ Software: In Vitro Study. Adv Radiol. 2015;2015(11):1–5. | ||
Schulze R, Heil U, Gross D, et al. Artefacts in CBCT: a review. Dentomaxillofac Radiol. 2011;40(5):265–273. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.