Back to Journals » Psychology Research and Behavior Management » Volume 7
Somatic perception, cultural differences and immigration: results from administration of the Modified Somatic Perception Questionnaire (MSPQ) to a sample of immigrants
Authors Bragazzi NL, Del Puente G ![]() , Natta WM
, Natta WM
Received 4 October 2013
Accepted for publication 30 January 2014
Published 12 June 2014 Volume 2014:7 Pages 161—166
DOI https://doi.org/10.2147/PRBM.S55393
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Nicola Luigi Bragazzi, Giovanni Del Puente, Werner Maria Natta
Department of Neuroscience, Rehabilitation, Ophthalmology, Genetics, Maternal and Child Health, Section of Psychiatry, University of Genoa, Genoa, Italy
Abstract: The number of immigrants in Italy has doubled every 10 years from 1972 and Genoa hosts two large communities of immigrants from South America and Africa. We investigated differences in the somatic perception between immigrants and Italians and between South Americans and Africans living in the city of Genoa. During a 7 month period, an anonymous questionnaire asking for sociodemographic information and the Modified Somatic Perception Questionnaire (MSPQ) were administered to all immigrants accessing an outpatient clinic or the general practitioners offices. MSPQ mean scores were significantly higher in immigrant patients than in Italian patients, after adjusting for sex and age differences. We found no differences between South Americans and Africans in MSPQ score. The tendency to express discomfort through physical symptoms appears to be related to being a foreigner who arrived in Italy through a migratory trip and also to being a person who comes from a cultural context that is very different from the one of developed countries.
Keywords: immigrants, Modified Somatic Perception Questionnaire (MSPQ), somatization, transcultural psychiatry
Introduction
Somatization is a complex array of behaviors characterized by an abundant usage of body expressions and language to convey feelings of personal complaint and social distress,1 amplifying or distorting sometimes subtle physiological changes. Somatization is a challenge for physicians, due to its vague nature and since it requires a mature biopsychosocial model rather than a mechanistic simple biomedical one.1 The body is no longer considered a simple natural entity, but rather it is considered the result of cultural production, reproduction, and construction. The mind/body relationship is not a notion universally shared by all cultures. There is enormous cultural and historic variability in the relationship between these two entities.2
The concept of “mindful-body” sees the body woven between nature and culture. For the immigrant, in some stressful situations and contexts, the body becomes an actual blackboard, on which the conflicts, the pressures, the defenses, and the emotional stress that derive from the encounter with a different culture are written.3 Immigrants particularly use somatization while seeking medical help and accessing primary care services,4 with a prevalence ranging from 21.9%–25.0%5,6 up to 35.2%.7
Differences in the modes of somatic perception and amplification derive from ethnic factors,8,9 as well as other socioeconomic factors. Sensations arise and acquire meaning, even symbolic, through psychological and physiological mechanisms that are socioculturally influenced. People of different cultures therefore have different “Sensation Schemas,”10 that are conceptual models of meanings associated with somatic experience. They determine the basic attitudes of the individual with regard to somatic experiences and they contribute to determining the core of bodily identity.
The processes that produce and amplify the sensations, and that produce a symbolic meaning associated to them, include the following: attention,11 mood alteration with depression12 and anxiety,13 and the cultural meanings of the illness.9,14 Furthermore the ethnic–cultural physiology determines the knowledge of bodily functioning and steers attention toward particular stimuli and it induces the body’s self-monitoring.
Some mechanisms may be considered generators of specific sensations in the cultural experience; a sensation can become the indicator of dysregulation of physiological functioning.
Therefore each culture determines which specific parts of the body and which sensations must be most closely monitored.15 Thus, correct interpretation of bodily sensations requires considering the socially shared explanations of both the illness and of the bodily functioning. In a more interconnected and globalized society, it is of high interest to explore somatization among immigrants. For this reason, we have carried out this study, with the aim of studying somatization among the immigrant population in the metropolitan area of Genoa, Italy.
Objectives
Since 1974 the number of immigrants to Italy has doubled every 10 years. The areas of origin are above all Eastern Europe, Africa, Asia, and to a lesser degree South America. Currently there are approximately 5 million (legal) immigrants living in Italy, ie, 8.3% of the total population. The peculiarity in Genoa is that on the contrary, most of the immigrants come from South America (42%). The Ecuadorian community is the most numerous in Italy (around 50,000).16
We have taken advantage of this peculiarity to verify whether there are any differences in somatic perception between immigrants and Italians. We also investigated whether possible differences depend solely on the immigrant’s position or if they derive from different cultural aspects. Therefore we carried out a comparison between immigrants and Italians. Within the group of immigrants, we then compared the group of South Americans to the Africans. Our research was done between March 2010 and October 2010. Both groups (immigrants and Italians) were recruited from the offices of general practitioners (GPs).
Methods
To maximize recruitment, we selected two outpatient clinics in the area of Genoa most densely populated by immigrants and we involved all GPs working in the area. During a 7 month period (from March to October 2010) all immigrants accessing the outpatient clinics or the GPs’ offices were asked to participate in the study by their GP. We assumed most of the patients would come from South America or Africa. During the same time period we recruited a control group of Italian citizens accessing the same outpatient clinics or GPs’ offices. All patients who were willing to participate in the study were included, regardless of their specific medical problem. However, all the pathologies were of mild/moderate degree.
The Modified Somatic Perception Questionnaire (MSPQ) was administered because it has proved to be effective at measuring the amplification of the bodily sensations.17 It is a 13 item four-point self-report scale that has been developed for investigating chronic backache17 or other forms of chronic pain,18–29 stroke and cardiovascular diseases,30–34 tinnitus and Meniere’s disease,34–37 and patients undergoing surgery.39–49 It has also been used to measure somatization in nonpainful conditions.50,51 To the best of our best knowledge this questionnaire has never been used in an immigrant population.
The study questionnaire was anonymous, self administered, and easy to fill in. It included some demographic data (sex, age, country of origin, and number of years spent in Italy) and the MSPQ. The MSPQ, in its Italian version, is a 22 item four-point Likert scale investigating body perception and physiologic functions. It was available in English, German,52 Spanish, and Italian. The Italian version was derived from Conti53 and we believed no further adaptation was needed because the educational level of immigrants in Italy does not differ a lot from that of Italians and the proportion of illiterates among immigrants is 4.0%.54 To ensure patient cooperation, the clinician was allowed to help patients who had trouble understanding the questionnaire. This study was reviewed and approved by the Local Committee of the Psychiatric Department, San Martino Hospital, Genoa, Italy.
We conducted two subsequent analyses: a) comparison between Italian and immigrant patients and b) comparison between South American and African patients. Results are presented as frequency and percentage for categorical variables and mean and standard deviations for continuous variables. Group differences were analyzed using Pearson’s chi square test and the Mann–Whitney U test. Linear regression was then used to model the relationship between immigrant condition and somatic perception after adjusting for the effect of age and sex. Statistical analysis was carried out using Statistical Package for Social Sciences (v 22; IBM Corporation, Armonk, NY, USA).
Results
Our sample consisted of 329 patients (143 immigrants and 186 Italians). Immigrants in the Liguria region represent 7.8% of the resident population (8.3% in the city of Genoa). Immigrants from South America (51.8%) and Africa (32.2%) represent the two most relevant communities of non-European immigrants. In the area where we conducted our study, the immigrant population is estimated to be 11% of the resident population and our sample included 46 immigrants from Africa (32.2%) and 97 from South America (67.8%). One hundred and ninety-seven patients were asked to participate and 143 accepted. Differences between groups are shown in the upper part of Table 1. Italian participants were predominantly female (61.8%) and were slightly younger than immigrants (mean age 35.0 versus 38.3 years). MSPQ mean scores were significantly higher in immigrant patients than in Italian patients (8.3 versus 6.0).
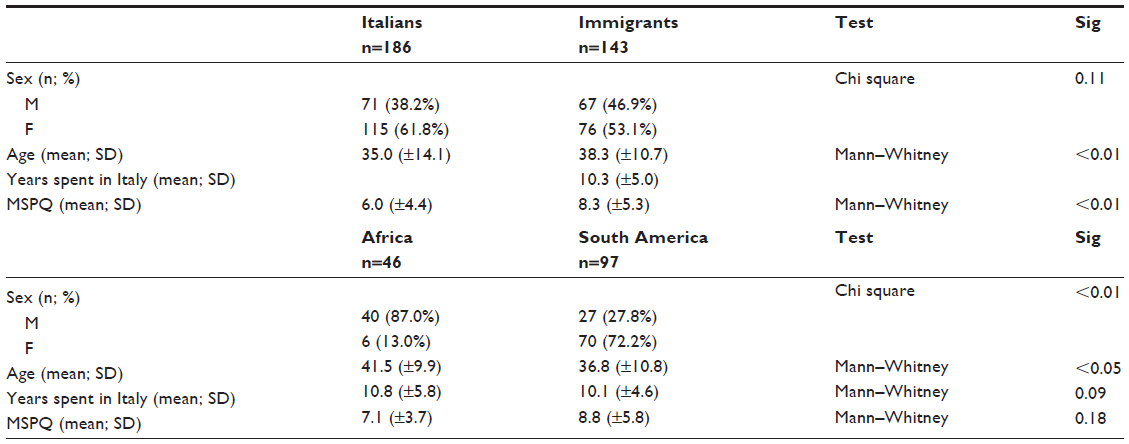 | Table 1 Group differences between Italian and immigrant patients (n=326) and immigrants from Africa and South America (n=143) |
Linear regression (Table 2) confirmed this significant relationship, after adjusting for sex and age differences. No relationship was found between age and somatic perception, while sex differences were statistically significant. In fact, female patients showed higher MSPQ scores after adjusting for age and immigrant condition. The overall effect of sex and immigrant conditions are similar (beta =0.25 and beta =0.26, respectively).
 | Table 2 Linear regression with Modified Somatic Perception Questionnaire as the independent variable and age, sex, and immigrant condition as dependent variables |
The lower part of Table 1 compares immigrants from Africa to immigrants from South America. Immigrants from Africa were older and predominantly male, while most of the immigrants from South America were female and mean age was lower. Such differences are statistically significant. We found no differences between groups in time spent in Italy and MSPQ score.
Discussion
Our results should be interpreted considering the following limitations: a) the cross-sectional nature and nonrandom study design of our survey; b) lack of specific information about social distress and other variables because of the phenomenon complexity, however, social conditions are virtually the same for all immigrants in the city of Genoa; c) lack of random selection of the sample (it is a convenience one), and therefore it may be not representative of the entire immigrant population in Genoa, since it is based on one set of clinics and on individuals who are attending that clinic; d) four patients needed to be helped in the questionnaire compilation and this may have slightly influenced the validity of some of the answers; and e) given the small number of people from each single country, the sample size was not sufficient to identify differences by countries of origin.
On the other hand, the study has some strengths: a) to the best of our best knowledge this is the first time the MSPQ has been used in a broad sample of an immigrant population; b) the methodology is clear and the questionnaire very simple; and c) the recruitment in GP offices provides specific information on immigrant population complaining about physical symptoms.
The comparison between immigrant and Italian patients showed a significant difference in the scores of the MSPQ scale. This means that the two groups express two different mean levels of somatization. Immigrants showed a greater tendency to somatize than the Italians, and this outcome is consistent with the extant literature.55,56 The higher somatization rates of immigrants may depend on their greater tendency to express psychic pain through their body. This tendency is characteristic of many developing countries and their cultural contexts.57 This theory is the so-called classical “somatization hypothesis.”
The comparison between African and South American immigrants did not show any statistically significant differences in MSPQ scales. This finding is different from the result obtained by Aragona et al5 who found a statistically significant difference among different nationality groups, with the somatization score being higher among the South Americans and Africans and lower among the Asian subjects. On the other hand, the classical “somatization hypothesis” mentioned above, for which some cultures are more likely to somatize than others, has been challenged by recent evidence that shows that the complaint of somatic symptoms is not influenced by the cultural background, and is more related to the immigration experience itself rather than to the cultural milieu.58 This means that the immigrants in our sample group tend to somatize more than the Italians. However, there are no substantial differences between the two ethnic groups we studied regarding how the mean level of physical distress is expressed. A hypothesis that may explain the greater tendency to somatize by immigrants is the particular condition of being an immigrant, in which they are confined and the psychosocial traits associated with it. Yet the Latin American group seemed to show a more marked, but not statistically significant, predisposition to somatization. Thus, the tendency to express discomfort through physical symptoms appears to be related to being a foreigner who arrived in Italy through a migratory trip and also to being a person who comes from a cultural context that is very different from the Western one.
Somatization is also believed to be very closely connected to the phenomenon of being an immigrant.14,59 However, our study is cross-sectional and not being a longitudinal one, we are not able to speculate whether the somatization is influenced by psychological distress and discomfort or if it is simply a transitory phenomenon due to the acculturation process as stated by some scholars.4,60,61 Further studies should clarify, by increasing the sample size per ethnic group, if there are differences among ethnicities and maybe enable study subjects in their country of origin to confirm the relationship between the migration phenomenon and somatization.
Specific training for GPs working in areas with high prevalence of immigrants could help them recognize physical symptoms as expression of psychological distress. A further step could be the development of health services for immigrants that address psychological problems related to migration and social integration.
Disclosure
The authors report no conflict of interest in this work.
References
Lin EH, Carter WB, Kleinman AM. An exploration of somatization among Asian refugees and immigrants in primary care. Am J Public Health. 1985;75(9):1080–1084. | |
Csordas TJ. Embodiment and Experience: The Existential Ground of Culture and Self. Cambridge: Cambridge University Press; 1994. | |
Scheper-Hughes N, Lock MM. The mindful body: a prolegomen to future work in medical anthropology. Medical Anthropology Quarterly. 1987;1(1):6–41. | |
Dastjerdi M. The case of Iranian immigrants in the greater Toronto area: a qualitative study. Int J Equity Health. 2012;11:9. | |
Aragona M, Rovetta E, Pucci D, Spoto J, Villa AM. Somatization in a primary care service for immigrants. Ethn Health. 2012;17(5):477–491. | |
Ritsner M, Ponizovsky A, Kurs R, Modai I. Somatization in an immigrant population in Israel: a community survey of prevalence, risk factors, and help-seeking behavior. Am J Psychiatry. 2000;157(3):385–392. | |
Aragona M, Tarsitani L, Colosimo F, et al. Somatization in primary care: a comparative survey of immigrants from various ethnic groups in Rome, Italy. Int J Psychiatry Med. 2005;35(3):241–248. | |
Kirmayer LJ, Young A, Robbins JM. Symptom attribution in cultural perspective. Can J Psychiatry. 1994;39(10):584–595. | |
Hinton DE, Howes D, Kirmayer LJ. Toward a medical anthropology of sensations: definition and research agenda. Transcult Psychiatry. 2008;1:142–162. | |
Hollan D. Self systems, cultural idioms of distress, and the psycho-bodily consequences of childhood suffering. Transcult Psychiatry. 2004;411:62–79. | |
Spence C. Multisensory integration, attention and perception. In: Roberts D, editor. Signals and Perception: The Fundamentals of Human Sensation. New York: Palgrave MacMillan; 2002:345–353. | |
Tylee A, Ghandi P. The importance of somatic symptoms in depression in primary care. Prim Care Companion J Clin Psychiatry. 2005;7:167–176. | |
Brown TA, Barlow DH. Classification of anxiety and mood disorders. In: Barlow DH, editor. Anxiety and Its Disorders: The Nature and Treatment of Anxiety and Panic. 2nd ed. New York: Guilford Press; 2002:292–327. | |
Kirmayer LJ, Sartorius N. Cultural models and somatic syndromes. Psychosom Med. 2007;69(9):832–840. | |
Lock MM. East Asian Medicine in Urban Japan: The Varieties of Medical Experience. Berkeley, CA: University of California Press; 1980. | |
Caritas/Migrantes. (2010). Immigrazione: Dossier Statistico [Immigration Statistical Dossier]. 2010, XX Rapporto. Roma: Idos Edizioni. Italian. | |
Main CJ. The Modified Somatic Perception Questionnaire MSPQ. J Psychosom Res. 1983;27(6):503–514. | |
Adams MA, Mannion AF, Dolan P. Personal risk factors for first-time low back pain. Spine (Phila Pa 1976). 1999;24(23):2497–2505. | |
Greenough CG. Recovery from low back pain. 1–5 year follow-up of 287 injury-related cases. Acta Orthop Scand Suppl. 1993;254:1–34. | |
Greenough CG, Fraser RD. Comparison of eight psychometric instruments in unselected patients with back pain. Spine (Phila Pa 1976). 1991;16(9):1068–1074. | |
Kerr HL, Dabke HV, Collins IE, Grevitt M. Claustrophobia: a proxy for psychological distress in patients with back pain. J Spinal Disord Tech. 2012;25(6):318–323. | |
Koho P, Aho S, Watson P, Hurri H. Assessment of chronic pain behaviour: reliability of the method and its relationship with perceived disability, physical impairment and function. J Rehabil Med. 2001;33(3):128–132. | |
Licciardone JC, Gatchel RJ, Kearns CM, Minotti DE. Depression, somatization, and somatic dysfunction in patients with nonspecific chronic low back pain: results from the OSTEOPATHIC Trial. J Am Osteopath Assoc. 2012;112(12):783–791. | |
Meyer K, Tschopp A, Sprott H, Mannion AF. Association between catastrophizing and self-rated pain and disability in patients with chronic low back pain. J Rehabil Med. 2009;41(8):620–625. | |
Patton CM, Hung M, Lawrence BD, et al. Psychological distress in a Department of Veterans Affairs spine patient population. Spine J. 2012;12(9):798–803. | |
Roh JH, Kim BJ, Jang JH, et al. The relationship of pain and health-related quality of life in Korean patients with Parkinson’s disease. Acta Neurol Scand. 2009;119(6):397–403. | |
Sikorski JM, Stampfer HG, Cole RM, Wheatley AE. Psychological aspects of chronic low back pain. Aust N Z J Surg. 1996;66(5):294–297. | |
Wand BM, Bird C, McAuley JH, Doré CJ, MacDowell M, De Souza LH. Early intervention for the management of acute low back pain: a single-blind randomized controlled trial of biopsychosocial education, manual therapy, and exercise. Spine (Phila Pa 1976). 2004;29(21):2350–2356. | |
Jansson-Fröjmark M, MacDonald S. Exploratory factor analysis of the Modified Somatic Perception Questionnaire on a sample with insomnia symptoms. Psychol Health Med. 2009;14(1):62–72. | |
Frasure-Smith N, Lespérance F. Depression and other psychological risks following myocardial infarction. Arch Gen Psychiatry. 2003;60(6):627–636. | |
Gockel M, Lindholm H, Alaranta H, Viljanen A, Lindquist A, Lindholm T. Cardiovascular functional disorder and stress among patients having neck-shoulder symptoms. Ann Rheum Dis. 1995;54(6):494–497. | |
Gockel M, Lindholm H, Vastamäki M, Lindqvist A, Viljanen A. Cardiovascular functional disorder and distress among patients with thoracic outlet syndrome. J Hand Surg Br. 1995;20(1):29–33. | |
Reynolds E, Ward L. Somatic awareness and symptom attribution in ischemic stroke patients. J Neurosci Nurs. 2014;46(1):55–62. | |
Warner CD. Somatic awareness and coronary artery disease in women with chest pain. Heart Lung. 1995;24(6):436–443. | |
Robinson SK, McQuaid JR, Viirre ES, et al. Relationship of tinnitus questionnaires to depressive symptoms, quality of well-being, and internal focus. Int Tinnitus J. 2003;9(2):97–103. | |
Newman CW, Jacobson GP, Spitzer JB. Development of the Tinnitus Handicap Inventory. Arch Otolaryngol Head Neck Surg. 1996;122(2):143–148. | |
Newman CW, Wharton JA, Jacobson GP. Self-focused and somatic attention in patients with tinnitus. J Am Acad Audiol. 1997;8(3):143–149. | |
Storper IS, Spitzer JB, Scanlan M. Use of glycopyrrolate in the treatment of Meniere’s disease. Laryngoscope. 1998;108(10):1442–1445. | |
Armaghani SJ, Lee DS, Bible JE, et al. Preoperative narcotic use and its relation to depression and anxiety in patients undergoing spine surgery. Spine (Phila Pa 1976). 2013;38(25):2196–2200. | |
Chaichana KL, Mukherjee D, Adogwa O, Cheng JS, McGirt MJ. Correlation of preoperative depression and somatic perception scales with postoperative disability and quality of life after lumbar discectomy. J Neurosurg Spine. 2011;14(2):261–267. | |
Donceel P, Du Bois M. Predictors for work incapacity continuing after disc surgery. Scand J Work Environ Health. 1999;25(3):264–271. | |
Gardner A, Pande KC. Graf ligamentoplasty: a 7-year follow-up. Eur Spine J. 2002;11 Suppl 2:S157–S163. | |
Godil SS, Parker SL, Zuckerman SL, et al. Determining the quality and effectiveness of surgical spine care: patient satisfaction is not a valid proxy. Spine J. 2013;13(9):1006–1012. | |
Havakeshian S, Mannion AF. Negative beliefs and psychological disturbance in spine surgery patients: a cause or consequence of a poor treatment outcome? Eur Spine J. 2013;22(12):2827–2835. | |
Lebow R, Parker SL, Adogwa O, et al. Microdiscectomy improves pain-associated depression, somatic anxiety, and mental well-being in patients with herniated lumbar disc. Neurosurgery. 2012;70(2):306–311. | |
Madan S, Boeree NR. Containment and stabilization of bone graft in anterior lumbar interbody fusion: the role of the Hartshill Horseshoe cage. J Spinal Disord. 2001;14(2):104–108. | |
Okoro T, Sell P. The prediction of outcome in somatised patients undergoing elective lumbar surgery. J Bone Joint Surg Br. 2009;91(4):517–521. | |
Penta M, Fraser RD. Anterior lumbar interbody fusion. A minimum 10-year follow-up. Spine (Phila Pa 1976). 1997;22(20):2429–2434. | |
Trief PM, Grant W, Fredrickson B. A prospective study of psychological predictors of lumbar surgery outcome. Spine (Phila Pa 1976). 2000;25(20):2616–2621. | |
Brasseux R, Greve KW, Gianoli GJ, Soileau JS, Bianchini KJ. The relationship between the modified somatic perception questionnaire and dynamic platform posturography. Otol Neurotol. 2008;29(3):359–362. | |
Larrabee GJ. Exaggerated pain report in litigants with malingered neurocognitive dysfunction. Clin Neuropsychol. 2003;17(3):395–401. | |
Meyer K, Sprott H, Mannion AF. Cross-cultural adaptation, reliability, and validity of the German version of the Pain Catastrophizing Scale. J Psychosom Res. 2008;64(5):469–478. | |
Conti L. Handbook of clinical rating scales and assessment in psychiatry. Florence:SEE (Firenze); 2000. | |
Devillanova C, Fasani F, Frattini T. (2009) Citizens without rights: to live and work in Milan illegaly. Università Commerciale Luigi Bocconi, Econpubblica Centre for Research on the Public Sector: Working Paper Series, Naga Report. 2007;125:1–71. Available from: http://www.naga.it/tl_files/naga/documenti/CittadiniSenzaDiritti2009.pdf. Accessed May 14, 2014. | |
Achotegui J. Emigration in hard conditions: the Immigrant Syndrome with chronic and multiple stress (Ulysses’ Syndrome). Vertex. 2005;16:105–113. Spanish. | |
Hoge EA, Tamrakar SM, Christian KM, et al. Cross-cultural differences in somatic presentation in patients with generalized anxiety disorder. J Nerv Ment Dis. 2006;194:962–966. | |
Kleinman AM. Anthropology and psychiatry: the role of culture in cross-cultural research on illness. Br J Psychiatry. 1987;151:447–454. | |
Heredia Montesinos A, Rapp MA, Temur-Erman S, Heinz A, Hegerl U, Schouler-Ocak M. The influence of stigma on depression, overall psychological distress, and somatization among female Turkish migrants. Eur Psychiatry. 2012;27 Suppl 2:S22–S26. | |
Escobar JI. Transcultural aspects of dissociative and somatoform disorders. Psychiatr Clin North Am. 1995;18:555–569. | |
Jurcik T, Chentsova-Dutton YE, Solopieieva-Jurcikova I, Ryder AG. Russians in treatment: the evidence base supporting cultural adaptations. J Clin Psychol. 2013;69(7):774–791. | |
Mak WW, Zane NW. The phenomenon of somatization among community Chinese Americans. Soc Psychiatry Psychiatr Epidemiol. 2004;39(12):967–974. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.