Back to Journals » Neuropsychiatric Disease and Treatment » Volume 14
Social adjustment and family function after drug switch from IR -methylphenidate to OROS-methylphenidate in patients with attention-deficit/hyperactivity disorder
Authors Chou WJ, Wang LJ ![]() , Lin CH, Liang SY, Chen VCH, Hou YM, Huang RR, Chou MC, Shang CY, Ho CP, Lai MC
, Lin CH, Liang SY, Chen VCH, Hou YM, Huang RR, Chou MC, Shang CY, Ho CP, Lai MC ![]()
Received 11 June 2018
Accepted for publication 3 October 2018
Published 23 October 2018 Volume 2018:14 Pages 2783—2791
DOI https://doi.org/10.2147/NDT.S176913
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Wen-Jiun Chou,1 Liang-Jen Wang,1 Chien-Ho Lin,2 Sun-Yuan Liang,3 Vincent Chin-Hung Chen,4 Yuh-Ming Hou,5 Rong-Rong Huang,6 Miao-Chun Chou,1 Chi-Yung Shang,7 Chi-Pui Ho,6 Meng-Chuan Lai8
1Department of Child and Adolescent Psychiatry, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, 2Department of Psychiatry, Chimei Medical Center, Tainan, 3Department of Psychiatry, Changhua Hospital, Changhua, 4Department of Psychiatry, Chang Gung Memorial Hospital and University, 5Chia-Yi Christian Hospital, Chiayi, 6Department of Child and Adolescent Psychiatry, Kai-Suan Psychiatric Hospital, Kaohsiung, 7Department of Psychiatry, National Taiwan University Hospital and College of Medicine, Taipei, Taiwan; 8Autism Research Centre, Department of Psychiatry, University of Cambridge, Cambridge, UK
Purpose: This prospective, single-arm, open-label, 8-week, multicenter study investigated the effectiveness of switching from immediate-release methylphenidate (IR-MPH) to osmotic controlled-release methylphenidate (OROS-MPH) in patients with attention-deficit/hyperactivity disorder (ADHD).
Patients and methods: Overall, 296 patients with ADHD (mean age: 9.5 years) already on IR-MPH treatment were enrolled. Upon enrollment, a flexible dose of OROS-MPH was administered, replacing IR-MPH. Patients were assessed at baseline and weeks 2, 4, and 8 using the Swanson, Nolan, and Pelham version IV scale (SNAP-IV) and the Clinical Global Impression for ADHD symptoms. The Social Adjustment Inventory for Children and Adolescents assessed social functions, and the Chinese Health Questionnaire (CHQ) and Family Adaptation, Partnership, Growth, Affection, and Resolve evaluated parental and family functions.
Results: Switching from IR-MPH to OROS-MPH yielded significant improvements in all ADHD symptoms, as rated by parents, teachers (SNAP-IV), and study investigators (Clinical Global Impression). CHQ scores and all Social Adjustment Inventory for Children and Adolescents subscores except spare time scores improved significantly. Patients with poor IR-MPH adherence had greater improvements in teacher-rated SNAP-IV and mothers’ mental health (CHQ) after switching.
Conclusion: Switching from IR-MPH to OROS-MPH improved patients’ behavioral ADHD symptoms and social adjustment, and mental health of patients’ mothers. This was most evident in patients who previously exhibited poor IR-MPH adherence.
Keywords: ADHD, central nervous system stimulant, drug adherence, family, social adjustment
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a common psychiatric disorder in children and adolescents. It occurs in 5.9%–7.1% of school-aged children worldwide,1,2 with a prevalence rate of 7.5% reported in a local Taiwan study.3 The core symptoms of ADHD are inattention, hyperactivity, and impulsivity. These symptoms frequently result in a negative impact on patients’ functional domains, including social adjustment, peer relationships, academic performance, and family function.4,5 Patients with ADHD commonly exhibit a pattern of behavioral difficulties, including noncompliance, increased demands on parents’ time, and decreased adaptability to change, all of which challenge the discipline within the family system.6,7 Previous studies have shown that parents or caregivers of children with ADHD can suffer significantly from poor familial relationships and severe psychological stress, rendering them at high risk for psychopathology.8,9
Pharmacotherapy is an effective therapeutic option, and the stimulant methylphenidate (MPH) has consistently been the first-line treatment for ADHD.10 Immediate-release MPH (IR-MPH) is a short-acting stimulant with a half-life of 2–3 hours, requiring multiple daily dosing to control symptoms throughout the day. In contrast, an osmotic controlled-release formulation of MPH (OROS-MPH) is an extended-release MPH HCl formulation. OROS-MPH facilitates easy administration to patients, with an added benefit of greater privacy, which helps avoid stigma and improves adherence to treatment.11,12 Compelling evidence indicates that OROS-MPH has clinical advantages and is cost-effective compared to IR-MPH.13–15 Among patients who had previously been treated with IR-MPH, the switch to OROS-MPH was associated with better symptom control in the after-school period,16,17 improved treatment adherence and effectiveness,18,19 better neurocognitive performance20 and health-related quality of life,21 and increased rates of ADHD symptom remission.22,23
However, there is a paucity of evidence regarding benefits related to the social adjustment and family function of patients with ADHD after switching from IR-MPH to OROS-MPH. Therefore, this study aimed to investigate the potential effects on clinical symptoms, social adjustment, and parents’ mental health status for children and adolescents with ADHD after a switch in pharmacotherapy from IR-MPH to OROS-MPH.
Patients and methods
Study population
The research protocol was approved by the Research Ethics Committee of the National Taiwan University (approval number, 200709006M; ClinicalTrials.gov number, NCT00758160). Eligible patients with a diagnosis of ADHD were recruited from the child psychiatry outpatient departments in ten Taiwanese hospitals.
The inclusion criteria were as follows: 1) clinical diagnosis of ADHD based on the criteria presented in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition;24 2) age between 6 and 18 years; 3) patients who had been treated with a daily dose of >10 mg IR-MPH for at least 4 weeks prior to enrollment, but for whom previous treatment was considered unsatisfactory due to one or more of the following reasons: lack of efficacy, lack of tolerability or safety, lack of adherence, and/or other reasons; and 4) a signed and dated informed consent form provided before study entry (the written informed consent was signed by the patient or the patient’s legally acceptable representative according to local requirements).
Patients were excluded if they 1) had any clinically significant abnormal physical or laboratory examination at baseline screening, such as significant gastrointestinal problems, glaucoma, or hypersensitivity to MPH; 2) were receiving concomitant medication that was likely, in the investigator’s opinion, to interfere with safe administration of MPH (eg, theophylline, coumarin, or anticonvulsants); or 3) were pregnant or lactating women or women of child-bearing potential who were not practicing a reliable form of birth control. Patients taking concomitant psychotropic medications that did not interfere with MPH administration (eg, fluoxetine and imipramine) were few (n=5) and were not excluded from the study.
Outcome measures
The Swanson, Nolan, and Pelham version IV (SNAP-IV) rating scale is a 26-item investigatory tool that has frequently been used in studies related to ADHD. SNAP-IV employs a 4-point Likert scale where a scoring range of 0–3 represents the qualitative judgments “not at all”, “just a little”, “quite a lot”, and “very much”, respectively.25 The SNAP-IV scale encompasses inattention, hyperactivity/impulsivity, and oppositional symptoms (items 1–9, 10–18, and 19–26, respectively). The norm and psychometric properties of the Chinese SNAP-IV scale have been established in Taiwanese child and adolescent populations.26,27
The Social Adjustment Inventory for Children and Adolescents (SAICA) is a 77-item semi-structured interview scale designed for administration to school-aged children (6–18 years) or their parents in order to collect information about their children.28 SAICA evaluates a child’s current level of function in the domains of school, spare time, peer relations, and home behaviors. A higher mean score (items rated on 4-point Likert scale from 1 to 4) indicates either poorer social function or a more severe social problem. The Chinese version of SAICA has been reported to have satisfactory levels of reliability (intraclass correlations: 0.45–0.84) and concurrent validity (Cronbach’s α: 0.71–0.76).29,30
The Clinical Global Impression-Severity (CGI-S) and Clinical Global Impression-Improvement (CGI-I) are single-item assessments of the global severity and improvement of ADHD symptoms in relation to the clinician’s total experience with other ADHD patients, after reviewing all returned questionnaires and conducting a clinical assessment of patients’ behavioral symptoms.31 Severity is rated on a 7-point scale with the extremes of 1 and 7 representing ratings ranging from normal to most extremely ill, respectively. The degree of improvement is also rated on a 7-point scale.
The Chinese Health Questionnaire (CHQ) is a 12-item self-reporting questionnaire that was derived from the General Health Questionnaire.32 The CHQ includes symptoms of anxiety, depression, and somatic complaints and has been widely used in primary care and community settings in Taiwan to screen for patients who have minor psychiatric disorders.33
The Family Adaptation, Partnership, Growth, Affection, and Resolve (Family APGAR) is a 5-item measure designed to assess the five dimensions of perceived family support: adaptation, partnership, growth, affection, and resolve. Each item is rated on a 3-point scale, with higher scores indicating greater family support.34 The Chinese Family APGAR has been used to assess family functioning in students with mental disabilities.35
Study design
This was a prospective, single-arm, open-label, 8-week, multicenter study. A total of 296 patients with ADHD were enrolled. After obtaining informed consent, we obtained baseline characteristics of the patients. The psychological status of the patients’ parents was assessed using the CHQ (by parents). Patients’ familial relationships were evaluated using the Family APGAR (by parents), whereas school performance and social adjustment were assessed using the SAICA (by parents). ADHD symptoms were measured using the SNAP-IV (by parents and teachers) and CGI rating (by study investigators).
The treatment phase commenced with the administration of OROS-MPH in place of IR-MPH. The dosage of OROS-MPH was flexible (18, 36, or 54 mg). Clinicians adjusted each patient’s dose according to the patient’s clinical responses and/or side effects. During the OROS-MPH dosing regimen, SNAP-IV, CGI-S, and CGI-I were assessed at baseline and weeks 2, 4, and 8, while Family APGAR and SAICA were assessed at baseline and weeks 4 and 8.
Safety assessments involved the monitoring and recording of all adverse events (noting, in particular, any serious adverse events), vital signs, and routine physical examinations. The amount of drug returned to medical professionals was used to determine treatment adherence. Patients’ administration of the medication once daily for >70% of the treatment days was recorded as good adherence. Patients were allowed to withdraw from the study at any time; the reasons for withdrawal or any loss to follow-up were recorded. Discontinuation was defined as a patient who was enrolled in the study and discontinued OROS-MPH treatment before his/her medical chart was reviewed.
Statistical analysis
Data were analyzed using SPSS version 16.0 for Windows (SPSS Inc., Chicago, IL, USA). Variables were presented as either mean±SD or frequency (%). All statistical tests were two-tailed, and differences were considered significant at P<0.05.
Analyses were conducted in the intent-to-treat analysis set. All patients who received OROS-MPH at least once and who provided at least one post-baseline efficacy measurement were included in the efficacy data analyses. The last observation carried forward method was used to account for missing data. Longitudinal trends in outcome measures (SNAP-IV, CGI, SAICA, CHQ, and Family APGAR) were analyzed using a generalized linear model, followed by a least significant difference post hoc test. The relationship between caregivers’ mental health status and their perception of their child’s symptoms was examined using the Pearson’s correlation. We calculated the changes in each outcome by documenting observations from baseline to the last visit. A multivariate linear regression model was used to identify the factors that predicted changes in outcomes of patients with ADHD.
Results
A total of 296 patients met the inclusion criteria and were enrolled in this study (mean age: 9.5 years, range: 6.0–17.0 years; Table 1). Of the study population, 247 (83.4%) were male and 49 (16.6%) were female. A majority of the patients were elementary school students (n=241, 81.4%). Most of the patients’ parents held a high school diploma or higher degree (father, 80.4%; mother, 83.4%). The combined ADHD subtype was predominant among patients (n=201, 67.9%), followed by the inattentive subtype (n=90, 30.4%) and the hyperactive subtype (n=3, 1.0%); subtype information was missing for two patients. In total, 252 (85.1%) patients completed the study. A majority of patients (75.0%–94.3%) had an acceptable level of adherence to OROS-MPH treatment at different doses.
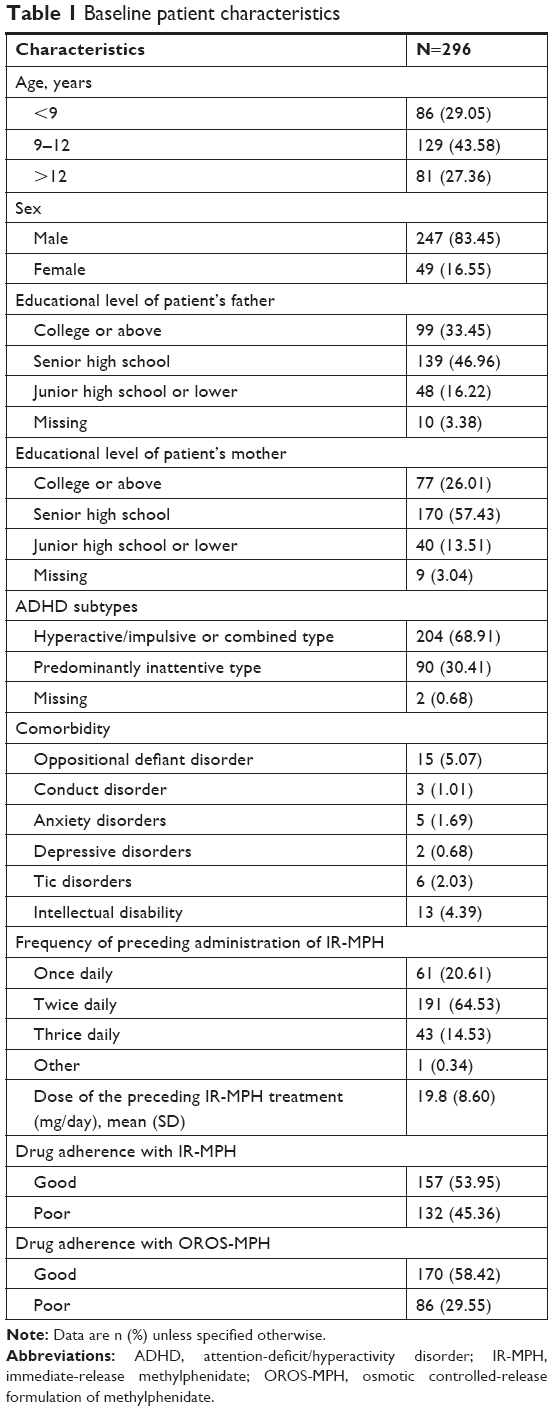 | Table 1 Baseline patient characteristics |
At baseline, a complete SNAP-IV assessment from parents and teachers was available for 293 (99.0%) and 281 (94.9%) patients, respectively. CHQ and Family APGAR scores were available for 275 (92.9%) mothers and 216 (73.0%) fathers. CGI scores were available for 290 (98.0%) patients. SAICA subscales for school function, spare time function, peer relationships, and home behaviors were available for 291 (98.3%), 295 (99.7%), 293 (99.0%), and 295 (99.7%) patients, respectively. At subsequent visits, the percentage of missing data was low (Table S1).
Measurements for patients with ADHD
After switching from IR-MPH to OROS-MPH, patients’ ADHD behavioral symptoms were perceived by their parents to have significantly improved in all three dimensions of SNAP-IV (inattention, hyperactivity/impulsivity, and oppositional symptoms) from baseline to the three follow-up visits (P<0.001; Table 2). All three dimensions of the SNAP-IV scores rated by patients’ teachers also showed significant improvements between baseline and the three visits (P<0.001).
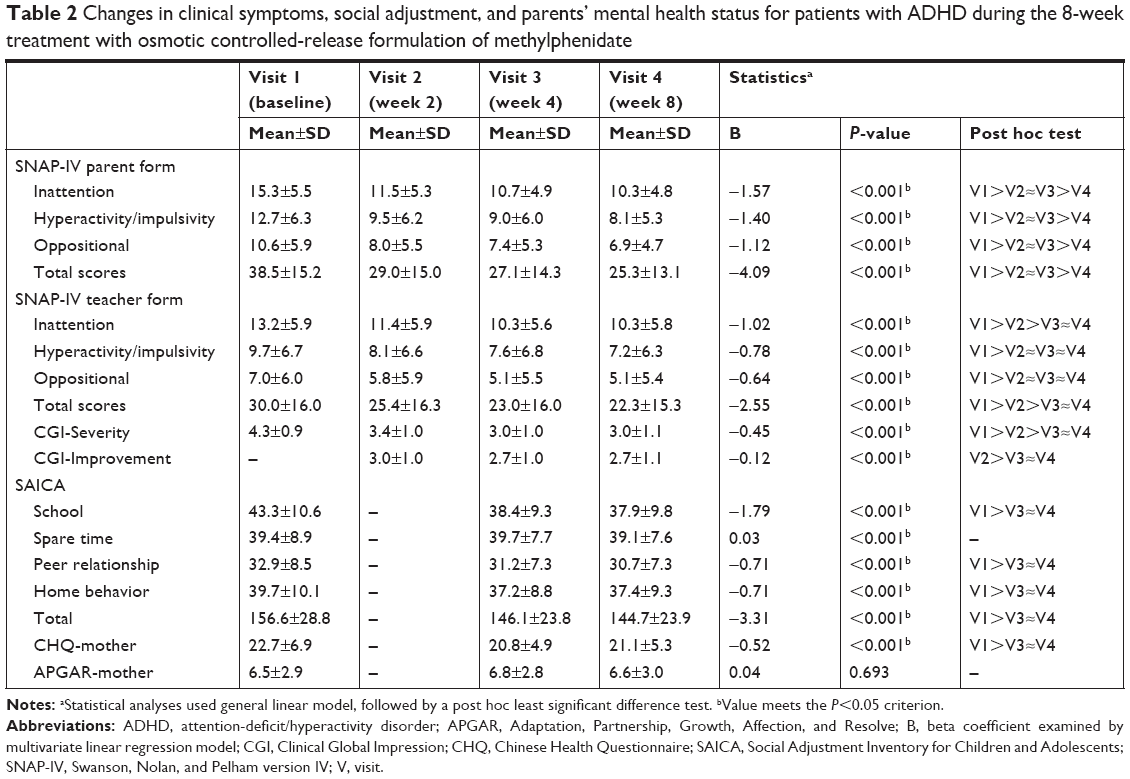 | Table 2 Changes in clinical symptoms, social adjustment, and parents’ mental health status for patients with ADHD during the 8-week treatment with osmotic controlled-release formulation of methylphenidate |
The SAICA assessment evaluated the change in patients’ social adjustment after they switched from IR-MPH to OROS-MPH for at least 4 weeks. With regard to SAICA subscales, school function (P<0.001), peer relationships (P<0.001), and home behaviors (P<0.001) significantly improved, but the spare time function did not (P=0.828).
The severity of patients’ overall ADHD symptoms (CGI-S) significantly improved after the medication switch, as assessed by the study investigator (P<0.001 for the differences between each of the three visits and baseline). Similarly, the CGI-I scores indicated significant improvement in ADHD symptoms (P<0.001).
Measurements for patients’ caregivers
The results of the CHQ completed by patients’ mothers indicated that the mothers’ mental health status significantly improved from baseline at weeks 4 (P<0.001) and 8 (P=0.003). However, the mental health status of patients’ fathers did not exhibit any significant changes during the study (P=0.587 and P=0.581 for the comparisons of weeks 4 and 8 to baseline, respectively). Family APGAR showed that, compared with the baseline period, there was no significant difference in familial support received by the caregivers (either father or mother) during the study (P=0.534 for father; P=0.882 for mother).
The Pearson’s correlation coefficients between CHQ and SNAP-IV scores (rated by patients’ caregivers) ranged from 0.22 to 0.38 (from baseline to week 8), which was statistically significant (P<0.001).
Factors associated with outcomes
We also examined the factors associated with changes in ADHD symptoms, social function, and mothers’ psychological status after patients with ADHD switched from IR-MPH to OROS-MPH (Table 3). Patients with poor adherence to IR-MPH dosing regimens before the drug switch had greater improvement in SNAP-IV total scores rated by teachers (P=0.031) and in CHQ scores rated by mothers (P=0.030). With the exception of adherence to previous IR-MPH treatment, no other baseline characteristics were reliable predictors of changes in the outcome measures.
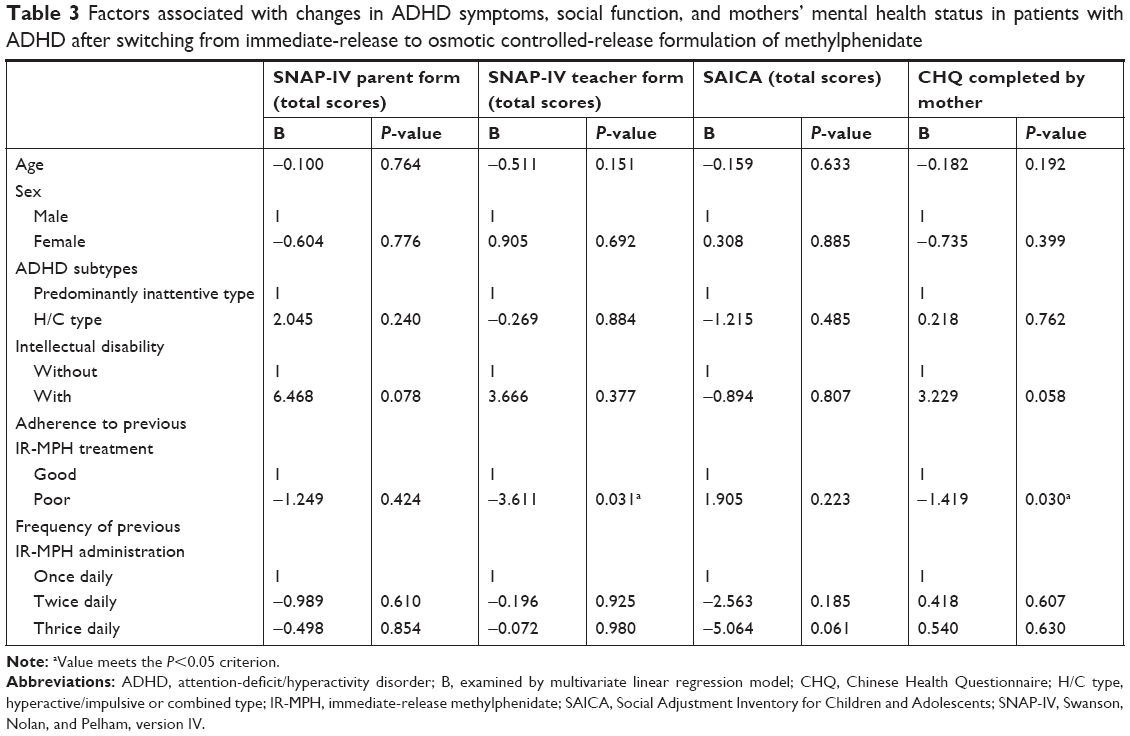 | Table 3 Factors associated with changes in ADHD symptoms, social function, and mothers’ mental health status in patients with ADHD after switching from immediate-release to osmotic controlled-release formulation of methylphenidate |
Safety
The most common adverse event that developed during the study was a decrease in appetite (27.0%–33.8%, reported during the three follow-up visits). Other adverse events included nausea, drowsiness, insomnia, headache, dizziness, stomachache, and abdominal pain. Patients’ body weight was significantly decreased at weeks 4 (0.8 kg, P=0.040) and 8 (1.0 kg, P=0.006). No notable changes in vital signs were detected during the study.
Discussion
The results of this prospective, open-label study suggest that switching from IR-MPH to OROS-MPH improves the core symptoms of ADHD, as reflected in both parent and teacher ratings. Inattention, hyperactivity/impulsivity, and oppositional symptom scores consistently declined from the second week after baseline through the duration of the study. These findings were generally comparable with previous research studies that investigated similar topics.36 In one randomized controlled trial of once-daily dosing of OROS-MPH compared with thrice-daily dosing of IR-MPH in children with ADHD, investigators observed an improvement in symptoms and a decrease in parental stress when children were switched to OROS-MPH compared with children who continued on IR-MPH.37 Among those patients who had been previously treated with IR-MPH, switching to OROS-MPH improved drug adherence and symptom control throughout the day.16–19 In addition, we found that three of the four dimensions of social function measured by the SAICA collectively improved after the switch. As ADHD symptoms frequently have a negative impact on patients’ social adjustment, peer relationships, and family function,4,5 increased treatment adherence and reduction in the severity of ADHD symptoms may result in improvements in these functional impairments. Taken together, these findings suggest that switching from IR-MPH to OROS-MPH may provide improvement both in terms of patients’ ADHD symptoms and their social function.
With regard to caregivers’ mental health status (CHQ scores), we found that mothers’ CHQ scores significantly improved, but fathers’ CHQ scores did not. Mothers’ mental health status was significantly correlated with the ADHD symptoms (SNAP-IV scores) of their children. Patients with ADHD commonly exhibit a pattern of behavioral difficulties,7 and patients’ parents may face challenging caregiving demands as they try to effectively manage their child’s difficult behaviors.6 Compared with fathers, mothers usually take on more responsibility for supervising their children’s school performance and taking care of their children at home. Therefore, mothers may more easily perceive their children’s improvement in ADHD symptoms and social function. One would predict that improvements in patients’ ADHD symptoms and social adjustment would reduce the psychological burden on patients’ mothers. However, family relationship, as assessed by the Family APGAR, did not reveal any improvement for either mothers or fathers. This finding suggests that the quality of family support, adaptation, and partnership might not be improved solely through a medication switch.38
We found that poor adherence to previous IR-MPH treatment was associated with greater improvements in teacher-rated ADHD symptoms and in mothers’ mental health after switching to OROS-MPH. Approximately half of the study population (45.4%) had poor adherence to IR-MPH (patients accurately administered the medication once daily for <70% of treatment days) before the drug switch. Drug adherence improved in a majority of patients after the medication was switched to OROS-MPH (rate of poor adherence: 5.7%–25%). Common reasons for poor adherence to IR-MPH treatment are intolerable side effects, multi-dose administration, and social stigma.39,40 Poor adherence to medication is often a limiting factor that prevents optimal symptom control in the treatment of ADHD.11 Therefore, it is critical for physicians to consider adherence to therapy while determining a treatment strategy for patients with ADHD. Switching from IR-MPH to OROS-MPH for the treatment of ADHD has been shown to provide better compliance and convenience.36 In patients with poor adherence to IR-MPH, switching to OROS-MPH can improve patients’ drug adherence, which can lead to better control of patients’ behavioral symptoms and a decrease in mothers’ stress and generally negative emotional state.
This study had several limitations. First, this was a prospective, open-label, non-randomized study, and therefore, there was no comparison group. Symptom improvements may easily have been inflated by the placebo effect and rater bias. Whether the improved ADHD symptoms and social adjustment were specifically derived from OROS-MPH administration requires further clarification. Second, the diagnosis of ADHD and its comorbidities was based primarily on a clinical interview according to criteria described in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition. However, without a structural diagnostic instrument or a standardized neuropsychological test, the psychiatric comorbidities in patients with ADHD might be underdiagnosed. Third, the measure of social adjustment (SAICA) relied solely on reports by patients’ caregivers. Compared with teachers, caregivers have fewer opportunities to directly observe patients’ performance in school, and this may reduce the reliability of measurements. Fourth, some crucial factors associated with social and family function, such as adverse life events and socioeconomic status, were not accounted for in this study. Whether changes in social function and parenting stress were moderated by this factor remains unknown. Finally, the treatment procedure for OROS-MPH was not standardized, and patients’ treatment-seeking behaviors were not strictly controlled. Thus, the findings reported herein may have been influenced by variations in dosing strategy or additional non-pharmacological interventions.
Conclusion
Switching medication from IR-MPH to OROS-MPH improved patients’ behavioral ADHD symptoms and their social adjustment at school and at home. In addition, patients’ mothers (primary caregivers) reported significantly reduced mental stress. These results might be attributed to either improved drug adherence or more stable concentrations of medication. However, long-term randomized controlled trials are warranted to confirm the beneficial effects of medication switching on social adjustment and parental stress.
Acknowledgments
This study (CCT-TWN-MA6) was sponsored by Janssen Taiwan. We would like to thank all of the child psychiatrists and the study participants and their parents who participated in this study. The abstract of this paper was presented at the IACAPAP 20th world congress as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in Neuropsychiatrie de l’Enfance et de l’Adolescence. 2012;60(5):S262 entitled “The family impact in children and adolescent with ADHD after the switch of treatment from immediate-release MPH to OROS-MPH”: http://www.em-consulte.com/en/article/736902.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Polanczyk G, de Lima MS, Horta BL, Biederman J, Rohde LA. The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatry. 2007;164(6):942–948. | ||
Polanczyk GV, Willcutt EG, Salum GA, Kieling C, Rohde LA. ADHD prevalence estimates across three decades: an updated systematic review and meta-regression analysis. Int J Epidemiol. 2014;43(2):434–442. | ||
Gau SS, Chong MY, Chen TH, Cheng AT. A 3-year panel study of mental disorders among adolescents in Taiwan. Am J Psychiatry. 2005;162(7):1344–1350. | ||
Feldman HM, Reiff MI. Clinical practice. Attention deficit-hyperactivity disorder in children and adolescents. N Engl J Med. 2014;370(9):838–846. | ||
Tarver J, Daley D, Sayal K. Attention-deficit hyperactivity disorder (ADHD): an updated review of the essential facts. Child Care Health Dev. 2014;40(6):762–774. | ||
Counts CA, Nigg JT, Stawicki JA, Rappley MD, von Eye A. Family adversity in DSM-IV ADHD combined and inattentive subtypes and associated disruptive behavior problems. J Am Acad Child Adolesc Psychiatry. 2005;44(7):690–698. | ||
Heath CL, Curtis DF, Fan W, Mcpherson R. The association between parenting stress, parenting self-efficacy, and the clinical significance of child ADHD symptom change following behavior therapy. Child Psychiatry Hum Dev. 2015;46(1):118–129. | ||
Deault LC. A systematic review of parenting in relation to the development of comorbidities and functional impairments in children with attention-deficit/hyperactivity disorder (ADHD). Child Psychiatry Hum Dev. 2010;41(2):168–192. | ||
Hernández-Otero I, Doddamani L, Dutray B, et al. Stress levels experienced by parents of children with and without attention-deficit/hyperactivity disorder during the back-to-school period: results of a European and Canadian survey. Int J Psychiatry Clin Pract. 2015;19(1):8–17. | ||
Findling RL. Evolution of the treatment of attention-deficit/hyperactivity disorder in children: a review. Clin Ther. 2008;30(5):942–957. | ||
Gau SS, Chen SJ, Chou WJ, et al. National survey of adherence, efficacy, and side effects of methylphenidate in children with attention-deficit/hyperactivity disorder in Taiwan. J Clin Psychiatry. 2008;69(1):131–140. | ||
Katzman MA, Sternat T. A review of OROS methylphenidate (Concerta(®)) in the treatment of attention-deficit/hyperactivity disorder. CNS Drugs. 2014;28(11):1005–1033. | ||
Punja S, Zorzela L, Hartling L, Urichuk L, Vohra S. Long-acting versus short-acting methylphenidate for paediatric ADHD: a systematic review and meta-analysis of comparative efficacy. BMJ Open. 2013;3(3):e002312. | ||
Schawo S, van der Kolk A, Bouwmans C, et al. Probabilistic Markov model estimating cost effectiveness of methylphenidate osmotic-release oral system versus immediate-release methylphenidate in children and adolescents: which information is needed? Pharmacoeconomics. 2015;33(5):489–509. | ||
van der Schans J, Kotsopoulos N, Hoekstra PJ, Hak E, Postma MJ. Cost-effectiveness of extended-release methylphenidate in children and adolescents with attention-deficit/hyperactivity disorder sub-optimally treated with immediate release methylphenidate. PLoS One. 2015;10(5):e0127237. | ||
Kim BN, Kim YN, Cheong US, et al. Switching from methylphenidate-immediate release (MPH-IR) to methylphenidate-OROS (OROS-MPH): a multi-center, open-label study in Korea. Clin Psychopharmacol Neurosci. 2011;9(1):29–35. | ||
Remschmidt H, Hoare P, Ettrich C, et al. Symptom control in children and adolescents with attention-deficit/hyperactivity disorder on switching from immediate-release MPH to OROS MPH Results of a 3-week open-label study. Eur Child Adolesc Psychiatry. 2005;14(6):297–304. | ||
Chou WJ, Chou MC, Tzang RF, et al. Better efficacy for the osmotic release oral system methylphenidate among poor adherents to immediate-release methylphenidate in the three ADHD subtypes. Psychiatry Clin Neurosci. 2009;63(2):167–175. | ||
Ramos-Quiroga JA, Bosch R, Castells X, et al. Effect of switching drug formulations from immediate-release to extended-release OROS methylphenidate: a chart review of Spanish adults with attention-deficit hyperactivity disorder. CNS Drugs. 2008;22(7):603–611. | ||
Kim Y, Shin MS, Kim JW, Yoo HJ, Cho SC, Kim BN. Neurocognitive effects of switching from methylphenidate-IR to OROS-methylphenidate in children with ADHD. Hum Psychopharmacol. 2009;24(2):95–102. | ||
Kordon A, Stollhoff K, Niederkirchner K, Mattejat F, Rettig K, Schäuble B. Exploring the impact of once-daily OROS® methylphenidate (MPH) on symptoms and quality of life in children and adolescents with ADHD transitioning from immediate-release MPH. Postgrad Med. 2011;123(5):27–38. | ||
Chou WJ, Chen SJ, Chen YS, et al. Remission in children and adolescents diagnosed with attention-deficit/hyperactivity disorder via an effective and tolerable titration scheme for osmotic release oral system methylphenidate. J Child Adolesc Psychopharmacol. 2012;22(3):215–225. | ||
Tzang RF, Wang YC, Yeh CB, et al. Naturalistic exploration of the effect of osmotic release oral system-methylphenidate on remission rate and functional improvement in Taiwanese children with attention-deficit-hyperactivity disorder. Psychiatry Clin Neurosci. 2012;66(1):53–63. | ||
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed. Washington, DC: American Psychiatric Association; 2000. | ||
Bussing R, Fernandez M, Harwood M, et al. Parent and teacher SNAP-IV ratings of attention deficit hyperactivity disorder symptoms: psychometric properties and normative ratings from a school district sample. Assessment. 2008;15(3):317–328. | ||
Gau SS, Lin CH, Hu FC, et al. Psychometric properties of the Chinese version of the Swanson, Nolan, and Pelham, Version IV Scale-Teacher Form. J Pediatr Psychol. 2009;34(8):850–861. | ||
Gau SS, Shang CY, Liu SK, et al. Psychometric properties of the Chinese version of the Swanson, Nolan, and Pelham, version IV scale – parent form. Int J Methods Psychiatr Res. 2008;17(1):35–44. | ||
John K, Gammon GD, Prusoff BA, Warner V. The Social Adjustment Inventory for Children and Adolescents (SAICA): testing of a new semistructured interview. J Am Acad Child Adolesc Psychiatry. 1987;26(6):898–911. | ||
Gau SS, Shen HY, Chou MC, Tang CS, Chiu YN, Gau CS. Determinants of adherence to methylphenidate and the impact of poor adherence on maternal and family measures. J Child Adolesc Psychopharmacol. 2006;16(3):286–297. | ||
Gau SS. Parental and family factors for attention-deficit hyperactivity disorder in Taiwanese children. Aust N Z J Psychiatry. 2007;41(8):688–696. | ||
Guy W. ECDEU Assessment Manual for Psychopharmacology. Revised 1976. Maryland: US Department of Health, Education, and Welfare. | ||
Goldberg DP, Gater R, Sartorius N, et al. The validity of two versions of the GHQ in the WHO study of mental illness in general health care. Psychol Med. 1997;27(1):191–197. | ||
Cheng TA, Williams P. The design and development of a screening questionnaire (CHQ) for use in community studies of mental disorders in Taiwan. Psychol Med. 1986;16(2):415–422. | ||
Smilkstein G, Ashworth C, Montano D. Validity and reliability of the family APGAR as a test of family function. J Fam Pract. 1982;15(2):303–311. | ||
Chau TT, Hsiao TM, Huang CT, Liu HW. 家庭關懷度指數的初步研究 [A preliminary study of family Apgar index in the Chinese]. Gaoxiong Yi Xue Ke Xue Za Zhi. 1991;7(1):27–31. Chinese. | ||
Gormez V, Avery B, Mann H. Switching from immediate release to sustained release methylphenidate in the treatment of children and adolescents with attention deficit/hyperactivity disorder. Eur Rev Med Pharmacol Sci. 2013;17(17):2345–2349. | ||
Steele M, Weiss M, Swanson J, Wang J, Prinzo RS, Binder CE. A randomized, controlled effectiveness trial of OROS-methylphenidate compared to usual care with immediate-release methylphenidate in attention deficit-hyperactivity disorder. Can J Clin Pharmacol. 2006;13(1):e50–e62. | ||
Kim JW, Park S, Kim BN, et al. Parental perceived benefits of OROS-methylphenidate treatment for the child with attention-deficit/hyperactivity disorder and for parents themselves. Pharmacopsychiatry. 2013;46(4):137–146. | ||
Ahmed R, McCaffery KJ, Aslani P. Factors influencing parental decision making about stimulant treatment for attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol. 2013;23(3):163–178. | ||
Gajria K, Lu M, Sikirica V, et al. Adherence, persistence, and medication discontinuation in patients with attention-deficit/hyperactivity disorder – a systematic literature review. Neuropsychiatr Dis Treat. 2014;10:1543–1569. |
Supplementary material
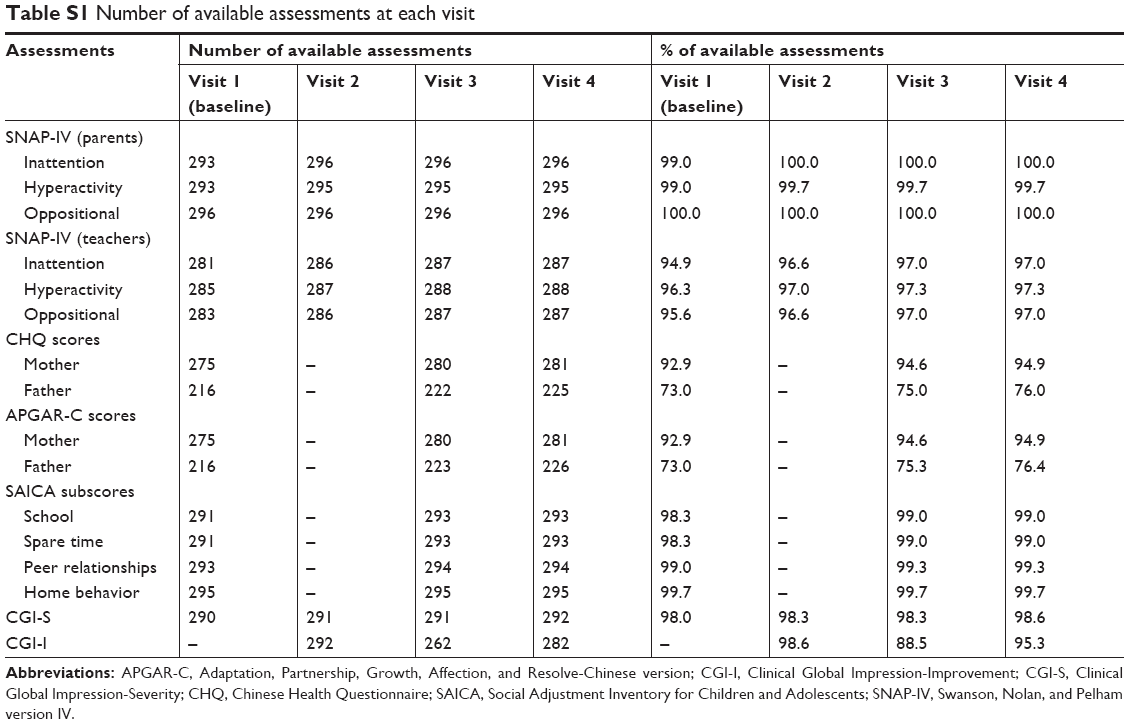 | Table S1 Number of available assessments at each visit |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.