Back to Journals » Clinical Ophthalmology » Volume 20
Standardized Ultra-Widefield Swept-Source OCT Imaging: A Reproducible Protocol for Peripheral Retinal Assessment
Authors Shah SH, Zhu Y, Bennett C, Tracy J, Ploumi I ![]() , Barton KM
, Barton KM ![]() , Gumustop S
, Gumustop S ![]() , Nodecker K, Wagner S, Chen C
, Nodecker K, Wagner S, Chen C ![]() , Ding X, Stevanovic M, Lains I
, Ding X, Stevanovic M, Lains I ![]() , Miller JB
, Miller JB ![]()
Received 14 November 2025
Accepted for publication 25 February 2026
Published 17 April 2026 Volume 2026:20 581561
DOI https://doi.org/10.2147/OPTH.S581561
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yousef Fouad
Shivesh H Shah,1,2,* Ying Zhu,1,2,* Cade Bennett,1,2 Jack Tracy,1,2 Ioanna Ploumi,1,2 Kailynn M Barton,1,2 Selin Gumustop,1,2 Kayla Nodecker,1,2 Sarah Wagner,1,2 Chong Chen,1,2 Xinyi Ding,1,2 Marta Stevanovic,2 Ines Lains,1– 3 John B Miller1– 3
1Harvard Retinal Imaging Lab, Massachusetts Eye and Ear, Boston, MA, USA; 2Department of Ophthalmology, Harvard Medical School, Boston, MA, USA; 3Retina Service, Massachusetts Eye and Ear, Department of Ophthalmology, Harvard Medical School, Boston, MA, USA
*These authors contributed equally to this work
Correspondence: John B Miller, Retina Service, Massachusetts Eye and Ear Infirmary, Department of Ophthalmology, Harvard Medical School, 243 Charles St, Boston, MA, 02114 1, USA, Tel +1 (617) 573-3750, Fax +1 (617) 573-3698, Email [email protected]
Background: The utilization of ultra-widefield (UWF) photography and, more recently, UWF-OCT has increased greatly in retina clinic. The most widely available UWF-OCT uses navigated swept-source OCT (SS-OCT), which lacks a standardized protocol, consequently limiting comparisons across patient visits or larger population-based studies. We present a structured imaging protocol to address this limitation.
Technique: A universal template standardizes the number, type, and anatomical positioning of seven scans per patient, including three 21 mm line scans and four UWF volume scans. Scans are automatically positioned per protocol and ultimately stitched into a composite image, which is optimized for longitudinal and inter-patient comparisons.
Discussion: This protocol enhances efficiency and ensures reproducible assessment of peripheral retinal findings. It may be adapted for other UWF systems and is currently being evaluated for clinical applications.
Keywords: standardized protocol, peripheral retina, ultrawidefield optical coherence tomography, age-related macular degeneration, diabetic retinopathy
Introduction
Optical coherence tomography (OCT) has transformed the diagnosis and treatment of retinal diseases.1 The development of swept source OCT (SS-OCT) has further advanced this field, enabling high-resolution visualization of the peripheral retina through ultra-widefield SS-OCT (UWF SS-OCT).2–4 Although UWF SS-OCT is being increasingly utilized in clinical settings, variability in fixation, anatomical differences, and the absence of a standardized reference limit its reproducibility.5 These factors hinder consistent comparisons across visits and complicate larger population-based studies. To address this gap, we propose a standardized protocol using a commercially available UWF SS-OCT device (Silverstone, Optos plc, Dunfermline, UK) to achieve consistent assessment of the peripheral retina. This protocol uniquely defines consistent fixation targets and scan positioning, reducing acquisition variability and providing a reproducible framework that may potentially be adopted across clinics and studies for longitudinal and population-level analysis.
Technique
Silverstone SS-OCT is an UWF imaging system that combines a 200° single-capture scanning laser ophthalmoscopy (UWF-SLO) fundus photograph with 1050 nm swept-source OCT. This technology allows for precise peripheral assessment using navigated line or volume scans mapped to UWF-SLO images. We propose a standardized protocol that uses a combination of both navigated line and volume scans based on foveal and vascular arcade landmarks to create a template that can be used for longitudinal and inter-patient comparisons.
In this protocol, a universal template is designed as a reference to standardize the number, types, and anatomical locations of all scans used for each patient (Figure 1). A color fundus photograph (CFP) with central fixation is first captured to guide the placement of subsequent OCT scans. A total of seven OCT scans per eye are acquired, consisting of three 21 mm line scans and four 12×12 mm UWF volume scans. Acquisition of these scans takes approximately 10 minutes per eye. Line scans are centered on the fovea, just above the superior arcade venule, and just below the inferior arcade venule. All four volume (cube) scans are positioned relative to the foveal line scan as follows: superior and inferior scans are positioned with their bottom and top edges 7 mm above and below the foveal line respectively, and both are centered horizontally on the fovea. Temporal and nasal scans are aligned with the temporal and nasal edges of the foveal line scan respectively. All OCT scans are positioned automatically per template specifications, with minor manual adjustments allowed to ensure alignment with anatomical landmarks. This standardized protocol ensures reproducible peripheral retinal assessment.
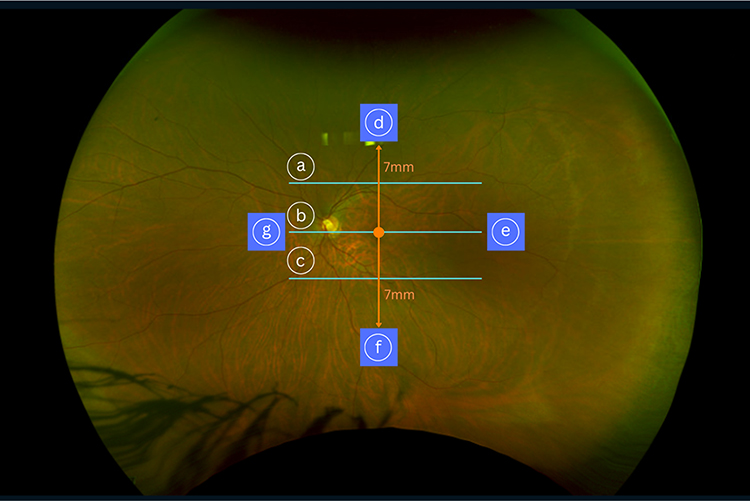 |
Figure 1 Schematic diagram of the proposed Silverstone ultra-widefield swept-source optical coherence tomography (UWF SS-OCT) imaging protocol. Three 21 mm line scans (light blue) are positioned (a) just above the superior arcade venule, (b) at the fovea, and (c) just below the inferior arcade venule. Four 12×12 mm UWF volume scans (dark blue) are positioned as follows: (d) the superior cube scan, with its bottom edge 7 mm above the foveal line and centered horizontally on the fovea; (e) the temporal cube scan, with its central scan positioned in line with the temporal edge of the foveal line scan; (f) the inferior cube scan, with its top edge 7 mm below the foveal line and centered horizontally on the fovea; and (g) the nasal cube scan, with its central scan positioned in line with the nasal edge of the foveal line scan. Orange lines indicate the 7 mm distances marking the placement of the superior and inferior scans relative to the foveal line scan. |
CFP and OCT scans are then automatically stitched together into a high-resolution composite UWF representation of the retina with both the en face view and cross-sectional OCT data. After being reviewed for clarity, alignment, and quality, data can be stored on OptosAdvance as DICOM (Digital Imaging and Communications in Medicine) files.
Discussion
A growing body of evidence suggests that detecting peripheral retinal pathology may play a critical role in the early diagnosis and management of chronic retinal diseases and inherited retinal dystrophies.6–8 Although UWF OCT has emerged as a valuable tool for visualizing the peripheral retina, a standardized protocol for UWF SS-OCT has not yet been established.2,6,9 The absence of a predefined, reproducible protocol may limit broader clinical adoption and research comparability of UWF SS-OCT, particularly in cases where precise longitudinal comparisons of peripheral findings are key to disease monitoring.5,10
Here, we propose a standardized imaging protocol for Silverstone UWF SS-OCT to improve consistency in peripheral retinal assessment with UWF SS-OCT. Just as the ETDRS (Early Treatment Diabetic Retinopathy Study) macular grid standardizes macular measurements, our protocol provides a structured framework for reproducible UWF SS-OCT imaging of the peripheral retina. Similar frameworks have been effectively applied in the assessment of peripheral lesions associated with age-related macular degeneration (AMD) using geometric distortion-corrected UWF imaging.11 We demonstrate implementation of this protocol in peripheral visualization of eyes with wet AMD (Figure 2) and severe nonproliferative diabetic retinopathy (Figure 3).
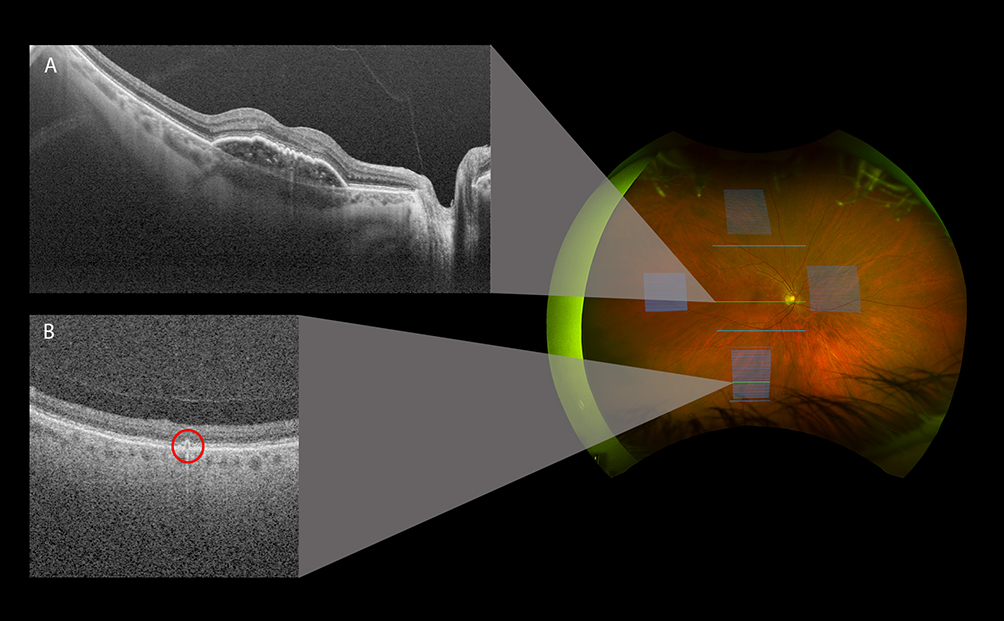 |
Figure 2 Silverstone SS-OCT of a patient with wet age-related macular degeneration (AMD). The main image illustrates the locations of the seven scans acquired for this eye, including three 21 mm line scans and four 12×12 mm ultra-widefield volume scans. (A) Cross-sectional OCT image from the 21 mm foveal line scan showing focal pigment epithelial detachment (PED). (B) Cross-sectional OCT image from the inferior volume scan, highlighting the presence of peripheral drusen (circled). |
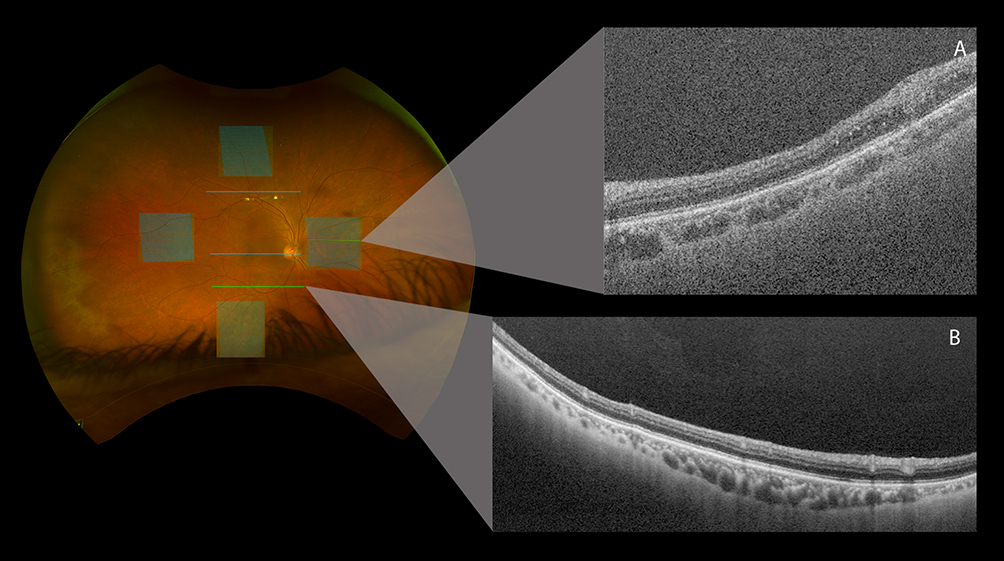 |
Figure 3 Silverstone SS-OCT of a patient with severe non-proliferative diabetic retinopathy (NPDR). The main image illustrates the locations of the seven scans acquired for this eye, including three 21 mm line scans and four 12×12 mm ultra-widefield volume scans. (A) Cross-sectional OCT image from the nasal volume scan, demonstrating hyperreflective foci and intraretinal cystoid spaces. (B) Cross-sectional OCT image from the 21 mm line scan at the inferior arcade. |
Our protocol is intended to address challenges related to scan reproducibility, ensuring accurate comparisons across longitudinal visits or larger population-based studies by enabling precise scan location replication. A standardized acquisition approach may improve confidence that interval differences in peripheral findings reflect true change rather than variability in scan location or fixation. This is particularly relevant in diabetic retinopathy, retinal vein occlusion, retinal vasculitis, and inherited retinal dystrophies, where peripheral findings may prompt closer follow-up or additional ultra-widefield angiography. Standardized peripheral UWF SS-OCT acquisition may therefore support more consistent longitudinal documentation. Additionally, by incorporating preset scan configurations, our approach may improve feasibility of clinical implementation via reduced imaging time and improved workflow efficiency. This method may also be adapted to other UWF-OCT systems without standardized protocols. One limitation of this study is that volume-scan placement was standardized by a fixed linear distance (7 mm) rather than angular eccentricity. Therefore, differences in axial length, especially in highly myopic or hyperopic eyes, may lead to variable true retinal eccentricity across subjects. In addition, this protocol was designed to prioritize peripheral assessment and therefore included only a single foveal line scan rather than a dedicated high-definition macular raster or macular volume scan. While comprehensive macular characterization may be limited within this acquisition framework, incorporating macular volume scans in future iterations would enable a more complete assessment.
As ultra-widefield technologies continue to expand the field of view while maintaining high resolution, standardized acquisition will remain essential for consistent detection and comparison of peripheral abnormalities. Standardization is increasingly important as peripheral imaging is used to derive quantitative biomarkers; SS-OCTA metrics have been associated with diabetic retinopathy progression, suggesting that similar reproducibility requirements may apply to UWF SS-OCT–based peripheral assessment.12 More broadly, protocol standardization may reduce operator-dependent variability and facilitate uniform interpretation across institutions. For instance, multi-center trials using standardized OCT grading have achieved intraclass correlations of 0.99 for thickness measurements with no grading drift over time.13 To support these future applications, this protocol is now being applied as a standardized baseline framework, with prospective longitudinal data collection underway to evaluate repeatability, feasibility, and downstream clinical utility across visits and operators.
Conclusion
In conclusion, we propose a standardized imaging protocol for Silverstone UWF SS-OCT that defines consistent fixation targets and scan positioning to improve reproducibility of peripheral retinal assessment. By using a universal template with preset line and volume scans that can be replicated across visits, this approach is intended to minimize acquisition variability and support more accurate longitudinal and inter-patient comparisons. Although scan placement is currently standardized by linear distance and macular imaging is limited within this framework, future iterations incorporating macular volume scans and ongoing prospective evaluation will further refine repeatability, feasibility, and downstream clinical utility.
Abbreviations
CFP, color fundus photograph; DICOM, Digital Imaging and Communications in Medicine; ETDRS, Early Treatment Diabetic Retinopathy Study; OCT, optical coherence tomography; SLO, scanning laser ophthalmoscopy; SS-OCT, swept-source OCT; UWF, ultra-widefield.
Ethics Statement
This study was reviewed by the Mass General Brigham Institutional Review Board (IRB) and determined to be exempt under 45 CFR 46.104(d)(4) (Protocol #2024P000689).
Acknowledgments
We would like to thank our lead photographer, John Hensel, for help with the technical implementation of this technique as well as image acquisition.
Author Contributions
Shivesh H Shah and Ying Zhu contributed equally as co-first authors. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
JBM is disclosing support by Intalight and Adaptive Sensory Technology and consulting work for Alcon, Allergan, Boehringer, Carl Zeiss, Sumitomo Pharma America, Inc., Sunovion, Topcon, and Genentech. All other authors have no disclosures, and no financial or non-financial competing interests.
References
1. Laíns I, Wang JC, Cui Y, et al. Retinal applications of swept source optical coherence tomography (OCT) and optical coherence tomography angiography (OCTA). Prog Retin Eye Res. 2021;84:100951. doi:10.1016/j.preteyeres.2021.100951
2. Kurobe R, Hirano Y, Ogura S, Yasukawa T, Ogura Y. Ultra-widefield swept-source optical coherence tomography findings of peripheral retinal degenerations and breaks. Clin Ophthalmol. 2021;15:4739–6. doi:10.2147/OPTH.S350080
3. Kovacs KD, Mahrous MA, Gonzalez L, et al. Feasibility and clinical utility of ultra-widefield–navigated swept-source optical coherence tomography imaging. J Vitreoretin Dis. 2021;5(5):396–404. doi:10.1177/2474126421997335
4. Takahashi H, Uramoto K, Ohno-Matsui K. Ultra-widefield optical coherence tomography for retinal detachment with proliferative vitreoretinopathy. Retin Cases Brief Rep. 2022;16(3):355–359. doi:10.1097/ICB.0000000000000980
5. Kalra G, Pichi F, Kumar Menia N, et al. Recent advances in wide field and ultrawide field optical coherence tomography angiography in retinochoroidal pathologies. Expert Rev Med Dev. 2021;18(4):375–386. doi:10.1080/17434440.2021.1902301
6. Marcus DM, Silva PS, Liu D, et al. Association of predominantly peripheral lesions on ultra-widefield imaging and the risk of diabetic retinopathy worsening over time. JAMA Ophthalmol. 2022;140(10):946. doi:10.1001/jamaophthalmol.2022.3131
7. Forshaw TRJ, Minör ÅS, Subhi Y, Sørensen TL. Peripheral retinal lesions in eyes with age-related macular degeneration using ultra-widefield imaging. Ophthalmol Retina. 2019;3(9):734–743. doi:10.1016/j.oret.2019.04.014
8. Cui Y, Zhu Y, Wang JC, et al. Comparison of widefield swept-source optical coherence tomography angiography with ultra-widefield colour fundus photography and fluorescein angiography for detection of lesions in diabetic retinopathy. Br J Ophthalmol. 2021;105(4):577–581. doi:10.1136/bjophthalmol-2020-316245
9. McNabb RP, Grewal DS, Mehta R, et al. Wide field of view swept-source optical coherence tomography for peripheral retinal disease. Br J Ophthalmol. 2016;100(10):1377–1382. doi:10.1136/bjophthalmol-2015-307480
10. Lee WW, Muni RH. Single-capture ultra-widefield guided swept-source optical coherence tomography in the management of rhegmatogenous retinal detachment and associated peripheral vitreoretinal pathology. Br J Ophthalmol. 2023;107(9):1356–1362. doi:10.1136/bjophthalmol-2021-320149
11. Oellers P, Laíns I, Mach S, et al. Novel grid combined with peripheral distortion correction for ultra-widefield image grading of age-related macular degeneration. Clin Ophthalmol. 2017;11:1967–1974. doi:10.2147/opth.s143246
12. Sun, Z, Tang, F, Wong, R, Szeto, SK et al OCT Angiography Metrics Predict Progression of Diabetic Retinopathy and Development of Diabetic Macular Edema: A Prospective Study. Ophthalmology. 2019;126(12):1777. doi:10.1016/j.ophtha.2020.09.022
13. DeCroos FC, Toth CA, Stinnett SS, Heydary CS, Burns R, Jaffe GJ. Optical coherence tomography grading reproducibility during the comparison of age-related macular degeneration treatments trials. Ophthalmology. 2012;119(12):2549–2557. doi:10.1016/j.ophtha.2012.06.040
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.