Back to Journals » Local and Regional Anesthesia » Volume 18
Spinal Anesthesia and Postoperative Complications Following Pediatric Hypospadias Repair: A Retrospective Review
Authors Heydinger G ![]() , Kerbage J, Roth C
, Kerbage J, Roth C ![]() , Yeleme Kitio SA, Veneziano G
, Yeleme Kitio SA, Veneziano G ![]() , Tobias JD
, Tobias JD ![]() , Jayanthi VR
, Jayanthi VR
Received 23 July 2025
Accepted for publication 18 October 2025
Published 31 October 2025 Volume 2025:18 Pages 121—129
DOI https://doi.org/10.2147/LRA.S552555
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Stefan Wirz
Grant Heydinger,1,2 Josiane Kerbage,1 Catherine Roth,1 Sibelle Aurelie Yeleme Kitio,1 Giorgio Veneziano,1,2 Joseph D Tobias,1,2 V Rama Jayanthi3
1Department of Anesthesiology & Pain Medicine, Nationwide Children’s Hospital, Columbus, OH, USA; 2Department of Anesthesiology, The Ohio State University Wexner Medical Center, Columbus, OH, USA; 3Department of Urology, Nationwide Children’s Hospital, Columbus, OH, USA
Correspondence: Grant Heydinger, Department of Anesthesiology & Pain Medicine, Nationwide Children’s Hospital, 700 Children’s Drive, Columbus, OH, 43205, USA, Email [email protected]
Introduction: Recently, concerns have been raised regarding the impact of anesthetic choice on outcomes for patients undergoing hypospadias repair. It has been suggested that caudal epidural anesthesia (CEA) may be associated with increased postoperative complications, such as urethrocutaneous fistula and glanular dehiscence. However, subsequent studies have found no association between CEA and increased complications. Spinal anesthesia (SA) is another technique that can provide surgical blockade during hypospadias repair. However, no studies have examined outcomes for pediatric patients undergoing hypospadias repair under awake SA.
Methods: We performed a single-center retrospective review on all patients who underwent single-stage primary hypospadias repair from 2016 until 2023. Data collected included patient demographics, anesthetic details, severity of hypospadias, duration of procedure, and postoperative complications.
Results: 805 patients underwent single-stage hypospadias repair during the study period. 117 (14.5%) had GA alone, 563 (70%) had GA with CEA, and 125 (15.5%) had SA. Duration of surgery was significantly longer for patients in the GA and CEA groups compared to the SA group, and more patients in the GA and CEA groups had a higher severity of hypospadias. We did not find significant differences in the odds ratio for postoperative complications between groups.
Discussion: In our retrospective analysis, we did not find a difference between anesthetic groups in the rate of postoperative complications. Patients who had SA were younger and had a shorter median surgical time. Because SA has a limited duration, patients with more complicated pathologies may not be offered SA as an option. SA is an underutilized technique for pediatric urologic procedures, but has several benefits over GA for infants and young children.
Conclusion: SA can be successfully utilized for hypospadias surgery in pediatric patients without an increase in postoperative complications. Future studies on this topic are warranted due to significant baseline differences between patient groups.
Plain Language Summary: There has been debate about whether anesthetic choice during hypospadias surgery may affect the risk of postoperative surgical complications. Spinal anesthesia is a less commonly employed technique that numbs the lower body, allowing this type of surgery to be performed. However, there have been no studies that directly evaluate its association with complications following surgery.
This study compared three anesthetic techniques (general anesthesia, general anesthesia with caudal nerve block, and awake spinal anesthesia) to determine if the incidence of postoperative complications differs between groups. We found that spinal anesthesia likely is not associated with more complications following surgery. It can be utilized safely and effectively as the primary anesthetic for infants and young children undergoing hypospadias repair for both simple and more complex pathologies.
Keywords: pediatric anesthesia, spinal anesthesia, pediatric urology, hypospadias complications
Introduction
Recently, concerns have been raised regarding how anesthetic choice can affect surgical outcomes for pediatric patients undergoing hypospadias repair.1–4 A 2017 retrospective review suggested that caudal epidural anesthesia (CEA) may be associated with a higher incidence of postoperative complications, including urethrocutaneous fistula (UCF) and glanular dehiscence (GD), when compared to general anesthesia (GA) alone. However, subsequent studies have found no association between CEA and increased postsurgical complications.5–9 As this remains a controversial topic, some institutions have looked at other regional options that can provide analgesia for hypospadias repair.
Spinal anesthesia is an option for pediatric patients undergoing various urological procedures including hypospadias repair, and can provide reliable surgical blockade for up to 100 minutes.10–12 Spinal anesthesia has several advantages over general anesthesia in pediatric surgical patients, especially in infants and patients with comorbidities that increase the risk of complications from general anesthesia.13,14 For example, patients with significant airway pathology or cardiopulmonary instability are likely to benefit from an anesthetic technique that mitigates the need for airway manipulation or hemodynamic instability, namely spinal anesthesia. Spinal anesthesia is feasible to perform in both the inpatient and ambulatory settings, and can be used for several common urologic procedures including circumcision, orchiopexy, hernia repair, and hypospadias repair.10,11 Because spinal anesthesia is used less commonly compared to general anesthesia and caudal epidural anesthesia in this patient population, there are few studies that have investigated postoperative outcomes for pediatric patients who underwent urologic surgery using spinal anesthesia. There have been no studies looking specifically at postsurgical complication rates for pediatric patients who have had hypospadias repair under awake spinal anesthesia.
Methods
Patient Population
We intended to identify all patients who had single-stage primary hypospadias repair at Nationwide Children’s Hospital (NCH) from 2016 through May 2023. Our primary aim was to look at anesthetic technique and its potential influence on postoperative surgical complications (ie urethrocutaneous fistula and glanular dehiscence). Ethical approval of the study was obtained from the Institutional Review Board at Nationwide Children’s Hospital (STUDY00003482). The study was conducted in accordance with the ethical standards of the Declaration of Helsinki. Individual patient informed consent was waived due to the retrospective nature of this study. All data was handled in strict compliance with NCH’s institutional and ethical guidelines. Patient information was de-identified prior to data analysis, and confidentiality was strictly maintained to ensure patient privacy. Patients were identified from the operating room (OR) schedule and electronic medical record using the search term “hypospadias repair”. Exclusion criteria included multi-stage repairs, revision operations, and patients who received combined spinal and caudal epidural anesthesia. As this was a retrospective review, patients were not randomized to anesthetic choice, which was left to the discretion of the attending anesthesiologist in discussion with the surgical team. Anesthetic choice (ie general vs spinal) is generally influenced by patient age, comorbidities, and expected duration or complexity of surgery. All patients meeting inclusion criteria during the study period were reviewed, regardless of anesthetic technique to minimize selection bias.
Patient Groups
We separated our cohort of 805 patients into three patient groups: GA, CEA, and SA. Patients in the GA group underwent inhalation or intravenous induction and were maintained under anesthesia with sevoflurane. Nearly all patients in this group also had penile blockade performed by the Urologist for postoperative analgesia at the conclusion of the case. Patients in the CEA group also underwent general anesthesia, followed by single-shot caudal epidural blockade by the Anesthesiologist prior to surgical incision. Patients in the SA group had single-shot spinal blockade performed, and underwent hypospadias repair without general anesthesia. Most patients in the SA group also had penile blockade performed following surgery.
Surgical and Anesthetic Considerations
It is our institution’s practice to perform single-shot SA using 0.5% isobaric bupivacaine with 1:200,000 epinephrine and 1 µg/kg adjunctive clonidine. A 22-gauge, 1.5-inch Quincke spinal needle is used to access the lumbar intrathecal space, and the medication is injected following free flow of cerebrospinal fluid. Subsequently, intravenous access is obtained ideally in the lower extremity and the surgical procedure begins. We have found that this reliably provides at least 90–100 minutes of surgical blockade. Patients that do not require additional sedation can bypass Phase I of the PACU and go immediately to their parents/caregivers from the operating room to recover prior to discharge.
For patients that have general anesthesia, patients will typically undergo inhalational induction with sevoflurane followed by IV access and placement of a laryngeal mask airway. Intraoperative analgesic strategy varies by attending anesthesiologist preference. Nearly all patients in both groups had a penile block performed at the end of the surgical procedure for postoperative analgesia. Caudal blockade is performed following induction of GA, and most patients receive 1mL/kg of 0.2% ropivacaine or 0.25% bupivacaine with 1:200,000 epinephrine and 1 µg/kg of clonidine.
Clinical Data
Demographic and clinical data that was collected included patient age; height and weight; ethnicity; American Society of Anesthesiologists (ASA) Physical Status Classification; anesthetic technique (spinal, general, or caudal epidural anesthesia); position of the urethral meatus defined as distal (glanular, coronal, or distal shaft) or proximal (mid-shaft, proximal shaft, penoscrotal); and years of experience of the Pediatric Urologist (based on the year of completion of Pediatric Urology fellowship). The primary outcome of this study was whether or not patients developed urethrocutaneous fistula or glanular dehiscence following initial hypospadias repair surgery.
Statistical Analysis
Continuous variables were summarized using median and interquartile ranges (IQR) due to their skewed nature, and group differences were assessed using a Wilcoxon sum rank test. Categorical variables were presented as counts and percentages, and statistical tests such as chi-square or Fisher’s exact test were employed as appropriate. The threshold for determining statistical significance was set at a p-value of less than 0.05. Subsequently, univariate logistic regression analysis was performed to evaluate if there was a statistically significant association between having a postoperative complication and anesthetic choice.
Results
Patient Characteristics
We were able to identify 805 patients who had hypospadias repair surgery under general (GA), spinal (SA), or general and caudal epidural anesthesia (CEA) from January 2016 until May 2023 at NCH. One hundred seventeen patients (14.5%) received GA, 125 patients (15.5%) received SA, and 563 (70%) received GA with CEA. Within the GA group, the median age was 11 months (IQR 8, 36), and median weight was 10.2 kg (9.0, 13.8). Within the SA group, the median age was 7 months (6, 9), and median weight was 8.4 kg (7.6, 9.2). Within the CEA group, median age was 8 months (7, 11), and median weight was 9 kg (8.0, 10.1). Nearly all patients (98%) were ASA I or II (Table 1).
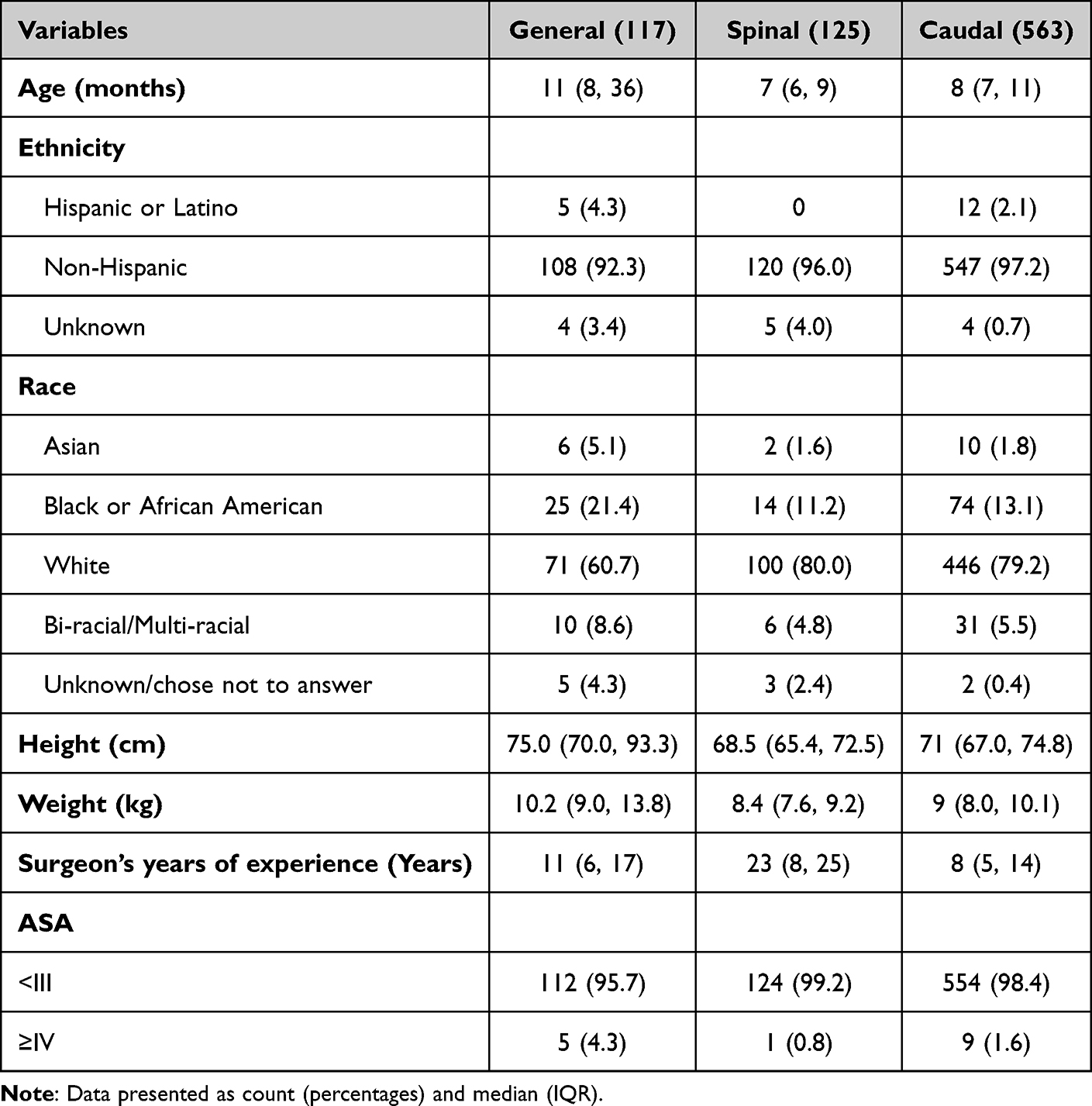 |
Table 1 Patient Characteristics (N=805) |
Surgical Characteristics
Most patients (88%) had surgery to repair more distal presentation of hypospadias (including glanular, coronal, or distal shaft), and 12% of patients had more severe or proximal hypospadias (including mid-shaft, proximal shaft, or penoscrotal). The median surgical time was 101 minutes (IQR 77, 122) for the GA group, 105 minutes for the CEA group (85, 122), and 63 minutes (52, 79) for the SA group. Median total anesthesia time was also significantly shorter for patients who had SA, compared to those who had GA (Table 2).
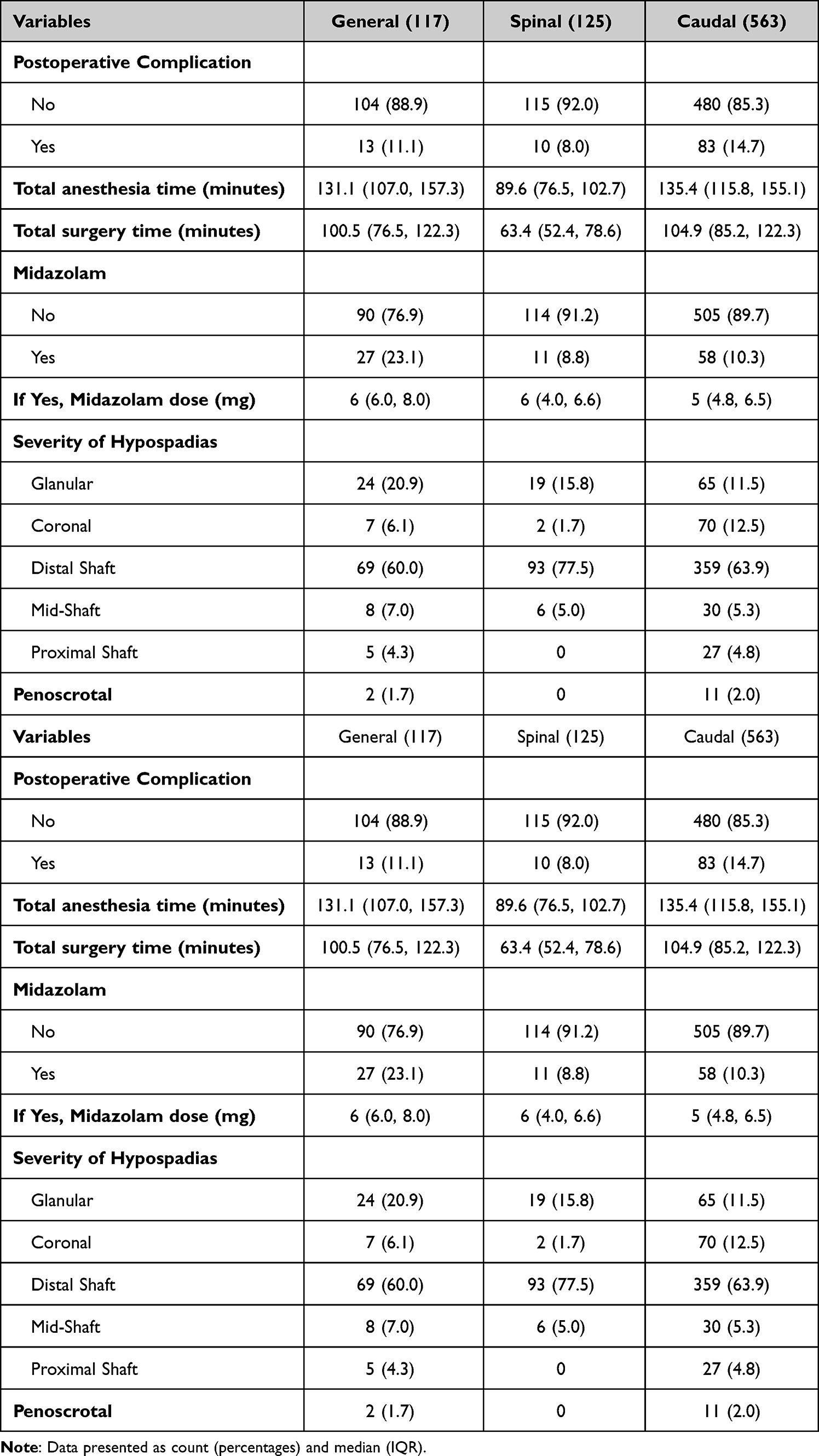 |
Table 2 Anesthesia and Surgical Characteristics (N=805) |
Postoperative Complications
Thirteen patients (11.1%) in the GA group had a postoperative complication in the form of UCF or GD. Ten patients (8.0%) in the SA group had postoperative complications, and 83 patients (14.7%) in the CEA group had postoperative complications (Table 3). Using GA as the reference group, we did not find a statistically significant difference in rate of postoperative complications compared to SA (OR 0.7 [95% CI 0.29–1.65]) or CEA (OR 1.38 [95% CI 0.74–2.58]). We were able to identify some variables other than anesthetic choice that had a statistical effect on incidence of postoperative complications. There was a small association with increased complications in patients who had a longer duration of surgical time (OR 1.02 [95% CI 1.01–1.02]) and had a more severe form of hypospadias; compared to patients with a diagnosis of glanular hypospadias, patients with mid-shaft (OR 3.90 [95% CI 1.32–11.54]), proximal shaft (4.43 [1.39–14.07]), and penoscrotal hypospadias (15.82 [3.64–68.69]) were all more likely to experience UCF or GD following surgery. More years of surgical experience was also associated with fewer postoperative complications (OR 0.95 [95% CI 0.92–0.99]). Seven hundred fifty-five patients (94%) had at least one initial follow-up Urology appointment following surgery. Five hundred sixty patients (70%) were seen at Urology clinic at some point more than two weeks following their hypospadias repair surgery.
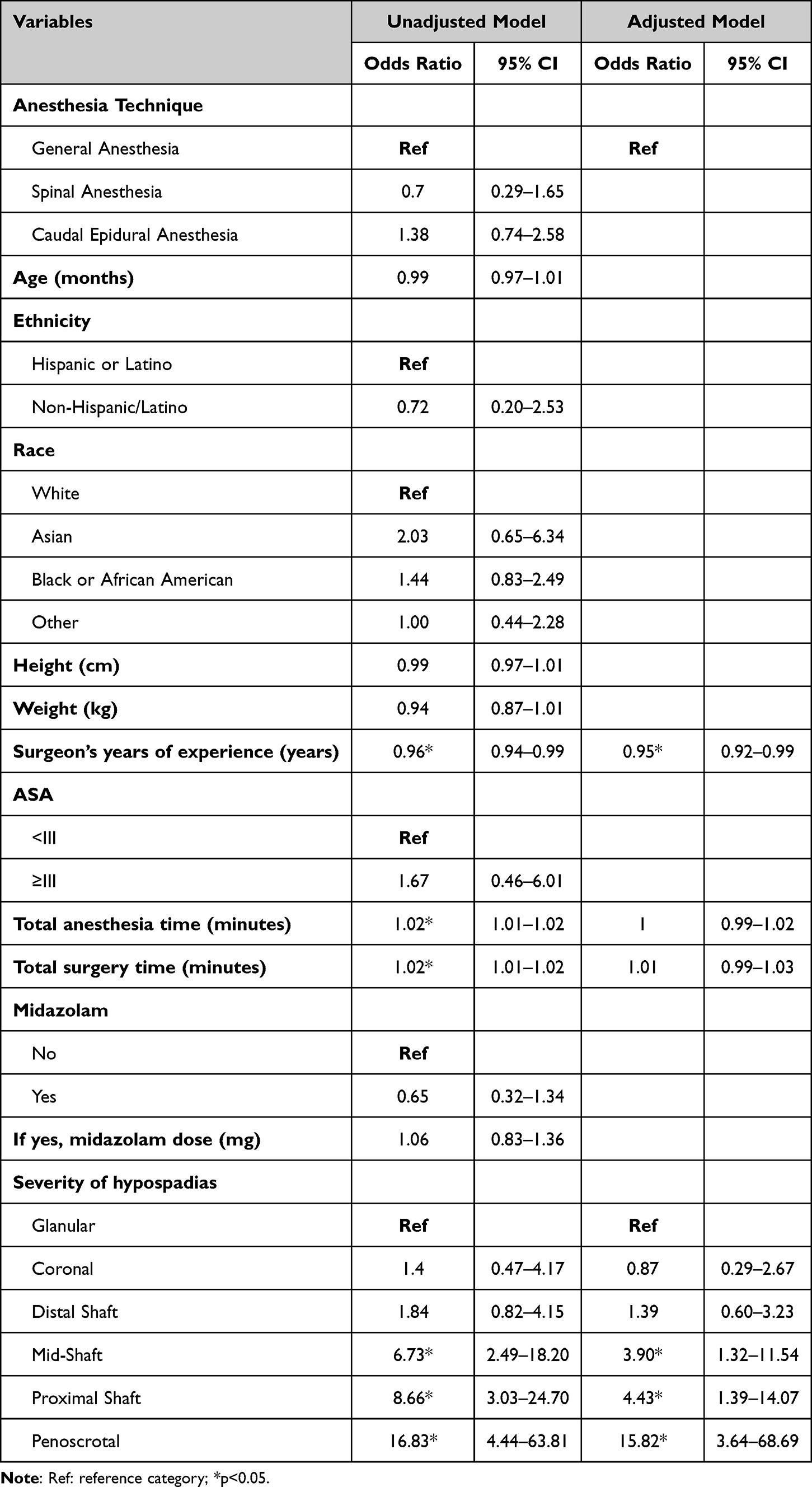 |
Table 3 Odds Ratio for Postoperative Complications in Children Undergoing Hypospadias Surgery |
Discussion
We performed a retrospective review of patients who had single-stage primary hypospadias repair under spinal anesthesia or general anesthesia from January 2016 through May 2023. Although there are some clinically relevant demographic differences between groups, our data does not indicate an association between anesthetic choice and incidence of postoperative complications (ie urethrocutaneous fistula and glanular dehiscence).
In recent years, the question of whether anesthetic choice can affect postoperative outcomes following hypospadias repair in children has been heavily disputed in the literature.15,16 Multiple studies have shown association,1–4 and others have indicated no effect.5–9 Most studies addressing this subject have been retrospective in nature and subject to different interpretations due to confounding factors, selection bias, and small sample size. While Taicher et al reported a greater than 13-fold increase in postoperative complications associated with CEA, even adjusting for hypospadias severity,1 no other studies have since been able to repeat such impressive results. Even among systemic review and meta-analyses, there have been conflicting outcomes.17,18 There has even been a study published indicating that CEA is associated with lower rates of complications compared to penile block.19 Interestingly, spinal anesthesia has not been considered as a focus of such studies. This is the first investigation which primarily compares GA to CEA and SA in regard to influence on postoperative hypospadias repair complications. SA is not widely performed in pediatric centers due to relative unfamiliarity and low acceptance rates among pediatric urologists.20 We believe that SA remains an underutilized technique for pediatric urologic surgeries, despite its excellent safety profile21 and number of advantages over GA in this population.10–12 SA has also been shown to decrease OR time and improve hospital cost and resource utilization.22,23
It is generally thought that SA does not provide postoperative analgesia long after resolution of blockade. Randomized, prospective studies have found that postoperative pain control is in fact more favorable in patients that receive CEA compared to SA.24,25 However, we utilize intrathecal clonidine in our preparation, which is thought to extend the duration of blockade and may have additional analgesic effect after resolution of sensory blockade. Intrathecal opioids (2 mcg/kg of morphine) have also been shown to improve postoperative pain control compared to placebo for patients who receive SA for hypospadias repair.26
Regarding the use of premedication, 23% of patients in the GA group received oral midazolam before surgery, compared to 10% of patients in the CEA group and 9% of patients in the SA group. At our institution, we find that preoperative midazolam is not necessary to help facilitate the performance of SA in awake infants. With adequate perioperative preparation (eg adequate patient positioning, topicalization at needle site, and calm operating room conditions), we have found that premedication does not add to the success rate or effectiveness of SA in most cases.
The current study has several limitations. Most importantly, there are clinically relevant differences between groups in terms of baseline demographics and surgical characteristics. It is not surprising that patients who receive SA are younger and smaller on average and have shorter surgical times. As patients approach one year of age or older, some anesthesiologists may feel less comfortable performing SA, and patients with more complicated pathology may not be ideal candidates for SA, as the operating time may outlast the duration of surgical blockade. This is an issue that is not as evident in the studies that only look at other anesthetic techniques, such as CEA, where patients are under GA as well.
Another limitation to our study is lack of information regarding choice of surgical technique and other complications besides UCF and GD. Information related to specific surgical technique was not consistently available within the retrospective dataset and therefore could not be included in our analysis. While surgical technique can influence complication rates, our primary focus was choice of anesthetic, rather than operative technique. Other complications such as bleeding, hematoma, and mental stenosis were also not included in our final analysis. We made the decision to solely look at rates of postoperative UCF and GD, as these complications had been the primary focus of the previous studies regarding CEA and postoperative outcomes. Another study limitation is that our cohort is rather small, which could bring study power into question. To account for weaknesses in the current study, either a prospective trial or retrospective, multi-institutional investigation is warranted. Utilizing a larger database, such as the Pediatric Hospital Information System (PHIS) would be helpful in providing a more robust sample size for a future study.
Conclusion
In this single-center retrospective study, our data does not indicate an increased risk of postoperative urethrocutaneous fistula formation or granular dehiscence for pediatric patients who undergo single-stage primary hypospadias repair under spinal anesthesia, when compared to general anesthesia. However, additional studies will be necessary to be certain that there is no association.
Abbreviations
ASA, American Society of Anesthesiologists; CEA, caudal epidural anesthesia; CI, confidence interval; GA, general anesthesia; GD, glanular dehiscence; IQR, interquartile range; OR, operating room; PHIS, Pediatric Hospital Information System; SA, spinal anesthesia; UCF, urethrocutaneous fistula.
Ethical Statement
Ethical approval of the study was obtained from the Institutional Review Board at Nationwide Children’s Hospital. This study involved a retrospective review of medical records and posed no greater than minimal risk.
Disclosure
The authors declare no conflicts of interest.
References
1. Taicher BM, Routh JC, Eck JB, Ross SS, Wiener JS, Ross AK. The association between caudal anesthesia and increased risk of postoperative surgical complications in boys undergoing hypospadias repair. Paediatr Anaesth. 2017;27(7):688–694. doi:10.1111/pan.13119
2. Kundra P, Yuvaraj K, Agrawal K, Krishnappa S, Kumar LT. Surgical outcome in children undergoing hypospadias repair under caudal epidural vs penile block. Paediatr Anaesth. 2012;22(7):707–712. doi:10.1111/j.1460-9592.2011.03702.x
3. Kim MH, Im YJ, Kil HK, Han SW, Joe YE, Lee JH. Impact of caudal block on postoperative complications in children undergoing tubularised incised plate urethroplasty for hypospadias repair: a retrospective cohort study. Anaesthesia. 2016;71(7):773–778. doi:10.1111/anae.13463
4. Saavedra-Belaunde JA, Soto-Aviles O, Jorge J, Escudero K, Vazquez-Cruz M, Perez-Brayfield M. Can regional anesthesia have an effect on surgical outcomes in patients undergoing distal hypospadias surgery? J Pediatr Urol. 2017;13(1):
5. Fischer KM, Van Batavia J, Hyacinthe N, et al. Caudal anesthesia is not associated with post-operative complications following distal hypospadias repair. J Pediatr Urol. 2023;19(4):374–379. doi:10.1016/j.jpurol.2023.03.019
6. Adler AC, Bhatia VP, Chandrakantan A, Nathanson BH, Ouellette L, Austin PF. Association of analgesic block with the incidence of complications following hypospadias surgery; a meta-analysis. Urology. 2022;166:11–17. doi:10.1016/j.urology.2022.03.002
7. Splinter WM, Kim J, Kim AM, Harrison MA. Effect of anesthesia for hypospadias repair on perioperative complications. Pediatr Anesth. 2019;29(7):760–767. doi:10.1111/pan.13657
8. Zaidi RH, Casanova NF, Haydar B, Voepel-Lewis T, Wan JH. Urethrocutaneous fistula following hypospadias repair: regional anesthesia and other factors. Pediatr Anesth. 2015;25(11):1144–1150. doi:10.1111/pan.12719
9. Alizadeh F, Amraei M, Haghdani S, Honarmand A. The effect of caudal epidural block on the surgical complications of hypospadias repair in children aged 6 to 35 months: a randomized controlled trial. J Pediatr Urol. 2022;18(1):
10. Whitaker EE, Wiemann BZ, DaJusta DG, et al. Spinal anesthesia for pediatric urological surgery: reducing the theoretic neurotoxic effects of general anesthesia. J Pediatr Urol. 2017;13(4):396–400. doi:10.1016/j.jpurol.2017.06.006
11. Heydinger G, Kim SS, Beltran RJ, et al. Ambulatory spinal anesthesia in infants ≤ six months of age: a retrospective review of outcomes and safety. J Clin Anesth. 2022;81:110920. doi:10.1016/j.jclinane.2022.110920
12. Jayanthi VR, Spisak K, Smith AE, et al. Combined spinal/caudal catheter anesthesia: extending the boundaries of regional anesthesia for complex pediatric urological surgery. J Pediatr Urol. 2019;15(5):442–447. doi:10.1016/j.jpurol.2019.04.004
13. Abajian JC, Mellish RW, Browne AF, Perkins FM, Lambert DH, Mazuzan JE. Spinal anesthesia for surgery in the high-risk infant. Anesth Analg. 1984;63:359–362. doi:10.1213/00000539-198403000-00015
14. Sartorelli KH, Abajian JC, Kreutz JM, Vane DW. Improved outcome utilizing spinal anesthesia in high-risk infants. J Pediatr Surg. 1992;27:1022–1025. doi:10.1016/0022-3468(92)90550-Q
15. Braga LH, McGrath M, Farrokhyar F. Dorsal penile block versus caudal epidural anesthesia effect on complications post-hypospadias repair: dilemmas, damned dilemmas and statistics. J Pediatr Urol. 2020;16(5):708–711. doi:10.1016/j.jpurol.2020.08.009
16. Ayob F, Arnold R. Do caudal blocks cause complications following hypospadias surgery in children? Anaesthesia. 2016l;71(7):759–763. doi:10.1111/anae.13490
17. Tanseco PP, Randhawa H, Chua ME, et al. Postoperative complications of hypospadias repair in patients receiving caudal block vs. non-caudal anesthesia: a meta-analysis. Can Urol Assoc J. 2019;13(8):E249–57. doi:10.5489/cuaj.5688
18. Goel P, Jain S, Bajpai M, Khanna P, Jain V, Yadav DK. Does caudal analgesia increase the rates of urethrocutaneous fistula formation after hypospadias repair? Systematic review and meta-analysis. Indian J Urol. 2019;35(3):222–229. doi:10.4103/iju.IJU_252_18
19. Ngoo A, Borzi P, McBride CA, Patel B. Penile nerve block predicts higher revision surgery rate following distal hypospadias repair when compared with caudal epidural block: a consecutive cohort study. J Pediatr Urol. 2020;16(4):
20. Rehfuss A, Bogaert G, Kogan BA. Spinal anesthesia in children: most pediatric urologists are not on board. J Pediatr Urol. 2019;15(5):582. doi:10.1016/j.jpurol.2019.07.007
21. Williams RK, Adams DC, Aladjem EV, et al. The safety and efficacy of spinal anesthesia for surgery in infants: the vermont infant spinal registry. Anesth Analg. 2006;102(1):67–71. doi:10.1213/01.ANE.0000159162.86033.21
22. Ing C, Sun LS, Friend AF, et al. Adverse events and resource utilization after spinal and general anesthesia in infants undergoing pyloromyotomy. Reg Anesth Pain Med. 2016;41:532e7. doi:10.1097/AAP.0000000000000421
23. Kokki H. Spinal blocks. Pediatr Anesth. 2012;22:56–64. doi:10.1111/j.1460-9592.2011.03693.x
24. Bozkurt C, Erturk E, Akdogan A, Kesicioglu T, Aydin I. Comparison of spinal versus caudal epidural anesthesia in the management of patients undergoing ambulatory perianal surgery: randomized, prospective study. J Clin Med Kaz. 2021;18(5):76–81. doi:10.23950/jcmk/11240
25. Al-Kershawy A, Noor El-Din T, Abd-Elsalam M, Ismail H. Spinal versus caudal anesthesia in lower abdominal surgeries in pediatrics. Int J Med Arts. 2020;2(4):705–711.
26. Apiliogullari S, Duman A, Gok F, Akillioglu I, Ciftci I. Efficacy of a low-dose spinal morphine with bupivacaine for postoperative analgesia in children undergoing hypospadias repair. Paediatr Anaesth. 2009;19(11):1078–1083. doi:10.1111/j.1460-9592.2009.03136.x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.