Back to Journals » Hepatic Medicine: Evidence and Research » Volume 14
Splenectomy Combined with Endoscopic Variceal Ligation (EVL) versus EVL Alone for Secondary Prophylaxis of Variceal Bleeding in Hepatosplenic Schistosomiasis: A Retrospective Case–Control Study
Authors Rakotomalala JA ![]() , Razafindrazoto CI
, Razafindrazoto CI ![]() , Randriamifidy NH
, Randriamifidy NH ![]() , Ralaizanaka BM
, Ralaizanaka BM ![]() , Maherison S, Hasina Laingonirina DH
, Maherison S, Hasina Laingonirina DH ![]() , Rakotomaharo M
, Rakotomaharo M ![]() , Rasolonjatovo AS, Rakotovao MA, Rakotozafindrabe ALR
, Rasolonjatovo AS, Rakotovao MA, Rakotozafindrabe ALR ![]() , Rabenjanahary TH
, Rabenjanahary TH ![]() , Fanantenantsoa R, Razafimahefa SH, Ramanampamonjy RM
, Fanantenantsoa R, Razafimahefa SH, Ramanampamonjy RM
Received 24 March 2022
Accepted for publication 12 May 2022
Published 18 May 2022 Volume 2022:14 Pages 79—85
DOI https://doi.org/10.2147/HMER.S367849
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gerry Lake-Bakaar
Jolivet Auguste Rakotomalala,1 Chantelli Iamblaudiot Razafindrazoto,2 Nitah Harivony Randriamifidy,2 Behoavy Mahafaly Ralaizanaka,3 Sonny Maherison,2 Domoina Harivonjy Hasina Laingonirina,2 Mialitiana Rakotomaharo,2 Anjaramalala Sitraka Rasolonjatovo,2 Mamisoa Anicet Rakotovao,4,5 Andry Lalaina Rinà Rakotozafindrabe,2 Tovo Harimanana Rabenjanahary,2 Rija Fanantenantsoa,4,5 Soloniaina Hélio Razafimahefa,3 Rado Manitrala Ramanampamonjy2
1Hepato-Gastroenterology Unit, University Hospital Mahavoky Atsimo, Mahajanga, Madagascar; 2Gastroenterology Unit, University Hospital Joseph Raseta Befelatanana, Antananarivo, Madagascar; 3Hepato-Gastroenterology Unit, University Hospital Andrainjato, Fianarantsoa, Madagascar; 4General Surgery Unit, University Hospital Andrainjato, Fianarantsoa, Madagascar; 5Visceral Surgery Unit, University Hospital Tambohobe, Fianarantsoa, Madagascar
Correspondence: Chantelli Iamblaudiot Razafindrazoto, Gastroenterology Unit, University Hospital Joseph Raseta Befelatanana, Antananarivo, Madagascar, Email [email protected]
Background: Hepatosplenic schistosomiasis (HSS) is one of the most common causes of portal hypertension in developing countries. Variceal bleeding is the most common cause of mortality during HSS. The objective of this study was to evaluate the efficacy of splenectomy associated with endoscopic variceal ligation (EVL) compared with EVL alone in preventing variceal bleeding in patients with HSS.
Methods: This was a single-center, retrospective, case–control study. Between January 2015 and December 2019, a total of 59 patients with HSS who had at least one variceal bleeding episode and received EVL with or without splenectomy were identified and stratified. In this case–control design, 22 patients had splenectomy + EVL (case group) and 37 patients had EVL alone (control group). The main endpoints were the rate of variceal rebleeding and the mortality rate between the two groups.
Results: The mean age of our patients was 39.92 ± 13.4 (19– 75) years with a sex ratio of 1.8. The recurrence rate of variceal bleeding was significantly lower in the case group (splenectomy + EVL) than in the control group (EVL alone) (4.45% vs 27.2%, p = 0.041). There was no significant difference between the two groups in terms of mortality (4.54 vs 2.7%, p = 1.00).
Conclusion: Splenectomy combined with EVL was effective than EVL alone in preventing variceal rebleeding in patients with HSS.
Keywords: endoscopic variceal ligation, mortality, variceal bleeding, hepatosplenic schistosomiasis, splenectomy
Background
Schistosomiasis or bilharzia is the second most common parasitic endemic disease worldwide after malaria. It remains a global public health problem; it is endemic in 78 countries around the world, and of the 207 million people with schistosomiasis, 85% live in Africa, including Madagascar.1 In Madagascar, Schistosoma mansoni intestinal bilharzia, threatening 2.5 million people, of whom two million are infected. It is prevalent in the east, south and highlands of the country. Two to ten percent of patients infected with Schistosoma mansoni and Schistosoma japonicum develop the hepatosplenic form of the disease, which is characterized by periportal hepatic fibrosis, pre-sinusoidal portal hypertension and splenomegaly. Variceal bleeding is a major cause of morbidity and mortality in patients with non-cirrhotic portal hypertension in developing countries. Hepatosplenic schistosomiasis (HSS) is complicated by variceal bleeding in 40% of cases with a mortality of 11% in the first episodes of bleeding.2,3 Secondary prevention of variceal bleeding in schistosomiasis-related portal hypertension does not present any particularities and calls upon the usual methods such as endoscopic variceal ligation (EVL) and non-selective betablockers. However, EVL still results in a similarly high rate of hemorrhagic recurrence, approximately 30%, and does not relieve portal hypertension and hypersplenism.4 Theoretically, the combination of splenectomy and EVL should correct not only portal hypertension but also hypersplenism, and thus prevent variceal bleeding.4 To our knowledge, there is no consensus to date on the secondary prevention of variceal bleeding in patients with HSS. This has been the subject of numerous studies based on different medical, endoscopic and surgical methods, including splenectomy associated with EVL.5–8 Recently, several case series indicate that combining surgical and endoscopic therapy may be more efficacious than using one technique alone.5–8 In fact, a retrospective study showed that endoscopic sclerotherapy was more effective in patients who had previously undergone surgical treatment for portal hypertension.5–8 The efficacy of combined surgical and endoscopic treatment in the secondary prevention of variceal bleeding in hepatosplenic schistosomiasis was reported in a recent Phase III randomized trial comparing sclerotherapy alone to sclerotherapy combined with surgery.9 The objective of this study was to evaluate the efficacy of the combination of EVL and splenectomy compared to EVL alone in the secondary prophylaxis of variceal bleeding in HSS patients in Madagascar.
Methods
Study Design, Participants, and Endpoints
This was a retrospective, single-center, case–control study conducted at the Gastroenterology Unit, University Hospital (UH) Joseph Raseta Befelatanana, Antananarivo, over a period of 5 years (60 months), from January 2015 to December 2019.
Our study concerned all patients with HSS, having at least one episode of variceal bleeding, treated by EVL with or without splenectomy. All patients meeting the following criteria were included in this study: having a diagnosis of HSS, having at least one episode of variceal bleeding and being managed by EVL. These patients were divided into 2 groups: the “Case” group included patients with splenectomy + EVL and the “Control” group included patients with EVL alone. The exclusion criteria were as follows: (a) HSS associated with cirrhosis of any cause or portal vein thrombosis, (b) HSS without variceal bleeding before EVL or before splenectomy.
The efficacy of each method was evaluated with respect to the rate of recurrence of variceal bleeding and the mortality rate.
Definitions
Hepatosplenic schistosomiasis diagnostic criteria were the following: (a) presence of splenomegaly, (b) presence of periportal fibrosis, (c) presence of radiological and/or endoscopic evidence of portal hypertension, and (d) positive schistosomiasis serology.
Esophageal varices were graded for size according to BAVENO VI: Grade 1 (Esophageal varices disappearing on insufflation), Grade 2 (Esophageal varices not disappearing on insufflation, nonconfluent), and Grade 3 (Esophageal varices not disappearing on insufflation, confluent).10
Splenomegaly was classified according to Hackett’s criteria (WHO, 1963) into five categories ranging from 0 to 5: spleen not palpable, even in deep inspiration, was classified as 0, and spleen descending well below the umbilicus, exceeding the line passing between the umbilicus and the pubic symphysis was classified 5.
An episode of variceal bleeding was retained by the combination of several criteria: evidence of portal hypertension, presence of esophageal varices with red signs or recent upper gastrointestinal bleeding (hematemesis and/or melena).
Management of Variceal Bleeding Episodes and Description of Procedures (EVL and Splenectomy)
Patients with variceal bleeding (first episode or recurrence) were hospitalized and supportively cared according to a standardized protocol, and EVL sessions were scheduled every 4 weeks. A non-selective beta-blocker such as propranolol was administered during hospitalization, in the absence of contraindications, at a starting dosage of 20 mg daily, increased every 3 days up to a total daily dose of 80–160 mg daily, to achieve the target heart rate (HR) between 55 and 60 beats/min or a decrease in HR of 25% from baseline HR. EVL was continued in all patients at 4-week intervals until eradication of esophageal varices. Splenectomy was performed in the Visceral Surgery Unit.
The indication for splenectomy in all patients in the splenectomy + EVL group was presence of significant splenomegaly associated with hypersplenism.
EVL consisted of the placement of rubber rings on variceal columns, which are sucked into a plastic hollow cylinder attached to the tip of the endoscope by an experienced senior endoscopist. Ligation was started at the lower end of the esophagus and proceeded upward in a spiral fashion. Splenectomy was performed open by an experienced senior surgeon but without esophagogastric devascularization.
Statistical Analysis
The data were recorded in predesigned formats and were statistically analyzed using Statistical Package for Social Sciences (SPSS) version 16 software. Data were expressed as mean ± standard deviation (SD) and number (percent) for nominal data. Comparisons between two groups were performed using Student’s t-test for parametric data and the Mann–Whitney test for nonparametric data. The chi-square (χ2) test and Fisher exact test were applied for analysis of categorical data. All P-values are two-tailed, with values <0.05 considered statistically significant.
Results
Characteristics of Study Population
During the study period, 68 patients had HSS, with at least one episode of variceal bleeding, treated by EVL with or without splenectomy. Fifty-nine patients were selected, including 22 patients in the case group (EVL + splenectomy) and 37 patients in the control group (EVL alone). Nine patients were excluded: 3 patients had a combination of HSS and cirrhosis, and 6 patients had unworkable records. The flow-chart of the study showed in Figure 1. The two groups are probably not similar in terms of severity of portal hypertension because the mean number of previous bleeding episodes was higher in the case group compared with the control group (3.25 ± 3.07 vs 2.24 ± 1.52, p = 0.003). All other characteristics of our study population were similar in both groups. The demographic and clinical characteristics of patients between the two groups are shown in Table 1.
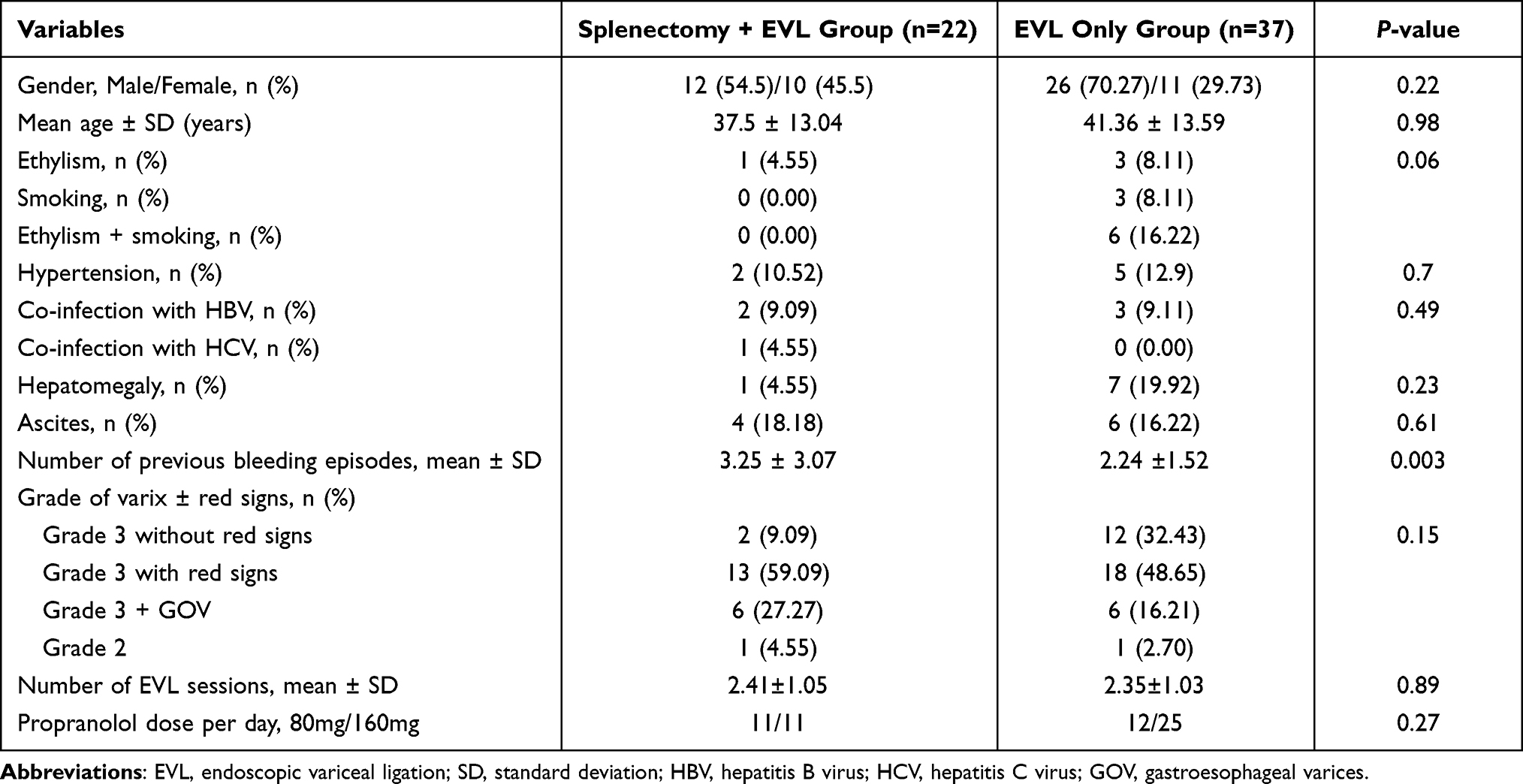 |
Table 1 Baseline Characteristic of Patients |
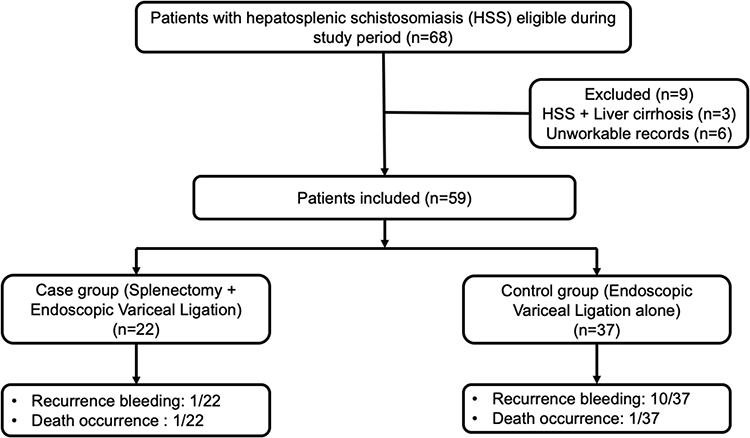 |
Figure 1 Flowchart of study. |
Treatment Outcomes
The rate of variceal bleeding recurrence was significantly lower in the case group (EVL + splenectomy) than the control group (EVL alone) (4.45% vs 27.2%, p = 0.041). There was no significant difference between the two groups in terms of mortality (1/22 vs 1/37, p = 1.00) (Table 2). One 22-year-old patient in the case group died of bacterial pneumonia with severe sepsis and one 59-year-old patient in the control group died of variceal bleeding with shock.
 |
Table 2 Hemorrhagic Recurrence and Death Occurrence |
Discussion
We conducted a retrospective case–control study in patients with HSS who presented with variceal bleeding and were managed in the Gastroenterology Unit, UH Joseph Raseta Befelatanana, Antananarivo. The objective of this study was to evaluate the efficacy of EVL associated with splenectomy compared to EVL alone in the context of secondary prevention of variceal bleeding.
To our knowledge, this was the first Malagasy study comparing these two therapeutic methods, which is the main focus of our study.
The seriousness of HSS lies in the risk of variceal bleeding episodes which could be fatal in the absence of adequate emergency management. The prevention of recurrent bleeding is a crucial element to decrease the risk of morbidity and mortality related to this pathology. Indeed, HSS is a state of circulatory hyperdynamia that is due to the formation of portosystemic shunts secondary to portal hypertension.11 Portal hypertension may also be responsible for hyperplasia of the reticuloendothelial system and chronic venous congestion leading to splenomegaly and its complications, notably hypersplenism.12 On the other hand, hypersplenism can induce an increase in splenic vein blood flow leading to an increase in portal blood flow and thus, can maintain this state of circulatory hyperdynamia.13,14 We suggested that hypersplenism was one of the factors in persistent portal hypertension even after eradication of esophageal varices. Thus, splenectomy might be justified in the management of noncirrhotic portal hypertension by correcting hypersplenism and thereby decreasing portal blood flow.3,14,15 In contrast to cirrhosis, there is still no consensus regarding the prevention of hemorrhagic recurrence in patients with HSS because of the lack of sufficient literature data. However, studies have suggested a combination of surgical (splenectomy) and endoscopic methods to prevent recurrent bleeding.9,16–18
In this study, the rate of hemorrhagic recurrence in the splenectomy + EVL group was significantly lower than in the EVL alone group (4.54% vs 27%, p = 0.041). These results differed from those of Jiang et al who found no significant difference in the rate of hemorrhagic recurrence between the two groups at 5 years (44.2% vs 52.3%, p = 0.449).16 On the other hand, a Brazilian phase III randomized clinical trial comparing 25 patients with endoscopic treatment alone and 22 patients with combined splenectomy and endoscopic treatment found a significantly lower rate of variceal bleeding recurrence in patients treated with combined splenectomy and endoscopic treatment compared to those treated with endoscopic treatment alone (9.1% vs 36.2%, p = 0.029).9
In our study, EVL was used as an endoscopic method to eradicate esophageal varices. According to the study by Siqueira et al, there was no difference between sclerotherapy and EVL in terms of efficacy for the management of esophageal varices on HSS.19 However, sclerotherapy is currently no longer recommended for the management of esophageal varices regardless of their cause.10 In our study, esophagogastric devascularization was not performed because of the complexity of this procedure, which may prolong the operative time during splenectomy. In the literature, various studies have shown a significant reduction in the intravascular pressure of esophageal varices in patients managed by splenectomy associated with esophagogastric devascularization.7,20,21 The combination of splenectomy and esophagogastric devascularization could also result in a significant decrease in the frequency of risk factors for recurrent bleeding, including the size of the varices, the presence of red signs, and the presence of portal hypertensive gastropathy.7 However, the eradication rate of esophageal varices related to the association of splenectomy and esophagogastric devascularization is 18.2% but this could increase up to 86%, when it is coupled with an endoscopic method.22,23 In this case, it could prevent hemorrhagic recurrence in 82.5% of cases over a period of 20 years after surgery.8
In terms of mortality, this study showed no significant difference between the two groups (4.54% vs 2.7%; p = 1.00). Two groups are probably not similar in terms of severity of portal hypertension. This is illustrated by the fact that the splenectomy group had a significantly higher number of prior bleeding episodes (3.25 versus 2.24, p < 0.001). This could explain the lack of survival benefit. These results were different from those reported in the Chinese study which found a significant difference between the two groups with a lower 5-year mortality rate in the EVL + splenectomy group (17.3% vs 46.8%; p = 0.037).16 Lacet et al reported a mortality rate of 4% in patients managed by endoscopy alone.9 A Brazilian study found a mortality rate of 4.5% after 20 years of evolution after the combined method (surgical and endoscopic).8 An African study reported that the one-year survival rate in patients treated with EVL + splenectomy was 97.3%.17
Limitations of the Study
The major limitation of the study was that the allocation to each group was at the discretion of the treating physician and the two groups are probably not similar in terms of severity of portal hypertension. This is illustrated by the fact that the splenectomy group had a significantly higher number of prior bleeding episodes (3.25 versus 2.24, p < 0.001). This could explain the lack of survival benefit and may have underestimated the differences in rebleeding rates between the two groups. The retrospective and monocentric nature of the study constituted additional limitations of the study inducing a bias in our research. Other associated factors that could influence prognosis were not studied and long-term follow-up could not be performed. The presence of selection bias remains possible in patients who underwent splenectomy + EVL.
Conclusion
EVL associated with splenectomy is more effective than EVL alone in reducing the risk of recurrence of variceal bleeding in patients with HSS. Because of the lack of current recommendations or consensus on the management of HSS, splenectomy combined with EVL may be a feasible method to prevent recurrence of variceal bleeding. However, our study is inconclusive in predicting the risk of mortality associated with each method. Thus, a new prospective, multicenter, long-term study is needed to indicate this therapeutic method for the prevention of morbidity and mortality related to complications of HSS.
Data Sharing Statement
Data supporting the conclusions of this study are available from the corresponding author on reasonable request.
Ethical Considerations
This study was ethically and scientifically approved by ethic committee of University Hospital Joseph Raseta Befelatanana, with a waiver for informed consent as all patients were de-identified. All study procedures were conducted in accordance with the Declaration of Helsinki. All authors had access to the study data and reviewed and approved the final manuscript before submission.
Acknowledgments
The authors would like to thank the members of the Gastroenterology Unit of the Joseph Raseta Befelatanana University Hospital, Visceral Surgery Unit, UH Joseph Ravoahangy Andrianavalona, Antananarivo, and Visceral Surgery Unit, UH Tambohobe, Fianarantsoa, Madagascar.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest in relation to this work.
References
1. OMS. Relevé épidémiologique hebdomadaire; 2019:601–612.
2. Roux J, Ravaoalimalala VA, Rakoto L, et al. Bases de réflexions et grandes lignes du Programme national de lutte contre les bilharzioses à Madagascar. Arch Inst Pasteur de Madagascar. 1994;61(1):
3. Leite LAC, Pimenta Filho AA, Ferreira RD, et al. Splenectomy improves hemostatic and liver functions in hepatosplenic schistosomiasis mansoni. PLoS One. 2015;10(8):e0135370. doi:10.1371/journal.pone.0135370
4. Lin N, Liu B, Xu RY, Fang HP, Deng MH. Splenectomy with endoscopic variceal ligation is superior splenectomy with pericardial devascularization in treatment of portal hypertension. World J Gastroenterol. 2006;12(45):7375–7379. doi:10.3748/wjg.v12.i45.7375
5. Ede CJ, Nikolova D, Brand M. Surgical portosystemic shunts versus devascularisation procedures for prevention of variceal rebleeding in people with hepatosplenic schistosomiasis. Cochrane Database Syst Rev. 2018;2018(8). doi:10.1002/14651858.CD011717.pub2
6. Colaneri RP, Coelho FF, de Cleva R, Perini MV, Herman P. Splenic artery ligature associated with endoscopic banding for schistosomal portal hypertension. World J Gastroenterol. 2014;20(44):
7. Lacerda CM, Freire W, Vieira de Melo PS, Lacerda HR, Carvalho G. Splenectomy and ligation of the left gastric vein in schistosomiasis mansoni: the effect on esophageal variceal pressure measured by a non-invasive technique. Keio J Med. 2002;51(2):
8. Makdissi FF, Herman P, Pugliese V, et al. Long-term results of esophagogastric devascularization and splenectomy associated with endoscopic treatment in schistosomal portal hypertension. World J Surg. 2010;34(11):
9. Lacet CMC, Neto JB, Ribeiro LT, Oliveira FS, Wyszomirska RF, Strauss E. Schistosomal portal hypertension: randomized trial comparing endoscopic therapy alone or preceded by esophagogastric devascularization and splenectomy. Ann Hepatol. 2016;15(5):
10. de Franchis R. Expanding consensus in portal hypertension: report of the baveno VI consensus workshop: stratifying risk and individualizing care for portal hypertension. J Hepatol. 2015;63(3):
11. Leite LAC, Domingues ALC, Lopes EP, et al. Relationship between splenomegaly and hematologic findings in patients with hepatosplenic schistosomiasis. Rev Bras Hematol Hemoter. 2013;35(5):
12. Lambertucci JR, Lambertucci JR. Revisiting the concept of hepatosplenic schistosomiasis and its challenges using traditional and new tools. Rev Soc Bras Med Trop. 2014;47(2):
13. Cleva R, Saad WA, Herman P, et al. Portal hyperflow in patients with hepatosplenic mansonic schistosomiasis. Rev Hosp Clin. 2004;59(1):
14. de Cleva R, Herman P, D’Albuquerque LAC, Pugliese V, Santarem OL, Saad WA. Pre-and postoperative systemic hemodynamic evaluation in patients subjected to esophagogastric devascularization plus splenectomy and distal splenorenal shunt: a comparative study in schistomomal portal hypertension. World J Gastroenterol. 2007;13(41):
15. Belhamidi MS, Hammi SE, Bouzroud M, Benmoussa M, Ali AA, Bounaim A. Place de la splénectomie dans la prise en charge de l’hypertension portale non cirrhotique: à propos de 3 cas. Pan Afr Med J. 2017;28. doi:10.11604/pamj.2017.28.84.11712
16. Jiang S, Huang X, Ni L, Xia R, Nakayama K, Chen S. Positive consequences of splenectomy for patients with schistosomiasis-induced variceal bleeding. Surg Endosc. 2021;35(5):
17. Al Bashir OM, Abbas AM, Saeed OK. Recurrent variceal bleeding after splenectomy in Sudanese patients with schistosomal periportal fibrosis. Afr J Med Sci. 2016;1(16):
18. Evangelista-Neto J, Pereira FF, França ST, et al. Splenectomy and gastric vein ligature in hepatosplenic schistosomiais: effects upon esophageal variceal pressure and endoscopic risk factors of esophageal variceal bleeding. Arq Bras Cir Dig. 2012;25(1):
19. Siqueira ES, Rohr MR, Libera ED, Castro RR, Ferrari AP. Band ligation or sclerotherapy as endoscopic treatment for oesophageal varices in schistosomotic patients: results of a randomized study. HPB Surg. 1998;11(1):
20. da Silva Neto WDB, Tredicci TM, Coelho FF, Makdissi F, Herman P. Portal pressure decrease after esophagogastric devascularization and splenectomy in schistosomiasis: long-term varices behavior, rebleeding rate, and role of endoscopic treatment. Arq Gastroenterol. 2018;55(2):
21. da Silva-Neto WDB, Quireze-Júnior C, Tredicci TM. Late results of esophagogastric devascularization and splenectomy associated with endoscopic treatment in patients with schistosomiasiS. Arq Bras Cir Dig. 2015;28(3):
22. Ferraz AA, Bacelar TS, Silveira MJ, et al. Surgical treatment of schistosomal portal hypertension. Int Surg. 2001;86(1):
23. Batista-Neto J, Tognetti LB, Ribeiro LT, Balwani M, Muritiba T, Alves EEC. Evolutional profile of the esophageal varices after splenectomy associated with ligation of the left gastric vein and sclerotherapy in schistosomal portal hypertension. Arq Bras Cir Dig. 2013;26(1):
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.