Back to Journals » Clinical Ophthalmology » Volume 20
SRF and SHRM in nAMD: Retrospective Analysis of Visual Prognosis
Authors Wu W ![]() , Guo H, Wang L
, Guo H, Wang L ![]() , Yang M
, Yang M ![]()
Received 31 December 2025
Accepted for publication 16 February 2026
Published 28 February 2026 Volume 2026:20 590001
DOI https://doi.org/10.2147/OPTH.S590001
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Weizhen Wu, Huiling Guo, Luping Wang, Ming Yang
Author affiliations:Department of Ophthalmology, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Ming Yang, Email [email protected]
Objective: This study aimed to investigate the correlation between subretinal fluid (SRF) and subretinal hyperreflective material (SHRM) with visual prognosis in neovascular age related macular degeneration (nAMD).
Methods: A retrospective analysis was conducted on 60 nAMD patients diagnosed at our ophthalmology department from March 2017 to December 2024. All patients received intravitreal anti-vascular endothelial growth factor (VEGF) injections monthly for the first 3 months, followed by pro re nata (PRN) treatment for the subsequent 9 months. Quantitative measurements of SRF and SHRM (height and width on OCT) were collected, along with patient demographics, best corrected visual acuity (BCVA), and central foveal thickness (CMT).
Results: After 12 months of treatment, BCVA, CMT, and SRF parameters significantly improved (P < 0.05). The visual improvement group showed superior reductions in SRF and SHRM height compared to the nonimprovement group (P < 0.05). Greater baseline SRF thickness (> 180 μm) was significantly associated with better final visual acuity (P = 0.034), while baseline SHRM presence correlated with worse final BCVA and CMT (P < 0.05). These findings indicate that SRF serves as a favorable prognostic indicator, whereas SHRM is a key predictor of poor visual outcomes (P = 0.001).
Discussion: SRF and SHRM morphological features are linked to nAMD treatment response. SRF thickness positively correlates with visual improvement, serving as a prognostic indicator. Persistent SHRM, however, is associated with fibrotic components that may impair retinal function, making it a key parameter for poor outcomes. These findings align with prior studies, highlighting the importance of quantitative SRF and SHRM assessment in predicting treatment response.
Conclusion: SRF and SHRM are clinically significant biomarkers in nAMD treatment, effectively predicting visual prognosis and guiding individualized therapeutic strategies. Their quantitative evaluation may aid in optimizing treatment tolerance strategies and improving real world clinical outcomes.
Keywords: neovascular age related macular degeneration, subretinal fluid, subretinal hyperreflective material
Introduction
Neovascular age related macular degeneration (nAMD) is one of the leading causes of blindness globally, with its incidence significantly increasing with age, posing a major public health challenge worldwide.1 Although intravitreal anti-vascular endothelial growth factor (VEGF) injections effectively inhibit neovascularization, there is a notable discrepancy between clinical efficacy and randomized controlled trial outcomes, highlighting the need for more reliable biomarkers to guide individualized treatment strategies.2
Optical coherence tomography (OCT) technology has identified multiple imaging features associated with nAMD, among which subretinal hyperreflective material (SHRM) and subretinal fluid (SRF) serve as clinically significant biomarkers.3 SRF is characterized as an exudate between the outer boundary of the photoreceptors and the inner boundary of the retinal pigment epithelium (RPE), representing the most common fluid localization in type 1 macular neovascularization.4 The clinical implications of SRF remain controversial. The CATT study revealed5,6 that eyes with foveal SRF at 5 year follow up exhibited significantly better visual outcomes. A post hoc analysis of the VIEW trial demonstrated7,8 that nAMD patients with baseline SRF had higher average best corrected visual acuity (BCVA) at baseline and during anti-VEGF treatment compared to those without SRF. However, Sadda et al contested the protective role of SRF, emphasizing that in the HARBOR study,4,9 patients with persistent SRF achieved favorable visual results due to continuous treatment throughout the study period.
SHRM is defined as an abnormal deposit between the outer layer of the neuroepithelium and the inner layer of the pigment epithelium, with highly heterogeneous composition potentially including exudates, fibrin, and other components.10 The CATT study5,6 showed that SHRM was detected in 77% of nAMD patients, with 54% remaining persistent after 2 years of treatment, suggesting its involvement in disease chronicity. As a key indicator of chronicity, SHRM’s well demarcated hyperreflective features are significantly associated with an increased risk of retinal scarring.11 During anti-VEGF therapy, the proportion of fibrotic components in SHRM may gradually increase, leading to reduced treatment responsiveness. This phenomenon not only reflects structural changes in the retina but may also impair retinal function through physical barriers and toxic effects.12
This study aims to address a critical knowledge gap regarding the quantitative prognostic significance of SRF and SHRM in real world anti-VEGF treated populations, where current clinical practice is limited by a lack of consensus on how these biomarkers interact to influence visual outcomes and disease progression. It is important to note that SRF differs fundamentally from intraretinal fluid (IRF) and pigment epithelial detachment (PED) in both biological implications and prognostic value: SRF primarily reflects exudative processes between the photoreceptors and the RPE, whereas IRF and PED involve distinct anatomical layers and pathophysiological mechanisms. This study specifically focuses on SRF and SHRM, rather than IRF, to more precisely elucidate their roles in the pathogenesis of neovascular nAMD.
The potentially protective role of SRF may be attributed to its nature as a transient exudate, which can be absorbed or stabilized through anti-VEGF therapy, thereby preserving retinal architecture. In contrast, the adverse impact of SHRM is likely due to its composition of fibrin and other fibrotic components, which may form a physical barrier that impairs photoreceptor function and promotes chronic inflammation. These findings have important implications for contemporary treatment paradigms, such as treat and extend or fluid tolerant strategies. A deeper understanding of the prognostic roles of SRF and SHRM may enable clinicians to tailor anti-VEGF therapy more precisely, ultimately improving visual outcomes and reducing treatment burden in patients with nAMD.
Materials and Methods
A retrospective analysis was conducted on 60 patients diagnosed with nAMD at our ophthalmology department from March 2017 to December 2024. Among the subjects, 38 were male (63%) and 22 were female (37%), with ages ranging from 53 to 92 years (mean age: 75.10 ± 1.70 years). The diagnosis of nAMD was based on ophthalmic examinations including fundoscopy, OCT, and fluorescein fundus angiography (FFA). All cases exhibited neovascularization, and patients with comorbid diabetic retinopathy, high myopia, or other systemic diseases that could interfere with retinal evaluation were excluded. Only eyes with a minimum follow up duration of 12 months were included. All enrolled eyes received intravitreal anti-VEGF injections at a frequency of once per month for the initial 3 months, followed by pro re nata (PRN) treatment for the subsequent 9 months.
General demographic data of all included patients were collected, including age, gender, type of AMD, and number of injections administered. Baseline and endpoint examinations (12 months post treatment) were conducted, encompassing BCVA assessments and imaging data obtained via fundus color photography (Topcon, Japan; Optos, UK), spectral domain OCT (SD-OCT; Heidelberg Engineering, Germany), and fluorescein fundus angiography (FFA, Carl Zeiss Meditec, Germany). Adverse events such as endophthalmitis, elevated intraocular pressure, anterior chamber inflammation, and rebleeding were also recorded.
SD-OCT scan the area centered on the macula with a 6×6 mm2 range. Central foveal retinal thickness (CMT) was measured manually using built in software on OCT linear scans, quantifying the vertical distance between the inner limiting membrane (ILM) and the RPE (Figure 1). SRF was defined as a hypo reflective area between the outer boundary of the photoreceptors and the inner boundary of the RPE on OCT linear scans. SRF height was measured as the vertical distance from the highest point of SRF to the RPE, while SRF width was determined as the farthest distance between the two ends of SRF on the same interface (Figure 1). SHRM was defined as a hyper reflective area above the RPE on OCT scans. SHRM height was measured as the vertical distance from the highest point of SHRM to the RPE, and SHRM width was measured as the farthest distance between the two ends of SHRM on the same interface (Figure 1).
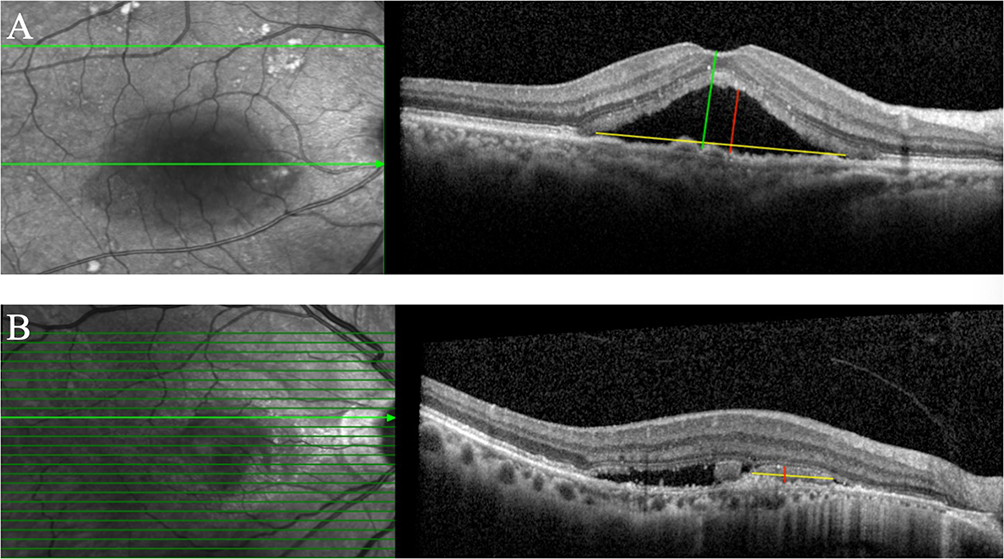 |
Figure 1 Presents the measurement methods for CMT, SRF, and SHRM. In (A), the green line indicates the measurement of CMT, the yellow and red lines represent the width and height measurements of SRF, respectively. In (B), the yellow and red lines represent the width and height measurements of SHRM, respectively. |
Using the international logarithmic visual acuity chart, patients were categorized into two groups based on comparisons between baseline and endpoint BCVA: the visual improvement group (≥1 line improvement in BCVA, comprising 42 eyes) and the nonimprovement group (≥1 line decline or no improvement in BCVA, comprising 18 eyes). The changes in BCVA, CMT, SRF width and height, and SHRM width and height between the two groups before and after treatment were analyzed and compared.
Patients were stratified into two groups based on baseline SRF thickness: Group 1 (SRF thickness ≤180 μm, 38 cases) and Group 2 (SRF thickness >180 μm, 22 cases), with their effects on baseline and endpoint BCVA assessed.
Patients were further grouped based on the presence or absence of SHRM at baseline and endpoint to evaluate its impact on baseline and endpoint BCVA.
All imaging results and measurements were independently evaluated by two senior ophthalmologists using a double blind method (κ=0.85). Standardized deidentified images were employed, with patient identifiers, medical history, and treatment information concealed. No clinical discussions were conducted prior to evaluation, and any discrepancies were resolved by a third party expert.
This study was approved by the Ethics Committee of Beijing Friendship Hospital and implemented under institutional guidance (2022-P2-308-01). As a retrospective study, it utilized preexisting medical records obtained during clinical practice, with deidentified data extracted via a clinical big data platform. Given the complete anonymization of data, rendering individual participants untraceable, and the absence of any personal privacy or commercial interests, all participants’ privacy and confidentiality were strictly protected. Based on these ethical considerations, informed consent was waived for this study. The principles of the Declaration of Helsinki were followed.
Statistical analyses were performed using SPSS 27.0 software. Continuous data are presented as mean ± standard deviation. Normally distributed continuous data between groups were compared using the t-test, while nonnormally distributed data were compared using the Mann–Whitney U-test. Categorical data are expressed as percentages (%), and comparisons between groups were made using the χ2-test or Fisher’s exact test. The significance level was set at α = 0.05.
Results
A total of 60 nAMD patients (60 eyes) were enrolled, including 38 males (38 eyes) and 22 females (22 eyes). Among them, 34 cases (57%) were classified as type 1 nAMD, and 26 cases (43%) as type 2 nAMD. The average number of injections administered was 4.96 ± 1.70. No adverse events such as endophthalmitis, elevated intraocular pressure, or anterior chamber inflammation were observed in any patient.
Comparisons between baseline and endpoint examinations (12 months post treatment) revealed statistically significant differences in BCVA, CMT, and the width and height of SRF (P = 0.017, P = 0.001, P < 0.001, P = 0.003, respectively) (Table 1).
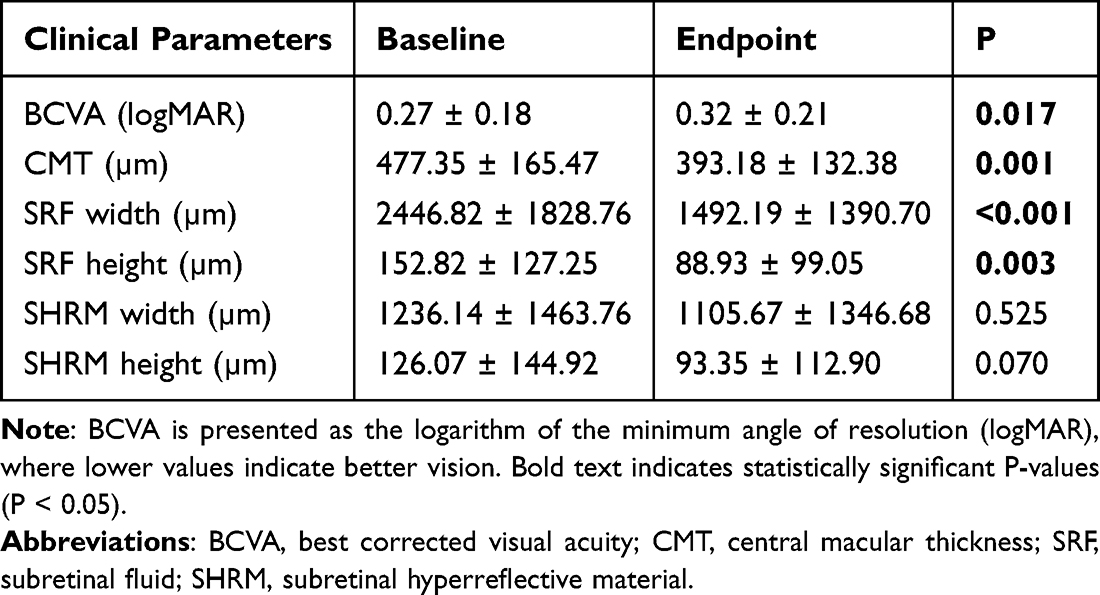 |
Table 1 Comparison of Clinical Parameters at Baseline and Endpoint in All Enrolled Patients |
Patients were stratified into two groups based on BCVA improvement: the BCVA improvement group (42 cases) and the nonimprovement group (18 cases). No statistically significant differences were observed between the two groups in terms of gender, age, type of nAMD, or number of injections administered (P = 0.310, P = 0.120, P = 0.823, P = 0.947, respectively). Similarly, no significant differences were found in baseline BCVA, CMT, SRF width and height, or SHRM width and height (P = 0.059, P = 0.521, P = 0.757, P = 0.289, P = 0.413, P = 0.549, respectively). However, endpoint examinations demonstrated statistically significant differences between the two groups in BCVA, CMT, SRF height, and SHRM width and height (P = 0.003, P = 0.018, P = 0.003, P = 0.017, P = 0.004, respectively) (Table 2).
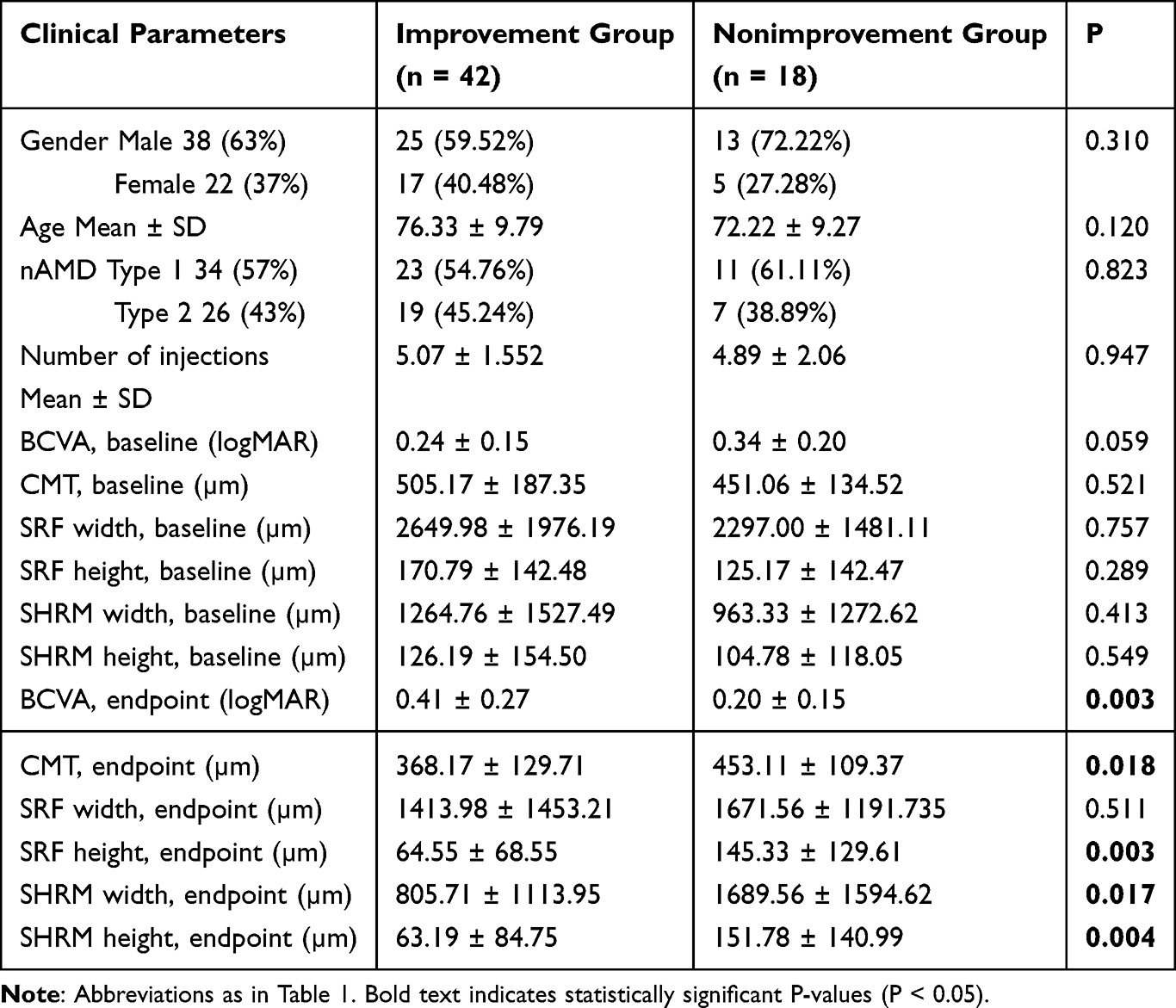 |
Table 2 Baseline and Endpoint Clinical Parameters by BCVA Improvement Status |
Patients were further divided into two groups based on baseline SRF thickness: Group 1 (SRF thickness ≤180 μm, n = 38) and Group 2 (SRF thickness >180 μm, n = 22). No statistically significant difference was observed in baseline BCVA between the two groups (P = 0.776), but endpoint BCVA exhibited a significant difference (P = 0.034). Patients in Group 2 (SRF thickness >180 μm) demonstrated significantly better endpoint BCVA (0.45 ± 0.31) compared to Group 1 (SRF thickness ≤180 μm), suggesting a positive correlation between SRF thickness and visual improvement. Analysis of covariance (ANCOVA) confirmed a statistically significant association between SRF and visual prognosis (P = 0.001) (Table 3).
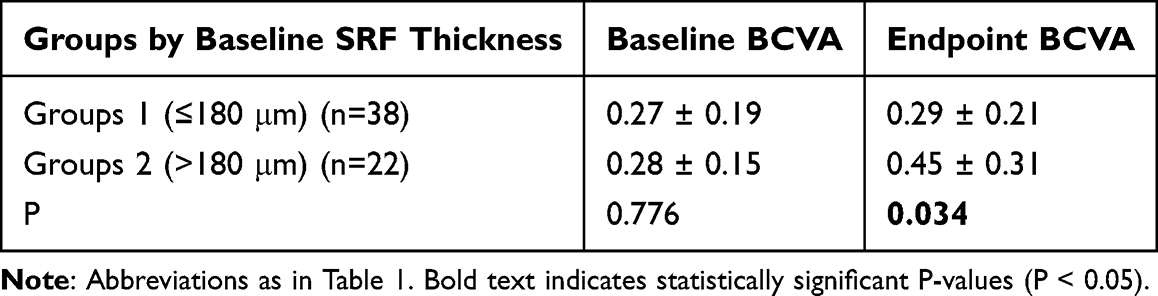 |
Table 3 Comparison of Visual Acuity Between Groups Stratified by Baseline SRF Thickness |
Patients were categorized into two groups based on the presence or absence of baseline SHRM: the baseline SHRM group (31 cases) and the baseline non-SHRM group (29 cases). Comparisons between the two groups revealed statistically significant differences in gender, age, and baseline BCVA (P = 0.039, P = 0.002, P = 0.008, respectively), with patients in the baseline SHRM group exhibiting lower baseline BCVA. Endpoint examinations showed statistically significant differences between the two groups in endpoint BCVA, CMT, and SRF height (P = 0.037, P = 0.010, P = 0.030, respectively), with patients in the baseline non-SHRM group achieving significantly better endpoint BCVA. ANCOVA analysis confirmed a statistically significant association between SHRM and visual prognosis (P = 0.001) (Table 4).
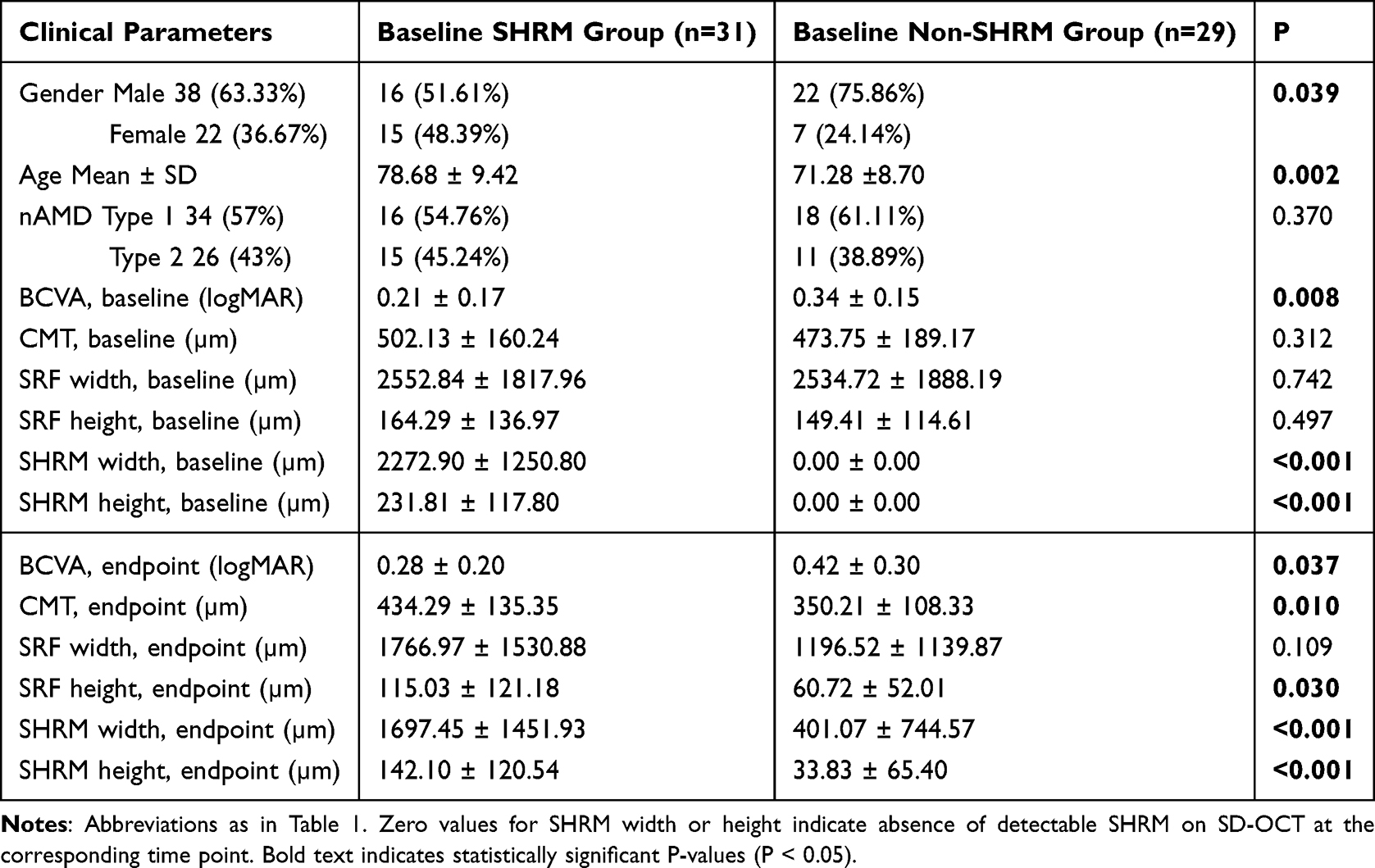 |
Table 4 Comparative Analysis of Clinical Parameters Stratified by Baseline SHRM Status |
Discussion
nAMD is characterized by choroidal neovascularization in the macular region as its core pathological mechanism, often accompanied by retinal exudation, hemorrhage, edema, and scar formation, ultimately leading to irreversible vision impairment.2 Intravitreal injection of anti-VEGF agents, as the current first line therapeutic strategy, effectively inhibits neovascularization and reduces fluid leakage. However, clinical data indicate that only 30%–40% of patients achieve significant vision improvement.13 This limitation underscores the critical importance of exploring novel biomarkers to optimize clinical management strategies.
Advancements in OCT technology have established retinal intraretinal fluid (IRF), pigment epithelial detachment (PED), SRF, and SHRM as key biomarkers in nAMD.14 The accumulation of SRF directly compromises retinal structural integrity, impairing photoreceptor function and consequently affecting BCVA. Clinical observations suggest that the presence of SRF is associated with an increased risk of vision decline, while its absorption following anti-VEGF therapy can effectively restore the macular microenvironment, promote retinal layer apposition, and thereby improve or stabilize visual outcomes. This mechanism has been validated in multiple clinical trials.9,15 For instance, baseline SRF presence exhibits a negative correlation with post treatment vision improvement, and its absorption extent serves as a pivotal indicator for evaluating therapeutic response and prognosis. However, the CATT study5,6 revealed that eyes with foveal SRF at 5 year follow up demonstrated significantly better visual outcomes, though this advantage disappeared after adjusting for IRF, SHRM, and large CNV. The VIEW 2 trial7,8 further confirmed that patients with baseline SRF had higher baseline visual acuity, and the prognostic value of SRF depends on its cooccurrence with IRF or PED. The prospective design of the FLUID trial16,17 innovatively demonstrated that a permissive treatment strategy allowing SRF thickness up to 200 μm maintained efficacy while significantly reducing injection frequency (40% fewer injections at 24 months). Compared to IRF, SRF presence is typically associated with superior visual outcomes and lower atrophy rates, prompting clinicians to reconsider its biological significance in nAMD.18,19 Intriguingly, our study found that the endpoint BCVA in the SRF > 180 μm group was significantly better than that in the SRF ≤ 180 μm group, suggesting a positive correlation between SRF thickness and vision improvement. This aligns with the findings of the VIEW study. SRF may facilitate functional recovery by preserving photoreceptor structural integrity. Our results indicate a statistically significant association between SRF and visual prognosis, supporting the use of SRF thickness as a predictive biomarker for treatment efficacy. However, the limited sample size and short follow up duration in this study constrain further investigations into SRF or residual SRF.
SHRM comprises diverse components, primarily including fibrous tissue, neovascularization, and exudates (eg, subretinal hyperreflective exudate, SHE). FFA and OCT are pivotal diagnostic tools for differentiating these components.5,10 The impact of these components on retinal structure and their responsiveness to anti-VEGF therapy vary significantly. Clinical observations indicate that neovascular SHRM is particularly sensitive to anti-VEGF treatment.10,11 While the exact composition of exudates remains unclear, existing studies hypothesize that SHE represents an avascular SHRM associated with active neovascularization. These exudates typically regress with effective anti-VEGF therapy, potentially originating from fibrin deposition.3 Notably, the CATT study demonstrated5,6 that SHRM is an independent predictor of the worst visual prognosis, highlighting its clinical value in forecasting AMD outcomes. Accurate identification and classification of SHRM components via advanced imaging techniques such as FFA and OCT can provide reliable guidance for individualized treatment strategies, thereby improving visual prognosis. In our study, nAMD patients with better visual outcomes exhibited significantly smaller SHRM width and height compared to those without improvement. This may be attributed to the association between persistent SHRM and increased risk of retinal scar atrophy. This finding corroborates the CATT study conclusions. During anti-VEGF therapy, as fluid components are absorbed and reduced, SHRM volume gradually decreases, while the proportion of fibrotic components relatively increases,20 leading to diminished therapeutic responsiveness. It is well established that the barrier between the retinal neuroepithelium and RPE disrupts tissue metabolism and nutrient exchange, damaging photoreceptors. Therefore, SHRM located at this site may exert toxic effects on photoreceptors, further disrupting the ellipsoid zone (EZ) and causing vision impairment.21 Scholars have proposed that the contact between SHRM and photoreceptors, along with the barrier it creates between photoreceptors and RPE, plays a role in the association between SHRM and poor visual prognosis.22 Additionally, Ehlers et al reported that as early as week 4 of anti-VEGF therapy, EZ integrity and SHRM volume in nAMD eyes showed improvement, with EZ integrity and SHRM volume serving as predictors of post treatment visual outcomes,23 consistent with our observations.
Conclusion
This study demonstrates that in the clinical management of nAMD, treatment regimen adjustments should incorporate quantitative imaging biomarkers such as SRF and SHRM. Our findings show that greater baseline SRF thickness (>180 μm) is associated with better visual outcomes, suggesting a potential structural buffering or physiological role for SRF within certain limits, which supports a strategy of “limited tolerance of SRF” in anti-VEGF therapy. However, it is important to emphasize that the 180 μm threshold is exploratory and cohort specific, requiring validation in multicenter, large sample prospective studies. In contrast, the presence and persistence of SHRM are clearly associated with poor visual prognosis, likely due to its fibrotic components forming a physical barrier and promoting chronic inflammation. The conclusions primarily reflect the overall prognostic value of SHRM, as its heterogeneity (eg, composition, location) was not assessed in stratified analyses.
The conclusions of this study are tempered by several limitations, including its single center, retrospective design and relatively small sample size, which constrain causal inference and generalizability. Additionally, the reliance on linear rather than volumetric measurements for SRF and SHRM may limit sensitivity in detecting subtle morphological changes. Future research should address these limitations by expanding the sample size, adopting prospective designs, and incorporating volumetric indices. Subsequent investigations should also further differentiate the clinical implications of various SHRM subtypes and SRF characteristics (eg, coexistence with IRF or PED) and integrate molecular analyses with advanced multimodal imaging to refine individualized treatment strategies and improve long term visual outcomes for patients with nAMD.
Acknowledgments
The authors would like to thank all the participants involved in the study.
Funding
This work was supported by the National Natural Science Foundation of China (Grant No. 82000899) and the Beijing Natural Science Foundation (Grant No. L2510058).
Disclosure
No potential conflict of interest was reported by the authors.
References
1. Zhang C, Owen LA, Lillvis JH, Zhang SX, Kim IK, DeAngelis MM. AMD genomics: non-coding RNAs as biomarkers and therapeutic targets. J Clin Med. 2022;11(6):1484. doi:10.3390/jcm11061484
2. Fleckenstein M, Schmitz-Valckenberg S, Chakravarthy U. Age-related macular degeneration: a review. JAMA. 2024;331(2):147–8. doi:10.1001/jama.2023.26074.
3. Baek J, Ra H, Lee SH, Cheung CMG, Lee WK. Subretinal hyperreflective material, atrophy, and intraretinal fluid in pachychoroid neovasculopathy. Am J Ophthalmol. 2025;280:472–480. doi:10.1016/j.ajo.2025.08.048
4. Sadda SR, Tuomi LL, Ding B, Fung AE, Hopkins JJ. Macular atrophy in the HARBOR study for neovascular age-related macular degeneration. Ophthalmology. 2018;125(6):878–886.
5. Miller JW. Comparison of age-related macular degeneration treatments trials 2: introducing comparative effectiveness research. Ophthalmology. 2020;127(4S):S133–S134. doi:10.1016/j.ophtha.2019.11.025
6. Jaffe GJ, Ying GS, Toth CA, et al. Comparison of Age-related Macular Degeneration Treatments Trials Research Group. Macular Morphology and Visual Acuity in Year Five of the Comparison of Age-related Macular Degeneration Treatments Trials. Ophthalmology. 2019;126(2):252–260. doi:10.1016/j.ophtha.2018.08.035
7. Schmidt-Erfurth U, Waldstein SM, Deak GG, Kundi M, Simader C. Pigment epithelial detachment followed by retinal cystoid degeneration leads to vision loss in treatment of neovascular age-related macular degeneration. Ophthalmology. 2015;122:822–832. doi:10.1016/j.ophtha.2014.11.017
8. Waldstein SM, Simader C, Staurenghi G, et al. Morphology and visual acuity in aflibercept and ranibizumab therapy for neovascular age-related macular degeneration in the VIEW trials. Ophthalmology. 2016;123(7):1521–1529. doi:10.1016/j.ophtha.2016.03.037
9. Sadda S, Holekamp NM, Sarraf D, et al. Relationship between retinal fluid characteristics and vision in neovascular age-related macular degeneration: HARBOR post hoc analysis. Graefes Arch Clin Exp Ophthalmol. 2022;260(12):3781–3789. doi:10.1007/s00417-022-05716-4
10. Metrangolo C, Donati S, Mazzola M, et al. OCT biomarkers in neovascular age-related macular degeneration: a narrative review. J Ophthalmol. 2021;2021:9994098. doi:10.1155/2021/9994098
11. Montolío-Marzo S, Gallego-Pinazo R, Palacios-Pozo E, Dolz-Marco R. Advantages of optical coherence tomography as a high dynamic range imaging modality in subretinal hyperreflective material. Retina. 2023;43(4):641–648. doi:10.1097/IAE.0000000000003705.
12. Feo A, Stradiotto E, Sacconi R, Menean M, Querques G, Romano MR. Subretinal hyperreflective material in retinal and chorioretinal disorders: a comprehensive review. Surv Ophthalmol. 2024;69(3):362–377. doi:10.1016/j.survophthal.2023.10.013
13. Yerramothu P. New Therapies of Neovascular AMD-Beyond Anti-VEGFs. Vision. 2018;2(3):31. doi:10.3390/vision2030031.
14. Gnanaraj R, Lisker-Cervantes A, Patnaik J, et al. Multimodal imaging biomarkers for progression from intermediate to advanced age-related macular degeneration (AMD): a 10-year prospective longitudinal cohort study from the University of Colorado AMD registry. BMJ Open Ophthalmol. 2025;10(1):e002112. doi:10.1136/bmjophth-2024-002112.
15. Gianniou C, Dirani A, Jang L, Mantel I. Refractory intraretinal or subretinal fluid in neovascular age-related macular degeneration treated with intravitreal ranizubimab: functional and structural outcome. Retina. 2015;35(6):1195–1201. doi:10.1097/IAE.0000000000000465
16. Arnold JJ, Markey CM, Kurstjens NP, Guymer RH. The role of sub-retinal fluid in determining treatment outcomes in patients with neovascular age-related macular degeneration--a Phase IV randomised clinical trial with ranibizumab: the FLUID study. BMC Ophthalmol. 2016;16:31. doi:10.1186/s12886-016-0207-3
17. Guymer RH, Markey CM, McAllister IL, Gillies MC, Hunyor AP, Arnold JJ. FLUID investigators. tolerating subretinal fluid in neovascular age-related macular degeneration treated with ranibizumab using a treat-and-extend regimen: fluid study 24-month results. Ophthalmology. 2019;126(5):723–734. doi:10.1016/j.ophtha.2018.11.025
18. Zarbin MA, Hill L, Maunz A, Gliem M, Stoilov I. Anti-VEGF-resistant subretinal fluid is associated with better vision and reduced risk of macular atrophy. Br J Ophthalmol. 2022;106(11):1561–1566. doi:10.1136/bjophthalmol-2020-318688
19. Sharma A, Parachuri N, Kumar N, et al. Notion of tolerating subretinal fluid in neovascular AMD: understanding the fine print before the injection pause. Br J Ophthalmol. 2021;105(2):149–150. doi:10.1136/bjophthalmol-2020-317933
20. Roberts PK, Schranz M, Motschi A, et al. Baseline predictors for subretinal fibrosis in neovascular age-related macular degeneration. Sci Rep. 2022;12(1):88. doi:10.1038/s41598-021-03716-8.
21. Ehlers JP, Lunasco LM, Yordi S, et al. Compartmental exudative dynamics in neovascular age-related macular degeneration: volumetric outcomes and impact of volatility in a phase iii clinical trial. Ophthalmol Retina. 2024;8(8):765–777. doi:10.1016/j.oret.2024.02.010
22. Kominami A, Tomita S, Kato A, et al. Japan Clinical Retina Study (J-CREST) group. factors affecting visual acuity after anti-vascular endothelial growth factor therapy in neovascular age-related macular degeneration: a multicenter study in Japan. J Clin Med. 2024;13(20):6244. doi:10.3390/jcm13206244
23. Ehlers JP, Patel N, Kaiser PK, et al. The association of fluid volatility with subretinal hyperreflective material and ellipsoid zone integrity in neovascular AMD. Invest Ophthalmol Vis Sci. 2022;63(6):17. doi:10.1167/iovs.63.6.17
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.