Back to Journals » Psychology Research and Behavior Management » Volume 12
Spanish Validation Of The Revised Depression Attitude Questionnaire (R-DAQ)
Authors Cherrez-Ojeda I ![]() , Haddad M
, Haddad M ![]() , Vera Paz C
, Vera Paz C ![]() , Valdevila Figueira JA
, Valdevila Figueira JA ![]() , Fabelo Roche J, Orellana Román C
, Fabelo Roche J, Orellana Román C ![]() , Iglesias Moré S, Felix M
, Iglesias Moré S, Felix M ![]() , Vanegas E
, Vanegas E ![]() , Alvarado-Villa GE
, Alvarado-Villa GE ![]()
Received 22 August 2019
Accepted for publication 25 October 2019
Published 13 November 2019 Volume 2019:12 Pages 1051—1058
DOI https://doi.org/10.2147/PRBM.S228249
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Ivan Cherrez-Ojeda,1,2 Mark Haddad,3 Carlos Vera Paz,1,2 Jose Alejandro Valdevila Figueira,4 Justo Fabelo Roche,5 Carlos Orellana Román,4 Serguei Iglesias Moré,5 Miguel Felix,1,2 Emanuel Vanegas,1,2 Geovanny Efraín Alvarado-Villa1
1Universidad Espíritu Santo, Samborondón, Ecuador; 2Respiralab Research Group, Guayaquil, Ecuador; 3Centre for Mental Health Research, School of Health Sciences, City University London, London, UK; 4Instituto de Neurociencias, Guayaquil, Ecuador; 5Universidad de Ciencias Médicas de la Habana, Habana, Cuba
Correspondence: Ivan Cherrez-Ojeda
Universidad Espíritu Santo, Km. 2.5 Vía La Puntilla, Samborondón 0901-952, Ecuador
Tel +5934511455
Email [email protected]
Purpose: The aim of the study was to develop and validate a Spanish version of the Revised Depression Attitude Questionnaire (R-DAQ).
Methods: The R-DAQ was used as a baseline for the study. It was translated and tested to ensure the instrument was appropriate for the target population. 537 Ecuadorian healthcare professionals completed the revised Spanish version of the R-DAQ (SR-DAQ). Statistical and exploratory factor analyses were performed to examine construct validity, internal consistency, readability and floor and ceiling effects.
Results: Three factors were obtained: “Professional confidence in depression care”; “Therapeutic optimism about depression”; and “Generalist perspective about depression occurrence, recognition, and management”. The internal consistency of the SR-DAQ was determined by means of Cronbach’s α coefficient, with values ranging between 0.61–0.8. The correlations with the English version reflected adequate validity. The model explained 39% of the variance. Subsequent analysis with a sample restricted to those who had received training in depression produced a model that explained 42% of the variance.
Conclusion: The SR-DAQ meets the psychometric requirements for measuring depression attitude in a Spanish-speaking population and shows adequate internal consistency and validity.
Keywords: attitudes, depression, Latin America, psychometric properties, validation
Introduction
A recent study on the global burden of diseases estimated that approximately 15% of the disability-adjusted life years were caused by mental and substance abuse disorders, with depression being the second leading cause of global disability worldwide.1 Depression is a common disease, affecting more than 300 million people globally, and it is regarded as the second leading cause of death in individuals aged 15 to 29 years.2 Furthermore, the prevalence of depression in diseases such as cancer, type 2 diabetes, and asthma is reported to be higher compared to the general population, influencing the course and prognosis of the disease, as well as having a negative impact on the quality of life from those who suffer from it.3
Although evidence-based mental health interventions have been found to be effective in places with limited resources, there is a documented “mental health treatment gap” where globally, more than two thirds of patients with mental disorders lack access to appropriate care.4–6 Various findings have been identified as possible contributors to this gap, including the stigmatization associated with mental diseases, the lack of implementation of mental health programs in health systems, and the inadequate training of healthcare professionals managing these patients.7 In addition, physicians’ perspectives on mental illness may incorporate part of the stereotypes and misunderstandings of society, highlighting the importance of measuring their attitudes to specific conditions such as depression.8
In this regard, a useful tool for assessing healthcare professionals’ attitudes to depression is the Revised Depression Attitude Questionnaire (R-DAQ). This instrument is a revised version developed to address methodological weaknesses of the original Depression Attitude Questionnaire (DAQ), by incorporating views of different healthcare professionals in a large sample size.8,9 The R-DAQ provides a tool for examining the understandings and views on depression by means of a 22 item-questionnaire that incorporates three dimensions: i) professional confidence, ii) therapeutic optimism, and iii) views about generalist or specialist perspectives on depression and its care.8 It has demonstrated face, content, and construct validity, as well as adequate internal consistency and test-retest reliability.8
To the best of our knowledge, there are no studies that validate the use of the R-DAQ in Spanish speaking healthcare professionals. Furthermore, in Ecuador, it is estimated that more than 90% of the population speaks Spanish as the main language, highlighting the need for adequate translation and validation of clinical instruments. As such, we have designed this study to develop and validate a Spanish version of the R-DAQ. The result is tool than can provide an objective assessment of healthcare professionals’ attitudes toward depression, information that might be useful to improve future educational approaches, and thus narrow the “mental health treatment gap”.
Methods
Study Design
The R-DAQ was used as a baseline for the study.8 The R-DAQ was used as a baseline for the study.8 The back-translation technique was selected as the method to meet the recommendations by guidelines for cross-cultural validation.10,11 For such purposes, original R-DAQ was translated to Spanish by a certified translator. After that, such Spanish version was back translated into the source language (English) by other independent and blinded translator. After that, both the original and the back-translated English versions of the questionnaire were revised by a committee of specialists to ensure similarity of form and meaning. The translated instrument was experimentally tested with 16 Ecuadorian health professionals to ensure that the wording, terminology, design and time needed to complete the survey was clear, understandable and appropriate for the target population of healthcare professionals.
Furthermore, 537 Ecuadorian healthcare professionals completed the revised questionnaire. Eligibility was restricted to physicians and psychologists from both private and public services with an active medical/clinical practice. The questionnaire was delivered by a previously trained physician who explained the participants the purpose of the study as well as the instructions to fill the survey properly. The participants were recruited from hospitals, outpatient clinics and private doctor’s and psychologist’s offices. Even though a total of 600 questionnaires were delivered, 63 professionals did not want to participate and left the survey in blank, reaching a response rate of 89.5%.
Statistical Analyses
Sampling Adequacy
Statistical analyses were carried out using R Studio and the psych package.12,13 Descriptive statistics were computed, including mean scores, standard deviations, and distribution of the responses for each item. They were later examined for normality, using measures of skewness, Q-Q plots, and kurtosis. In order to proceed with the factor analysis, the sampling adequacy of the responses was analyzed. The Kaiser-Meyer-Olkin (KMO) measure was used to examine each item on the anti-image of the correlation matrix.14 All sampling measures had to be above 0.5 to be considered acceptable.15 Barlett’s test of sphericity was also applied for the overall scale. It consisted of a chi-square test of the null hypothesis of no relationship between the items (with significant results indicating suitability for analysis).16
Construct Validity
Several indicators were taken into account to determine the scale structure and the number of factors. First, eigenvalues were extracted. The kaiser criterion was then applied; this is, the number of factors with eigenvalues >1.17 A scree plot was made out of the eigenvalues collected in order to identify the inflection or elbow in the slope.18 Parallel analysis was performed to test the factors that explain the most variance against a set of random values.19
Exploratory factor analysis (EFA) with principal axis factoring and “Oblimin” rotation with Kaiser normalization was used to determine the dimensionality of the scale.20 A threshold of 0.3 was considered as an acceptable factor loading. Items were removed if they could not reach this threshold or for cross-loading on multiple factors with values equal to or greater than 0.3.21,22 Three items were considered as the minimum required to retain a factor. A parsimonious and straightforward solution was sought, with the intention of preserving interpretability of the factor structure.23
Convergent Validity And Internal Consistency
Convergent validity was evaluated by performing item scale correlations corrected for overlaps; this was done by calculating Pearson’s product-moment correlation coefficient, with a value corrected item-total correlation ≥ 0.2 as acceptable. Cronbach’s alpha was calculated to evaluate internal consistency; it was performed both for the total scale and each of the subscales found in EFA. Cronbach’s alpha measures interrelatedness of items, with values ranging from 0 to 1. Results were regarded as acceptable above the 0.60 threshold.24
Floor And Ceiling Effects
The floor and ceiling effects refer to the proportion of people who have scored at the bottom or top of the possible scores, impairing the responsiveness of the tool as it will not necessarily measure change. Response patterns for each of the factors obtained from exploratory factor analysis were analyzed. Histograms of the distribution of the scores were created and inspected; the percentage of individuals with the lowest and highest possible score in each of the factors were noted, considering values greater than 20% as floor and ceiling effects.
Readability
Readability was assessed using the Fernandez-Huerta index and the grade level estimate by Crawford.25,26 The first test is a modified Flesch-Kinkaid index for the Spanish language that evaluates readability based on syllables per word and words per sentence. Scores for the former are typically reported from 0–100 (though theoretically there is no lower bound and the upper limit may be around 120). Higher scores indicate greater ease of understanding, and scores of 60–70 represent wording easily understood by 13- to 15-year-old students, whereas scores between 0 and 30 indicate that the text is better suited to graduate-level readers. The Crawford level scale provides the readability level concerning the years of schooling required to read the questionnaire
Ethical Considerations
This study was approved by the ethics committee: Comité de ética e Investigación en Seres Humanos (CEISH), Guayaquil-Ecuador (#HCK-CEISH-18-0060). Informed consent was obtained from every participant before their voluntary participation in the survey.
Results
Sample
A total of 537 respondents completed the survey, all of them from Ecuador. The average age was 42.9 years (SD = 10.9 range 23 to 79). 49.7% were primary care physicians, 6.1% were family medicine specialists, 7.4% psychiatrists and 6.7% were psychologists. 83.1% worked in urban settings. 73.4% of the respondents never received continuing medical education courses in depression (Table 1).
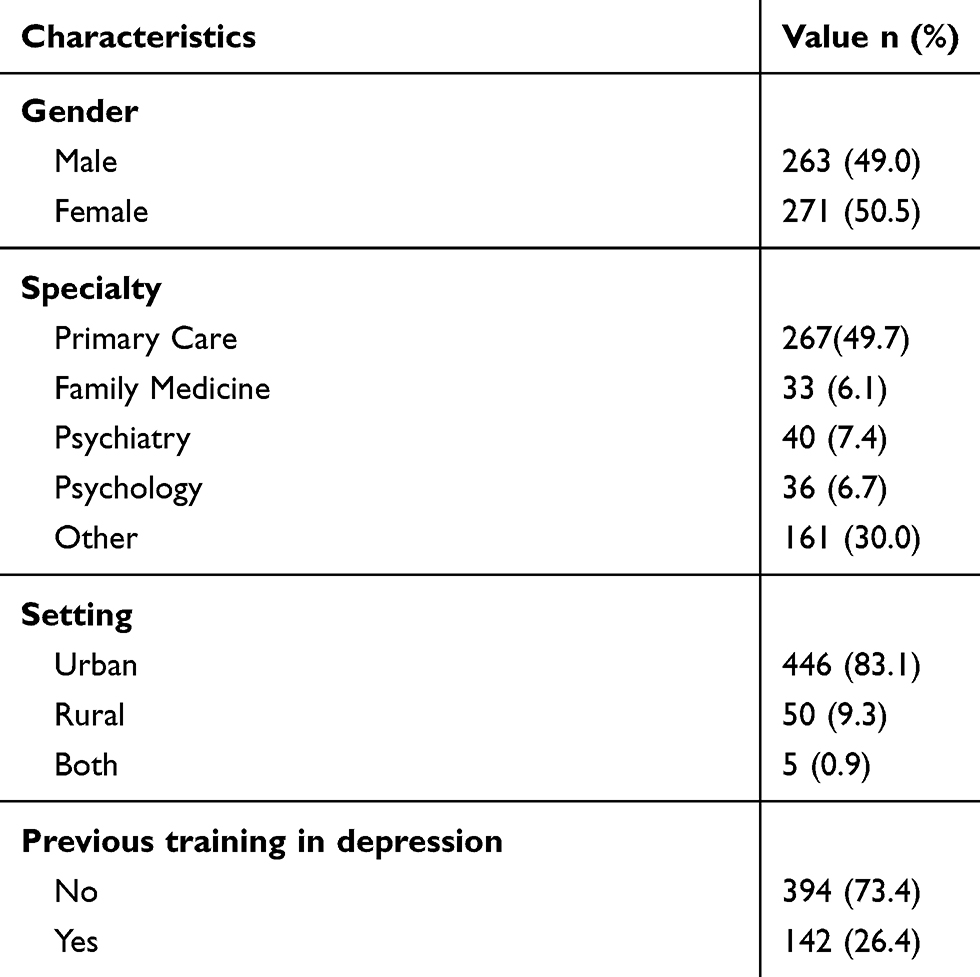 |
Table 1 General Characteristics Of The Surveyed Population (n=537) |
Descriptive
Likert scales are discrete; therefore, the item distribution was expected to be non-normal. Consistent with this, there was mild to moderate skewness (−1.36−0.89) and kurtosis (−1.16−1.55). Individual items had mean values ranging from 4.1 (SD = 0.99) [Item 10] to 2.07 (SD=1.05) [Item 9]. Q-Q plot analysis demonstrated that the data was not normal.
Exploratory Factor Analysis
Before conducting factor analysis, the adequacy of the data was analyzed. The KMO statistic for the overall scale was 0.79, while Barlett’s test was significant (p = < 0.05). Sampling adequacy for all of the 22 items was examined with the anti-image of the correlation matrix. There was no extreme multicollinearity found, as shown in Figure 1. Notably, Item 18 was virtually unrelated to all other items (Table 2 and Figure 3).
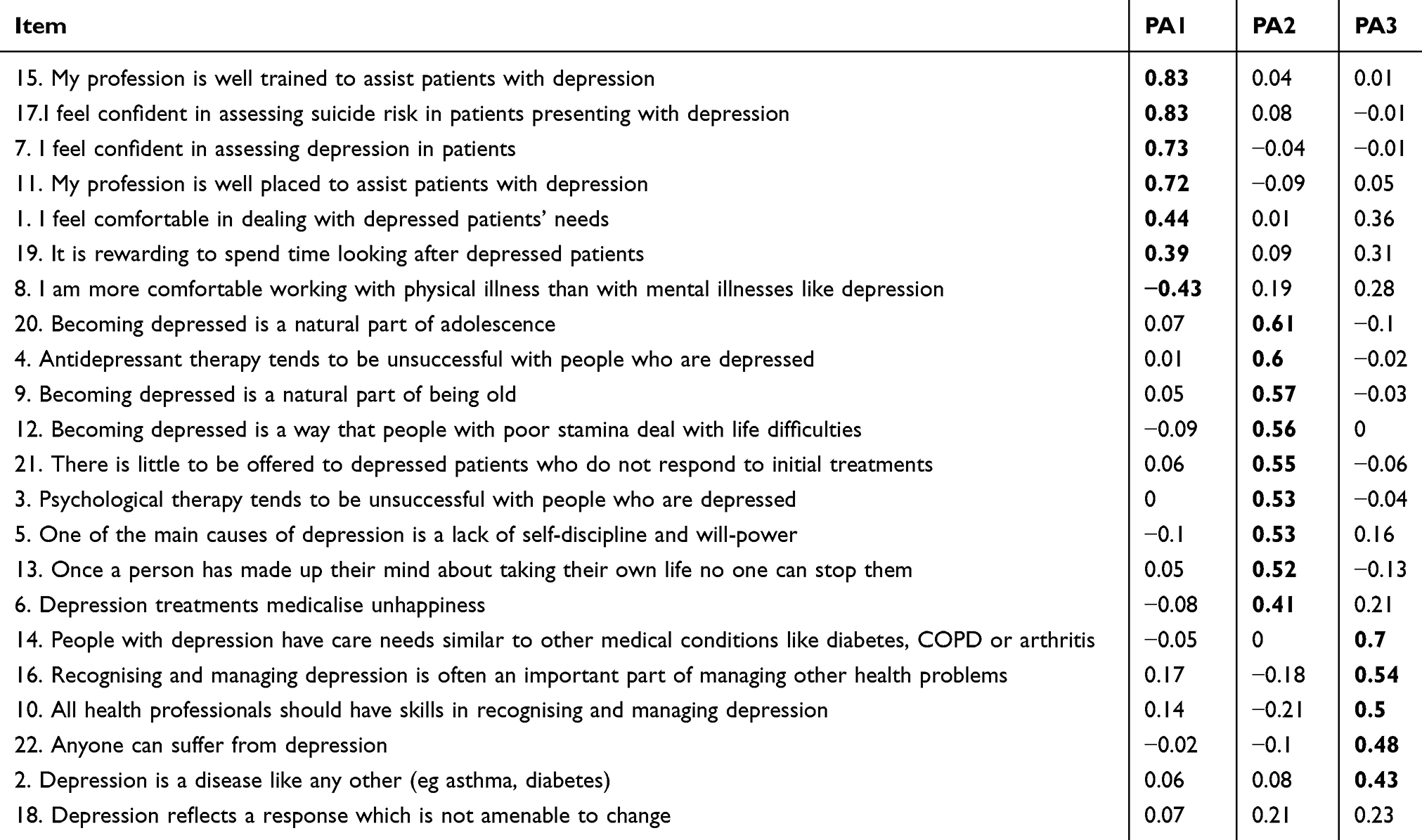 |
Table 2 Factor Analysis Pattern Matrix Of The SR-DAQ |
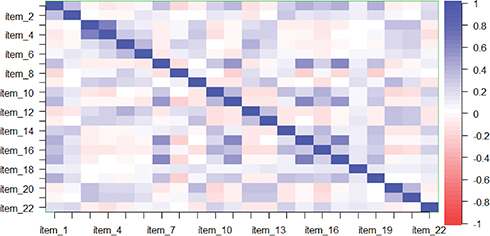 |
Figure 1 Correlation matrix. Item correlations are color graded. Blue indicates positive correlation. |
The selection of the number of factors involved the use of the Kaiser criterion, scree plots and the amount of variance explained by potential models, with emphasis on interpretability. There were six eigenvalues above 1.0 for the 22-item scale, which explained 56% of the variance. The scree plot indicated that a 3 or 4-factor solution would be optimal (Figure 2).
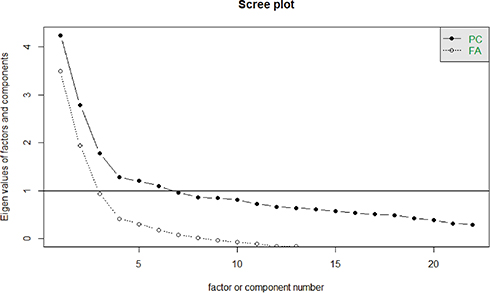 |
Figure 2 Scree Plot. Eigenvalues are plotted to reveal the scree point, where the variance explained by the next factor drops to form an elbow. |
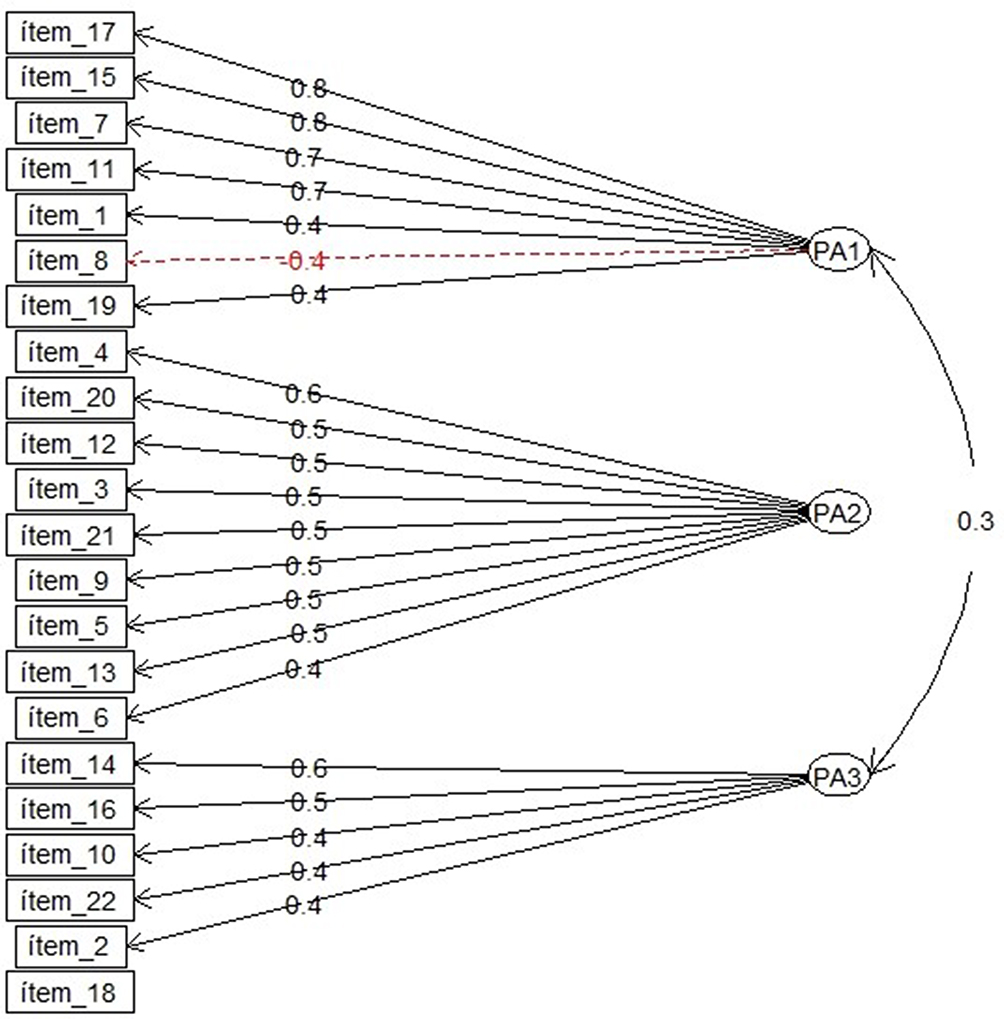 |
Figure 3 Factor analysis diagram. Model diagram shows factor loadings and component structure. Item 18 failed to load on any components. Abbreviation: PA, principal analysis. |
A 4-factor solution was tested, but the fourth factor found only had two items which were insufficient to retain it. A three-factor solution was found to be the most parsimonious and in accordance to the theorized dimensions. The final factor-analytic solution comprised 21 items, with item 18 being dropped because of failure to load on any of the components found. The KMO measure was 0.79 and the model explained 41.6% of the variance.
Internal Consistency And Convergent Validity
For the 21-item scale, Cronbach’s α for internal consistency was 0.78, with item-total correlations corrected for overlap ranging between 0.21 and 0.57 for all items.
The first factor, “Professional confidence in depression care,” was comprised of 7 items regarding the feeling of comfort, confidence and being well trained to provide depression care. The Cronbach’s α was 0.8 for this scale, with item-subscale correlations between 0.32 and 0.76. This factor was responsible for 20.1% of the total variance within the factor structure.
The second factor was named “Therapeutic optimism about depression” and was comprised of 9 reversed scored items. The Cronbach’s α was 0.71 and corrected item-subscale correlations were between 0.34 and 0.6. This factor was responsible for 13.1% of the total scale variance.
The third factor included five items, named “generalist perspective about depression occurrence, recognition, and management.” Cronbach’s α was 0.61 with corrected item-subscale correlations ranging from 0.34 to 0.57. This factor explained 8.4% of the total variance.
Floor And Ceiling Effects
The three factors showed a negative skew, with a tendency for higher response values, showing a positive attitude towards the statements. Further inspection indicated that the effect was more pronounced in the third factor, which had a response mean of 3.9 (SD = 0.16). For the second factor, therapeutic optimism, the mean response was 2.38 (SD = 0.28), while for the first factor “professional confidence in managing depression” the mean score was 3.32 (SD = 0.16). These results indicate that there is room for improvement in this respect, especially in components 1 and 3.
Readability
The readability analysis of the 21-item scale provided a Fernandez-Huerta score of 59.4, and a Crawford Grade level of 6.0, indicating that these items are likely to be understandable to a typical 14–15-year-old individual and require six years of schooling, respectively. These results are somewhat similar to the English version which provided a Flesch Reading Ease score of 46.7, and a Flesch-Kincaid Grade Level of 9.4, indicating that these items are likely to be at the same complexity level.
Discussion
Depression is a widespread issue, encountered by all providers and a correct approach is essential to address it adequately.27 The aim of this study was to develop and validate a Spanish version of the R-DAQ suitable for assessing healthcare professional’s attitude toward depression. The proposed questionnaire contains 21-items, one less than the original R-DAQ questionnaire it is based upon. The decision to drop one question (item 18) was taken from a statistical standpoint. Item 18 had a very low loading on all three factors: 0.14, 0.23, 0.16. Furthermore, when inspecting the correlation matrix there was virtually no correlation between item 18 and the rest of the items in the questionnaire. A possible explanation for this might be attributed to differences in perceptions related to the low frequency of specific depression training. Item 18 defines depression as a response not amenable to change. Such subjective concept may differ between individuals, since as stated by Khatro et al, the faculty of an individual to become depressed or not lies on the magnitude of dysfunctional attitudes they have about their life experiences, which as a matter of fact, do also vary in a case by case scenario.28 As such, it is not surprising that low correlation coefficients (<0.30) were found between this item and the rest of the questionnaire, proving to be a robust indicator to drop the item in question.29
In contrast to the original R-DAQ development, the floor and ceiling effect in our study was less pronounced for factors 2 and 3 (4.09 and 4.29 for factors 2 and 3 in the original R-DAQ, vs 2.38 and 3.32 for factors 2 and 3 in our sample), meaning that our instrument is better suited to detect changes in the population for which it was designed.8 Factor 1 had similar scores compared to the original R-DAQ (3.89, vs 3.63, respectively). The translated version explained 39% of the variance, however, when restricted to those who had training in depression the model explained 42% of the variance in the responses. This observation is comparable to what was achieved with the original English version (45.3%).8 Furthermore, Cronbach’s alpha for the 21-item scale was 0.78, a higher value compared to that reported in another validation study, which yielded a Cronbach’s alpha of 0.638 in a 15-item model.30
Focused interventions can have a more significant impact on improving the quality and outcomes of depression care. Validated instruments, such as the R-DAQ, allows researchers and policymakers to determine the relative need for different interventions and to identify specific points in depression management from the provider’s side that could be improved upon. In this regard, our Spanish version of the Revised Depression Attitude Questionnaire (SR-DAQ) is able to quantify the attitude of health professionals towards depression with a sufficient psychometric profile. Our study provides an initial Spanish validation to be further refined with samples that represent a more comprehensive portion of the healthcare community. Future research should focus on finding a set of questions that are understandable to practitioners across the region as well as exploring refinements in wording that can better capture the theorized construct. The Spanish Revised Depression Attitude Questionnaire (SR-DAQ) is provided as Supplementary Material.
Strengths And Limitations
One of the main strengths of this instrument is the ample knowledge base it is built upon; the R-DAQ is a refined instrument, created from existing work and involving a representative expert panel ensuring a robust theoretical base for the constructs. Participant characteristics and sample size (n=537) ensured that this instrument is appropriate and useful to evaluate healthcare professionals across a spectrum of disciplines and care settings.
However, there are several limitations to our study that need to be discussed. First, the study population was based entirely in one city in Ecuador; therefore, the sample may not be representative of healthcare professionals in other regions or countries, affecting its generalizability. Second, there was a slight decrease in the variance explained, possibly related to cultural differences in perception, which should be addressed with a further revision by Spanish-speaking experts. Finally, it should be noted that we limited our analyses to psychometric parameters but did not take into consideration the clinimetric properties of the instrument. In the clinimetric approach, the clinical validity of the rating scale takes the priority, rather than its statistical significance.31–33 We recommend future studies to evaluate this emerging approach, in order to determine the clinical validity of the R-DAQ.
Conclusion
Mental illnesses, such as depression and anxiety, are heavily influenced by the attitudes experienced by the patient. A negative or unhelpful attitude by the provider can be a strong reinforcement to the issue the patient is presenting with, whereas a positive outlook can help disrupt the negative cognitive bias associated with these conditions, which has been demonstrated to improve outcomes in these diseases.34 Although the perception and acceptance of depression and mental health, in general, has improved over the last decade it is essential to identify which stigmatizing or negative perspectives persist among the healthcare professionals in order to address them in an effective manner.
Our study provides a translated and validated version of the R-DAQ for use in Spanish speaking healthcare professionals. The SR-DAQ consists of 21 items and incorporates three dimensions, including i) professional confidence, ii) therapeutic optimism, and iii) generalist or specialist perspectives related to depression and its care. The extent of the mental health epidemic and its impact on the quality of life and the outcome of other medical conditions provide a strong rationale for a specific instrument for the Spanish language. The translated instrument provides a valid, clear, and interpretable construct, with adequate internal consistency and readability, appropriate to be applied in the healthcare setting.
Abbreviations
R-DAQ, Revised Depression Attitude Questionnaire; KMO, Kaiser-Meyer-Olkin; EFA, Exploratory factor analysis; CEISH, Comité de ética e Investigación en Seres Humanos; SD, Standar deviation; SR-DAQ, Spanish Revised Depression Attitude Questionnaire.
Ethics Approval And Consent To Participate
This study was performed in compliance with the World Medical Association Declaration of Helsinki on Ethical Principles for medical research involving human subjects and was reviewed by the Comité de ética e Investigación en Seres Humanos (CEISH) IRB.
Availability Of Data And Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We want to acknowledge the Inspectoría, Gerencia y Dirección Técnica del Instituto de Neurociencias de Guayaquil for their support. Special thanks to all the colleagues who kindly participated in the application of the scale and who contributed to this research. Finally, we want to express our gratitude to Universidad Espiritu Santo for their continuous support. This work was funded and supported by Universidad Espiritu Santo. The sponsor had no role in the study design, data recollection or statistical analyses.
Author Contributions
All authors made substantial contributions to conception and design, acquisition, analysis and interpretation of data, involved in drafting the manuscript or revising it critically for important intellectual content, gave final approval of the version to be published, and agree to be accountable for all aspects of the work. ICO, MH, CVP, JAVF, JFR, COR, VE, MF participated in the study design process. CVP, SIM performed the statistical analyses and results. CVP, MF drafted the tables and figures. CVP, ICO, GEAV, EV interpreted the analyses, and wrote the manuscript.
Disclosure
The authors declare no conflicts of interest related to this work.
References
1. Mokdad AH, Forouzanfar MH, Daoud F, et al. Global burden of diseases, injuries, and risk factors for young people’s health during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2016;387(10036):2383–2401. doi:10.1016/S0140-6736(16)00648-6
2. Organization WH. Depression; 2018. Available from: https://www.who.int/es/news-room/fact-sheets/detail/depression.
3. Moussavi S, Chatterji S, Verdes E, Tandon A, Patel V, Ustun B. Depression, chronic diseases, and decrements in health: results from the World Health Surveys. Lancet. 2007;370(9590):851–858. doi:10.1016/S0140-6736(07)61415-9
4. Rahman A, Malik A, Sikander S, Roberts C, Creed F. Cognitive behaviour therapy-based intervention by community health workers for mothers with depression and their infants in rural Pakistan: a cluster-randomised controlled trial. Lancet. 2008;372(9642):902–909. doi:10.1016/S0140-6736(08)61400-2
5. Bass JK, Annan J, McIvor Murray S, et al. Controlled trial of psychotherapy for Congolese survivors of sexual violence. N Engl J Med. 2013;368(23):2182–2191. doi:10.1056/NEJMoa1211853
6. Kohn R, Saxena S, Levav I, Saraceno B. The treatment gap in mental health care. Bull World Health Organ. 2004;82:858–866. doi:/S0042-96862004001100011
7. Wainberg ML, Scorza P, Shultz JM, et al. Challenges and opportunities in global mental health: a research-to-practice perspective. Curr Psychiatry Rep. 2017;19(5):28. doi:10.1007/s11920-017-0780-z
8. Haddad M, Menchetti M, McKeown E, Tylee A, Mann A. The development and psychometric properties of a measure of clinicians’ attitudes to depression: the revised Depression Attitude Questionnaire (R-DAQ). BMC Psychiatry. 2015;15(1):7. doi:10.1186/s12888-014-0381-x
9. Botega N, Mann A, Blizard R, Wilkinson G. General practitioners and depression—first use of the depression attitude questionnaire. Int J Methods Psychiatr Res. 1992:169–180.
10. Sperber AD, Devellis RF, Boehlecke B. Cross-cultural translation: methodology and validation. J Cross Cult Psychol. 1994;25(4):501–524. doi:10.1177/0022022194254006
11. Brislin RW. Translation and content analysis of oral and written materials. Methodology. 1980:389–444.
12. R: the R project for statistical computing. Available from: https://www.r-project.org/.
13. Revelle W. Procedures for psychological, psychometric, and personality research. Acesso Em. 2012;9.
14. Williams B, Onsman A, Brown T. Exploratory factor analysis: A five-step guide for novices. Australas J Paramed. 2010;8:3. doi:10.33151/ajp.8.3.93
15. Courtney MGR, Gordon M. Determining the number of factors to retain in EFA: using the SPSS R-menu v2. 0 to make more judicious estimations. Pract Assess Res Eval. 2013;18(8):1–14.
16. Canatan R. A note on the statistical approximation properties of the modified discrete operators. Open J Discrete Math. 2012;2(03):114. doi:10.4236/ojdm.2012.23022
17. Yeomans KA, Golder PA. The Guttman-Kaiser criterion as a predictor of the number of common factors. Statistician. 1982;221–229. doi:10.2307/2987988
18. Cattell RB. The scree test for the number of factors. Multivariate Behav Res. 1966;1(2):245–276. doi:10.1207/s15327906mbr0102_10
19. Hayton JC, Allen DG, Scarpello V. Factor retention decisions in exploratory factor analysis: a tutorial on parallel analysis. Organizational Res Methods. 2004;7(2):191–205. doi:10.1177/1094428104263675
20. Corner S. Choosing the right type of rotation in PCA and EFA. JALT Test Eval SIG Newsl. 2009;13(3):20–25.
21. Osborne JW, Costello AB, Kellow JT. Best practices in exploratory factor analysis. Best Pract Quantit Methods. 2008:86–99.
22. Riedwyl H. Multivariate Statistics: A Practical Approach. Chapman and Hall; 1988.
23. McHorney CA, Jr JE W, Lu JR, Sherbourne CD, The MOS. 36-item Short-Form Health Survey (SF-36): III. Tests of data quality, scaling assumptions, and reliability across diverse patient groups. Med Care. 1994;40-66.
24. Stanley RM, Ridley K, Olds TS, Dollman J. Development and psychometric properties of the Y-PASS questionnaire to assess correlates of lunchtime and after-school physical activity in children. BMC Public Health. 2014;14(1):412. doi:10.1186/1471-2458-14-412
25. AM F Lecturabilidad de Fernández Huerta; 2016. Available from: https://legible.es/blog/lecturabilidad-fernandez-huerta/.
26. Crawford A. Fórmula y gráfico para determinar la comprensibilidad de textos del nivel primario en castellano. Lectura Y Vida. 1985;4:18–24.
27. Bhugra D. Attitudes towards mental illness: a review of the literature. Acta Psychiatr Scand. 1989;80(1):1–12. doi:10.1111/acp.1989.80.issue-1
28. Kërqeli A, Kelpi M, Tsigilis N. Dysfunctional attitudes and their effect on depression. Procedia-Social Behav Sci. 2013;84:196–204. doi:10.1016/j.sbspro.2013.06.534
29. Mukaka MM. A guide to appropriate use of correlation coefficient in medical research. Malawi Med J. 2012;24(3):69–71.
30. Haddad M, Waqas A, Sukhera AB, Tarar AZ. The psychometric characteristics of the revised depression attitude questionnaire (R-DAQ) in Pakistani medical practitioners: a cross-sectional study of doctors in Lahore. BMC Res Notes. 2017;10(1):333. doi:10.1186/s13104-017-2652-3
31. Carrozzino D. Clinimetric approach to rating scales for the assessment of apathy in Parkinson’s disease: a systematic review. Prog Neuro-Psychopharmacol Biol Psychiatry. 2019;109641. doi:10.1016/j.pnpbp.2019.109641
32. Carrozzino D, Svicher A, Patierno C, Berrocal C, Cosci F. The euthymia scale: a clinimetric analysis. Psychother Psychosom. 2019;88(2):119–121. doi:10.1159/000496230
33. Fava GA, Carrozzino D, Lindberg L, Tomba E. The clinimetric approach to psychological assessment: a tribute to per bech, MD (1942–2018). Psychother Psychosom. 2018;87(6):321–326. doi:10.1159/000493746
34. Sin NL, Lyubomirsky S. Enhancing well-being and alleviating depressive symptoms with positive psychology interventions: a practice-friendly meta-analysis. J Clin Psychol. 2009;65(5):467–487. doi:10.1002/jclp.20593
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.