Back to Journals » International Medical Case Reports Journal » Volume 8
Spontaneous resolution of massive expulsive suprachoroidal hemorrhage with good long-term visual outcome: a case report
Authors Lee S, Lee JH, Park SW, Kim M, Han SB, Yang HK
Received 8 July 2015
Accepted for publication 7 August 2015
Published 9 September 2015 Volume 2015:8 Pages 185—187
DOI https://doi.org/10.2147/IMCRJ.S92007
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Seung-Jun Lee,* Jang Hun Lee,* Sang Wook Park, Moosang Kim, Sang Beom Han
Department of Ophthalmology, Kangwon National University Hospital, Kangwon National University Graduate School of Medicine, Chuncheon, Korea
*These authors contributed equally to this work
Introduction: Massive suprachoroidal hemorrhage (SCH) that completely fills the vitreous cavity rarely resolves spontaneously. Even in cases with spontaneous resolution, long-term visual prognosis is disappointing due to retinal detachment or deterioration of preexisting ocular diseases. To the best of our knowledge, the first case of spontaneous resolution of massive SCH is reported with good long-term visual and anatomic outcome.
Case presentation: An 80-year-old Asian woman with high myopia underwent cataract surgery in the right eye. Posterior capsular rupture occurred during phacoemulsification. At the conclusion of scleral fixation of intraocular lens, expulsive SCH developed. After 1 day, best-corrected visual acuity (BCVA) was hand motion. Ultrasonography revealed massive SCH with central apposition. At 2nd week, decrease in SCH with resolution of central apposition was observed. At 6th week, BCVA improved to 20/120. Ultrasonography and fundus examination revealed complete resorption of the SCH and flat retina. At 1 year, BCVA was 20/50. Fundus was flat without any signs of retinal detachment.
Conclusion: Favorable anatomic and visual outcomes can be attained with conservative management even in cases of massive expulsive SCH, particularly when central retinal apposition resolves in 2 weeks.
Keywords: conservative management, suprachoroidal hemorrhage, spontaneous resolution
Introduction
Suprachoroidal hemorrhage (SCH) is a rare but potentially devastating complication of intraocular surgery.1 Although surgical intervention is often tried particularly in massive SCH, visual outcome is disappointing.1–4 Although resolution of massive SCH with conservative management has been reported, long-term visual prognosis is poor.2 A case of spontaneous resolution of intraoperative massive SCH is recently examined with a good long-term visual outcome, thus herein report the case.
Case presentation
An 80-year-old Asian woman underwent cataract surgery in the right eye (OD). Preoperatively, best-corrected visual acuity (BCVA) was 20/70 OD with spherical equivalent of −6.50 diopters. Axial length measured with an optical biometer (IOLMaster, Carl Zeiss Meditec AG, Jena, Germany) was 26.08 mm OD. During phacoemulsification, posterior capsular rupture occurred. After aspiration of the lens fragments, anterior vitrectomy and scleral fixation of intraocular lens (IOL) was performed. Immediately after finishing the scleral fixation, a sudden elevation of dark-brown choroidal mass with rapid progression was detected. The main and side-port incisions were promptly closed with an intracameral instillation of 2% pilocarpine hydrochloride. A small amount of viscoelastic was left in the intracameral space to prevent vitreous incarceration. Intraocular pressure (IOP) was 37 mmHg OD immediately after surgery. After administration of intravenous 15% mannitol 200 mL, IOP decreased to 22 mmHg. After 1 day, BCVA was hand motion (HM), and IOP was 15 mmHg OD. Ultrasonography revealed SCH with central apposition (Figure 1A), and anterior segment examination showed a massive SCH touching the IOL (Figure 1B). Vitreous incarceration to wound was never found, although vitreous prolapse to intracameral space was observed. After 2 weeks, BCVA was HM, and IOP was 11 mmHg OD. Ultrasonography showed decrease in SCH with resolution of central apposition. At postoperative 6 weeks, BCVA improved to 20/120 and IOP was 11 mmHg. Ultrasonography showed a complete resorption of the SCH (Figure 1C), and the fundus was flat (Figure 1D). At postoperative 1 year, BCVA improved to 20/50 and IOP was 12 mmHg. Fundus was flat without any signs of retinal detachment.
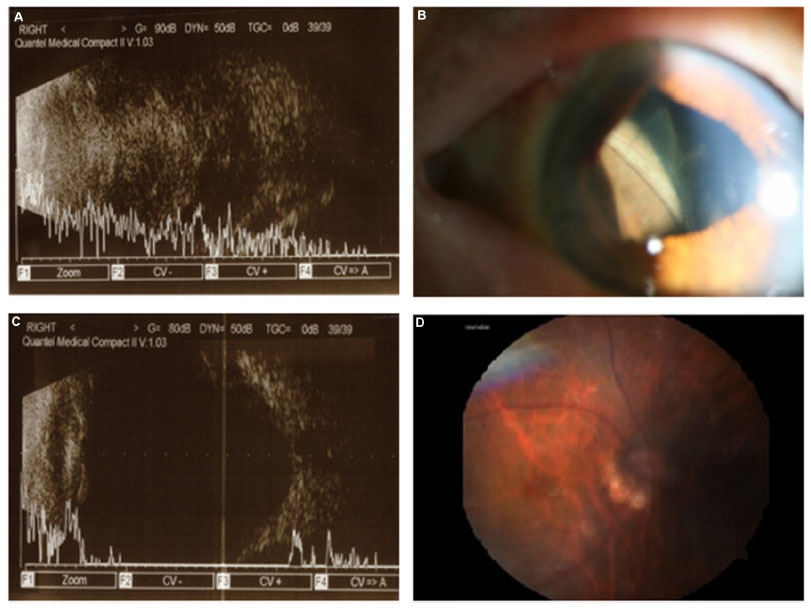 | Figure 1 Changes in suprachoroidal hemorrhage with time. |
Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. Due to the retrospective nature and report of a single case, ethics approval was not requested. This study conformed to the tenets of the Declaration of Helsinki in respect of the testing of the device on humans. A copy of the written consent is available for review by the Editor of this journal.
Discussion
Current trend in the treatment of SCH includes early surgical intervention, particularly in cases of massive SCH with central retinal apposition, so-called “kissing configuration”.1 Meier and Wiedemann4 suggested that surgical treatment, including drainage by sclerotomy and vitrectomy, should be performed to minimize the damage caused by SCH. However, there exist evidences that central apposition may not be an absolute indication for surgery.2,3 Chu et al2 reported that the mean duration of central apposition in SCH was 15 days, and central choroidal elevation began to decrease rapidly at 3rd week, although peripheral elevation persisted for 6 weeks or longer. They also showed that all four cases with massive intraoperative SCH spontaneously resolved.2 Scott et al3 demonstrated that no significant difference in visual outcome between observational management and surgical intervention in a study including 51 cases of massive SCH. They reported that the duration of central apposition for more than 14 days was a risk factor of poor visual outcome, suggesting that surgical intervention may be necessary if the central apposition persists longer than 14 days.3 In our case, we decided to continue the conservative monitoring as resolution of central retinal apposition was found in 2nd week, and the hemorrhage was completely absorbed in 6 weeks.
Although good initial visual recovery can be achieved with the resolution of the SCH, previous studies revealed that long-term visual prognosis was poor because of subsequent retinal detachment or progression of underlying ocular disease.2 Therefore, this case is noteworthy, because good visual acuity of 20/60 with stable retina was maintained at 1 year after the expulsive SCH.
Axial myopia increases the risk of SCH due to reduced scleral rigidity and choroidal vascular fragility.1,5 Surgical aphakia is also a predisposing factor of SCH, because the loss of the lens and zonular support can promote stretching and separation of the uvea from the sclera during ciliochoroidal effusions.1 Advanced age and hypertension also associated with choroidal vascular fragility and sclerosis, and are considered to be risk factors of SCH.1,5 In the present case, the patient was 80 years of age, had hypertension and high myopia, all of which might contribute to the development of SCH. Moreover, aphakic state before sclera fixation might also aggravate the hemorrhage. Fortunately, the IOL fixed to sclera appears to prevent further protrusion of the choroid tissue. Early recognition followed by prompt meiosis and would closure might also prevent the deterioration of the SCH. Factors associated with poor outcome, such as vitreous incarceration to the wound or retinal detachment, were never detected, which might also contribute to the visual recovery.2
Conclusion
This case report suggests that favorable anatomic and visual outcomes can be attained with conservative management even in cases of massive expulsive SCH, particularly when central retinal apposition resolves in 2 weeks.
Author contributions
SJL carried out data acquisition and drafted the manuscript. JHL interpreted the data and drafted the manuscript. SWP interpreted the data and drafted the manuscript. MK analyzed the data and critically revised the manuscript. SBH analyzed the data and critically revised the manuscript. All authors read and approved the final paper, and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosure
The authors report no conflicts of interest in this work.
References
Chu TG, Green RL. Suprachoroidal hemorrhage. Surv Ophthalmol. 1999;43:471–486. | |
Chu TG, Cano MR, Green RL, et al. Massive suprachoroidal hemorrhage with central retinal apposition. A clinical and echographic study. Arch Ophthalmol. 1991;109:1575–1581. | |
Scott IU, Flynn HW Jr, Schiffman J, et al. Visual acuity outcomes among patients with appositional suprachoroidal hemorrhage. Ophthalmology. 1997;104:2039–2046. | |
Meier P, Wiedemann P. Massive suprachoroidal hemorrhage: secondary treatment and outcome. Graefes Arch Clin Exp Ophthalmol. 2000;238: 28–32. | |
Chak M, Williamson TH. Spontaneous suprachoroidal haemorrhage associated with high myopia and aspirin. Eye. 2003;17:525–527. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.