Back to Journals » Vascular Health and Risk Management » Volume 16
Spotlight on Icosapent Ethyl for Cardiovascular Risk Reduction: Evidence to Date
Authors Jia X, Koh S ![]() , Al Rifai M
, Al Rifai M ![]() , Blumenthal RS, Virani SS
, Blumenthal RS, Virani SS ![]()
Received 3 November 2019
Accepted for publication 28 December 2019
Published 9 January 2020 Volume 2020:16 Pages 1—10
DOI https://doi.org/10.2147/VHRM.S210149
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Pietro Scicchitano
Xiaoming Jia,1,* Stephanie Koh,1,* Mahmoud Al Rifai,1 Roger S Blumenthal,2 Salim S Virani1,3,4
1Section of Cardiology, Department of Medicine, Baylor College of Medicine, Houston, TX, USA; 2The Johns Hopkins Ciccarone Center for the Prevention of Cardiovascular Disease, Baltimore, MD, USA; 3Health Policy, Quality & Informatics Program, Michael E. DeBakey Veterans Affairs Medical Center Health Services Research and Development Center for Innovations, Houston, TX, USA; 4Section of Cardiology, Michael E. DeBakey Veterans Affairs Medical Center, Houston, TX, USA
*These authors contributed equally to this work
Correspondence: Salim S Virani
Health Services Research and Development, Michael E. DeBakey Veterans Affairs Medical Center, 2002 Holcombe Boulevard, Houston, TX 77030, USA
Tel +1 713-440-4410
Email [email protected]
Abstract: Icosapent ethyl is a highly purified formulation of eicosapentaenoic acid, a type of omega-3 fatty acid contained in fish oil. While omega-3 fatty acids have long been thought to have cardioprotective benefits, the Reduction of Cardiovascular Events with EPA-Intervention Trial (REDUCE-IT) has helped to establish icosapent ethyl as an evidence-based therapy for risk reduction of atherosclerotic cardiovascular disease (ASCVD). REDUCE-IT, however, was by no means an overnight success story. Close examination of the evidence shows that the trial was a culmination of many lessons learned from previous studies. The purpose of this manuscript is to review contemporary evidence of icosapent ethyl in ASCVD risk reduction and the clinical implication of this promising therapy.
Keywords: omega-3 fatty acids, icosapent ethyl, eicosapentaneoic acid, cardiovascular outcome
Introduction
Icosapent ethyl is a highly purified formulation of eicosapentaenoic acid (EPA), which is a type of omega-3 fatty acid found in fish oil. In the Reduction of Cardiovascular Events with EPA-Intervention Trial (REDUCE-IT) trial, treatment with icosapent ethyl was shown to be associated with significant reduction in risk for atherosclerotic cardiovascular disease (ASCVD) events in secondary prevention and high-risk primary prevention patients with diabetes and elevated triglycerides but well-controlled low-density lipoprotein cholesterol (LDL-C) on optimal statin therapy. While omega-3 fatty acids have long been thought to have cardioprotective benefits, results of randomized controlled trials examining cardiovascular outcomes prior to REDUCE-IT have been inconsistent and mostly negative, especially in the era of statin therapy. What set the REDUCE-IT trial apart was likely the utilization of a higher dose of purified EPA formulation in combination with strategic patient selection that reflects mounting evidence supporting elevated triglycerides (TGs) as an important marker of increased residual ASCVD risk.
Since the publication of REDUCE-IT, several clinical practice guidelines, including those of the American Diabetes Association (ADA), National Lipid Association (NLA) and the European Society of Cardiology (ESC)/European Atherosclerosis Society (EAS), have endorsed the use of icosapent ethyl in their recommendations to further reduce ASCVD risk in select patients. Meanwhile, research is ongoing to further investigate mechanism of action, implementation and cost-effectiveness as well as the efficacy and safety of related therapies. The aim of this manuscript is to review contemporary evidence of icosapent ethyl in ASCVD risk reduction with a focus on the clinical implication of this promising therapy.
From Fish-to-Fish Oil: A Historical Context
Populations with high fish consumption have been associated with lower cardiovascular risk through various mechanisms. Long-chain n-3 polyunsaturated fatty acids (n-3 PUFA) in fish oil include eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA). In pre-clinical studies, these fatty acids are associated with cardiovascular benefit through altering cell membrane fluidity by integration into cell membrane, acting on ion channels to produce anti-arrhythmic and anti-inflammatory effects, and regulating gene expression.1–3 However, these findings have not been directly validated in large clinical studies. EPA and DHA lower serum TGs in a dose-dependent manner, with higher doses (3 to 4 g/day) leading to higher reductions in TGs.4 Mendelian randomization studies suggest that triglyceride-rich lipoproteins, especially very low-density lipoprotein (VLDL) and their remnants, are causally associated with atherosclerotic cardiovascular disease (ASCVD).5–7 Thus, elevated triglycerides are thought to be a marker of at least some of the residual risk in patients with optimized LDL-C on statin therapy. Yet, addressing this residual risk in ASCVD likely necessitates strategies beyond simply targeting TGs, as older triglyceride-lowering therapies such as fibrates and niacin have not shown to improve cardiovascular outcomes.8,9
EPA Effects on Lipids, Lipoproteins and Markers of Inflammation
Omega-3 FA agents are known to reduce TGs and have been used for the treatment of hypertriglyceridemia. Prior to icosapent ethyl, fish oil prescriptions available contained a combination of EPA and DHA. However, findings from previous studies found that DHA may increase LDL-C levels while EPA did not.10 One important rationale for using a formulation of EPA without DHA in the treatment of hypertriglyceridemia was therefore to avoid the undesired side effect of increased LDL-C, a known causal risk factor for ASCVD.
Two Phase III studies, The Efficacy and Safety of AMR101 (Ethyl Icosapentate) in Patients With Fasting Triglyceride (Tg) Levels ≥ 500 and ≤ 2000 mg/dL (MARINE) and Effect of AMR101 (Ethyl Icosapentate) on Triglyceride (TG) Levels in Patients on Statins With High Tg Levels (≥200 and <500 mg/dL) (ANCHOR), assessed the efficacy of icosapent ethyl in reducing TG among patients with very high and high TG levels11,12 (Table 1). In the MARINE trial, patients with fasting TG levels ≥500 and ≤2000 mg/dL were randomized 1:1:1 to receive icosapent ethyl 4g/day (baseline TG 680 mg/dL), 2g/day (baseline TG 657 mg/dL) and placebo (baseline TG 703 mg/dL). The median baseline LDL-C of the study population was 86.0 mg/dL (measured directly) and 25% of patients were on a statin. After 12 weeks, treatment with icosapent ethyl 4g/day and 2g/day resulted in the reduction of TG levels by 33.1% (p<0.0001) and 19.7% (p=0051) respectively from baseline when compared with placebo. LDL-C levels did not significantly increase during the study period.
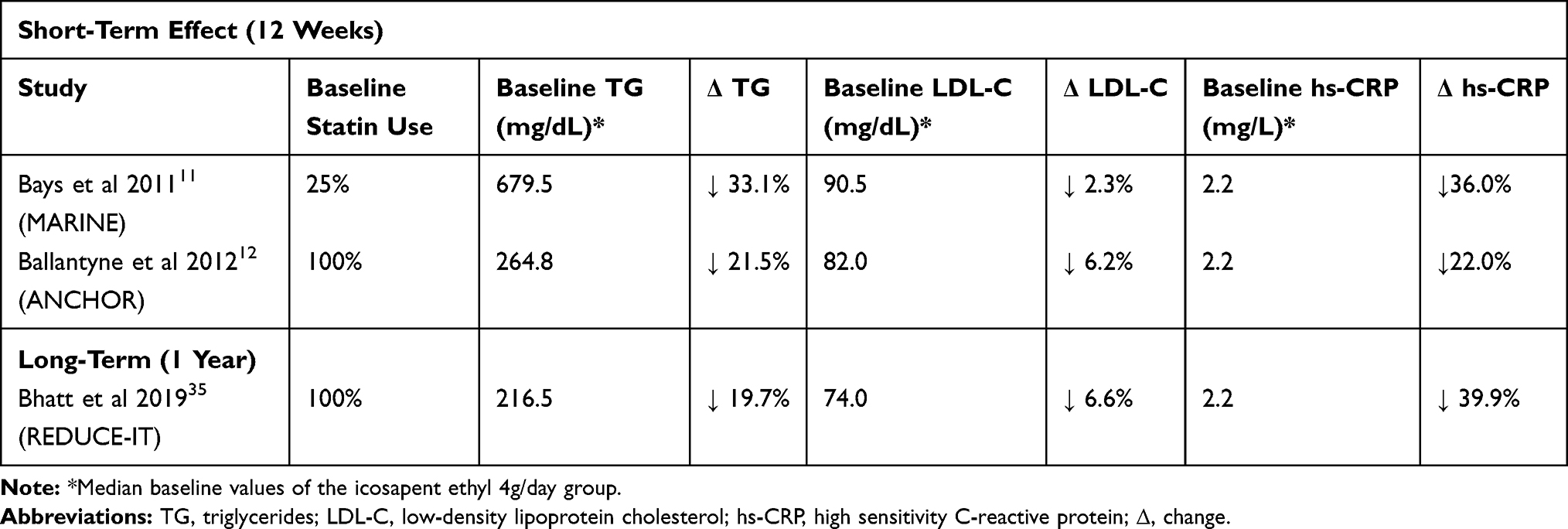 |
Table 1 Short-Term and Long-Term Effect of Icosapent Ethyl 4g/Daily Compared to Placebo on TGs, LDL-C and hs-CRP from the MARINE, ANCHOR and REDUCE-IT Trials |
Moreover, in the ANCHOR trial, 702 patients with TG level ≥200 and <500 mg/dL who were on stable statin regimens (with or without ezetimibe) with LDL-C ≥ 40 and < 100 mg/dL were randomized to receive either icosapent ethyl 4g/day, 2g/day or placebo. The median baseline TG level of the study population was 259 mg/dL, median LDL-C level was 83 mg/dL with 93.2% of patients taking either a moderate or high-intensity statin. At 12 weeks, treatment with icosapent ethyl reduced TG levels in a dose-dependent manner, respectively. Individuals in the icosapent ethyl 4g/day and 2g/day groups had at 21.5% (p<0.0001) and 10.1% (p=0.0005) decrease in TG levels from baseline compared to placebo. Furthermore, treatment with icosapent ethyl 4g/day significantly reduced VLDL-C (24.4%), LDL-C (6.2%), and apolipoprotein B (9.3%), when compared to placebo.
In subsequent exploratory analyses from MARINE and ANCHOR, icosapent ethyl 4g/day was also shown to reduce total particle concentration and VLDL size as well as levels of apolipoprotein CIII and remnant-like particle cholesterol.13–15 Data from genetic studies suggest that apolipoprotein CIII likely is casually associated with ASCVD.16 Other secondary analyses from these trials have further demonstrated that icosapent ethyl decreases inflammatory markers including high-sensitivity C-reactive protein (hs-CRP), oxidized LDL and lipoprotein-associated phospholipase A2 when compared with placebo.17–19 The above mechanisms may account for the effect of EPA on atherosclerosis. Studies have shown that treatment with EPA resulted reduction in the progression of carotid intima-media thickness and stabilization of vulnerable coronary plaques.20,21
Potential Mechanisms of Action of EPA
The mechanism of action by which icosapent ethyl reduces triglycerides and its effect on other lipids and lipoproteins is not fully understood. Both EPA and DHA reduce hepatic VLDL-TG production via interference of non-esterified fatty acid influx into the liver.22 Omega-3 FAs are also thought to prevent VLDL assembly and secretion by promoting degradation of apoB100 and upregulating beta-oxidation of free fatty acid in hepatocytes, resulting in a decrease in TG synthesis as well as an increase in VLDL-TG clearance by promoting upregulation of lipoprotein lipase (LpL) expression in adipose tissue; this may help to redirect fatty acids away from the liver towards peripheral tissue.23–26
During the post-prandial state, EPA and DHA have been shown to increase endothelial binding of chylomicron-like particles, stimulate increased circulating LpL activity and decrease secretion of ApoB48, all of which lead to a reduction in post-prandial lipemia. EPA-co-enzyme A esters have further been shown in animal studies to inhibit diacylglycerol acyltransferase, which directly reduces synthesis of TGs.27
In addition to its effect on circulating lipoprotein particles and lipids, EPA serves as the precursor for the omega-3 series of eicosanoids including prostaglandins, thromboxanes, leukotrienes, and protectins. Omega-3 derived eicosanoids are thought to have anti-inflammatory properties as opposed to omega-6 derived eicosanoids derived from arachidonic acid.28 EPA also serves as the substrate for E-series resolvins, which are a class of specialized pro-resolving mediators (SPMs). SPMs play an important role in counter-regulation of inflammation including in atherosclerosis.29,30 When incorporated into cell membranes, EPA confers membrane stability even in the setting of increased cholesterol load, which in turn imparts a protective effect against endothelial dysfunction.31 Moreover, higher concentration of EPA found in atherosclerotic plaques has been shown to be associated with less foam cells and a decrease in the expression of matrix metalloproteinases, which are thought to increase plaque stability.32
EPA Effects on Cardiovascular Outcomes (Table 2)
The first cardiovascular outcomes trial on EPA was the Japan EPA Lipid Intervention Study (JELIS) study published in 2007.33 JELIS was a prospective randomized open-blinded endpoint (PROBE) trial that assessed the efficacy of purified EPA 1.8g/day in the prevention of major coronary events (composite of sudden cardiac death, fatal and non-fatal myocardial infarction, and other non-fatal events including unstable angina pectoris and revascularization) among 18,645 Japanese patients with hypercholesterolemia. The mean baseline total cholesterol was 7.11mmol/L (275mg/dL) while the median baseline TG level was 1.73mmol/L (~153mg/dL) in the EPA group and 1.74mmol/L (~154mg/dL) for the control group. It should be noted that most patients in JELIS were treated with a low-intensity statin (either pravastatin 10mg daily or simvastatin 5mg daily).
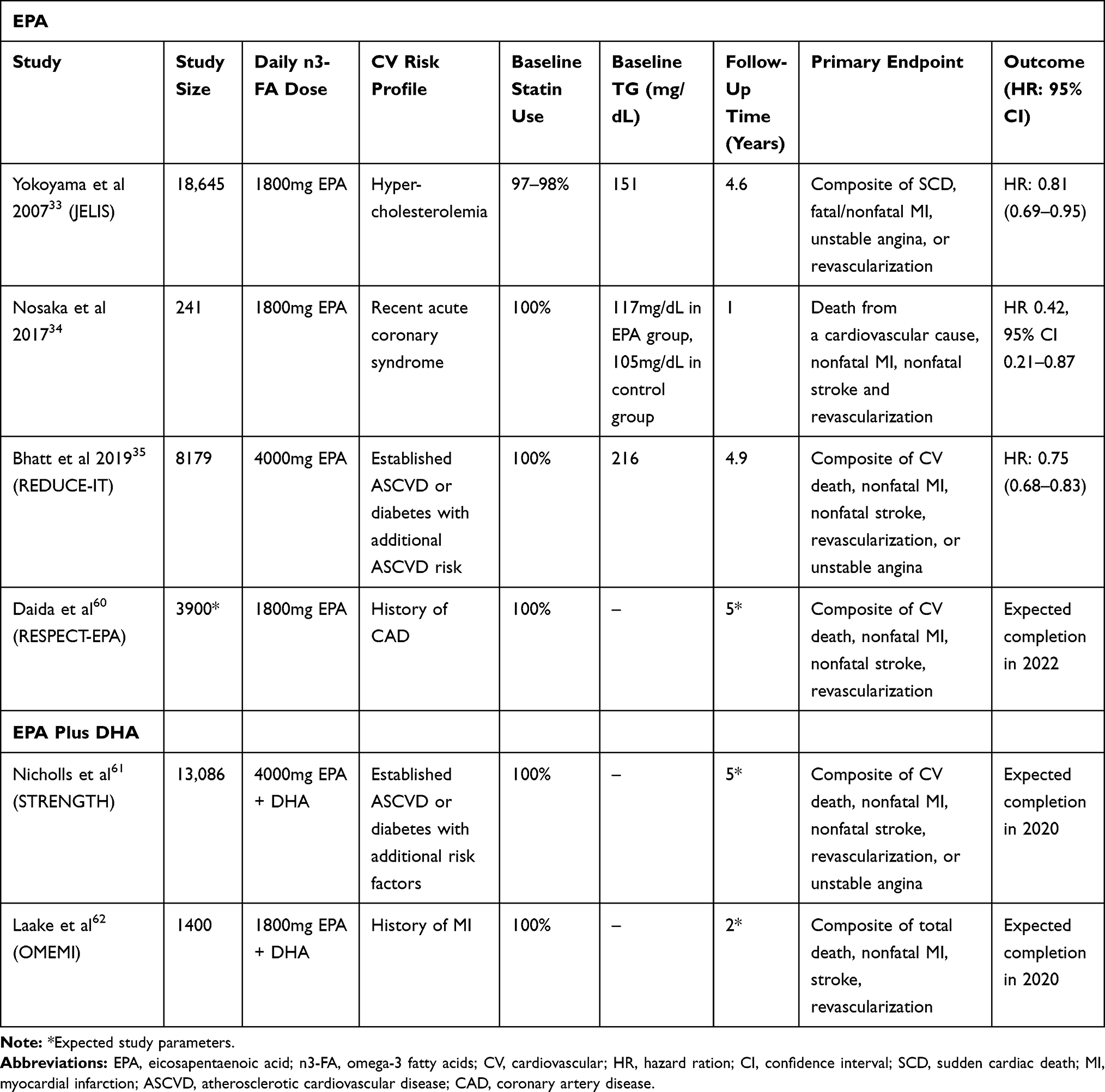 |
Table 2 Completed/Ongoing Cardiovascular Outcome Trials of High-Dose EPA and High-Dose EPA Plus DHA |
At a median follow-up of 4.6 years, the primary endpoint occurred in 2.8% of patients in the EPA group vs 3.5% of patients in the control group (HR 0.81, 95% CI 0.69–0.95, p=0.011). Treatment with EPA resulted in a modest but significant reduction in TG levels (9% from baseline in the EPA group vs 4% in controls, p<0.0001) with no differences in the reduction of LDL-C. It is important to note that JELIS was an open-label study and that there was no placebo. Furthermore, while there was a significant reduction in the primary composite outcome, subgroup analyses from JELIS, there was not a significant reduction observed in individual endpoints except reduction in unstable angina.
A smaller, single-centered Japanese trial, utilizing PROBE design, of 241 patients with acute coronary syndrome has also been reported. Patients were randomized 1:1 to receiving either pitavastatin 2mg/day plus purified EPA 1.8g/day vs pitavastatin 2mg/day alone (control) within 24 hrs of undergoing percutaneous coronary intervention. The baseline TG was 117mg/dL in EPA group and 105mg/dL in control group. After 1 year, individuals treated with statin plus EPA had lower rates of primary endpoint (including death from a cardiovascular cause, nonfatal MI, nonfatal stroke and revascularization) compared with those receiving statin alone (9.2% vs 20.2%, HR 0.42, 95% CI 0.21–0.87, p=0.02). Cardiovascular-related death was also significantly lower in the EPA treated group compared to the control group (0.8% vs 4.2%, p=0.04).34
Building upon the findings of the previous trials, REDUCE-IT was a multi-centered, double-blinded, randomized placebo-controlled trial of 8,179 participants evaluating the efficacy and safety of icosapent ethyl 2g twice daily compared to mineral oil as placebo.35 It should be noted that though the dose of EPA in REDUCE-IT was higher than in JELIS; a previous analysis showed that circulating EPA levels were similar between a daily dose of 4g in a western population compared to the 1.8g daily dose in the Japanese population in JELIS due to very high background dietary intake of omega-3 fatty acids in the latter.36
Individuals included in REDUCE-IT had either established ASCVD or diabetes mellitus with additional ASCVD risk factors, had elevated fasting TG levels but relatively well-controlled LDL-C levels on maximally tolerated statin therapy (~93% of the patients were on either moderate or high-intensity statin therapy). The median baseline TG levels were 216.5 mg/dL and 216.0 mg/dL in the icosapent ethyl and placebo groups, respectively. Median baseline LDL-C levels were 74 mg/dL and 76 mg/dL, respectively. The primary endpoint was a composite of cardiovascular death, non-fatal MI, nonfatal stroke, coronary revascularization or unstable angina requiring hospitalization. The median follow-up period was 4.9 years.
Individuals treated with icosapent ethyl had lower rates of primary endpoint events compared to placebo (mineral oil), 17.2% vs 22.0% (ARR=4.8%; HR 0.75; 95% CI, 0.68–0.83; p<0.001). Moreover, there was also significant reduction in individual components of the primary endpoint including cardiovascular death (HR 0.80; 95% CI, 0.66–0.98; p=0.03; ARR=0.9%), fatal or non-fatal MI (ARR=2.6%; HR 0.69; 95% CI, 0.58–0.81; p<0.001), fatal or nonfatal stroke (ARR=0.9%; HR 0.72; 95% CI, 0.55–0.93; p=0.01), hospitalization for unstable angina (ARR=1.2%; HR 0.68; 95% CI, 0.53–0.87; p=0.002) and urgent or emergent revascularization (ARR=2.5%; HR 0.65; 95% CI, 0.55–0.78; p<0.001). The only individual outcome measure not significantly different between the icosapent ethyl and placebo groups was all-cause mortality (HR 0.87; 95% CI, 0.74–1.02).Secondary analysis from REDUCE-IT further showed that treatment with icosapent ethyl decreased the risk for not only the first primary endpoint event but also reduced the risk for developing subsequent major cardiovascular events.37 The relative risk reduction (RRR) of icosapent ethyl was 25% with respect to first primary endpoint events, 32% for second events, 31% for third events and 48% for fourth or more events. Compared to placebo, treatment with icosapent ethyl significantly reduced total ischemic events (first event plus subsequent events) (RR 0.70, 95% CI 0.62–0.78, p<0.0001). There was a relative risk reduction (RRR) for first events of 25%, second events of 32%, third events of 31% and fourth or more events of 48%.
REDUCE-IT results also demonstrated that icosapent ethyl exerted a significant long-term effect on lipids and inflammatory markers. The icosapent ethyl group had a 19.7% (−44.5 mg/dL) greater reduction in TG level at 1 year compared to placebo. At 1 year, the LDL-C increased by 3.1% in the icosapent ethyl group compared with 10.2% in the placebo group. The effect of TG and LDL-C persisted throughout the study. At last visit, the icosapent ethyl group had a reduction in TG level of 21.6% (−45.0 mg/dL) from baseline compared with a reduction of 6.5% (−13.0 mg/dL) for placebo. The LDL-C in the icosapent ethyl group was reduced by 1.2% (−1.0 mg/dL), while the LDL-C in the placebo arm increased by 6.5% from baseline (5.7 mg/dL). Meanwhile, there was a reduction by 12.6% in hs-CRP with icosapent ethyl compared with an increase in 29.9% (0.4 mg/L) with placebo.
It is thought that the use of mineral oil as placebo may decrease the absorption of medications including statins and adversely affect the lipid profile and inflammatory markers.38 Beyond potential effects on direct absorption of medications including statins, studies have shown that different effect on gut microbiota by different dietary oils, which can, in turn, impact the expression of inflammatory mediators.39,40 It is unclear whether mineral oil may shift the gut microbiome towards a more pro-inflammatory milieu compared to EPA. More studies are warranted. The degree of increase in LDL-C and hs-CRP observed in the placebo group compared to the icosapent ethyl group, however, is unlikely to fully account for the risk reduction in ASCVD outcomes for patients treated with EPA.41
Interestingly, there was no significant heterogeneity of effect in the primary endpoint that was detected across categories of TG levels in both the main REDUCE-IT analysis on first ischemic events and secondary analysis on total events. These findings suggest that even high-risk patients with even mildly elevated TG levels individuals can derive ASCVD risk reduction from icosapent ethyl. However, icosapent ethyl was noted to have significant greater effect in patients with high TG (≥200 mg/dL) and low HDL-C (≤35 mg/dL). Subgroup analysis from JELIS also showed a more pronounced reduction in coronary events in patients with mixed dyslipidemia with TGs ≥150mg/dL and HDL-C < 40mg/dL.42 This pattern of TG and HDL-C is often associated with a more atherogenic lipid profile, insulin resistance, increased inflammation, central obesity and metabolic syndrome. Icosapent ethyl may be a particularly important therapy for ASCVD risk reduction in this subgroup.
Safety of Icosapent Ethyl
In long-term follow-up, adverse events were more common in the EPA group compared to the control group in JELIS (25.3% vs 21.7%, p<0.0001), including higher rates of abnormal laboratory data, gastrointestinal disturbances, dermatologic side effects and bleeding.33 Conversely, serious adverse events were observed to be similar between icosapent ethyl and placebo in REDUCE-IT (30.6% vs 30.7%, p=0.98).35 There was actually a lower rate of gastrointestinal adverse events, though this may be attributable to the use of mineral oil as the placebo. Meanwhile, the rate of atrial fibrillation (AF) (3.1% vs 2.1%, p=0.004) was significantly higher with icosapent ethyl in REDUCE-IT, while no difference in new heart failure or heart failure hospitalization was observed between the icosapent ethyl and placebo groups. The rate of anemia was lower in the icosapent ethyl group compared to placebo. Serious adverse bleeding events were numerically higher in the treatment arm compared to control and approached statistical significance (2.7% vs 2.1%, p = 0.06).
Cardiovascular Outcome Trials with EPA Plus DHA
Multiple trials have assessed the efficacy of n-3 PUFA in reducing cardiovascular events, most of which involved formulations with a combination of EPA plus DHA. The GISSI-Prevenzione trial randomized patients with myocardial infarction (MI) within the past 3 months to n-3 PUFA 1 g daily, vitamin E 300 mg daily, both, or none.43 Treatment with n-3 PUFA significantly lowered the risk of the primary endpoint (death, non-fatal MI, non-stroke) (12.6% vs 13.9%, p=0.048). The GISSI-HF trial showed decreased all-cause mortality and cardiovascular hospital admissions in patients with chronic heart failure treated with n-3 PUFA (death: 27% vs 29%, p =0.041; composite of death and heart failure admission: 57% vs 59%, p=0.009).44
Later secondary prevention trials, however, did not show significant improvement in cardiovascular outcomes. The ORIGIN trial showed no reduction in cardiovascular events in high-risk patients with impaired fasting glucose, impaired glucose tolerance, or diabetes given 1g capsule containing 900 mg of n-3 PUFA or placebo (16.5% vs 15.3%, HR 1.01, 95% CI 0.93–1.10, p=0.81).45 The Alpha Omega trial randomized 4,837 patients with a history of MI within 10 years of randomization to 400 mg daily of EPA and DHA, 2 g daily of alpha-linolenic acid (ALA), both, or placebo over 40 months. There was no reduction in major cardiovascular events (EPA-DHA 14% vs 13.8%, HR 1.01, 95% CI 0.87–1.17, p=0.93).46 Finally, the OMEGA trial showed no difference in sudden cardiac death at 1 year in survivors of acute MI randomized to 900 mg of n-3 PUFA versus placebo (1.5% vs 1.5%, 95% CI 0.56–1.60, p=0.84).47
With respect to primary prevention, the Risk and Prevention Study Collaborative Group randomized n-3 PUFA 1 g daily to placebo of olive oil in patients with multiple cardiovascular risk factors or ASCVD without prior myocardial infarction, but n-3 PUFA did not reduce cardiovascular morbidity and mortality compared to placebo.48 The ASCEND trial showed no difference in serious vascular events and all-cause mortality among patients with diabetes without known cardiovascular disease treated with n-3 PUFA (daily intake of 1g capsule containing 460mg EPA and 380mg DHA) versus placebo (olive oil) after mean follow up of 7.4 years.49 The VITAL study also did not show a benefit from n-3 PUFA therapy (daily intake of 1g capsule containing 460mg EPA and 380mg DHA) in primary prevention of cardiovascular events (3.0% vs 3.2%, p=0.24) over 5 years of follow up, although there was a lower risk for MI in patients treated with n-3 PUFA (1.1% vs 1.5%; HR 0.72, 95% CI 0.59–0.90).50
There are several potential reasons why EPA trials have more consistently shown cardioprotective effects on outcomes compared with trials using EPA plus DHA beyond differences in biochemical properties of the two types of n-3 PUFAs. First, EPA trials have employed higher doses therapy. Most trials involving n-3 FA mixtures utilized daily doses close to 1g. On the other hand, EPA was given at 4g/day in the REDUCE-IT trial and 1.8g/day in the JELIS trial. Second, particularly in REDUCE-IT, selection of patients with elevated TGs resulted in a study population with likely substantial residual risk beyond elevated LDL-C and thus are less likely to be attenuated by statins alone. This differs from other trials, involving both primary and secondary prevention populations, which included participants with relatively normal TGs. For instance, while the GISSI-P trial showed positive results, the study population was mostly not on statin at baseline. Greater rate of statin use in later trials, therefore, may have tempered the detectable effect of the lower doses of n-3 PUFA in more recent trials involving mixture formulation.
Impact on Clinical Practice
The impressive results from REDUCE-IT have prompted several treatment guidelines to incorporate the use of icosapent ethyl into clinical practice recommendations. Based on the 2019 ADA guidelines on Standards of Medical Care in Diabetes, the addition of icosapent ethyl should be considered in diabetic patients with ASCVD or other cardiac risk factors on a statin with controlled LDL-C, but elevated TGs (135–499 mg/dL) (Level A).51 Similarly, the 2019 EAS/ESC Guidelines for the Management of Dyslipidemia recommend consideration of icosapent ethyl 2x2g/day in combination with a statin in high-risk patients (defined as individuals with documented ASCVD, DM with risk features, moderate to severe chronic kidney disease, SCORE ≥ 5% for 10-year risk for fatal CVD) with TG levels between 135 and 499 mg/dL despite statin therapy (Class IIa, Level B).52 Scientific statement from the NLA also recommends the use of icosapent ethyl in patients with clinical ASCVD, or with diabetes mellitus plus ≥1 addition risk factor with hypertriglyceridemia and on maximally tolerated statin therapy (Class I; evidence B-R).53 While the use of icosapent ethyl for ASCVD risk reduction was not included in the 2018 ACC/AHA Multisociety Guideline on the Management of Blood Cholesterol, it should be noted that the results of REDUCE-IT were not yet available.54
Previous data show that a substantial number of patients may benefit from treatment with icosapent ethyl based on REDUCE-IT entry criteria. One study estimated that 14.5% of ASCVD patients and 17.1% of high-risk diabetes patients would be eligible for icosapent ethyl within the Veterans Affairs healthcare system.55 Analysis from the National Health and Nutrition Examination Survey (NHANES) estimates that 2.9 million individuals from the United States would potentially be candidates for icosapent ethyl, resulting in an estimated cost to the US healthcare system of almost $9 billion dollars.56 Although there will be substantial upfront cost for icosapent ethyl, the ASCVD risk reduction conferred may make overall cost-effectiveness more favorable. One cost-effective analysis of EPA 1.8g/day in Japanese patients with hypercholesterolemia, based on the JELIS study, found that a combination of EPA with statins had acceptable cost-effectiveness in secondary prevention but not in primary prevention.57 The Institute for Clinical and Economic Review (ICER) also conducted a cost-effectiveness analysis based on REDUCE-IT results, showing that icosapent ethyl price falls below cost to achieve the $50,000 and $100,000 quality-adjusted life year (QALY) thresholds, suggesting that the agent has long-term cost-effectiveness.58
Future Directions
There are currently several ongoing cardiovascular outcome trials that aim to further elucidate the role of EPA as well as EPA+DHA formulations for ASCVD prevention. The Randomized trial for Evaluation in Secondary Prevention Efficacy of Combination Therapy – Statin and Eicosapentaenoic Acid (RESPECT-EPA) aims to assess the efficacy and safety of EPA 1.8g/day in secondary prevention of ASCVD events among 3,900 Japanese patients with stable coronary artery disease.59,60 Meanwhile, the Statin Residual Risk Reduction with EpaNova in High Cardiovascular Risk (STRENGTH) trial will assess the efficacy and safety of EPA+DHA carboxylic acid at 4g/day vs placebo (corn oil) for ASCVD risk reduction in 13,086 high-risk patients with elevated TGs (≥180mg/dL and <500mg/dL), low HDL-C (<42mg/dL in men and <47mg/dL for women) and relatively well-controlled LDL-C (<100mg/dL), a similar population that was studied in REDUCE-IT.61 A second EPA+DHA outcomes trial, the Omega-3 Fatty Acids in Elderly Patients with Myocardial Infarction (OMEMI) trial will assess efficacy for secondary prevention of EPA+DHA 1.8g/day in 1,400 high-risk Norwegian patients who have had a history of MI.62 These ongoing trials will help to answer the question of whether ASCVD risk reduction observed in REDUCE-IT and JELIS were due primarily to the use of pure EPA formulations or if use of higher dosages of overall omega-3 are also efficacious. The studies will also help to elucidate whether some of the apparent benefit observed in REDUCE-IT was due to adverse effects of mineral oil used in the placebo group, which may have impacted efficacy of the concomitant statin therapy.
Conclusion
The efficacy of icosapent ethyl in the reduction of ASCVD risk is built upon a confluence of evidence, culminating in the REDUCE-IT trial. The cardioprotective effect of EPA is likely in part due to triglyceride lowering. However, there are also likely important pleiotropic effects such as anti-inflammatory properties may play a role. There remains much to be learned about icosapent ethyl from better understanding of the molecular mechanism of action to real-world implementation and cost-effectiveness. Despite these unknowns, icosapent ethyl appears to have a strong potential in reducing residual ASCVD risk in high-risk patients already optimized on statin therapy.
Disclosure
Salim Virani report grants from US Department of Veterans Affairs, grants from World Heart Federation, grants from Jooma and Tahir Family, Honorarium for role as the Associate Editor for Innovations acc.org from American College of Cardiology, Steering Committee Member (No financial remuneration) from Patient and Provider Assessment of Lipid Management, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. McLennan PL. Myocardial membrane fatty acids and the antiarrhythmic actions of dietary fish oil in animal models. Lipids. 2001;36(Suppl):S111–S114. doi:10.1007/s11745-001-0692-x
2. Leaf A, Kang JX, Xiao YF, Billman GE. Clinical prevention of sudden cardiac death by n-3 polyunsaturated fatty acids and mechanism of prevention of arrhythmias by n-3 fish oils. Circulation. 2003;107(21):2646–2652. doi:10.1161/01.CIR.0000069566.78305.33
3. Kim W, Khan NA, McMurray DN, Prior IA, Wang N, Chapkin RS. Regulatory activity of polyunsaturated fatty acids in T-cell signaling. Prog Lipid Res. 2010;49(3):250–261. doi:10.1016/j.plipres.2010.01.002
4. Mozaffarian D, Wu JH. Omega-3 fatty acids and cardiovascular disease: effects on risk factors, molecular pathways, and clinical events. J Am Coll Cardiol. 2011;58(20):2047–2067. doi:10.1016/j.jacc.2011.06.063
5. Musunuru K, Kathiresan S. Surprises from genetic analyses of lipid risk factors for atherosclerosis. Circ Res. 2016;118(4):579–585. doi:10.1161/CIRCRESAHA.115.306398
6. Do R, Willer CJ, Schmidt EM, et al. Common variants associated with plasma triglycerides and risk for coronary artery disease. Nat Genet. 2013;45(11):1345–1352. doi:10.1038/ng.2795
7. Sarwar N, Sandhu MS, Ricketts SL, et al. Triglyceride-mediated pathways and coronary disease: collaborative analysis of 101 studies. Lancet. 2010;375(9726):1634–1639.
8. Ginsberg HN, Elam MB, Lovato LC, et al. Effects of combination lipid therapy in type 2 diabetes mellitus. N Engl J Med. 2010;362(17):1563–1574.
9. Keech A, Simes RJ, Barter P, et al. Effects of long-term fenofibrate therapy on cardiovascular events in 9795 people with type 2 diabetes mellitus (the FIELD study): randomised controlled trial. Lancet. 2005;366(9500):1849–1861.
10. Jacobson TA, Glickstein SB, Rowe JD, Soni PN. Effects of eicosapentaenoic acid and docosahexaenoic acid on low-density lipoprotein cholesterol and other lipids: a review. J Clin Lipidol. 2012;6(1):5–18. doi:10.1016/j.jacl.2011.10.018
11. Bays HE, Ballantyne CM, Kastelein JJ, Isaacsohn JL, Braeckman RA, Soni PN. Eicosapentaenoic acid ethyl ester (AMR101) therapy in patients with very high triglyceride levels (from the multi-center, plAcebo-controlled, randomized, double-blINd, 12-week study with an open-label Extension [MARINE] trial). Am J Cardiol. 2011;108(5):682–690. doi:10.1016/j.amjcard.2011.04.015
12. Ballantyne CM, Bays HE, Kastelein JJ, et al. Efficacy and safety of eicosapentaenoic acid ethyl ester (AMR101) therapy in statin-treated patients with persistent high triglycerides (from the ANCHOR study). Am J Cardiol. 2012;110(7):984–992. doi:10.1016/j.amjcard.2012.05.031
13. Bays HE, Ballantyne CM, Braeckman RA, Stirtan WG, Soni PN. Icosapent ethyl, a pure ethyl ester of eicosapentaenoic acid: effects on circulating markers of inflammation from the MARINE and ANCHOR studies. Am J Cardiovasc Drugs. 2013;13(1):37–46. doi:10.1007/s40256-012-0002-3
14. Ballantyne CM, Bays HE, Braeckman RA, et al. Icosapent ethyl (eicosapentaenoic acid ethyl ester): effects on plasma apolipoprotein C-III levels in patients from the MARINE and ANCHOR studies. J Clin Lipidol. 2016;10(3):635–645.e631. doi:10.1016/j.jacl.2016.02.008
15. Ballantyne CM, Braeckman RA, Bays HE, et al. Effects of icosapent ethyl on lipoprotein particle concentration and size in statin-treated patients with persistent high triglycerides (The ANCHOR study). J Clin Lipidol. 2015;9(3):377–383. doi:10.1016/j.jacl.2014.11.009
16. Crosby J, Peloso GM, Auer PL, et al. Loss-of-function mutations in APOC3, triglycerides, and coronary disease. N Engl J Med. 2014;371(1):22–31.
17. Brinton EA, Ballantyne CM, Bays HE, Kastelein JJ, Braeckman RA, Soni PN. Effects of icosapent ethyl on lipid and inflammatory parameters in patients with diabetes mellitus-2, residual elevated triglycerides (200–500 mg/dL), and on statin therapy at LDL-C goal: the ANCHOR study. Cardiovasc Diabetol. 2013;12:100. doi:10.1186/1475-2840-12-100
18. Ballantyne CM, Manku MS, Bays HE, et al. Icosapent ethyl effects on fatty acid profiles in statin-treated patients with high triglycerides: the randomized, Placebo-controlled ANCHOR study. Cardiol Ther. 2019;8(1):79–90. doi:10.1007/s40119-019-0131-8
19. Miller M, Ballantyne CM, Bays HE, et al. Effects of icosapent ethyl (eicosapentaenoic acid ethyl ester) on atherogenic lipid/ lipoprotein,apolipoprotein, and inflammatory parameters in patients with elevated high-sensitivity C-reactive protein (from the ANCHOR study). Am J Cardiol. 2019;124(5):696–701. doi:10.1016/j.amjcard.2019.05.057
20. Mita T, Watada H, Ogihara T, et al. Eicosapentaenoic acid reduces the progression of carotid intima-media thickness in patients with type 2 diabetes. Atherosclerosis. 2007;191(1):162–167. doi:10.1016/j.atherosclerosis.2006.03.005
21. Nishio R, Shinke T, Otake H, et al. Stabilizing effect of combined eicosapentaenoic acid and statin therapy on coronary thin-cap fibroatheroma. Atherosclerosis. 2014;234(1):114–119. doi:10.1016/j.atherosclerosis.2014.02.025
22. Shearer GC, Savinova OV, Harris WS. Fish oil – how does it reduce plasma triglycerides? Biochim Biophys Acta. 2012;1821(5):843–851. doi:10.1016/j.bbalip.2011.10.011
23. Clarke SD, Jump D. Polyunsaturated fatty acids regulate lipogenic and peroxisomal gene expression by independent mechanisms. Prostaglandins Leukot Essent Fatty Acids. 1997;57(1):65–69. doi:10.1016/S0952-3278(97)90494-4
24. Lang CA, Davis RA. Fish oil fatty acids impair VLDL assembly and/or secretion by cultured rat hepatocytes. J Lipid Res. 1990;31(11):2079–2086.
25. Park Y, Jones PG, Harris WS. Triacylglycerol-rich lipoprotein margination: a potential surrogate for whole-body lipoprotein lipase activity and effects of eicosapentaenoic and docosahexaenoic acids. Am J Clin Nutr. 2004;80(1):45–50. doi:10.1093/ajcn/80.1.45
26. Khan S, Minihane AM, Talmud PJ, et al. Dietary long-chain n-3 PUFAs increase LPL gene expression in adipose tissue of subjects with an atherogenic lipoprotein phenotype. J Lipid Res. 2002;43(6):979–985.
27. Berge RK, Madsen L, Vaagenes H, Tronstad KJ, Göttlicher M, Rustan AC. In contrast with docosahexaenoic acid, eicosapentaenoic acid and hypolipidaemic derivatives decrease hepatic synthesis and secretion of triacylglycerol by decreased diacylglycerol acyltransferase activity and stimulation of fatty acid oxidation. Biochem J. 1999;343(Pt 1):191–197. doi:10.1042/bj3430191
28. Wall R, Ross RP, Fitzgerald GF, Stanton C. Fatty acids from fish: the anti-inflammatory potential of long-chain omega-3 fatty acids. Nutr Rev. 2010;68(5):280–289. doi:10.1111/nure.2010.68.issue-5
29. Fredman G, Hellmann J, Proto JD, et al. An imbalance between specialized pro-resolving lipid mediators and pro-inflammatory leukotrienes promotes instability of atherosclerotic plaques. Nat Commun. 2016;7:12859. doi:10.1038/ncomms12859
30. Serhan CN. Pro-resolving lipid mediators are leads for resolution physiology. Nature. 2014;510(7503):92–101. doi:10.1038/nature13479
31. Mason RP, Jacob RF, Shrivastava S, Sherratt SCR, Chattopadhyay A. Eicosapentaenoic acid reduces membrane fluidity, inhibits cholesterol domain formation, and normalizes bilayer width in atherosclerotic-like model membranes. Biochim Biophys Acta. 2016;1858(12):3131–3140. doi:10.1016/j.bbamem.2016.10.002
32. Cawood AL, Ding R, Napper FL, et al. Eicosapentaenoic acid (EPA) from highly concentrated n-3 fatty acid ethyl esters is incorporated into advanced atherosclerotic plaques and higher plaque EPA is associated with decreased plaque inflammation and increased stability. Atherosclerosis. 2010;212(1):252–259. doi:10.1016/j.atherosclerosis.2010.05.022
33. Yokoyama M, Origasa H, Matsuzaki M, et al. Effects of eicosapentaenoic acid on major coronary events in hypercholesterolaemic patients (JELIS): a randomised open-label, blinded endpoint analysis. Lancet. 2007;369(9567):1090–1098. doi:10.1016/S0140-6736(07)60527-3
34. Nosaka K, Miyoshi T, Iwamoto M, et al. Early initiation of eicosapentaenoic acid and statin treatment is associated with better clinical outcomes than statin alone in patients with acute coronary syndromes: 1-year outcomes of a randomized controlled study. Int J Cardiol. 2017;228:173–179. doi:10.1016/j.ijcard.2016.11.105
35. Bhatt DL, Steg PG, Miller M, et al. Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia. N Engl J Med. 2019;380(1):11–22. doi:10.1056/NEJMoa1812792
36. Bays HE, Ballantyne CM, Doyle RT, Juliano RA, Philip S. Icosapent ethyl: eicosapentaenoic acid concentration and triglyceride-lowering effects across clinical studies. Prostaglandins Other Lipid Mediat. 2016;125:57–64. doi:10.1016/j.prostaglandins.2016.07.007
37. Bhatt DL, Steg PG, Miller M, et al. Effects of icosapent ethyl on total ischemic events: from REDUCE-IT. J Am Coll Cardiol. 2019;73(22):2791–2802. doi:10.1016/j.jacc.2019.02.032
38. Baum SJ. ANCHOR trial conclusions regarding the effects of pure eicosapentaenoic acid on low-density lipoprotein cholesterol. Am J Cardiol. 2013;111(3):454–455. doi:10.1016/j.amjcard.2012.11.035
39. Patrone V, Minuti A, Lizier M, et al. Differential effects of coconut versus soy oil on gut microbiota composition and predicted metabolic function in adult mice. BMC Genomics. 2018;19(1):808. doi:10.1186/s12864-018-5202-z
40. Costantini L, Molinari R, Farinon B, Merendino N. Impact of omega-3 fatty acids on the gut microbiota. Int J Mol Sci. 2017;18(12):2645. doi:10.3390/ijms18122645
41. Jia X, Kohli P, Virani SS. Omega-3 fatty acid and cardiovascular outcomes: insights from recent clinical trials. Curr Atheroscler Rep. 2019;21(1):1. doi:10.1007/s11883-019-0763-0
42. Saito Y, Yokoyama M, Origasa H, et al. Effects of EPA on coronary artery disease in hypercholesterolemic patients with multiple risk factors: sub-analysis of primary prevention cases from the Japan EPA lipid intervention study (JELIS). Atherosclerosis. 2008;200(1):135–140. doi:10.1016/j.atherosclerosis.2008.06.003
43. Dietary supplementation with. n-3 polyunsaturated fatty acids and vitamin E after myocardial infarction: results of the GISSI-Prevenzione trial. Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto miocardico. Lancet. 1999;354(9177):447–455. doi:10.1016/S0140-6736(99)07072-5
44. Tavazzi L, Maggioni AP, Marchioli R, et al. Effect of n-3 polyunsaturated fatty acids in patients with chronic heart failure (the GISSI-HF trial): a randomised, double-blind, placebo-controlled trial. Lancet. 2008;372(9645):1223–1230. doi:10.1016/S0140-6736(08)61239-8
45. Bosch J, Gerstein HC, Dagenais GR, et al. n-3 fatty acids and cardiovascular outcomes in patients with dysglycemia. N Engl J Med. 2012;367(4):309–318.
46. Kromhout D, Giltay EJ, Geleijnse JM, Group AOT. n-3 fatty acids and cardiovascular events after myocardial infarction. N Engl J Med. 2010;363(21):2015–2026. doi:10.1056/NEJMoa1003603
47. Rauch B, Schiele R, Schneider S, et al. OMEGA, a randomized, placebo-controlled trial to test the effect of highly purified omega-3 fatty acids on top of modern guideline-adjusted therapy after myocardial infarction. Circulation. 2010;122(21):2152–2159. doi:10.1161/CIRCULATIONAHA.110.948562
48. Roncaglioni MC, Tombesi M, Avanzini F, et al. n-3 fatty acids in patients with multiple cardiovascular risk factors. N Engl J Med. 2013;368(19):1800–1808.
49. Bowman L, Mafham M, Wallendszus K, et al. Effects of n-3 Fatty Acid Supplements in Diabetes Mellitus. N Engl J Med. 2018;379(16):1540–1550.
50. Manson JE, Cook NR, Lee IM, et al. Marine n-3 fatty acids and prevention of cardiovascular disease and cancer. N Engl J Med. 2018;380(1):23-32.
51. Association AD. 10. Cardiovascular disease and risk management. Diabetes Care. 2019;42(Suppl 1):S103–S123. doi:10.2337/dc19-S010
52. Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2019;290:140–205.
53. Orringer CE, Jacobson TA, Maki KC. National lipid association scientific statement on the use of icosapent ethyl in statin-treated patients with elevated triglycerides and high or very-high ASCVD risk. J Clin Lipidol. 2019;13(6):860–872. doi:10.1016/j.jacl.2019.10.014
54. Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: a Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice guidelines. Circulation. 2019;139(25):e1082–e1143. doi:10.1161/CIR.0000000000000625
55. Jia X, Akeroyd JM, Nasir K, et al. Eligibility and cost for icosapent ethyl based on the REDUCE-IT trial. Circulation. 2019;139(10):1341–1343. doi:10.1161/CIRCULATIONAHA.118.038691
56. Khera R, Valero-Elizondo J, Saxena A, Virani SS, Krumholz HM, Nasir K. National population and cost implications of treatment with icosapentyl ethyl in the united states: an assessment based on the REDUCE-IT trial. bioRxiv. 2018.
57. Kodera S, Morita H, Kiyosue A, Ando J, Komuro I. Cost-effectiveness of statin plus eicosapentaenoic acid combination therapy for cardiovascular disease prevention in japanese patients with hypercholesterolemia- an analysis based on the Japan eicosapentaenoic acid lipid intervention study (JELIS). Circ J. 2018;82(4):1076–1082. doi:10.1253/circj.CJ-17-0995
58. Institute for Clinical and Economic Review. Additive Therapies for Cardiovascular Disease: Effectiveness and Value; 2019. Available from: https://icer-review.org/wp-content/uploads/2019/02/ICER_CVD_Draft_Evidence_Report_072419.pdf. Accessed December 2, 2019.
59. Ganda OP, Bhatt DL, Mason RP, Miller M, Boden WE. Unmet need for adjunctive dyslipidemia therapy in hypertriglyceridemia management. J Am Coll Cardiol. 2018;72(3):330–343. doi:10.1016/j.jacc.2018.04.061
60. UMIN-CTR Clinical Trial. Randomized trial for evaluation in secondary prevention efficacy of combination therapy — statin and eicosapentaenoic acid UMIN000012069; 2018. Available from: https://upload.umin.ac.jp/cgi-open-bin/ctr_e/ctr_view.cgi?recptno=R000014051. Accessed November 22, 2019.
61. Nicholls SJ, Lincoff AM, Bash D, et al. Assessment of omega-3 carboxylic acids in statin-treated patients with high levels of triglycerides and low levels of high-density lipoprotein cholesterol: rationale and design of the STRENGTH trial. Clin Cardiol. 2018;41(10):1281–1288. doi:10.1002/clc.23055
62. Laake K, Myhre P, Nordby LM, et al. Effects of ω3 supplementation in elderly patients with acute myocardial infarction: design of a prospective randomized placebo controlled study. BMC Geriatr. 2014;14:74. doi:10.1186/1471-2318-14-74
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.