Back to Journals » International Medical Case Reports Journal » Volume 18
Splenectomy for Primary Sjögren’s Syndrome Associated with Massive Splenomegaly: Two Case Reports
Authors Gui F, Zhou LX, Liu XM, He YL, Yang QB
Received 9 May 2025
Accepted for publication 25 July 2025
Published 4 August 2025 Volume 2025:18 Pages 963—968
DOI https://doi.org/10.2147/IMCRJ.S539313
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Fang Gui,* Li-Xuan Zhou,* Xue-Mei Liu, Yong-Long He, Qi-Bin Yang
Department of Rheumatology and Immunology, Affiliated Hospital of North Sichuan Medical College, Nanchong, Sichuan, 637000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qi-Bin Yang, Department of Rheumatology and Immunology, Affiliated Hospital of North Sichuan Medical College, 1 Maoyuannan Road, Nanchong, Sichuan, 637000, People’s Republic of China, Tel +86-817-259-8221, Email [email protected]
Background: Primary Sjögren’s syndrome (pSS) is an autoimmune disease characterized by exocrine glands involving mainly the lacrimal and salivary glands. Splenomegaly from pSS is a rare clinical feature unless the pSS is complicated by lymphoma. Splenectomy could exclude malignant lymphoma, reduce the risk of spontaneous spleen rupture and remove hypersplenism to improve pancytopenia.
Case Presentation: We reported the case of a 49-year-old female patient who was diagnosed with pSS according to dry mouth, dry eyes, splenomegaly, multiple positive autoantibodies, positive Schirmer’s test and biopsy of labial gland with decreased number of acini and focal lymphocytic infiltration. Due to hematological involvement and liver dysfunction repeatedly, the pSS patient was admitted to the hospital and treated with glucocorticoids, immunosuppressants and hepatoprotective drugs. However, the pancytopenia failed to improve. Considering pancytopenia of the pSS patient caused by massive splenomegaly, splenectomy was recommended to the patient. The hematological involvement was significantly improved after splenectomy. Besides, another 46-year-old woman with a similar clinical manifestation was diagnosed with pSS complicated by massive splenomegaly, however, the patient refused to undergo the splenectomy.
Conclusion: Splenectomy may be an effective treatment of pSS complicated by massive splenomegaly resulting in hematological involvement.
Keywords: Sjogren’s syndrome, splenomegaly, splenectomy, autoimmune diseases, case report
Introduction
Primary Sjögren’s syndrome (pSS) is a chronic inflammatory autoimmune disease of unknown origin, attacking in particular the tear and salivary glands.1 Sicca symptoms are the most common manifestation of the pSS which may also present with various organ manifestations such as the skin, lung, liver and blood.2 It was reported in the literature that the hematological involvement is one of the most commonly affected systems of pSS with an incidence of 31.5%.3 It can be manifested as thrombocytopenia, anemia and leukopenia, which can occur in single or multiple lineages at the same time. In addition, liver involvement is the most common non-exocrine complication of pSS.4 However, splenomegaly as the clinical manifestation of pSS is rare. Here, we reported two cases of massive splenomegaly from pSS. Considering hematological involvement caused by massive splenomegaly after exclusion of secondary factors including viral infection, tumors and drugs, splenectomy was recommended to the patient who failed to respond to treatment with glucocorticoids and immunosuppressants. We thought it was important to share our clinical experience on this rare topic of pSS complicated by massive splenomegaly. Splenectomy is viewed as a standard treatment for some hematological diseases, such as hereditary spherocytosis (HSC), idiopathic thrombocytopenic purpura (ITP).5 With a deeper understanding of the mechanism of splenectomy, splenectomy has been applied to certain secondary hematological dysfunction changes. It had a good curative effect in rheumatic diseases such as refractory immune thrombocytopenia secondary to systemic lupus erythematosus.6 Written informed consent was obtained from the patient for publication of the case report. This manuscript adheres to the applicable CARE guideline.
Case Presentation
Case 1
A 49-year-old female patient who was admitted to the hospital presented with a diagnosis of primary Sjögren’s syndrome based on a history of eye and mouth dryness, and oral ulcers. Physical examination was normal except for splenomegaly. A series of examinations at hospital revealed massive splenomegaly (length 15cm) with an abdominal ultrasonic imaging (sonography), abnormal liver function [aspartate aminotransferase (AST): 499 U/L, alanine aminotransferase (ALT): 383 U/L] and blood routine [white blood cells (WBC): 3.18*109/L, Hemoglobin (Hb): 116 g/L, platelet (PLT): 192*109/L]. Laboratory autoantibody test showed multiple positive autoantibodies (antinuclear antibody: 1:100 +, anti-SS-A antibody 50.70 RU/mL, anti-Jo-1 antibody 28.17 RU/mL). Autoimmune-related hepatopathy antibodies, Epstein-Barr virus, cytomegalovirus, hepatitis B virus antibody and hepatitis C virus antibody showed no abnormality. Bone marrow aspiration showed that bone marrow cells were not abnormal by morphology and flow cytometry. The Schirmer’s test was positive. Biopsy of labial gland showed a mild decrease of acini with focal lymphocytic infiltration (more than 50 cells/focus). These findings were consistent with primary Sjögren’s syndrome. According to a previous report,3 the hematological involvement was considered to be caused by Sjögren’s syndrome. To explore the reasons of the liver injury, liver biopsy was performed. The pathological biopsy indicated that the liver suffered from chronic inflammation. The patient had no evidence of viral hepatitis, drug-induced liver injury, liver tumor or biliary tract disease. Her liver dysfunction was considered to be Sjögren’s syndrome-related immune liver injury. Compound glycyrrhizin and glutathione were given for liver treatment. At the same time, methylprednisolone 40 mg once daily and mycophenolate mofetil 500 mg twice daily was used to induce remission of disease activity. The patient was discharged after liver improvement.
The patient as an outpatient took methylprednisolone and mycophenolate mofetil regularly. Follow-up examination in the outpatient department showed significant abnormal liver function (AST: 907 U/L, ALT: 1050 U/L) and pancytopenia (WBC: 1.33*109/L, neutrophil: 0.64*109/L, Hb: 96 g/L, PLT: 88*109/L). She was admitted to the hospital for the second time. Bone marrow aspiration showed active nucleocyte proliferation, decreased granulocyte ratio, increased erythroid ratio, and myelogram of hemophagocytosis. Epstein-Barr Virus DNA was 1.5*104 Copies/mL (positive). The diagnosis of hemophagocytic syndrome was lack of evidence according to the normal ferritin, blood lipids, fibrinogen, soluble CD25 receptor and NK cells activity. Considering abnormal liver function and pancytopenia associated with Epstein-Barr virus infection, the patient was treated with ganciclovir for 3 weeks, reexamination of liver enzymes (AST: 28U/L, ALT: 38U/L), blood routine (WBC: 3.13*109/L, neutrophil: 1.52*109/L, Hb: 97g/L, PLT: 163*109/L), Epstein-Barr virus DNA (not detected) were significantly improved after that treatment. The patient was discharged and recommended with therapeutic strategy of Sjögren’s syndrome with methylprednisolone 32 mg once daily, hydroxychloroquine 200 mg and mycophenolate mofetil 500 mg twice daily.
The dosage of methylprednisolone was regularly reduced to 12 mg once daily. The blood routine and liver function tests were performed at a local hospital. She was admitted to the hospital for a third time due to the detection of pancytopenia (WBC: 1.59*109/L, neutrophil: 0.58*109/L, Hb: 90 g/L, PLT: 72*109/L) and liver dysfunction (AST: 487 U/L, ALT: 283 U/L). Epstein-Barr virus DNA showed less than 4.0*102 Copies/mL (negative), abnormal liver function was irrelevant to Epstein-Barr virus. Bone marrow aspiration showed that morphology of bone marrow cells was not abnormal to exclude hematonosis. The abdominal computer tomography (CT) scan showed massive splenomegaly (length 19.0 cm × width 5.2 cm) (Figure 1). According to the previous report,7 the patient had a diagnosis of pSS associated with massive splenomegaly resulting in the hematological involvement. Splenectomy was recommended to the patient in order to improve pancytopenia. With hepatoprotective drugs treatment for one week, the liver enzymes recovered to normal levels (Figure 2). With the approval of the patient, splenectomy was performed using laparoscopy by the gastrointestinal surgeon. The immunohistochemical staining of the spleen (Figure 3) showed that CD20, CD23 and CD79a were positive in the white medulla area, CD3, CD5 were positive in the red medulla area, 20% of Ki-67 was positive, Cyclin D1 was negative. The lymphoma was excluded according to the immunohistochemical staining. As shown in Figure 4, the pancytopenia was improved after 3 days of the splenectomy (WBC: 5.05*109/L, neutrophil: 3.54*109/L, Hb: 102 g/L, PLT: 208*109/L). The patient was discharged and followed up regularly in the outpatient department.
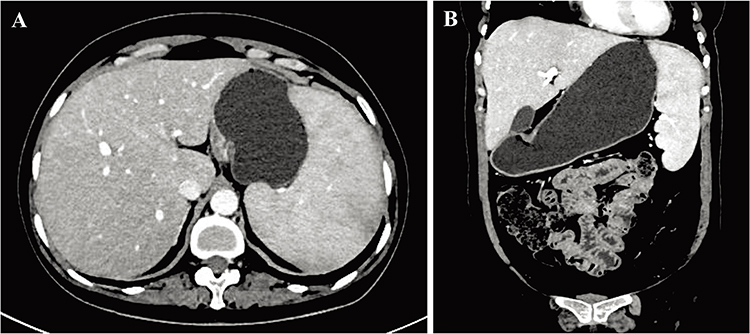 |
Figure 1 Abdominal changes shown by enhanced computer tomography (CT) scan. Splenomegaly shown in the axial (A) plus coronal (B) plane. |
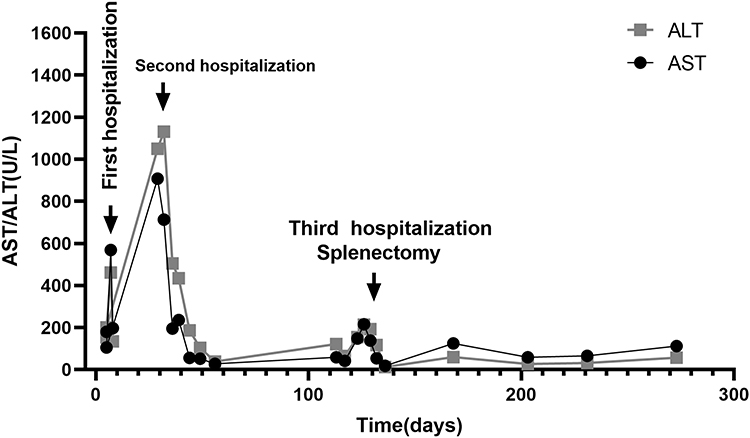 |
Figure 2 The record of liver transaminase before and after splenectomy began with the first hospitalization. |
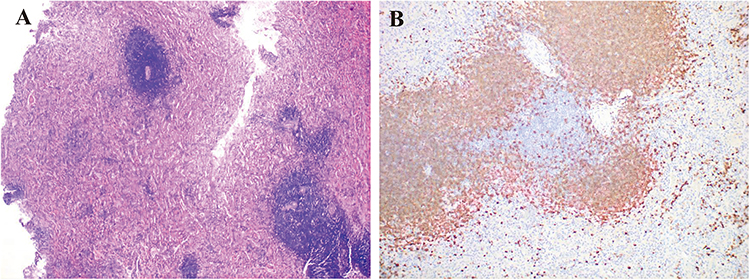 |
Figure 3 The immunohistochemical staining of the spleen. (A) Histiocytic hyperplasia in the red medulla area. (B) Lymphocytosis in the white medulla area. |
 |
Figure 4 The record of blood routine before and after splenectomy began with the first hospitalization. |
Case 2
A 46-year-old woman who was admitted to hospital presented with eye and mouth dryness, progressive abdominal distention and pancytopenia (white blood cell 2.67*109/L, hemoglobin 92 g/L, platelet 60*109/L). Physical examination was normal except for splenomegaly. Laboratory autoantibody test showed multiple positive autoantibodies (anti-ANA1:320+, anti-Ro52+). The Schirmer’s test was positive, and emission computed tomography (ECT) examination of salivary glands showed extremely poor uptake and secretion. Abdominal magnetic resonance imaging (MRI) revealed massive splenomegaly (length 22.1 cm) (Figure 5A and B). Bone marrow cells were not abnormal by morphology and flow cytometry. These findings were consistent with primary Sjögren’s syndrome. According to a previous report,7 the massive splenomegaly was considered to be caused by Sjögren’s syndrome. Although splenectomy as the best treatment was recommended, the patient refused to perform the splenectomy. She was discharged from hospital without special treatment and lost to follow-up visit.
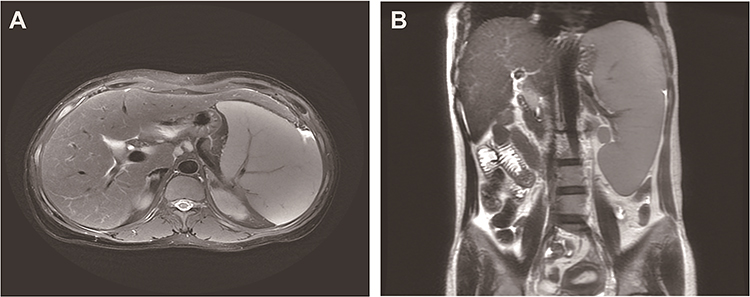 |
Figure 5 Abdominal changes shown by magnetic resonance imaging (MRI) scan. Splenomegaly shown in the axial (A) plus coronal (B) plane. |
Discussion
Primary Sjögren’s syndrome is an autoimmune disease that mainly affects exocrine glands such as the salivary and lacrimal glands. Due to the wide variety of signs and symptoms, patients with Sjögren’s syndrome at the first consultation may visit a diverse range of healthcare practitioners, including ophthalmologists, dentists, ENT specialists and even family physicians.8
It has been reported that up to 34% of pSS patients reported episodic or chronic, typically bilateral swelling of the parotid glands.9 10~20% of pSS patients had abnormal liver function.10 Hematological involvement of pSS patients is also common, such as leukopenia and thrombocytopenia.11 However, the pathogenesis of pSS complicated by hematological involvement is still poorly understood. It is known that the pathogenesis is mostly attributed to T cells dysfunction, the effect of B cells producing autoantibodies, a variety of autoantibodies or immune complexes presenting in the peripheral circulating blood and destroying peripheral blood cells. Once the decline of one or more hematopoietic cell lineages occurs in pSS, the cause should firstly be the primary disease. Meanwhile, the other factors, such as virus infection, tumor, drugs and so on, should be excluded. The principle of treatment is mainly focused on the pSS with the glucocorticoids and immunosuppressants.
For the patient of case 1, combination of methylprednisolone and mycophenolate mofetil were used to induce remission of disease activity. The hematological involvement was not significantly improved (Figure 4). Therefore, hematological involvement in the pSS may be a result of massive splenomegaly associated with the pSS. Splenomegaly from pSS is a rare clinical feature unless the disease is complicated by lymphoma. It is essential to exclude malignant non-Hodgkin lymphoma (NHL) which occurrs in about 5% of patients with pSS, who are at a significantly increased risk of developing NHL compared with the general population (risk ratio [RR]: 13.7).12 Notably, a current research reported 2.6% of lymphoma prevalence in pSS, lower than previously reported in the literature.13 To our knowledge, splenectomy as the best treatment was recommended to the patient with pSS complicated by massive splenomegaly. Splenectomy was reported to exclude malignant lymphoma, reduce the risk of spontaneous spleen rupture and remove hypersplenism to improve pancytopenia.7 In this reported case, the pancytopenia was quickly improved after the splenectomy (Figure 4). Notably, as shown in Figure 4, the dramatically increased platelet levels peaked 4 weeks later and recovered to the normal level by 6 months later.
It is suggested that splenectomy is an effective treatment of primary Sjögren’s syndrome complicated by massive splenomegaly resulting in hematological involvement.
Conclusion
Massive splenomegaly is a rare clinical manifestation of pSS. Particularly, hematological involvement attributed to massive splenomegaly. Splenectomy may be considered for the pSS patient who has failed to respond to treatment with glucocorticoids and immunosuppressants. In this study, we reported that splenectomy was an effective treatment of pSS complicated for massive splenomegaly resulting in hematological involvement.
Ethical Approval
The institutional approval for the study of the case was not required to publish the case details.
Patient Consent for Publication`
Written informed consent obtained from the patients.
Acknowledgments
We thank gastrointestinal surgeon Dr. Jin Tang for the splenectomy.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by National Natural Science Foundation of China (81800776), Science and Technology Strategic Cooperation Program between Nanchong City and University (20SXQT0167) and Doctoral Scientific Research Foundation of North Sichuan Medical College (CBY20-QD07). The funders had no role in the study design, data collection, analysis, or interpretation of the data, or in writing the manuscript or the decision to submit the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Negrini S, Emmi G, Greco M, et al. Sjögren’s syndrome: a systemic autoimmune disease. Clin Exp Med. 2022;22(1):9–25. doi:10.1007/s10238-021-00728-6
2. Cornec D, Devauchelle-Pensec V, Mariette X, et al. Severe health-related quality of life impairment in active primary Sjögren’s syndrome and patient-reported outcomes: data from a large therapeutic trial. Arthritis Care Res. 2017;69(4):528–535. doi:10.1002/acr.22974
3. Nocturne G, Mariette X. Sjögren syndrome-associated lymphomas: an update on pathogenesis and management. Br J Haematol. 2015;168(3):317–327. doi:10.1111/bjh.13192
4. Kaplan MJ, Ike RW. The liver is a common non-exocrine target in primary Sjögren’s syndrome: a retrospective review. BMC Gastroenterol. 2002;2:21. doi:10.1186/1471-230X-2-21
5. Marble KR, Deckers PJ, Kern KA. Changing role of splenectomy for hematologic disease. J Surg Oncol. 1993;52(3):169–171. doi:10.1002/jso.2930520310
6. You YN, Tefferi A, Nagorney DM. Outcome of splenectomy for thrombocytopenia associated with systemic lupus erythematosus. Ann Surg. 2004;240(2):286–292. doi:10.1097/01.sla.0000133182.92780.9c
7. Appel H, Loddenkemper C, Rohweder J, Rudwaleit M, Zeitz M, Sieper J. Massive splenomegaly and hypersplenism in a young woman with primary Sjogren’s syndrome. J Rheumatol. 2002;29(9):2012–2013.
8. Stefanski AL, Tomiak C, Pleyer U, Dietrich T, Burmester GR, Dorner T. The diagnosis and treatment of sjogren’s syndrome. Deutsches Arzteblatt Int. 2017;114(20):354–361. doi:10.3238/arztebl.2017.0354
9. Ramos-Casals M, Brito-Zeron P, Solans R, et al. Systemic involvement in primary sjogren’s syndrome evaluated by the EULAR-SS disease activity index: analysis of 921 Spanish patients (GEAS-SS registry). Rheumatology. 2014;53(2):321–331. doi:10.1093/rheumatology/ket349
10. Csepregi A, Szodoray P, Zeher M. Do autoantibodies predict autoimmune liver disease in primary sjogren’s syndrome? Data of 180 patients upon a 5 year follow-up. Scand J Immunol. 2002;56(6):623–629. doi:10.1046/j.1365-3083.2002.01165.x
11. Manganelli P, Fietta P, Quaini F. Hematologic manifestations of primary sjogren’s syndrome. Clin Experiment Rheumatol. 2006;24(4):438–448.
12. Nishishinya MB, Pereda CA, Munoz-Fernandez S, et al. Identification of lymphoma predictors in patients with primary sjogren’s syndrome: a systematic literature review and meta-analysis. Rheumatol Int. 2015;35(1):17–26. doi:10.1007/s00296-014-3051-x
13. Saleh W, Elashry MM, Winn N, Mona M, Katz J, Cha S. A lower prevalence of malignant lymphoma in Sjögren’s syndrome patients: a cross-sectional study. Oral Dis. 2023;29(8):3313–3324. doi:10.1111/odi.14435
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.