Back to Journals » Clinical Ophthalmology » Volume 16
Spotlight on iPad Visual Field Tests Efficacy
Authors Ichhpujani P ![]() , Dhillon H
, Dhillon H
Received 8 March 2022
Accepted for publication 27 June 2022
Published 5 July 2022 Volume 2022:16 Pages 2179—2185
DOI https://doi.org/10.2147/OPTH.S340508
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Parul Ichhpujani, Hennaav Dhillon
Department of Ophthalmology, Government Medical College and Hospital, Chandigarh, India
Correspondence: Parul Ichhpujani, Department of Ophthalmology, Government Medical College and Hospital, Chandigarh, 160030, India, Tel +91-9501071591, Fax +91-172-2608488, Email [email protected]
Abstract: Tablet based perimetry has the potential to be used as a low-cost, portable method for glaucoma screening. With the advent of tablets with large dynamic luminance range and high spatial resolution, perimetry applications can test visual field locations within the central 30 degrees, just like bowl perimetry. Tablet perimetry has garnered interest in this COVID era as it can be promptly done in the waiting room or even from the comfort of home. The current review focuses on evaluating glaucoma detection sensitivities, diagnostic abilities and correlation of each parameter and examination time of the iPad based perimetry applications with those of HFA.
Keywords: visual field, standard automated perimetry, tablet perimetry, iPad
Introduction
Glaucoma is one of the leading causes of irreversible blindness across the globe occurring due to retinal ganglion cell (RGC) loss leading to visual field (VF) defects. With the growing number and proportion of elderlies in the population, it is projected that 111.8 million people will have glaucoma in 2040.1 Testing of the VFs is the only method to quantify the extent of functional loss in glaucoma patients.2
Humphrey Field Analyzer (HFA), Medmont Automated Perimeter (MAP) and Octopus are commonly used perimeters for standard automated perimetry (SAP). SAP using the HFA Swedish Interactive Threshold Algorithm (SITA) Standard and SITA Fast program is widely accepted as the “clinical standard”.3 Automated perimeters have several inherent disadvantages such as their bulky nature, exclusive space for installation, need for a dark room for examination and limited portability in addition to being costly and requiring trained personnel to run it.4 Many patients have difficulty concentrating throughout the test and find the test tiring.5 Fixation Losses are consistently elevated after the third decade of life, and False Negatives elevated after the seventh decade.6 Therefore, portable, tablet (iPad) based tests and virtual reality (VR) headset based perimetry are gaining popularity as an alternative form of VF testing. Tablet perimetry has the potential to be used as a low-cost method for glaucoma screening. Tablet based perimetry has become possible as the newer tablets have a high spatial resolution, large dynamic luminance range and 8-bit luminance control, that makes them suited for this purpose.7,8
Additionally, the ongoing coronavirus pandemic has highlighted the need for sanitisation of all ophthalmic equipment, in the interest of patient safety. The guidelines given by the American Academy of Ophthalmology highlight the importance of following manufacturer’s instructions for disinfection between patients. The makers of HFA warn against the risk of damage to the Ganzfield bowl because of the rubbing motion against the surface. It is recommended to use an atomizing sprayer followed by allowing a full 10 to 15 minutes to let it dry.9 Haag-Streit, makers of Octopus, suggest that frequent use of even an atomizer spray can cause damage to the bowl surface.10 Disinfection procedures for an iPad/tablet is simple as the surface can be wiped without causing damage to the screen.
The current review focuses on evaluating glaucoma detection sensitivities, diagnostic abilities and correlation of each parameter and examination time of the iPad based perimetry applications with those of HFA.
Visual Field Easy
The first, free iPad (Apple, Cupertino, CA) suprathreshold perimetric screening application was the Visual Field Easy (VFE) application [https://itunes.apple.com/us/app/visualfields-easy/id495389227]. It is a “free of cost” application, requiring purchase of only an iPad. The VFE program tests 96 visual field locations within the central 30 degrees, using a background luminance of 31.5 apostilbs (10 cd/m2), a size V target (when placed at a 33 cm test distance) and a 16 dB suprathreshold static perimetry target for screening purposes.
Studies using VFE have shown that it could detect only moderate and advanced visual field loss. Johnson and co-workers conducted a study in rural/suburban Nepal to evaluate the efficacy of VFE and compared it with the HFA 24–2 SITA standard test procedure. On the VFE application the missed locations correlated with the mean deviation (MD) (r = 0.79), pattern standard deviation (PSD) (r = 0.60), locations worse than the 95% confidence limits for total deviation (r = 0.51) and pattern deviation (r = 0.68) using SITA standard. iPad suprathreshold perimetry had greater difficulty in detecting early VF deficits (MD < –6 dB) but could detect most VF deficits with moderate (MD: −6 to −12 dB) and advanced (MD > −12 dB) loss, due to high false positivity.11
In another prospective study conducted by Ichhpujani et al, 210 eyes (60 normal and 150 glaucomatous) were tested using the VFE and the results were compared with HFA 24–2 SITA standard program.12 On correlating the missed points, for mild glaucoma, missed points were 37.5, sensitivity and specificity were 77.8% and 52.6%, respectively. For moderate glaucoma, missed points were 33.5, sensitivity was 90% and specificity was 48% while for severe glaucoma, missed points were 23, both sensitivity and specificity improved to 97% and 70%, respectively. VFE was found to be not suitable as a rapid screening tool for community/mass screening of glaucoma as it cannot detect early and moderate glaucoma. Other limitations of this application cited by the authors included the smudging of the screen due to repeated display touch by the subjects leading to an altered contrast of the target but this can now be overcome by the use of a Bluetooth linked keyboard with the iPad.
The VFE incorporates a large number of test positions (96), and it remains to be shown whether all of these locations are needed for the optimal performance of the application. Additionally, it needs a parser code to get the missed point data, thus making the data analysis slightly impractical for day-to-day use.
Kitayama et al compared VFE with Humphrey Frequency Doubling Technology (FDT) N-30-5 for detecting abnormal visual fields in a health fair setting for community screening of high-risk Latino adults.13 VFE testing took on average 141 seconds longer per eye than FDT and FDT resulted in 7.50% more missed points than VFE (p = 0.002). For VFE, they reported a sensitivity and specificity of 67% and 77%, respectively, with an area under the receiver operator curve (ARUC) of 0.71. Agreement between FDT and VFE was greater for patients with mild-to-moderate visual field loss.
Melbourne Rapid Field
Melbourne Rapid Field (MRF) (GLANCE Optical Ltd, Melbourne, Australia) is an iPad-based application approved by the FDA as a class 1 device. It has been validated as a tangent perimeter. MRF, is an improved thresholding version of the VFE, developed by the same research group as VFE.
In the current version of the app, the iPad luminance output is calibrated automatically by the MRF software before starting the test. The MRF assessment can be done in two modes, a full threshold test and a screening test. Full-threshold module has been evaluated in several studies.
The screening module was derived from the full-threshold MRF test using minimum required suprathreshold intensity at each test location. The full threshold version of MRF uses a modified 24–2 grid or a full test centred at fixation, which tests 66 points in the 30° × 20° of the VF, equivalent to the HFA 24–2 program. Initially, the central field is tested (36 points tested with fixation in the center of the screen) followed by the peripheral field (30 test points). As the screen size is small, subtending around 15° × 12°, the patient must fixate on all the four corners of the iPad screen at different times to cover the entire 30°. Fixation changes during testing for 9.7 inch, 10.5 inch and 11 inch iPads.14 Patients wear their near correction while taking the test. Targets are presented for 300 milliseconds. The thresholding strategy is started with a 17 dB stimulus and uses a three-presentation binary Bayesian protocol to yield eight steps (0, 3, 6, 12, 17, 22, 26, and 30 dB) across the 30 dB range (Zippy Estimation by Sequential Testing, ZEST). More intermediate points adjacent to a detected area of scotoma are also tested.15,16 This contrasts with the SITA algorithms, which use a post hoc Bayes prediction returned from 4 dB step (as in SITA-fast) or 4–2 dB (as in SITA-standard). In the test printout, color-coded indicators appear; “Green” refers to within normal limits (95% of normals), “Amber” refers to borderline (<5% of normals), and “Red” indicates outside normal limits (<1% of normals). Additionally, the test spot size increases into the periphery (from Size III to Size IV) and this is expected to reduce variability of outcome.
Although head-to-head comparison between MRF and HFA should be interpreted carefully as both use entirely different test paradigms, still since the output is similar in terms of global indices and regional threshold values, researchers have compared the two tests.
Schultz et al examined the validity of MRF testing with HFA 24–2 SITA standard. They recruited 60 glaucoma patients; where 17 had pre-perimetric glaucoma and 43 had manifest VF defects. All patients found the MRF test easy to use with mean test duration of 4 minutes 16 seconds ±1 minute 8 seconds vis-a-vis HFA test duration of 5 minutes 44 seconds ± 1 minute 1 second MRF performed well in terms of VF abnormality detection in comparison to HVF. For the MRF, MD, PSD, and Visual Field Index (VFI) it showed good overall performance for sensitivity and specificity with ARUC values of 0.84 for MD, 0.81 for PSD and 0.85 for VFI. AUC values for MD (0.85) and VFI (0.88) were significantly comparable to those obtained with HFA, whilst the difference between the devices was noted for PSD (0.81 for MRF and 0.93 for HFA).15 The authors noted that although some early cases were not picked by MRF, it provided additional information in some cases, as there are several additional test points in the central field (similar to a 10–2 strategy). This fact needs to be explored in larger studies with early glaucoma.
The point to point reproducibility of threshold values with MRF was less in cases with manifest glaucoma vis-à-vis HFA. This can be explained by the fact that during the MRF test the patient has to change fixation points four times to four corners of the iPad screen, unlike the solitary, conventional central fixation for the HFA.14 These multiple fixation shifts are likely to contribute to increased variability in threshold. For improving reliability of outcome, a headrest was be used by the authors. But screen malalignment and tilting can cause issues with variation of luminance.16
Vingrys et al validated that at numerous test locations the MRF application accomplished fast thresholding within 30 degrees of fixation. MRF perimetry has adequate potential to find early defects which have MD values smaller than 3.3 dB.8 In another study, Kong et al studied correlation between the perimetric outcomes from MRF application and those from the HFA in 90 subjects. They found that the test durations were longer on HFA than MRF (6.3 ± 0.1 minutes versus 5.7 ± 0.1 minutes, p < 0.001). Intraclass coefficient (ICC) was 0.93 for MD and 0.86 for PSD, HFA giving more negative MD (1.4 dB bias) than MRF. MRF Test 1 and Test 2 results were correlated with test-retest reliability of HFA SITA-standard, with MRF having an ICC of 0.93 for MD and 0.89 for PSD and HFA showing an ICC of 0.95 for MD and 0.90 for PSD.16 There was a high level of concordance in outcomes and the test-retest reliability of MRF was also found to be comparable to HFA.17
Prea et al enrolled 60 patients (stable ocular hypertensives as well as glaucoma patients on treatment and glaucoma suspects) from two clinical sites to establish MRF applications medium-term repeatability compared to HFA 24–2 SITA-standard and SITA-fast programs. MRF was found to have a better coefficient of repeatability (8.1%) than both SITA-fast (17.9%, p = 0.001) or SITA-standard (12.2%, p = 0.02). Results showed MRF was faster than SITA-standard (mean test duration of MRF being 4.6 ± 0.1 minutes versus mean test duration on SITA-fast 4.3 ± 0.2 minutes versus SITA-standard mean test duration being 6.2 ± 0.1 minutes, p < 0.001) and was similar to SITA-fast in terms of speed.18 The authors also found that although the global MD of the MRF compared well to the MD of both SITA-standard and SITA-fast tests, the tests did not have concordance on a point-wise or regional basis.
Kumar et al compared VF using MRF and HFA in 28 eyes of glaucoma patients. Mean test times were 342.07 ± 56.70 seconds for MRF and 375.11 ± 88.95 seconds for HFA 24–2 SITA standard (p: −0.046).19 Mean MD was significantly lower for MRF (Δ-3.09, p < 0.001), and mean PSD was significantly higher for MRF (Δ-1.40, P-0.005) compared with HFA. The mean foveal threshold for the MRF was significantly lower than the mean HFA foveal threshold (Δ-9.25, p < 0.001). The number of points depressed at p < 5% on the PSD probability plot was significantly less for MRF (p < 0.001). Other perimetric outcomes showed no significant differences between both. They concluded that MRF is a cost-effective, time-saving as well as user-friendly tool for monitoring visual fields in settings where access to traditional perimetry is limited. However, the lack of internet connectivity/strength in rural areas and questionable detection of early damage are potential cons.
In a recent study conducted at Tema (low-resource setting) in Ghana by Prince et al, the performance of the MRF was evaluated. For glaucoma patients, MD and PSD from the HFA and MRF correlated strongly (r = 0.84; p < 0.001) and moderately (r = 0.61; p < 0.001), respectively. On agreement analysis, MRF generated significantly higher PSD values (bias, 1.9 ± 2.8 dB; p = 0.03) and MD (bias, 3.3 ± 4.1 dB; p = 0.03), with wide limits of agreement. Significant agreement biases suggested a weak agreement between the MRF and HFA.
For detecting moderate to advanced glaucoma, the sensitivity and specificity was 60.9% and 86.5% for the MRF while for HFA sensitivity was 78.3% and specificity was 83.8%.20
Prea et al studied the short-term uptake, compliance, and performance of a tablet device (using MRF) for home monitoring of visual field by glaucoma patients. The uptake of home monitoring was good to the tune of 88% and high correlation was noted for the MD between in-clinic (HFA) and at-home (MRF) outcomes (R = 0.85). They found that information technology logistical reasons, lack of motivation, and/or competing life demands were the chief barriers to uptake and compliance of app-based home testing.21
Prea, Kong and Vingrys reported a 12 month home-monitoring trial using MRF for glaucoma patients and showed MRF to be similar to HFA Guided Progression Analysis (GPA) for detecting progression in glaucoma cases. The benefit of the home monitoring process was that the volume of testing (weekly) allowed detection of change in those patients who progressed in under 3 months compared with GPA which took 30 months for the same outcome.22
One of the disadvantages with MRF for home monitoring is nonavailability of Size V stimulus which results in some patient discomfort due to the need for appropriate positioning.
Peristat Online Perimetry
Peristat online perimetry (POP) was first developed in 2002 by two resident doctors of Doheny Eye Institute (University of Southern California), Dr Ianchulev and Dr Peter Pham.
POP is delivered via the KYS telemedicine platform (https://kysvision.com/peristat-test/).
POP allows perimetry testing of up to 24° of VF from fixation horizontally and 20° vertically using four levels of standardized threshold stimuli. POP testing is performed with dimmed ambient light and no direct light sources over the screen. The Red Green Blue range for the target is between 64 and 225 with a differential light intensity between 30 and 300 lux. Target is presented for 0.2 seconds, and an additional grace period of 1.8 seconds is given to the patient to respond. The appropriate working distance is determined by adjusting positioning until the flashing light temporal to the fixation point disappears in the blind spot. Gaze fixation assurance and false-positive/false-negative registration is also present. Patient responses can then be composed into a grayscale visual field image. Earlier, POP was available for use by any patient across the globe, but now it is available only for registered practices in the United States.
In a prospective study conducted by Ianchulev et al, 58 eyes of 33 patients underwent POP and HVF and their scores were compared. All the patients were able to complete the test with no difficulty within 2 to 5 minutes (longer test time in patients with severe defects). There was a high degree of correlation between the Peristat and the HFA. The sensitivity of Peristat for mild to severe HVF defects exceeded 80% with a specificity around 94%. They observed that more than 70% of the disparity was due to the Peristat false negatives, signifying that Peristat is unable to register very early defects in the far periphery of the test range. When the mild defects were excluded from the study, both the sensitivity and specificity increased.23
Lowry et al, compared the two modalities among 77 glaucoma patients in a clinic-based setting. POP and HFA abnormal points highly correlated with Spearman rank correlations ranging from 0.55 to 0.77 (all p < 0.001). They also plotted the curve to test the ability of Peristat to identify the severity of glaucoma. There was no significant difference between the AUC of the three receiver operating characteristics curves (ie, −16.7, −21.7, or −26.7 dB) for distinguishing mild or worse glaucoma versus controls (p = 0.36) or moderate or worse glaucoma from the combined controls and mild glaucoma patients (p = 0.75, χ2 test). They concluded that the number of abnormal points correlated significantly among both the tests and Peristat exhibited a significant correlation with the 24° HFA.24
Visual Field Fast
The “Visual Field Fast” (VFF) application draws its inspiration from noise field campimetry or snowfield perimetry, wherein the entire VF is simultaneously tested by confronting patients with a screen of randomly flickering, black and white stimulus.
“Visual Field Fast” (VFF) (Leonard Yip, Apple App Store), is available for free on the Apple App Store and operates on any iPad running iOS 10.0 or higher. VFF covers the same VF area as the HFA 24–2 assessment. For performing perimetry using the VFF app an iPad with a 9.7 inch screen is used in a dark room with all light sources switched off (<0.1 Lux). The screen brightness of the app is recommended to be set to auto-brightness mode (5 cd/m2). The test is performed at 33 cm using near correction. Patients can perceive scotomas as zones of abnormal flickering in terms of colour and frequency and delineate the scotomas using the touch screen for automated quantification of the VF loss.25
Eyecatcher
Eyecatcher is an open-source eye-movement perimeter. The Goldmann Size III stimuli are displayed on a Windows tablet computer (not on iPad) and the eye movements are recorded using a Tobii EyeX eye-tracker (Tobii Technology, Stockholm, Sweden). This is a low cost, near infrared, remote eye tracker which allows a precision of >0.6 degrees. There is no response button or central fixation target. A target comparable to Goldman Size III is presented on a 24–2 grid, against a 10 cd/m2 white background. Patient’s receive a visual feedback (a confirmation flashing dot) confirming the true stimulus location after each button press. The output from Eyecatcher is a retinotopic map, giving the probability of seeing the target at 22 paracentral locations. A summary measure of performance is computed by mean-averaging the probability-of-seeing values across all 22 test locations. The resultant metric is “mean hit rate”, which is a scalar value between 0 and 1 (reflects the amount of “greenness” in the VF plot). Mean hit rate is potentially comparable to MD of HFA.26
The complete source code for Eyecatcher is available online at https://github.com/petejonze/Eyecatcher. The codebase in principle supports iOS, but the latest version of Eyecatcher will work on an Android system.
Jones et al conducted a study to compare the results of eyecatcher with SAP using HFA in subjects with glaucoma and healthy age matched controls. They observed that the application was clearly able to distinguish between the glaucomatous and healthy eyes and also between eyes with mild and severe impairment. The results were consistent with SAP. The eyecatcher scores strongly correlated with MD (r2 = 0.64, p < 0.0001), and there was good concordance between corresponding VF locations (~84%). In a single eye analysis the test was also able to localise scotomas with a reasonable spatial precision. The test was found to be more user friendly than SAP using HFA.26
A disadvantage noted by the authors was the inability to track eye movements in eyes with very high refractive error through thick lenses. Thick lenses restrict spatial range as majority of the stimuli are presented within ± 15 degrees horizontally and ± 9 degrees vertically.
Jones et al conducted another study to assess the accuracy and adherence of VF home monitoring in 20 glaucoma patients using the Eyecatcher application over a period of six months. They found a good concordance between VFs measured at home and in the clinic (r = 0.94, p < 0.001). Data from 6 home-monitoring tests correlated well with the in-office SAP. In 21 of 236 tests (9%) MD deviated by more than ±3 dB from the median. These anomalous tests could be identified by applying machine learning techniques to recordings from the tablets’ front-facing camera.27
Eyecatcher can be used as a “rapid triage” tool to screen glaucoma in the community and waiting areas in hospitals to screen glaucomatous eyes from healthy ones and false positive referrals having no VF or optic nerve damage. Further studies are required to ascertain the boundaries for this test and to ascertain its role as a home-monitoring tool. Currently, due to the absence of a photometrically calibrated display, the test is not available as a downloadable “app” for all.28 Basic parameters of available applications (Apps) for tablet perimetry are elucidated in Table 1.
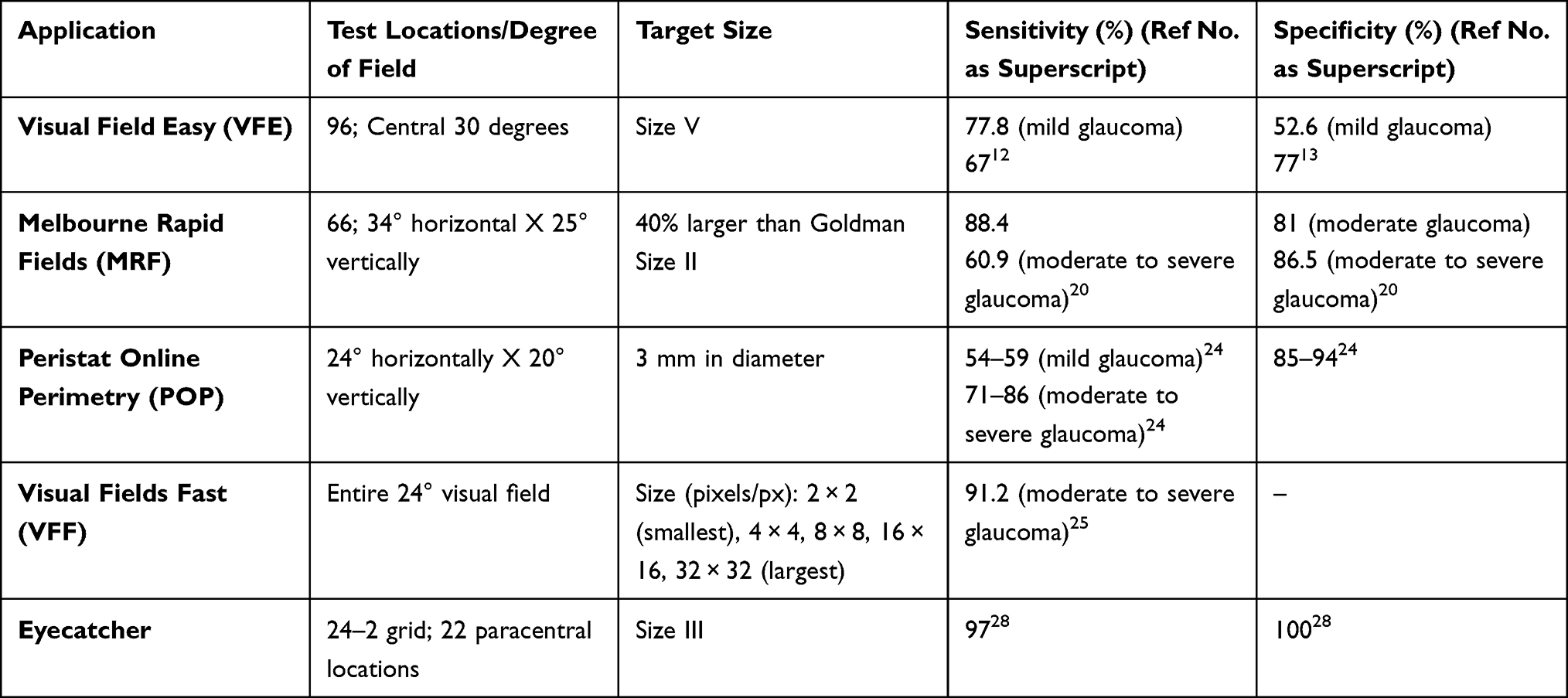 |
Table 1 Basic Parameters of Available Applications (Apps) for Tablet Perimetry |
iPad (tablet) based perimetry can allow for more datapoints for monitoring of glaucoma as patients can test their visual function in home settings, avoiding travel and waiting time in busy clinics.29 Additionally, since the tests are less time consuming, it reduces the element of fatigue in elderly and debilitated patients as many of them have arthritic problems which makes repeatedly pressing a button difficult.
To conclude, tablet perimetry is a promising tool for tele-glaucoma care, but the sensitivity and specificity of the currently available applications for glaucoma detection is insufficient for stand-alone screening. When combined with other risk factors such as optic nerve appearance using portable non-mydriatic fundus photography, as well as clinical and demographic risk factors such as age, IOP, and family history of glaucoma when available, the sensitivity, specificity, and positive predictive value of app-based perimetry tests can be improved.29
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kang JM, Tanna AP. Glaucoma. Med Clin North Am. 2021;105(3):493–510. doi:10.1016/j.mcna.2021.01.004
2. European Glaucoma Society. Terminology and Guidelines for Glaucoma.
3. Bosworth CF, Sample PA, Johnson CA, Weinreb RN. Current practice with standard automated perimetry. Semin Ophthalmol. 2000;15(4):172–181. doi:10.3109/08820530009037869
4. Kutzko KE, Brito CF, Wall M. Effect of instructions on conventional automated perimetry. Invest Ophthalmol Vis Sci. 2000;41(7):2006–2013.
5. Marra G, Flammer J. The learning and fatigue effect in automated perimetry. Graefes Arch Clin Exp Ophthalmol. 1991;229(6):501–504. doi:10.1007/BF00203309
6. Shirakami T, Omura T, Fukuda H, Asaoka R, Tanito M. Real-world analysis of the aging effects on visual field reliability indices in humans. J Clin Med. 2021;10(24):5775. doi:10.3390/jcm10245775
7. Turpin A, Lawson DJ, McKendrick AM. PsyPad: a platform for visual psychophysics on the iPad. J Vis. 2014;14(3):16. doi:10.1167/14.3.16
8. Vingrys AJ, Healey JK, Liew S, et al. Validation of a tablet as a tangent perimeter. Transl Vis Sci Technol. 2016;5(4):3. doi:10.1167/tvst.5.4.3
9. Meditec CZ. Cleaning guidance for the Humphrey field analyzer. Available from: http://www.zeiss.com.
10. Diagnostics H-S. Cleaning and disinfection of octopus perimeters. Available from: http://www.haag-streit.com.
11. Johnson CA, Thapa S, George Kong YX, Robin AL. Performance of an iPad application to detect moderate and advanced visual field loss in Nepal. Am J Ophthalmol. 2017;182:147–154. doi:10.1016/j.ajo.2017.08.007
12. Ichhpujani P, Thakur S, Sahi RK, Kumar S. Validating tablet perimetry against standard Humphrey visual field analyzer for glaucoma screening in Indian population. Indian J Ophthalmol. 2021;69(1):87–91. doi:10.4103/ijo.IJO_1847_19
13. Kitayama K, Young AG, Ochoa A
14. Appview Technologies. c2019. FAQ. Available from: https://www.appviewmrf.com/faq/.
15. Schulz AM, Graham EC, You YY, Klistorner A, Graham SL. Performance of iPad-based threshold perimetry in glaucoma and controls. Clin Exp Ophthalmol. 2018;46(4):346–355. doi:10.1111/ceo.13082
16. Kong YXG. Visual field testing in the era of portable consumer technology. Clin Exp Ophthalmol. 2018;46(4):325–326. doi:10.1111/ceo.13308
17. Kong YX, He M, Crowston JG, Vingrys AJ. A comparison of perimetric results from a tablet perimeter and Humphrey field analyzer in glaucoma patients. Transl Vis Sci Technol. 2016;5(6):2. doi:10.1167/tvst.5.6.2
18. Prea SM, Kong YXG, Mehta A, et al. Six-month longitudinal comparison of a portable tablet perimeter with the Humphrey field analyzer. Am J Ophthalmol. 2018;190:9–16. doi:10.1016/j.ajo.2018.03.009
19. Kumar H, Thulasidas M. Comparison of perimetric outcomes from Melbourne rapid fields tablet perimeter software and Humphrey field analyzer in glaucoma patients. J Ophthalmol. 2020;2020(8384509):1–9. doi:10.1155/2020/8384509
20. Prince J, Thompson A, Mwanza JC, Tolleson-Rinehart S, Budenz DL. Glaucoma screening using an iPad-based visual field test in a West African Population. Ophthalmol Glaucoma. 2021;5(3):275–283. doi:10.1016/j.ogla.2021.09.002
21. Prea SM, Kong GYX, Guymer RH, Vingrys AJ. Uptake, persistence, and performance of weekly home monitoring of visual field in a large cohort of patients with glaucoma. Am J Ophthalmol. 2021;223:286–295. doi:10.1016/j.ajo.2020.10.023
22. Prea SM, Kong G, Vingrys AJ. Visual field home-monitoring with a tablet perimeter by glaucoma patients.Invest. Ophthalmol. Vis. Sci. 2022;63(7):4381–A0424.
23. Ianchulev T, Pham P, Makarov V, Francis B, Minckler D. Peristat: a computer-based perimetry self-test for cost-effective population screening of glaucoma. Curr Eye Res. 2005;30(1):1–6. doi:10.1080/02713680490522399
24. Lowry EA, Hou J, Hennein L, et al. Comparison of peristat online perimetry with the Humphrey perimetry in a clinic-based setting. Trans Vis Sci Tech. 2016;5(4):4. doi:10.1167/tvst.5.4.4
25. Ding J, Tecson IC, Ang BCH, Chiew W, Chua C, Yip LWL. The performance of iPad-based noise-field perimeter versus Humphrey field analyser in detecting glaucomatous visual field loss. Eye. 2021;20:1–12.
26. Jones PR, Smith ND, Bi W, Crabb DP. Portable perimetry using eye-tracking on a tablet computer-A feasibility assessment. Transl Vis Sci Technol. 2019;8(1):17. doi:10.1167/tvst.8.1.17
27. Jones PR. An open-source static threshold perimetry test using remote eye-tracking (Eyecatcher): description, validation, and preliminary normative data. Transl Vis Sci Technol. 2020;9(8):18. doi:10.1167/tvst.9.8.18
28. Jones PR, Lindfield D, Crabb DP. Using an open-source tablet perimeter (Eyecatcher) as a rapid triage measure for glaucoma clinic waiting areas. Brit J Ophthalmol. 2021;105:681–686. doi:10.1136/bjophthalmol-2020-316018
29. Krishnadas R. Commentary: evolving role of portable visual field testing in communities. Indian J Ophthalmol. 2021;69(1):92–93. doi:10.4103/ijo.IJO_731_20
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Virtual Reality Visual Field Testing in Glaucoma: Benefits and Drawbacks
Babel AT, Soumakieh MM, Chen AY, Wong C, R da Costa D, Almeida DR
Clinical Ophthalmology 2025, 19:933-937
Published Date: 17 March 2025
Assessment of Visual Function Using Yellow-Tinted Filter in Patients with Pre-Perimetric and Early Open Angle Glaucoma
Triantafyllopoulos GI, Karabatsas CH, Pateras E, Chandrinos A, Kapralos D, Georgiou I, Tsiogka A, Kourkoutas D
Clinical Optometry 2025, 17:255-268
Published Date: 18 August 2025