Back to Journals » International Medical Case Reports Journal » Volume 18
Stem Cell Transplantation for Ovarian Cancer Patient with Associated Myelodysplasia After Maintenance Therapy with Olaparib: A Case Report
Authors Linn Z ![]() , Gu Z, Wang L, Cai S
, Gu Z, Wang L, Cai S
Received 1 September 2024
Accepted for publication 24 January 2025
Published 11 February 2025 Volume 2025:18 Pages 241—248
DOI https://doi.org/10.2147/IMCRJ.S491062
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Zeyar Linn,1 Zhongyi Gu,1 Libing Wang,2 Shengyun Cai1
1Department of Obstetrics and Gynecology, The First Affiliated Hospital of Naval Medical University (Changhai Hospital), Naval Medical University, Shanghai, People’s Republic of China; 2Department of Hematology, The First Affiliated Hospital of Naval Medical University (Changhai Hospital), Naval Medical University, Shanghai, People’s Republic of China
Correspondence: Shengyun Cai, Department of Obstetrics and Gynecology, The First Affiliated Hospital of Naval Medical University (Changhai Hospital), Naval Medical University, 168 Changhai Road, Shanghai, 200433, People’s Republic of China, Email [email protected]
Abstract: Ovarian cancer remains a significant cause of morbidity and mortality in women worldwide. Olaparib, a poly ADP-ribose polymerase (PARP) inhibitor, has been shown in studies to increase the time that people with cancer do not get worse. However, reports have indicated rare adverse effects, like myelodysplastic syndrome (MDS). In this report, we highlight the case of a 42-year-old female patient who was diagnosed with ovarian endometrioid carcinoma, FIGO Stage IIB. Following surgery and chemotherapy, the patient commenced maintenance therapy with Olaparib. After two years, she experienced abnormal blood test results, which ultimately led to a diagnosis of myelodysplastic syndrome (MDS), confirmed through a bone marrow biopsy. Despite initial obstacles, the patient underwent stem cell transplantation as a treatment for MDS. After undergoing stem cell transplantation, the patient experienced a notable improvement in their condition. Upon reevaluation, the transplantation proved successful as it resolved the abnormalities related to MDS. Furthermore, the ovarian cancer status showed a positive response, with no signs of disease progression during the follow-up period. This particular case emphasizes the importance of being vigilant for uncommon adverse effects, such as MDS, in ovarian cancer patients undergoing Olaparib maintenance therapy. Early diagnosis and treatment, which may include stem cell transplantation, can lead to favorable results, not only in managing MDS but also in possibly slowing down the progression of ovarian cancer that is causing it. Additional research is necessary to understand the risk factors and the most effective management approaches for these complications in this specific group of patients.
Keywords: stem cell transplantation, ovarian cancer, myelodysplasia, olaparib, case report
Introduction
Among gynecologic cancers, ovarian cancer is the most prevalent cause of mortality in high-income nations and the seventh most common cancer in women worldwide.1,2 For newly diagnosed advanced ovarian cancer, platinum-based chemotherapy and cytoreductive surgery are the standard treatments.3 First-line platinum-based chemotherapy is generally well-received by most women with epithelial ovarian cancer; nonetheless, recurrence is common, and the gap between chemotherapy and disease progression can range from 10 to 26 months.4,5
Response Evaluation Criteria in Solid Tumors, Poly (ADP-ribose) polymerase (PARP) inhibitors, according to guidelines, have great potential to increase the survival rate of women with ovarian cancer who have just received a diagnosis or who have had the disease return.6,7
The Food and Drug Administration (FDA) includes a warning on the label for uncommon but serious adverse effects, such as myelodysplastic syndrome (MDS) and acute myeloid leukemia (AML), which have become more common due to the increased use of PARP inhibitors. Despite having a similar mechanism of action, PARP inhibitors might differ significantly in their particular toxicity profiles. Furthermore, evidence from clinical trials indicated that MDS and AML incidence rates with poly (ADP-ribose) polymerase inhibitors (PARPi) were low, ranging from 0.5% to 1.4%.8
The incidence of myeloid neoplasms in individuals with ovarian cancer who have undergone treatment with PARPi has been steadily increasing in recent years. The cumulative exposure to PARPi and the enhanced overall survival rates observed in ovarian cancer patients could potentially contribute to this upward trend. Fortunately, the early administration of PARPi in the initial treatment phase reduces the likelihood of developing secondary myeloid neoplasms. The exact etiopathogenesis of this phenomenon remains uncertain; however, it is likely to involve multiple factors. Notably, the first two years of PARPi exposure seem crucial for starting myeloid neoplasms after PARPi treatment, with persistent cytopenia being an early sign.9
Case Presentation
On August 31, 2020, a 42-year-old female patient presented at Shanghai First Maternal and Infant Health Hospital, reporting lower abdominal distension and discomfort lasting for over half a month. At that time, her diagnosis was a suspected borderline ovarian tumor, and she had undergone laparoscopic right fallopian tube oophorectomy, laparoscopic intestinal adhesion-lysis, laparoscopic left ovarian biopsy, and omentum resection through laparotomy in September 2020. Before the surgical procedure, the tumor markers were recorded as follows: Alpha-fetoprotein (AFP): 1.52 ng/mL, Carcinoembryonic Antigen (CEA): 2.16 ng/mL, Cancer Antigen 125 (CA125): 2525.00 U/mL, Cancer Antigen 153 (CA153): 153.90 U/mL, Cancer Antigen 19–9 (CA199): >1200.00 U/mL, Squamous Cell Carcinoma Antigen (SCCA): 0.40 ng/mL, Human Epididymis Protein 4 (HE4): 506.4 pmol/L, with a Premenopausal ROMA Value of 96.48% and a Postmenopausal ROMA Value of 98.40%. The postoperative pathological examination revealed the following findings: on the right side, there was grade I ovarian endometrioid carcinoma, squamous differentiation, adhesive lesions on the right pelvic wall, and rough intestinal surface lesions. Cancer also affected the fallopian tubes serosa surface.
On November 20, 2020, this local hospital performed the surgery again. It included a laparoscopic abdominal total hysterectomy, a laparoscopic left fallopian tube-oophorectomy, and a laparoscopic intestinal adhesiolysis. The operation was conducted to excise all visible macroscopic disease, but some residual disease was observed post-operative. The patient received a diagnosis of FIGO Stage IIB ovarian endometrioid carcinoma. In the total uterus, postoperative pathological findings revealed endometrial hyperplasia disorder and chronic cervicitis. The left fallopian tube and ovary showed no abnormalities. The pelvic flush fluid smear revealed a few cells, but no tumor cells were found. The patient subsequently received six cycles of postoperative chemotherapy (paclitaxel and carboplatin).
The March 2021 homologous Recombination Deficiency (HRD) Test Report showed that the BRCA1/2 gene could be found in a single tissue sample [Table 1] and [Table 2]. From April 2021 to March 2023, we administered Lynparza as her primary treatment for her condition.
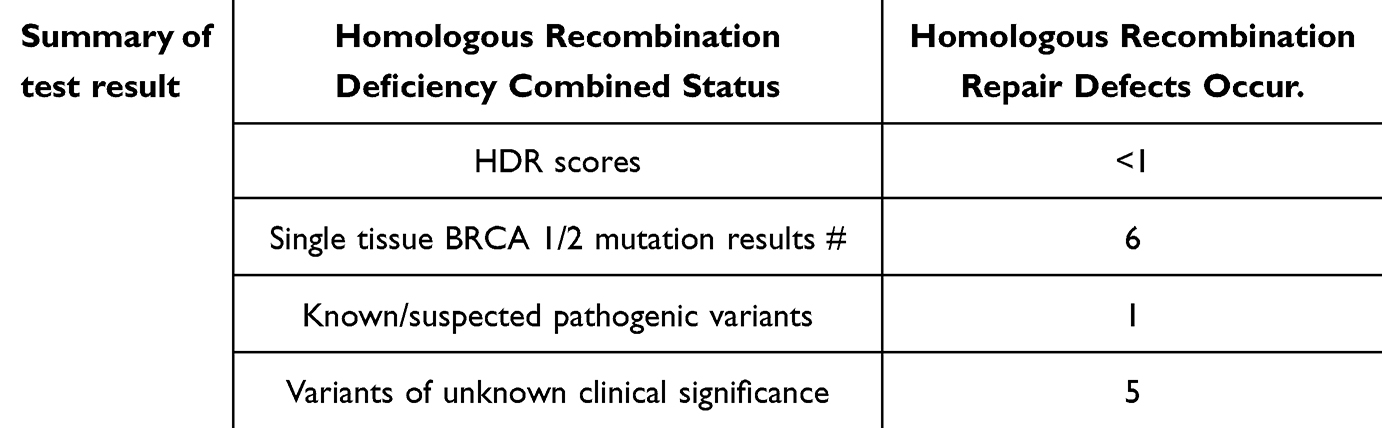 |
Table 1 Homologous Recombination Deficiency (HRD) Test Report Detection Summary |
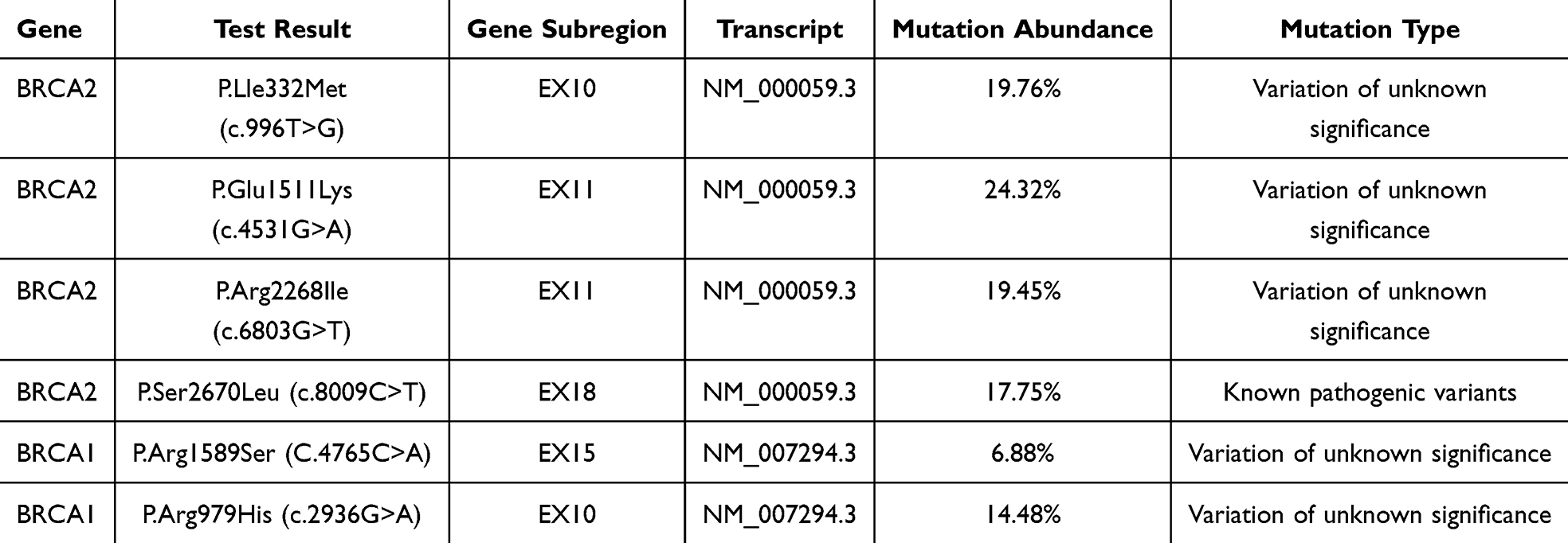 |
Table 2 Single-Tissue BRCA1/2 Gene Test Results |
In February 2023, she reported prolonged exhaustion lasting over five months, with a noticeable deterioration in the preceding month, prompting her to seek medical treatment at a local hospital. After a routine blood test showed that her platelet count (PLT) was 12x10^9/L and her hemoglobin level was 20 g/L, she was given blood products, thrombop aoietin (TPO), hatrodoxylin, platelet liter, and other treatments.
On July 20, 2023, a bone marrow aspiration showed that the shape of the myelodysplastic syndrome with low blasts (MDS-LB) was annular. We observed an increase in side oblasts, constituting 4.8% of the bone marrow. Flow cytometry analysis revealed that 30.561% of aberrantly nucleated red blood cells expressed the markers CD36, CD235a, and CD71 (Cluster of Differentiation). A bone marrow biopsy showed that the bone marrow was dividing very quickly, a sign of MDS because it means more blast cells. Gene testing showed that there was a TP53 mutation. A bone marrow biopsy revealed active bone marrow proliferation, indicating MDS with more blast cells.
In August 2023, bone marrow morphology will be helpful for MDS-LB (partial dilution) bone marrow imaging. The abnormal biopsies (bone marrow aspiration and iliac bone) showed signs of MDS [Figure 1] and [Figure 2]. These included myelofibrosis (MF grade 3), P53 abnormality, CSFIR abnormality, EGR1 abnormality, D7S486 abnormality, D75522 abnormality, D20S108 normal, and CEP8 normal. Chromosome analysis revealed that a limited number of cells were examined, with no signs of the mitotic phase observed. Additionally, with a mutation ratio of 11.37%.
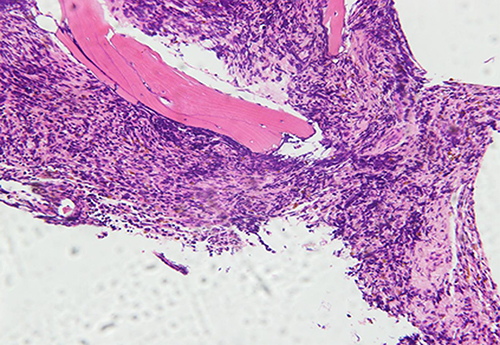 |
Figure 1 The bone marrow morphology of iliac bone. The bone marrow hyperplasia is active and filling. The fibrous tissue proliferates significantly, and the granulosa and red blood cell proportion decreases (200X). |
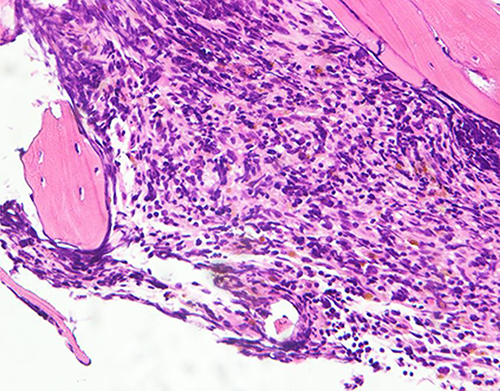 |
Figure 2 The bone marrow morphology of iliac bone. Consistent with MDS accompanied by myelofibrosis (400X). |
The AZA+VEN (Azacytidine and Venetoclax combination) chemotherapy regimen began on August 3, 2023. The specific medications were azacitidine 100 mg day 1–7, Venetoclax 100 mg day 1, 200 mg day 2–15, and 100 mg day 16–28. Hydration and alkalization were added to the medicines, and the ongoing symptomatic treatment included medicines to stop vomiting and diarrhea, protect the liver and stomach, supirocin, tigecycline to prevent fungal growth, and posaconazole to fight infections.
On October 20, 2023, a bone marrow reexamination revealed a diagnosis of myelodysplastic syndrome with increased blasts (MDS-IB1), with blast cells accounting for 7% of the total. The number of developing granulocytes decreased, with mature granulocytes comprising most of the total (39.8%). 21.0% of the erythrocytes are from the erythroid system and are mostly mid-late erythroblasts. A small number of immature erythrocytes have problems with their nuclei. In October 2023, we completed the ‘Dec + modified BuCy regimen’ (Decitabine, Busulfan, Cytarabine) pretreatment. The dosage was as follows: 30 mg of Decitabine day 13 to day 6–9, 4.5 mg of Cytarabine day 10 to day 9, 30 mg of Busulfan q6h day 8, 42.5 mg q6h day 7, 45 mg q6h day 6, 2.6 g of Cyclophosphamide Day 5 to day 4, and 350 mg of Semustine day 3. To stop GVHD (Graft-Versus-Host Disease), we gave ATG (100 mg from day 5 to day 2), CSA (cyclosporine), MMF (mycophenolate mofetil), and MTX (day 1, day 3, day 6). An unrelated donor hematopoietic stem cell infusion was performed, and 10.7×108/Kg and 4.8×106/Kg of MNCs and CD34+ cells were administered in total. After 15 days, bone marrow punctured was done. It showed a bone marrow image with low proliferation (partially diluted) [Figure 3, Figure 4], a chromosome number of 40 XY 20, a chimerism rate of 99.42%, and a negative TP53 mutation. Following the transplantation, the laboratory findings indicated CA 125 at 14.30 U/mL, HE4 at 68.4 pmol/L, and CA 199 at 19.96 U/mL.
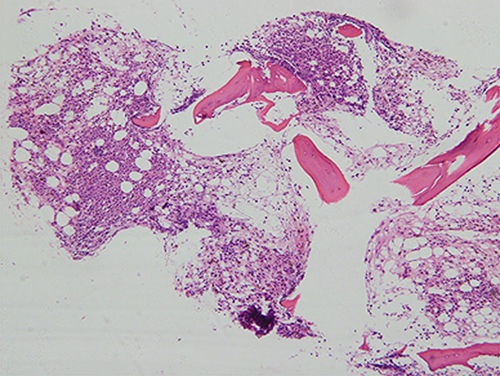 |
Figure 3 The bone marrow morphology of iliac bone. A small amount of bone marrow hyperplasia is present due to the proliferation of myeloid blast cells (100X). |
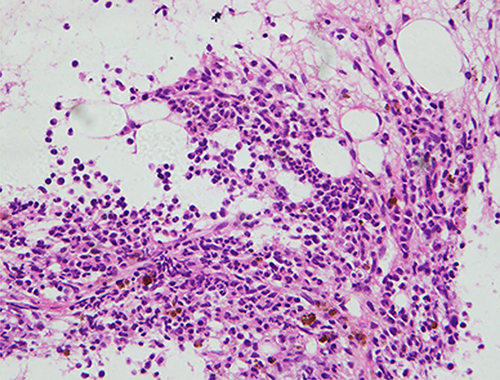 |
Figure 4 The bone marrow morphology of iliac bone. Patients with consistent MDS improved after bone marrow transplantation (400X). |
In February, the bone marrow morphology was often normal; the pathology revealed a small amount of low-proliferating bone marrow; the chimerism rate was 99.76%; and the chromosome was 46 XY (20). The biochemistry results showed an albumin level of 36 g/L, an alanine aminotransferase level of 460 g/L, and an alkaline phosphatase level of 2270 g/L. On the other hand, the blood routine examination indicated a white blood cell count of 3.79 x 10^9/L, a platelet count of 84 x 10^9/L, a hemoglobin level of 112 g/L, and reticulocytes at 1.54%. In February 2024, the patient received a maintenance treatment of decitabine, specifically 7.5 mg intravenously on dl-5, supplemented by liver-protecting medication, Stomach-protecting, anti-emetic, and other treatments.
The patient was hospitalized for the fourth time on March 23, 2024, for routine sequential treatment and outpatient follow-up. The latest CT revealed no signs of recurrence. She had been suffering from the illness for over a year.
Discussion
Patients with ovarian cancer have demonstrated the effectiveness of Olaparib maintenance therapy, but what happens when a patient also has myelodysplastic syndrome (MDS)? This case report explores the potential risks and benefits of using Olaparib in this patient population. MDS is a group of disorders characterized by abnormal blood cell production in the bone marrow, leading to a higher risk of developing leukemia. Patients with MDS often have compromised immune systems and are at a higher risk of developing infections. Given these risks, the use of olaparib in patients with MDS raises concerns about potential side effects and complications.
Olaparib serves as the first-line treatment for women with BRCA-mutated ovarian cancer and as a maintenance therapy following treatment for platinum-sensitive recurrent disease. The FDA and EMA have approved rucaparib and niraparib, in addition to olaparib, for use as maintenance therapy for ovarian cancer.10 Cancer patients’ tumors with homologous recombination deficiency (HRD) are targeted explicitly by poly (ADP ribose) polymerase (PARP) inhibitor-based therapy. Patients with impaired homologous recombination, particularly those with BRCA1/2 mutations, have demonstrated the benefits of PARP medications.11,12
In the study of Chandhok 2019, Olaparib showed potential as a PARP inhibitor for relapsed or refractory IDH1/2 (isocitrate dehydrogenase 1 and 2) mutant acute myeloid leukemia and myelodysplastic syndrome patients, potentially leading to synthetic lethality through inhibition of HR (homologous recombination) and SSB (single-strand breaks)-mediated DNA repair.13
Compared to AML, there was a significantly greater risk of MDS when using PARP inhibitors. MDS exhibits fewer primitive cells (<20%) in the bone marrow and peripheral blood than AML, but it has many clinical and pathological characteristics.14
According to the results, there is a greater chance of MDS than AML when using PARP inhibitors. However, the findings of the meta-analysis encompassing multiple RCTs showed no appreciable differences in the risks of MDS and AML linked to PARP inhibitors.15
A family of enzymes known as poly (ADP-ribose) polymerases transfer ADP-ribose to other proteins via the oxidized form of nicotinamide adenine dinucleotide (poly ADP-ribosylation). They contribute to the preservation of genomic stability, the control of apoptosis, and the reaction to damage to deoxyribonucleic acid (DNA).16
Two primary components comprise PARP inhibitors’ anticancer action. They can stop DNA single-strand repair and inhibit PARP enzyme activity. Additionally, by stabilizing their structure, PARP inhibitors can prevent DNA-PARP complexes from separating. This mechanism, commonly known as trapping, generates DNA-PARP complexes that hinder subsequent DNA repair processes for a prolonged period of time.17
Acute myelogenous leukemia cells control the expression of these proteins in a way that is different from healthy cells. PARA family proteins play a significant role in maintaining hematological function.18 PARP inhibitors can damage DNA and cause acquired mutations in clonal hematopoiesis in the circulatory system, heightening the risk of MDS and AML. Additionally, PARP inhibitors can trigger MDS and AML by altering epigenetics unexpectedly, resulting in alterations in clonal hematology.19
Olaparib has been linked to a heightened risk of myelodysplastic syndromes (MDS) and acute myeloid leukemia (AML), especially among patients with BRCA mutations, those who have undergone multiple courses of platinum-based chemotherapy, and individuals with extended exposure to PARP inhibitors. In these high-risk categories, the occurrence of MDS/AML can reach up to 10%, in contrast to less than 1% in the general population. Although other PARP inhibitors, such as rucaparib and niraparib, are also utilized in the treatment of ovarian cancer, the risk of MDS/AML seems to be more significant with olaparib. This may be attributed to its unique mechanism of action and the specific patient demographics in which it is predominantly administered.20
Recently, there has been a surge in research and scientific progress focused on hematopoietic stem cells (HSC). Therapeutic strategies are now utilizing these cells to treat solid tumors like ovarian cancer. Within this framework, researchers have proposed and clinically examined various approaches. The “autologous” method involves using HSC for hematologic support during high-dose chemotherapy treatments and utilizing them as a rich source of dendritic cells for cancer vaccination programs.21
In this case, we support the implementation of personalized treatment strategies for ovarian cancer patients diagnosed with MDS. We emphasize that although olaparib, utilized as a maintenance therapy, is effective in managing cancer, it may lead to severe neutropenia characterized by a low neutrophil count. For those patients who develop MDS following olaparib treatment, stem cell transplantation emerges as a viable option. This procedure addresses the issue of ineffective blood cell production by substituting damaged bone marrow with healthy stem cells, thereby enhancing blood cell production and overall health. Despite the risks, stem cell transplantation can provide significant benefits, potentially leading to long-term MDS and ovarian cancer remission, thus enhancing the patient’s quality of life. It is crucial to ensure close monitoring and proactive management of any side effects to safeguard patient safety throughout treatment.
Conclusion
Olaparib maintenance therapy in ovarian cancer patients with MDS requires a multidisciplinary approach involving oncologists, hematologists, and supportive care teams. By carefully considering the risks and benefits of treatment, healthcare providers can optimize patient outcomes in this complex clinical scenario. This case report highlights the potential for PARP inhibitors, particularly olaparib, to induce MDS and acute myeloid leukemia AML toxicity, especially with prolonged administration, which is linked to elevated mortality rates. Clinicians must carefully consider these risks when prescribing PARP inhibitors. For ovarian cancer patients who develop MDS after undergoing olaparib maintenance therapy, stem cell transplantation represents a crucial treatment alternative, offering a promising strategy for addressing their hematological complications. Furthermore, there may be a stronger association between olaparib and these adverse effects, necessitating further research into its long-term safety profile. Ongoing studies and clinical trials are vital to enhance management approaches and improve these individuals’ prognosis and quality of life.
List of Abbreviations
PARP, Poly ADP-ribose Polymerase (PARP) Inhibitor; MDS, Myelodysplastic Syndrome; FIGO, International Federation of Gynecology and Obstetrics; FDA, Food and Drug Administration; AML, Acute Myeloid Leukemia; HRD, Homologous Recombination Deficiency; BRAC 1/2, Breast Cancer Gene 1 and 2; PLT, Platelet; TPO, Thrombopoietin; MDS-LB, Myelodysplastic Syndrome with Low Blasts; AZA+VEN, Azacytidine and Venetoclax; Dec+ modified BuCy, Decitabine, Busulfan, Cytarabine; GVHD, Graft-Versus-Host Disease; CSA, Cyclosporine; MMF, Mycophenolate Mofetil; MTX, Methotrexate.
Data Sharing Statement
The data sets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The First Affiliated Hospital of Naval Medical University (Changhai Hospital), Naval Medical University, the local legislation and institutional requirements did not require Ethical review and approval for the study on human participants. The patients/participants provided written informed consent to participate in this study. Written informed consent was obtained from the individual(s) to publish any potentially identifiable images or data in this article.
Acknowledgments
We greatly appreciate the patients and their families’ invaluable contribution to this study. Gu Zhongyin participated in collecting data, so I would like to give special thanks to him. Furthermore, we sincerely thank the investigator for their unwavering commitment and profound expertise. Notably, we would like to extend our special thanks to Professor Cai Shengyun and Professor Wang Libing for their invaluable guidance and steadfast support throughout the entire research endeavor.
Funding
This paper is funded by The “234” Discipline Climbing Plan of the First Affiliated Hospital of Naval Medical University (2019YXK014).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Webb PM, Jordan SJ. Epidemiology of epithelial ovarian cancer. Best Pract Res Clin Obstet Gynaecol. 2017;41:3–14. doi:10.1016/j.bpobgyn.2016.08.006
2. Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61(2):69–90. doi:10.3322/caac.20107
3. National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology, ovarian cancer version 1; Available from: https://www.nccn.org/professionals/physician_gls/pdf/ovarian_blocks.pdf.
4. Walker JL, Brady MF, Wenzel L, et al. Randomized trial of intravenous versus intraperitoneal chemotherapy plus bevacizumab in advanced ovarian carcinoma: an NRG Oncology/Gynecologic oncology group study. J Clin Oncol. 2019;37(16):1380–1390. doi:10.1200/JCO.18.01568
5. Burger RA, Brady MF, Bookman MA, et al. Incorporation of bevacizumab in the primary treatment of ovarian cancer. N Engl J Med. 2011;365(26):2473–2483. doi:10.1056/NEJMoa1104390
6. Suh DH, Kim M, Lee KH, et al. Major clinical research advances in gynecologic cancer in 2017. J Gynecol Oncol. 2018;29(2). doi:10.3802/jgo.2018.29.e31
7. Ledermann J, Harter P, Gourley C, et al. Olaparib maintenance therapy in platinum-sensitive relapsed ovarian cancer. N Engl J Med. 2012;366(15):1382–1392. doi:10.1056/NEJMoa1105535
8. LaFargue CJ, Dal Molin GZ, Sood AK, Coleman RL. Exploring and comparing adverse events between PARP inhibitors. Lancet Oncol. 2019;20(1):e15–e28. doi:10.1016/S1470-2045(18)30786-1
9. Caruso G, Gigli F, Parma G, et al. Myeloid neoplasms post PARP inhibitors for ovarian cancer. Int J Gynecol Cancer. 2023;33(4):598–606. doi:10.1136/ijgc-2022-004190
10. Montemorano L, Lightfoot M, Bixel K. Role of olaparib as maintenance treatment for ovarian cancer: the evidence to date. Onco Targets Ther. 2019;12:11497–11506. doi:10.2147/OTT.S195552
11. Gelmon KA, Tischkowitz M, Mackay H, et al. Olaparib in patients with recurrent high-grade serous or poorly differentiated ovarian carcinoma or triple-negative breast cancer: a Phase 2, multicentre, open-label, non-randomised study. Lancet Oncol. 2011;12(9):852–861. doi:10.1016/S1470-2045(11)70214-5
12. Mirza MR, Monk BJ, Herrstedt J, et al. Niraparib maintenance therapy in platinum-sensitive, recurrent ovarian cancer. N Engl J Med. 2016;375(22):2154–2164. doi:10.1056/NEJMoa1611310
13. Chandhok NS, Wei W, Bindra R, et al. The PRIME Trial: PARP inhibition in IDH mutant effectiveness trial. a phase ii study of olaparib in isocitrate dehydrogenase (IDH) mutant relapsed/refractory acute myeloid leukemia and myelodysplastic syndrome. Blood. 2019;134(Supplement_1):3909. doi:10.1182/blood-2019-129168
14. Arber DA, Orazi A, Hasserjian R, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127(20):2391–2405. doi:10.1182/blood-2016-03-643544
15. Morice PM, Leary A, Dolladille C, et al. Myelodysplastic syndrome and acute myeloid leukaemia in patients treated with PARP inhibitors: a safety meta-analysis of randomised controlled trials and a retrospective study of the WHO pharmacovigilance database. Lancet Haematol. 2021;8(2):e122–e134. doi:10.1016/S2352-3026(20)30360-4
16. Anderson RC, Makvandi M, Xu K, et al. Iodinated benzimidazole PARP radiotracer for evaluating PARP1/2 expression in vitro and in vivo. Nucl Med Biol. 2016;43(12):752–758. doi:10.1016/j.nucmedbio.2016.08.007
17. Murai J, Huang SYN, Renaud A, et al. Stereospecific PARP Trapping by BMN 673 and comparison with olaparib and rucaparib. mol Cancer Ther. 2014;13(2):433–443. doi:10.1158/1535-7163.MCT-13-0803
18. Gil-Kulik P, Dudzińska E, Radzikowska-Büchner E, et al. Different regulation of PARP1, PARP2, PARP3 and TRPM2 genes expression in acute myeloid leukemia cells. BMC Cancer. 2020;20(1):435. doi:10.1186/s12885-020-06903-4
19. Bolton KL, Moukarzel LA, Ptashkin R, et al. The impact of poly ADP ribose polymerase (PARP) inhibitors on clonal hematopoiesis. J Clin Oncol. 2020;38(15_suppl):1513. doi:10.1200/JCO.2020.38.15_suppl.1513
20. Cottrell K, Clark CL, Penson RT. An update on the safety of olaparib for treating ovarian cancer. Expert Opin Drug Saf. 2022;21(4):447–451. doi:10.1080/14740338.2022.2047176
21. Perillo A, Pierelli L, Scambia G, Leone G, Mancuso S. The role of hematopoietic stem cells in the treatment of ovarian cancer. Panminerva Med. 2002;44(3):197–204.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.