Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 6
STD patients’ preferences for HIV prevention strategies
Authors Castro J, Jones D, Weiss S ![]()
Received 30 July 2014
Accepted for publication 18 August 2014
Published 12 December 2014 Volume 2014:6 Pages 171—175
DOI https://doi.org/10.2147/HIV.S71975
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Shenghan Lai
Jose G Castro,1 Deborah L Jones,2 Stephen M Weiss2
1Infectious Diseases, Department of Medicine, 2Department of Psychiatry and Behavioral Sciences, University of Miami, Miami, FL, USA
Abstract: The objective of this pilot study was to explore the knowledge of and preferences regarding effective biomedical interventions among high risk individuals attending a sexually transmitted diseases clinic, and to examine the effect of a brief information intervention on preference. Participants completed a baseline assessment, attended a presentation on human immunodeficiency virus (HIV) prevention methods, and completed a postintervention assessment. Outcome measures included: demographics and sexual risk factors, self-perceived HIV risk, and knowledge and attitudes regarding new biomedical methods of HIV prevention. After the baseline evaluation, participants were provided with information on new biomedical prevention strategies. Participants were given the option to review the information by reading a pamphlet or by viewing a brief video containing the same information. Participants (n=97) were female (n=51) and male (n=46). At baseline, only a small minority of participants were aware of the newer biomedical strategies to prevent HIV infection. Postintervention, 40% endorsed having heard about the use of HIV medications to prevent HIV infection; 72% had heard that male circumcision can decrease the risk of acquiring HIV infection in men; and 73% endorsed knowledge of the potential role of microbicides in decreasing the risk of acquiring HIV. Following the intervention, the most preferred prevention method was male condoms, followed by preexposure prophylaxis, and microbicides. The least preferred methods were male circumcision and female condoms. This study provides preliminary information on knowledge and attitudes regarding newer biomedical interventions to protect against HIV infection.
Keywords: STD clinic, biomedical HIV prevention, PrEP, male circumcision, microbicides
Introduction
In recent years, several studies have demonstrated the efficacy of diverse biomedical interventions to prevent the acquisition of human immunodeficiency virus (HIV).1–6 Major developments in the field of prevention of sexual transmission of HIV include male circumcision,1–3 the use of antiretrovirals before exposure to HIV (preexposure prophylaxis [PrEP]),4,7–9 and HIV viral suppression of HIV-infected individuals (treatment as prevention).6 The use of microbicides containing antiretrovirals has shown promise as a potentially viable option in a recent trial.5
Well-controlled studies have shown different levels of protection, ranging from 55% to more than 90% when a single intervention has been studied.1–6 In real-world situations, it is foreseeable that individuals will soon have the option to choose and ideally, to combine appropriate prevention interventions according to their individual circumstances, attitudes, preferences, and the availability of effective methods. To facilitate this process, research is needed to develop a triage system that could be integrated into the existing clinical service infrastructure.
Sexually transmitted disease (STD) clinics conduct HIV/sexually transmitted infection (STI) testing with large numbers of individuals at high risk of HIV infection. This study explored the knowledge of and preferences for effective biomedical interventions among high-risk individuals attending an urban STD clinic in South Florida and examined the effect of a brief information intervention on their preferences. We are not aware of any studies in the US that have explored individual preference for newer prevention methods or that have explored how familiar those most at risk for HIV infection are with these methods. It was anticipated that this study would provide information to develop a triage system to streamline decision making regarding the most effective and acceptable interventions. In this context, triage refers to the process by which health care centers will create mechanisms that will match patient preferences and risk factors to available HIV prevention services.
Methods
Ethics approval
Institutional Review Board (IRB) (University of Miami Miller School of Medicine and Florida Department of Health) approvals and written client informed consent were obtained before recruitment, assessment, and any study-related intervention.
Recruitment/participants
The study was conducted between November 2012 and September 2013 at the Miami-Dade County Health Department STD clinic in South Florida. Enrollment of participants was open for about 4 months. During the active days of recruitment, recruitment was strong, and only a few people referred by providers refused to participate. No information about people who refused to participate was collected as it was not allowed by the IRB.
The clinic is located in downtown Miami and serves primarily low income, ethnic minority county residents; in 2012, 2.7% of all patients tested HIV seropositive. Study staff acquainted all clinic personnel regarding the objectives of the study, and potential participants were referred for assessment of eligibility. Interested individuals were interviewed by study staff in a private room at the clinic, and those eligible provided informed consent. In order to be eligible, participants had to be: men and women who presented at the clinic for STD testing; 18 years of age or older; and of HIV-negative or unknown status. There were no exclusions based on literacy as all materials for assessment were verbally administered by study staff. Following consent, participants completed a baseline assessment, attended a presentation on HIV prevention methods, and completed a postintervention assessment.
Participants of the study were compensated for their time (1.5 to 2 hours) to complete the intervention and questionnaires, and received $15. The estimated minimum time needed to complete study procedures was: eligibility and coordination with referring health care provider (5 minutes), informed consent process (20 minutes), baseline assessment (20 minutes), intervention (15 minutes), postintervention assessment (20 minutes), and final check, review of all forms, compensation, and receipt (10 minutes).
Questionnaires
Demographics and sexual risk factors
This questionnaire’s topics included age, race, ethnicity, educational level, marital status, number of partners in the prior 2 months, and use of condoms in the last sexual encounter.
Outcome measure: preference
Self-perceived HIV risk and knowledge, and attitudes regarding traditional and new biomedical methods of HIV prevention (ie, male circumcision, PrEP, microbicides, male and female condoms, a hypothetical HIV vaccine) were assessed. Items assessed willingness to use HIV prevention methods, using a Likert scale scored 1 to 5 (5= strongly agree, 4= somewhat agree, 3= neutral, 2= somewhat disagree, and 1= strongly disagree); higher scores indicated greater willingness.
Intervention
Participants were provided with information on new biomedical prevention strategies, in their preferred language. The information was given in simple terms and included the definition of the method, and the main advantages and disadvantages of each method. It also included a representative graphic (eg, drawing of status pre- and postcircumcision, pill box, and a microbicide applicator). Participants were given the option to review the information by reading a pamphlet or by viewing a brief video (5 minutes) containing the same information. The information about each HIV prevention method was provided in a randomly alternating order to avoid ordering effect bias. The study coordinator was also available to answer any questions about the information provided. Postintervention assessment of biomedical HIV prevention preferences used the same scales as in the baseline evaluation. Questionnaires were completed by participants, but study staff were also available to clarify questions.
Data analysis
Data was coded and uploaded into the Statistical Package for Social Sciences (SPSS) software for statistical analysis. Descriptive statistics were performed on the total sample and subgroups by sex, ethnicity/race, and sexual preference. Associations (chi square) between all the subgroups and preferences for the three interventions were examined.
Results
Demographics and HIV risk
Study participants (n=97) included 51 women and 46 men. Demographic characteristics are presented in Table 1. Most participants (61%) reported at least one prior episode of an STD. The majority (87%) had undergone an HIV test within the past year, but almost half (44%) were not aware of the HIV status of all of their sexual partners, and about a third (28%) endorsed sex with someone they did not know. Only 31% of participants felt they were at risk of HIV infection if they continued to engage in their current sexual behavior. As well, 38% of participants reported having sex while intoxicated by drugs or alcohol. Finally, 28% reported never using condoms with regular partners, and 20% reported using condoms less than 10% of the time with “other” partners.
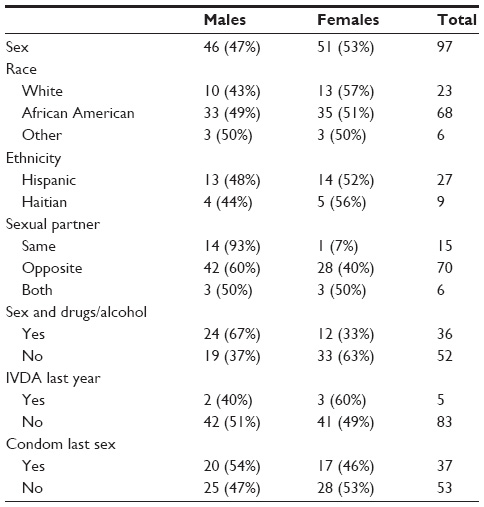 | Table 1 Demographic characteristics* |
Baseline
Awareness of HIV prevention methods
At baseline, only 13% of the participants had heard of taking HIV medications to prevent HIV infection (PrEP). Most reported knowing about male circumcision, but only 21% had heard that male circumcision decreased the risk of acquiring HIV infection in men. Only 9% of participants had heard that microbicides could decrease the risk of sexually acquiring HIV infection.
Attitudes regarding HIV prevention methods
At baseline, the first choice for prevention method among all participants was male condoms (52%), followed by male circumcision (18%) and PrEP (14%). The least preferred methods were the use of microbicides (3%) and female condoms (13%). Preferences for these methods were similar between sexes, with the exception of PrEP, which was more favored by males (χ2=3.78, P=0.05, odds ratio [OR] =3.264, confidence interval [CI] =0.8–13.6), and female condoms, which were more favored by females (χ2=3.25, P=0.07, OR =4.1, CI =0.7–30). The wide confidence intervals are a reflection of the small sample, but the tendency is interesting. Most participants (80%) were interested in learning more about the option of taking pills daily to prevent HIV infection in comparison with the other preventive methods; 54% of uncircumcised men expressed willingness to be circumcised, and 69% were willing to use microbicides. More than 90% of the participants would be willing to get vaccinated if a vaccine was available.
Postintervention
Awareness of HIV prevention methods
Postintervention, 48% endorsed having heard about the use of HIV medications to prevent HIV infection; 72% had heard that male circumcision can decrease the risk of acquiring HIV infection in men; and 73% endorsed knowledge of the potential role of microbicides in decreasing the risk of acquiring HIV. The increase in awareness about each of these three methods was similar between both sexes.
Attitudes toward HIV prevention methods
Following the intervention, the most preferred prevention method was male condoms (34%), followed by PrEp (18%) and microbicides (18%). The least preferred methods were male circumcision (14%) and female condoms (14%).
Discussion
This pilot study was designed to explore knowledge of and hypothetical preferences regarding prevention methods among high risk individuals and to examine the effect of a brief informational intervention on preference. Results indicate that in this sample, awareness of the newer biomedical interventions to prevent HIV transmission was low. At study entry, most preferred male condoms as a prevention method, though condom use was low or suboptimal. However, following a brief intervention, participants’ preferences would include other prevention methods.
The low awareness regarding PrEP in this study is similar to that reported in other settings;10–13 however, we are not aware of any other reports from the USA that also evaluated knowledge and preferences for male circumcision and microbicides. A recent report of serodiscordant couples in South Carolina found high levels of acceptability of PrEP if available; but participants’ awareness of PrEP prior to the study was not assessed.13 Results from the present study suggest that the relative acceptance of a prevention method can be affected by the availability of other more appealing methods. Results may also suggest that the ability to fully understand some of these methods may vary by the type of method and that the concept of PrEP in particular may be more difficult to comprehend than the others.
Interestingly, the current study also showed that the interest in a vaccine is high, though neither the pamphlet nor video included any information on vaccines. These findings would suggest that the concept of “vaccines” is much more familiar (and acceptable) to patients as a preventive strategy than these other novel methods.
This study highlights the need to provide more information about newer methods of HIV prevention to at-risk patients. It also demonstrates the need for assessment of patient knowledge and preferences for these methods, to better design a triage system to optimize the delivery of these prevention strategies.
Strengths
The sample of participants was drawn from a multiracial and multiethnic STD clinic that should be one of the primary targets to implement HIV prevention interventions, given the high incidence of HIV in the city and in the clinic.
Limitations
During the conduct of this study, there was an ongoing demonstration project in the clinic to provide PrEP to men who have sex with men. This exposure may have biased participant knowledge and preference for this method of HIV prevention. A randomized control group was not used, and as a result, it was not possible to be certain that the intervention caused the outcome. The reason why this study did not include a control arm was that this study was funded as a pilot. However, this study has generated the need to plan for a larger study that will include a control arm. The sample size of this pilot study prevented subanalyses by ethnicity or sexual preference; future research should be conducted with larger samples and control groups to address these issues. In addition, follow-up assessment was only done immediately postintervention; preferences for method may change over time or with additional consideration. Finally, it is possible that responses to hypothetical scenarios may be a poor proxy for future patient preferences.
Conclusion
This study provides preliminary information on knowledge and attitudes regarding newer biomedical interventions to protect against HIV infection. Further research is needed to explore the role of brief informational interventions, to better inform patients and practitioners, and enhance patients’ willingness to engage in HIV prevention strategies. A triage system is needed to effectively tailor current prevention strategies to patients, in order to provide the most effective outcomes.
Acknowledgment
We acknowledge support from the Miami Center for AIDS Research at the University of Miami Miller School of Medicine funded by a grant (P30A1073961) from the National Institutes of Health (NIH).
Disclosure
The authors report no conflicts of interest in this work.
References
Auvert B, Taljaard D, Lagarde E, Sobngwi-Tambekou J, Sitta R, Puren A. Randomized, controlled intervention trial of male circumcision for reduction of HIV infection risk: The ANRS 1265 trial. PLoSMed. 2005;2(11):1112–1122. | |
Bailey RC, Moses S, Parker CB, et al. Male circumcision for HIV prevention in young men in Kisumu, Kenya: a randomised controlled trial. Lancet. 2007;369(9562):643–656. | |
Gray RH, Kigozi G, Serwadda D, et al. Male circumcision for HIV prevention in men in Rakai, Uganda: A randomized trial. Lancet. 2007;369(9562):657–666. | |
Grant RM, Lama JR, Anderson PL, et al; iPrEx Study Team. Preexposure chemoprophylaxis for HIV prevention in men who have sex with men. N Engl J Med. 2010;363(27):2587–2599. | |
Abdool Karim Q, Abdool Karim SS, Frohlich JA, et al; CAPRISA 004 Trial Group. Effectiveness and safety of tenofovir gel, an antiretroviral microbicide, for the prevention of HIV infection in women. Science. 2010;329(5996):1168–1174. | |
Cohen MS, Chen YQ, McCauley M, et al; HPTN 052 Study Team. Prevention of HIV-1 infection with early antiretroviral therapy. N Eng J Med. 2011;365(6):493–505. | |
Michael NL. Oral preexposure prophylaxis for HIV – another arrow in the quiver? N Engl J Med. 2010;363(27):2663–2665. | |
Whiteside YO, Harris T, Scanlon C, Clarkson S, Duffus W. Self-perceived risk of HIV infection and attitudes about preexposure prophylaxis among sexually transmitted disease clinic attendees in South Carolina. AIDS Patient Care STDS. 2011;25(6):365–370. | |
Myers GM, Mayer KH. Oral preexposure anti-HIV prophylaxis for high-risk US populations: current considerations in light of new findings. AIDS Patient Care STDS. 2011;25(2):63–71. | |
Krakower DS, Mimiaga MJ, Rosenberger JG, et al. Limited awareness and low immediate uptake of pre-exposure prophylaxis among men who have sex with men using an internet social networking site. PLoS One. 2012;7(3):e33119. | |
Barash EA, Golden M. Awareness and use of HIV pre-exposure prophylaxis among attendees of a seattle gay pride event and sexually transmitted disease clinic. AIDS Patient Care STDS. 2010;24(11):689–691. | |
Galea JT, Kinsler JJ, Salazar X, et al. Acceptability of pre-exposure prophylaxis as an HIV prevention strategy: barriers and facilitators to pre-exposure prophylaxis uptake among at-risk Peruvian populations. Int J STD AIDS. 2011;22(5):256–262. | |
Tripathi A, Whiteside YO, Duffus WA. Perceptions and attitudes about preexposure prophylaxis among seronegative partners and the potential of sexual disinhibition. South Med J. 2013;106(10):558–564. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.