Back to Journals » International Medical Case Reports Journal » Volume 19
Spontaneous Recovery from Hepatitis A–Induced Acute Liver Failure in a Child: A Rare Case Report from Hargeisa Group Hospital, Somaliland
Authors Ibrahim KJ ![]() , H Ali AM, Dirir MJ, Ahmed SI
, H Ali AM, Dirir MJ, Ahmed SI ![]()
Received 10 January 2026
Accepted for publication 14 April 2026
Published 21 April 2026 Volume 2026:19 595240
DOI https://doi.org/10.2147/IMCRJ.S595240
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Thomas E Hutson
Khadar Jama Ibrahim,1 Abdisamed Mohamoud H Ali,1 Mohamoud Jimale Dirir,1 Sadam Ismail Ahmed2,3
1Department of Emergency, Hargeisa Group Hospital, Hargeisa, Somaliland; 2Faculty of Medicine and Health Science, University of Burao, Burao, Somaliland; 3Department of Anesthesia and Critical Care Unit, Haldoor Multi-Specialty Teaching Hospital, Hargeisa, Somaliland
Correspondence: Sadam Ismail Ahmed, Email [email protected]
Background: Hepatitis A–induced acute liver failure (ALF) is a rare but leading cause of pediatric ALF in developing countries. ALF is defined as severe acute liver injury with coagulopathy and hepatic encephalopathy occurring within 26 weeks of symptom onset in patients without pre-existing chronic liver disease. It carries high mortality, accounting for approximately 8% of liver transplants worldwide, with reported survival rates ranging from 30– 60% in the absence of transplantation. Fewer than 1% of patients with hepatitis A progress to ALF.
Case Presentation: A 5-year-old girl from Wajaale, Somaliland, presented with fever, jaundice, and altered consciousness. She also developed hematemesis secondary to severe coagulopathy (INR 4.0), with no evidence of esophageal varices. Laboratory evaluation revealed markedly elevated transaminases and hyperbilirubinemia. HAV IgM was positive. Supportive therapy with lactulose, neomycin, vitamin K, and nutritional support resulted in full clinical and biochemical recovery without the need for liver transplantation.
Conclusion: This case demonstrates that spontaneous recovery from HAV-induced ALF is possible with timely supportive care, even in resource-limited settings where monitoring and grading of encephalopathy are vital. It underscores the public health importance of strengthening supportive care protocols and implementing universal HAV vaccination to prevent these high-mortality emergencies.
Keywords: hepatitis a, acute liver failure, pediatrics, spontaneous recovery, Somaliland, public health
Introduction
Acute liver failure (ALF) is a rare but life-threatening condition characterized by severe acute liver injury, coagulopathy, and hepatic encephalopathy occurring within 26 weeks of symptom onset in patients without pre-existing chronic liver disease.1 ALF carries a high mortality rate and accounts for approximately 8% of liver transplants worldwide.2 In pediatric populations, the etiology of ALF varies significantly by geographic region and age. In developed countries, metabolic disorders, drug-induced liver injury, and autoimmune hepatitis are common causes, whereas in developing countries, viral hepatitis—particularly hepatitis A and hepatitis E—remains the predominant etiology.3,4
Hepatitis A virus (HAV) infection is typically self-limiting in children, with fewer than 1% of cases progressing to ALF.5 However, in regions where HAV is endemic and routine vaccination is not implemented, the burden of HAV-induced ALF remains substantial. In sub-Saharan Africa, including Somaliland, hepatitis A accounts for a significant proportion of pediatric ALF cases, though population-level data are limited due to underreporting and diagnostic constraints.6
The pathogenesis of HAV-induced ALF involves immune-mediated hepatocyte injury rather than direct viral cytopathy, leading to extensive hepatic necrosis and subsequent synthetic dysfunction.7 The resulting coagulopathy, hyperbilirubinemia, and encephalopathy contribute to the high morbidity and mortality associated with this condition. In resource-limited settings where liver transplantation is unavailable, management relies entirely on timely supportive care, including correction of coagulopathy, management of encephalopathy, and nutritional support.8
This case report describes a 5-year-old child from Somaliland with HAV-induced ALF who achieved spontaneous recovery with supportive therapy alone. The case highlights the potential for favorable outcomes even in resource-limited settings and underscores the importance of strengthening supportive care protocols and preventive vaccination programs. This report has been prepared in accordance with the SCARE 2025 guidelines.9
Case Presentation
A 5-year-old female from Wajaale, Somaliland, presented with a 7-day history of fever, predominantly at night, partially relieved by paracetamol. The fever was associated with hematemesis (two episodes) and poor oral intake, followed by altered consciousness. She had no previous medical or surgical history, no history of blood transfusions, and no chronic illnesses in the family. All siblings were healthy, and there was no history of exposure to hepatotoxic drugs or herbal remedies.
Physical Examination
On examination, the child appeared ill and was unconscious, with a Glasgow Coma Scale (GCS) score of 6/15, generalized hypertonia, and absent deep tendon reflexes. She had pallor and jaundice; pupils were equal and reactive to light.
Vital signs: heart rate 123 beats per minute (tachycardia), blood pressure 95/60 mmHg (within normal range for age), respiratory rate 24 breaths per minute, temperature 37.8°C, and oxygen saturation 96% on room air. Despite tachycardia, there was no evidence of hypotension or distributive shock.
Airway Assessment: Although the patient presented with a GCS of 6/15, she maintained intact gag and cough reflexes with no signs of airway compromise or respiratory distress. Therefore, endotracheal intubation was not required. The patient was closely monitored in a high-acuity setting with continuous cardiorespiratory monitoring, head-of-bed elevation, and frequent neurological assessments.
Abdominal examination revealed mild hepatomegaly (liver edge palpable 2 cm below the right costal margin) with no splenomegaly or palpable masses. Chest examination was unremarkable, with normal heart sounds and no respiratory distress.
Laboratory and Imaging Findings
Differential Diagnosis and Exclusion of Other Causes
Differential diagnoses considered included Wilson’s disease, drug-induced liver injury, and other viral hepatitides. Wilson’s disease was excluded by normal serum ceruloplasmin (26 mg/dL; reference range: 20–40 mg/dL) and the absence of Kayser–Fleischer rings on slit-lamp ophthalmologic examination. Drug-induced liver injury was excluded by negative history of hepatotoxic medication or herbal remedy exposure. Serological testing for hepatitis B (HBsAg), hepatitis C (anti-HCV), and hepatitis E (HEV IgM) were all negative. Malaria smear was negative, and serum acetaminophen level was undetectable (<5 µg/mL).
Laboratory investigations revealed markedly elevated liver enzymes (AST 2020 IU/L, ALT 2150 IU/L), hyperbilirubinemia (total bilirubin 8.0 mg/dL, direct bilirubin 6.5 mg/dL), and severe coagulopathy (PT 40 sec, INR 4.0). Serum ammonia was elevated at 156 µmol/L (reference range: 11–35 µmol/L), supporting hepatic encephalopathy as the etiology of altered consciousness. White blood cell count, hemoglobin, platelets, albumin, renal function, electrolytes, and ESR were within normal limits. Serology confirmed acute Hepatitis A infection (HAV IgM reactive).
Abdominal ultrasound (Figure 1A and B) revealed mild hepatomegaly with diffusely increased hepatic echogenicity and coarse parenchymal texture, consistent with acute hepatitis. Diffuse gallbladder wall thickening, mild ascites, and mild bilateral pleural effusion were also noted. No evidence of biliary dilatation or focal liver lesions was observed.
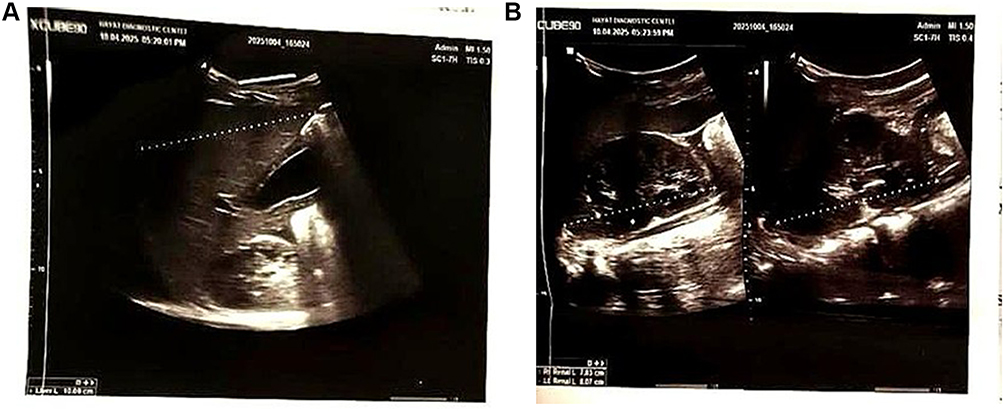 |
Figure 1 (A) Ultrasound image showing diffuse hepatic involvement consistent with acute liver injury and hepatomegaly. (B) Ultrasound showing hepatic parenchymal changes with altered echogenicity. |
Abdominal ultrasound showed mild hepatomegaly, diffuse gallbladder wall thickening, mild ascites, and mild bilateral pleural effusion (Table 1 and Figure 1A and B).
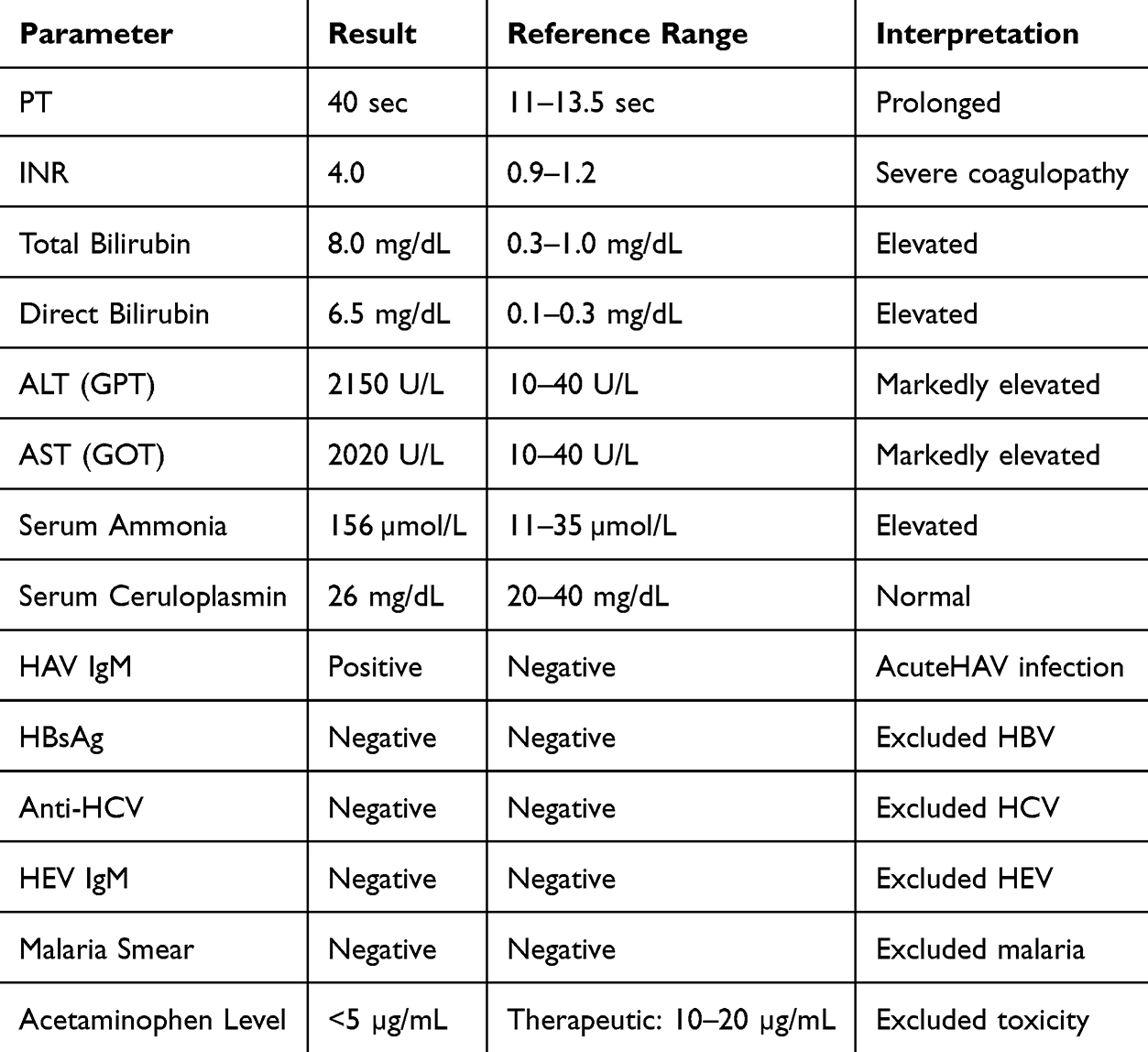 |
Table 1 Admission Laboratory Findings |
Therapeutic Intervention and Hospital Course
The patient received conservative management for acute Hepatitis A with acute liver failure and hepatic encephalopathy. Supportive care included:
- Lactulose (5 mL orally every 8 hours) and neomycin (50 mg/kg/day orally divided every 6 hours) for hepatic encephalopathy
- Vitamin K (10 mg intravenously once daily for 3 days) for coagulopathy
- Empiric antibiotics (ceftriaxone) and antivirals (acyclovir) initially, discontinued after negative infectious workup
- Acid suppression therapy (pantoprazole) for stress ulcer prophylaxis
- Nutritional and fluid support (intravenous fluids followed by nasogastric enteral feeds with high-carbohydrate, moderate-protein content)
Serial laboratory monitoring demonstrated progressive improvement (Table 2). The patient’s mental status improved gradually, with GCS increasing to 12/15 by day 3 and 15/15 by day 5. Hepatic encephalopathy resolved completely by day 7. The patient remained hemodynamically stable throughout hospitalization without the need for vasopressor support.
 |
Table 2 Laboratory Trends During Hospitalization |
Outcome
Over 18 days, she became fully conscious and alert, with complete resolution of jaundice, stable vital signs, adequate oral intake, and normal urine output. At discharge, laboratory evaluation showed INR 1.1, albumin 2.8 g/dL, and near-normalization of transaminases, reflecting recovery of liver function. The patient was discharged home in good condition without the need for liver transplantation. At one-month follow-up, she remained asymptomatic with normal growth and development.
Case Discussion
HAV infection usually results in an acute, self-limiting illness that confers lifelong immunity and only rarely leads to fulminant hepatic failure. Fulminant hepatic failure occurs more commonly in patients with underlying liver disease, particularly chronic hepatitis B or C infection, advanced age, or intravenous drug use.10,11 In this case, a 5-year-old child developed acute Hepatitis A complicated by severe coagulopathy and encephalopathy. A review of the literature reveals few reported cases of pediatric HAV-induced ALF with spontaneous recovery. In a multicenter study by Squires et al, HAV accounted for approximately 4% of pediatric ALF cases in developed countries, with transplant-free survival rates varying by etiology. Our case contributes to the limited data from sub-Saharan Africa, where HAV remains a leading cause of pediatric ALF.12
Hepatitis A is the leading cause of pediatric acute liver failure (PALF) in developing countries, accounting for 28.9% of cases, followed by unspecified infections (9.52%) and Wilson’s disease (7.78%). In contrast, in developed countries, acetaminophen toxicity (9.24%), unspecified metabolic disorders (5.47%), and unspecified infections (5.06%) are the most common etiologies.12 The patient tested positive for HAV IgM, confirming acute Hepatitis A as the cause of liver failure. This aligns with global data and emphasizes the importance of early recognition, supportive management, and preventive vaccination programs in endemic areas. Recent epidemiological data from sub-Saharan Africa indicate that hepatitis A remains endemic, with seroprevalence exceeding 90% in some regions by adolescence, highlighting the public health relevance of this case.
Liver injury in Hepatitis A is believed to result from immune-mediated destruction of infected hepatocytes rather than direct viral toxicity.13 This immune response explains the abrupt elevation of ALT and AST. Encephalopathy develops due to accumulation of ammonia and neurotoxins from impaired hepatic detoxification.13,14 The clinical presentation—coagulopathy, jaundice, and encephalopathy—reflects insufficient functioning liver parenchymal mass to sustain life.15
The King’s College Hospital Criteria for non-acetaminophen-induced ALF include: INR > 6.5, or three of the following: unfavorable etiology (eg., idiosyncratic drug reaction), age < 10 or > 40 years, duration of jaundice before encephalopathy > 7 days, INR > 3.5, and bilirubin > 17 mg/dL.16 In our patient, age < 10 years was the only criterion met, with INR 4.0 (less than the threshold of 6.5) and total bilirubin 8.0 mg/dL (well below 17 mg/dL). Therefore, the patient did not meet the King’s College Criteria for liver transplantation, supporting the decision for conservative management.
Management of acute Hepatitis A is primarily supportive, focusing on hydration, correction of coagulopathy, and prevention of complications such as encephalopathy. Liver transplantation is reserved for patients meeting poor prognostic criteria.16,17 While HAV infection itself carries a favorable prognosis with spontaneous recovery in over 99% of cases, progression to ALF is rare (less than 1%). Among those who develop ALF, outcomes vary widely, with transplant-free survival ranging from 30–60% depending on the severity of encephalopathy and coagulopathy. Several factors may explain spontaneous recovery in this case: the immune-mediated nature of HAV injury allows for hepatocyte regeneration once the immune response resolves; the patient had no underlying chronic liver disease or comorbidities; and timely supportive care optimized nutritional status, controlled encephalopathy, and corrected coagulopathy, allowing time for hepatic regeneration. In this case, the patient improved with supportive therapy alone—lactulose, neomycin, vitamin K, and nutritional support—without requiring transplantation, demonstrating the liver’s regenerative capacity and the clinical significance of spontaneous recovery in resource-limited settings. Regarding neomycin use, while rifaximin is preferred in resource-rich settings due to its favorable side effect profile, neomycin was used in this case due to local availability and affordability constraints.
This case report has several limitations. As a single-case study, the findings are not generalizable to all pediatric patients with HAV-induced ALF. Long-term follow-up beyond one month was not available to assess for potential late sequelae such as persistent liver dysfunction or growth impairment. Additionally, advanced molecular testing (eg., viral genotyping, host genetic factors influencing disease severity) was not performed due to resource constraints. Despite these limitations, this case provides valuable clinical insight into the management of HAV-induced ALF in a resource-limited setting.
Conclusion
This case demonstrates that children with HAV-induced ALF can achieve full recovery with timely supportive care, even without liver transplantation. Lessons for clinicians include the importance of rigorous INR monitoring, ammonia management, and careful airway assessment. This case also highlights the urgent need for universal Hepatitis A vaccination in Somaliland to reduce the burden of this life-threatening condition.
Ethical Approval
In our institute, the ethical approval is not required for publication of case reports, so our hospital is waived for case reports.
Informed Consent
Informed consent was obtained from the patient’s parents (Primary Care giver) for the publication of this case report.
Consent for Publication
Written informed consent was obtained from the patient’s parents (Primary care Giver) for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding for this case.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Kramarov S, Yevtushenko V, Seriakova I. et al. A case report of acute liver failure in a child with hepatitis A virus and Epstein–Barr virus coinfection on the background of autoimmune sclerosing cholangitis. Int Med Case Rep J. 2024;17:801–6. doi:10.2147/IMCRJ.S477802
2. Rh S, et al. Acute liver failure in children. J Pediatr Gastroenterol Nutr. 2017;64(4):663–670.
3. Narkewicz MR, et al. Etiology and outcome of pediatric acute liver failure. J Pediatr. 2016;171:263–268.
4. Jagadisan B, Dhawan A. Acute liver failure in children. Clin Liver Dis. 2020;24(3):471–485.
5. Ciocca M. Clinical course and consequences of hepatitis A infection. Vaccine. 2000;18(Suppl 1):S71–S74. doi:10.1016/S0264-410X(99)00470-3
6. Bigna JJ, et al. Epidemiology of hepatitis A virus infection in sub-Saharan Africa: a systematic review. J Viral Hepat. 2019;26(4):442–452.
7. Shin EC, Sung PS, Park SH. Immune responses and immunopathology in acute and chronic viral hepatitis. Nat Rev Immunol. 2016;16(8):509–523. doi:10.1038/nri.2016.69
8. Deep A, et al. Acute liver failure in children. Lancet Child Adolesc Health. 2022;6(9):628–641.
9. Ahmed K, et al. Revised SCARE guideline: an update for the age of artificial intelligence. Premier J Sci. 2025;2.
10. Rasheed A, Saeed S. Acute hepatitis A virus infection presenting with multiorgan dysfunction: a case report. Cases J. 2009;2:8124. doi:10.4076/1757-1626-2-8124
11. BaAlawi F, Hassan K, Al Maamari K, Balkhair A. Fatal hepatitis A virus infection in an adolescent. IDCases. 2020;20:e00721. doi:10.1016/j.idcr.2020.e00721
12. Berardi G, Tuckfield L, DelVecchio MT, Aronoff S. Differential diagnosis of acute liver failure in children: a systematic review. Pediatr Gastroenterol Hepatol Nutr. 2020;23(6):501–510. doi:10.5223/pghn.2020.23.6.501
13. Debray D, Cullufi P, Devictor D, Fabre M, Bernard O. Acute liver failure in children with hepatitis A. J Pediatr Gastroenterol Nutr. 1996;22(4):433.
14. Dong V, Nanchal R, Karvellas CJ. Pathophysiology of acute liver failure. Nutr Clin Pract. 2020;35(1):24–29. doi:10.1002/ncp.10459
15. Fernández J, Bassegoda O, Toapanta D, Bernal W. Acute liver failure: a practical update. JHEP Rep. 2024;6(9):101131. doi:10.1016/j.jhepr.2024.101131
16. Webb GW, Kelly S, Dalton HR. Hepatitis A and hepatitis E: clinical and epidemiological features, diagnosis, treatment, and prevention. Clin Microbiol Newsl. 2020;42(21):171–179. doi:10.1016/j.clinmicnews.2020.10.001
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.