Back to Journals » International Medical Case Reports Journal » Volume 19
Split Hand/Foot Malformation with Acquired Middle Ear Cholesteatoma Secondary to Eustachian Tube Dysfunction: A Case Report and Literature Review
Authors Yan W, Li L, Mao Y, Lu Y, Sun P, Zhang X, Fan Z, Han Y
Received 18 March 2026
Accepted for publication 30 May 2026
Published 23 June 2026 Volume 2026:19 609036
DOI https://doi.org/10.2147/IMCRJ.S609036
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Wenqing Yan,1 Li Li,1 Yanyan Mao,1 Yanqing Lu,1 Pengcheng Sun,2 Xiaoman Zhang,1 Zhaomin Fan,1 Yuechen Han2
1Department of Otolaryngology-Head and Neck Surgery, Shandong Second Provincial General Hospital, Jinan, People’s Republic of China; 2Department of Otoneurology and Lateral Skull Base Surgery, Shandong Second Provincial General Hospital, Jinan, People’s Republic of China
Correspondence: Yuechen Han, Department of Otoneurology and Lateral Skull Base Surgery, Shandong Second Provincial General Hospital, No. 4, Duanxing West Road, Huaiyin District, Jinan, Shandong, People’s Republic of China, Email [email protected]
Abstract: Cholesteatoma is a rare otologic manifestation in patients with split-hand/foot malformation (SHFM), and previously reported cases have predominantly focused on congenital auricular malformations and external auditory canal atresia rather than acquired middle ear lesions. We herein describe the case of an 8-year-old girl with clinically diagnosed SHFM who presented with left otalgia and persistent purulent otorrhoea. Otoscopic examination revealed middle ear granulation tissue, and high-resolution temporal bone imaging confirmed the presence of middle ear cholesteatoma complicated by tympanic-mastoid bone destruction, semicircular canal fistula, and facial canal erosion. Pure tone audiometry demonstrated a 50 dB air-bone gap indicative of conductive hearing loss. The patient underwent canal wall-down tympanoplasty, which achieved complete cholesteatoma resection and definitive resolution of otorrhea. Considering the patient’s concurrent cleft palate and tympanic membrane retraction, the cholesteatoma in this case is most consistent with an acquired lesion secondary to congenital craniofacial malformation-related eustachian tube dysfunction, rather than a novel phenotypic variant of SHFM. Surgical excision remains the standard definitive treatment for such destructive middle ear lesions. This case expands the spectrum of otological complications associated with SHFM and highlights the importance of routine long-term otologic surveillance, early evaluation, and timely surgical intervention in paediatric SHFM patients to prevent progressive bony erosion, hearing impairment, and potentially life-threatening neurotologic complications.
Keywords: split-hand/foot malformation, cholesteatoma, mastoidectomy, case report
Introduction
Split-hand/foot malformation (SHFM) is a rare congenital limb disorder primarily affecting the central rays of the hands and/or feet, with severity ranging from mild digital changes to monodactyly (only the fifth finger remaining).1 As a heterogeneous genetic syndrome, SHFM and EEC spectrum disorders are associated with multisystem congenital anomalies, among which cleft lip and palate, and otological manifestations are common.2 Previously reported ear complications mainly include structural malformations and hearing loss, whereas acquired middle ear cholesteatoma secondary to cleft palate–related Eustachian tube dysfunction has rarely been documented in this population.3,4
Cholesteatoma is a benign cystic lesion caused by abnormal growth of keratinizing squamous epithelium in the temporal bone. The retraction pocket theory is a key mechanism in acquired middle ear cholesteatoma: chronic negative pressure invaginates the flaccid part of the tympanic membrane, forming a pocket where desquamated keratin debris accumulates.5 This triggers local inflammation, epithelial proliferation, and eventually mature cholesteatoma formation. Lesion-related enzymatic activity leads to progressive destruction of middle ear and mastoid structures. Without timely surgery, cholesteatoma can cause serious complications such as labyrinthine fistula, facial nerve palsy, and intracranial infection, making it a major cause of pediatric otologic morbidity.6
Cleft palate is a well-established risk factor for Eustachian tube dysfunction.7,8 Impaired ventilation and drainage lead to persistent middle ear negative pressure, retraction pocket formation, and recurrent inflammation, collectively promoting acquired cholesteatoma.8 Here in, we report a rare case of SHFM complicated by cleft palate and secondary acquired middle ear cholesteatoma.
Case Presentation
An 8-year-old girl with genetically confirmed SHFM was admitted to our department with a two-year history of persistent purulent discharge in the left ear and recent ear pain and swelling for two months. Seven days before admission, the left mastoid skin had ruptured, causing significant pus discharge, which was temporarily treated with intravenous antibiotics at a local clinic.
Systematic otologic and auxiliary examinations were performed upon admission. Otoscopic examination revealed purulent accumulation and hyperplastic granulation tissue filling the left external auditory canal (Figure 1A). The right tympanic membrane was adherent to the promontory without obvious auricular deformities (Figure 1B and C). Pure tone audiometry demonstrated bilateral conductive hearing loss (Figure 1D). Temporal bone high-resolution computed tomography (HRCT) of the left ear showed soft tissue opacification within the middle ear and mastoid cavity, accompanied by ossicular chain erosion, lateral semicircular canal fistula, and facial canal dehiscence. The right middle ear presented soft tissue opacification with an intact ossicular chain (Figure 1E–H). Magnetic resonance imaging (MRI) and diffusion-weighted imaging (DWI) further verified left middle ear cholesteatoma and incidental right ear cholesterol granuloma (Figure 1I–L).
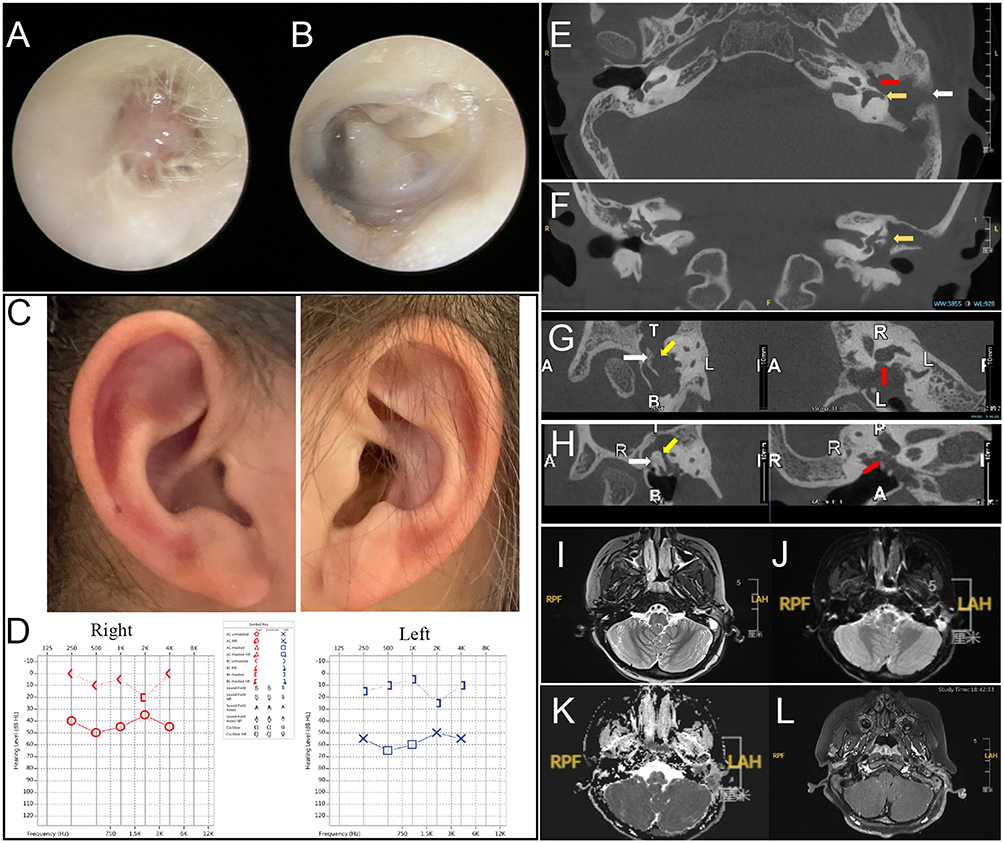 |
Figure 1 (A and B) Otoscopy examination of the bilateral external auditory canals and tympanic membranes. (C) Bilateral auricles unremarkable. (D) Behavioral audiometry confirmed bilateral conductive hearing loss. (E and F) CT demonstrated left fistulae in the horizontal semicircular canal (yellow arrow), mastoid periosteal erosion (white arrow), and facial nerve dehiscence (red arrow). (G and H) CT ossicular reconstruction showed erosion of the left malleus head (white arrow), absent incus (yellow arrow), and lost stapes superstructure (red arrow), contrasting with intact right ossicles (white, yellow, red arrow). (I–L) Preoperative axial MRI identified a left middle ear and mastoid lesion with restricted diffusion on DWI (red arrow). |
Her medical history included congenital cleft lip and palate as well as limb digital deformities. She underwent sequential cleft lip repair at 9 months of age and cleft palate repair at 12 months of age (Figure 2E), and reconstructive surgery for digital malformations two years prior to this admission (Figure 2A–D).
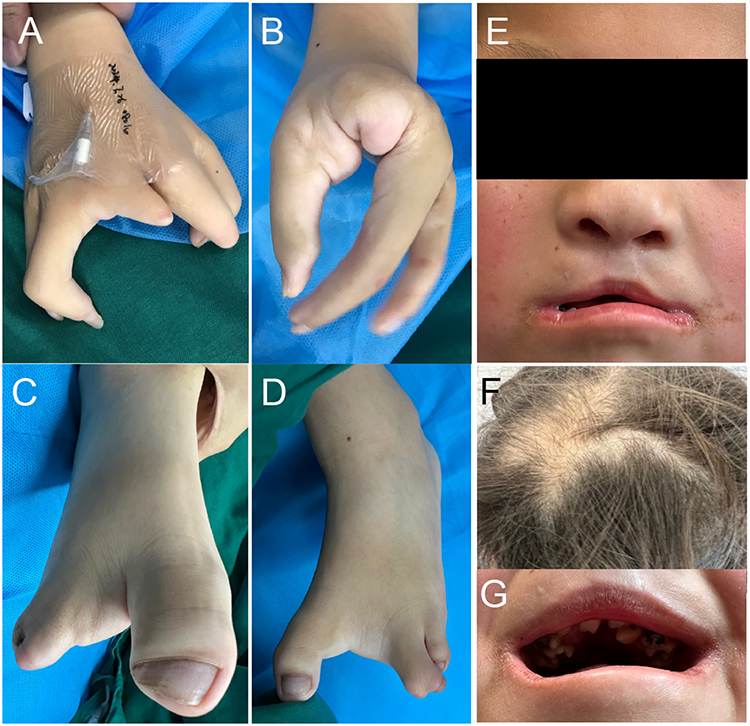 |
Figure 2 (A–D) Congenital deformities of the fingers and toes, with hands shown post-correction. (E) Facial features include a broad nasal tip and status post cleft lip/palate repair. (F) Sparse, yellowish hair. (G) Dental dysplasia. |
Combining the patient’s congenital craniofacial malformations, typical clinical symptoms, and characteristic imaging manifestations, the diagnosis of left acquired middle ear cholesteatoma was established.
Considering the extensive mastoid bone destruction, semicircular canal fistula, and persistent inflammatory exudation, canal wall-down mastoidectomy and tympanoplasty was performed for the left ear to achieve complete cholesteatoma excision and thorough debridement. Elective second-stage canal-wall-up mastoidectomy was planned for the right ear to manage the cholesterol granuloma and middle ear effusion.
Given the rarity of SHFM in otolaryngology and the young age of the patient (8 years), a multidisciplinary safety assessment was conducted. Surgery was scheduled only after laryngoscopy, echocardiography, and other tests confirmed the patient’s suitability for general anesthesia.
Postauricular mastoidectomy was then performed. The cholesteatoma sac (Figure 3A, white arrow) and purulent discharge (Figure 3A, yellow arrow) were meticulously dissected, granulation tissue in the external auditory canal was removed, revealing retraction pockets in the pars flaccida of the tympanic membrane. The mastoid showed localized bone destruction in the middle cranial fossa dura, sigmoid sinus, and horizontal semicircular canal, with intact endosteum (Figure 3B, yellow arrow). Partial erosion of the facial nerve canal exposed the tympanic segment (Figure 3B white arrow). The incus was largely destroyed, and the stapes superstructure was absent, with a mobile footplate (Figure 3B, yellow circle). After complete removal, ossicular chain reconstruction was performed using autologous cartilage and meatoplasty was completed. The goal was to create a safe, dry ear while preserving function.
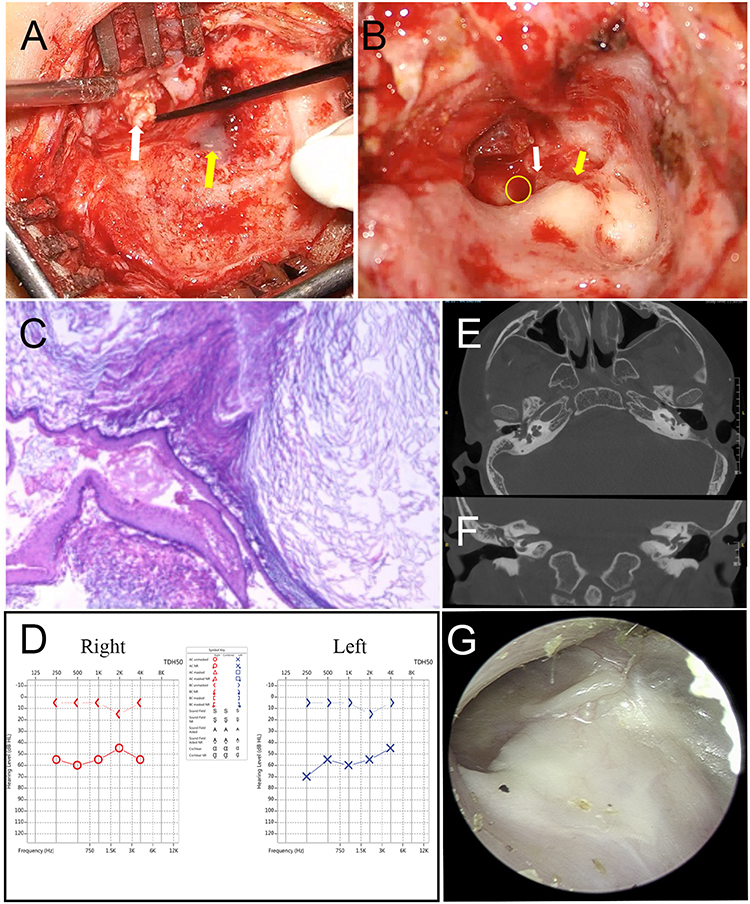 |
Figure 3 (A) Intraoperative photograph demonstrating the cholesteatoma (white arrow) and purulence in the mastoid cavity (yellow arrow). (B) the stapes footplate (yellow round), the horizontal segment of the facial nerve without the bony canal (white arrow), the fistula in the horizontal semicircular canal (yellow arrow). (C) Cholesteatoma confirmed on histology. (D and E) Post-op CT: Tympanic cavity aeration reduced; horizontal semicircular canal fistula repaired. (F) 8-month follow-up: Left ear hearing unchanged (bone conduction normal). (G) Surgical cavity: Well-healed and clean. |
Histopathological examination confirmed a cholesteatoma associated with inflammation (Figure 3C). Postoperatively, facial nerve function remained intact, and hearing was preserved without improvement (Figure 3D).No recurrence was observed during the eight-month follow-up (Figure 3E, F, G).
Discussion
The patient met the diagnostic criteria for Ectrodactyly Ectodermal Dysplasia-Clefting (EEC) syndrome, a subtype of SHFM with the characteristic triad of ectrodactyly, ectodermal dysplasia, and cleft lip/palate (Figure 2E, F, G).9,10 While her developmental milestones were delayed, she achieved basic self-care and communication skills, further consolidating the diagnosis.
Patients with SHFM and EEC syndrome frequently exhibit a range of otologic manifestations.1 The spectrum of ear anomalies documented in the literature includes conductive and sensorineural hearing loss, chronic otitis media, auricular deformities, external auditory canal anomalies, and structural abnormalities of the temporal bone.2,11 However, the development of extensive middle ear cholestatoma remains a rarely reported entity in this specific syndromic context, underscoring the need for detailed otologic evaluation in these patients.
This case may also represent an acquired cholesteatoma from cleft palate-induced ET dysfunction—a known high-risk association.12,13 Persistent recurrent middle ear infection and chronic inflammatory stimulation further promote the progressive formation and expansion of cholesteatoma. This pathogenic hypothesis is strongly supported by our intraoperative finding of an invaginated pocket located in the pars flaccida, which is consistent with the classic invagination pocket theory of acquired cholesteatoma. Retraction pockets induced by sustained middle ear negative pressure secondary to eustachian tube dysfunction serve as the primary prerequisite for cholesteatoma genesis.8,14,15 The scarcity of similar acquired cholesteatoma cases in existing SHFM literature may be attributable to patient attrition caused by early mortality, as well as the clinical tendency to prioritize the management of life-threatening severe congenital malformations over subtle otologic complications.1,2
In addition, patients with cleft lip and palate may have relatively poor prognoses, with high risks of postoperative cholesteatoma recurrence, persistent tympanic cavity effusion, intractable ear fullness, and limited hearing recovery.16,17 Although the present patient achieved complete cholesteatoma resection and resolved otorrhea after surgery, significant hearing impairment persisted. Therefore, regular long-term postoperative otologic surveillance and sequential follow-up are essential for such high-risk patients to monitor lesion recurrence and optimize auditory outcomes.
Organ developmental abnormalities significantly increase the risk of general anesthesia. Before surgery, the patient underwent comprehensive preoperative evaluation, ruling out significant organ abnormalities. The patient had previously undergone three successful general anesthesia procedures. The ALL in these patients facilitated smooth completion of this surgery. Careful attention to potential anomalies and cautious planning are essential, particularly in patients with associated malformations. Thorough preoperative evaluation and meticulous intraoperative monitoring of vital signs are indispensable.
Conclusion
This study reports a rare case of acquired middle ear cholesteatoma in a pediatric patient with genetically confirmed SHFM and concurrent cleft lip and palate. The cholesteatoma is secondary to Eustachian tube dysfunction associated with the cleft palate, underscoring that SHFM patients with craniofacial anomalies are at high risk for progressive otologic complications. As a single case report, this study cannot establish a direct causal relationship between SHFM genotype and cholesteatoma development. Although timely surgical resection successfully eliminated the lesion and controlled acute infection, these patients inherently have unstable middle ear ventilation, predisposing them to postoperative recurrence and persistent hearing impairment.
In conclusion, this case expands the known otologic phenotype of SHFM/EEC syndrome and highlights the need for routine otologic monitoring, early management of Eustachian tube dysfunction, and extended postoperative follow-up in high-risk SHFM patients with craniofacial anomalies. Such systematic care is essential to prevent irreversible middle ear damage and improve long-term outcomes.
Ethical Statement
This study was approved by the Ethics Committee of Shandong Second Hospital (No 2026-022-01), and institutional approval was obtained prior to the collection of all clinical case data and the conduct of the study.
Consent Statement
Written informed consent for the publication of this case report and any accompanying images was obtained from the patient’s parents.
Funding
This study was supported by the National Key Research and Development Program of China (Grant no. 2022YFC2703705).
Disclosure
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest in the subject matter or materials discussed in this manuscript.
References
1. Evans JA, Vitez M, Czeizel A. Congenital abnormalities associated with limb deficiency defects: a population study based on cases from the Hungarian congenital malformation registry (1975–1984). Am J Med Genet. 1994;49(1):52–6. doi:10.1002/ajmg.1320490111
2. Elliott AM, Evans JA, Chudley AE. Split hand foot malformation (SHFM). Clin Genet. 2005;68(6):501–505. doi:10.1111/j.1399-0004.2005.00530.x
3. Lourencone LFM, Koga FDT, Oliveira EB, Jorge JC, de Brito R. Evolution of acquired middle ear cholesteatoma in patients with ectrodactyly, ectodermal dysplasia, cleft lip/palate (EEC) syndrome. Otol Neurotol. 2018;39(8):e679–e82. doi:10.1097/MAO.0000000000001921
4. Yang Y, Huang L-Y, Han J, Li D-Z. Prenatal diagnosis of Ectrodactyly–Ectodermal dysplasia–Cleft (EEC) syndrome in a Chinese woman with a TP63 mutation. Eur J Obstet Gynecol Reprod Biol. 2017;213:146–147. doi:10.1016/j.ejogrb.2017.04.012
5. Hamed MA, Nakata S, Sayed RH, et al. Pathogenesis and bone resorption in acquired cholesteatoma: current knowledge and future prospectives. Clin Experim Otorhinolaryngol. 2016;9(4):298–308. doi:10.21053/ceo.2015.01662
6. Diom ES, Cisse Z, Tall A, et al. Management of acquired cholesteatoma in children: a 15 year review in ENT service of CHNU de FANN Dakar. Int J Pediatr Otorhinolaryngol. 2013;77(12):1998–2003. doi:10.1016/j.ijporl.2013.09.021
7. Doyle WJ, Cantekin EI, Bluestone CD. Eustachian tube function in cleft palate children. Ann Otol Rhinol Laryngol. 1980;89(3_suppl):34–40. doi:10.1177/00034894800890s311
8. Matsuzawa S, Iino Y, Yamamoto D, et al. Attic cholesteatoma with closure of the entrance to pars flaccida retraction pocket. Auris Nasus Larynx. 2017;44(6):766–770. doi:10.1016/j.anl.2016.11.014
9. Yang W, Zhou J, Si N, Zhang X. A NovelTP63Missense mutation in the sumoylation motif causes isolated split-hand/foot malformation 4: a pedigree report and literature review. Mol Genet Genomic Med. 2025;13(9):e70140. doi:10.1002/mgg3.70140
10. van Bokhoven H, Hamel BCJ, Bamshad M, et al. p63 gene mutations in EEC syndrome, limb-mammary syndrome, and isolated split hand–split foot malformation suggest a genotype-phenotype correlation. Am J Hum Genet. 2001;69(3):481–492. doi:10.1086/323123
11. Buss PW, Hughes HE, Clarke A. Twenty-four cases of the EEC syndrome: clinical presentation and management. J Med Genet. 1995;32(9):716–723. doi:10.1136/jmg.32.9.716
12. Harris L, Cushing SL, Hubbard B, Fisher D, Papsin BC, James AL. Impact of cleft palate type on the incidence of acquired cholesteatoma. Int J Pediatr Otorhinolaryngol. 2013;77(5):695–698. doi:10.1016/j.ijporl.2013.01.020
13. Martin HL, Poehlein ER, Allori AC, et al. Relevance of cleft palatal width in short-term otologic outcomes. Int J Pediatr Otorhinolaryngol. 2023;171:111647. doi:10.1016/j.ijporl.2023.111647
14. Patel TR, Welch CM. The Science of Cholesteatoma. Otolaryngol Clin North Am. 2025;58(1):1–27. doi:10.1016/j.otc.2024.07.022
15. Austin DF. The retraction pocket in the treatment of cholesteatoma. Arch Otolaryngol. 1976;102(12):741–743. doi:10.1001/archotol.1976.00780170059009
16. Stangerup S-E, Drozdziewicz D, Tos M. Cholesteatoma in children, predictors and calculation of recurrence rates. Int J Pediatr Otorhinolaryngol. 1999;49(Suppl 1):S69–73. doi:10.1016/s0165-5876(99)00136-6
17. Chao WY, Tseng HZ, Chang SJ. Eustachian tube dysfunction in the pathogenesis of cholesteatoma: clinical considerations. J Otolaryngol. 1996;25(5):334–338.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Role of Stepwise Imaging in the Diagnosis and Management of Cholesteatoma in a Resource-Limited Setting: A Case Report
Hassan SA, Mukhtar MY, Osman MH, Mohamed AA
International Medical Case Reports Journal 2025, 18:1593-1597
Published Date: 11 December 2025