Back to Journals » Patient Preference and Adherence » Volume 20
Smart Blister System with and without Mobile App Support: A Randomized Controlled Usability Trial
Authors Eikholt AA ![]() , Chan AHY, Van Boven JFM
, Chan AHY, Van Boven JFM ![]()
Received 8 October 2025
Accepted for publication 2 February 2026
Published 11 March 2026 Volume 2026:20 567253
DOI https://doi.org/10.2147/PPA.S567253
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Emma Veale
Amber A Eikholt,1 Amy HY Chan,2 Job FM Van Boven1,3
1Department of Clinical Pharmacy & Pharmacology, University Medical Center Groningen, University of Groningen, Groningen, the Netherlands; 2School of Pharmacy, Faculty of Medical and Health Sciences, The University of Auckland, Auckland, New Zealand; 3Medication Adherence Expertise Centre of the Northern Netherlands (MAECON), Groningen, the Netherlands
Correspondence: Job FM Van Boven, Department of Clinical Pharmacy & Pharmacology, University Medical Center Groningen, University of Groningen, Hanzeplein 1 (Internal Postcode AP50), Groningen, 9700 RB, the Netherlands, Tel +31503617893, Email [email protected]
Purpose: Medication non-adherence remains a major barrier to effective long-term disease management. Smart packaging technologies offer digital solutions to monitor and support adherence. This study evaluated the usability and feasibility of a smart blister pack (Cerepak®) for monitoring medication adherence, both with and without a mobile adherence app (MEMS® Mobile), in healthy adult participants.
Methods: In this randomized controlled trial, 36 participants were assigned to use the smart blister pack either with the mobile adherence app (intervention) or without the app (control) over eight weeks, simulating twice-daily medication intake. Usability was assessed using the System Usability Scale (SUS) and user experience surveys. Semi-structured interviews explored user satisfaction, barriers, and suggestions for improvement. Adherence was measured electronically and via pill counts.
Results: Usability scores were significantly higher in the intervention group (median SUS: 80.0) compared to the control group (67.5; p = 0.0007). Participants appreciated the packaging’s visual layout and the app’s reminder and tracking features. Qualitative findings highlighted improved structure, motivation, and ease of use with the app, alongside technical and packaging challenges. Electronic adherence was 91.7% in the app group and 86.2% in the non-app group. Pill count adherence was 96.4% and 88.0%, respectively. No statistically significant differences were observed. Intermittent data capture issues associated with the smart blister pack led to minor performance inconsistencies in 10.4% of packages, which were accounted for in the analysis, ensuring data integrity.
Conclusion: The smart blister pack is usable and feasible for daily medication taking and tracking, particularly when supported by a mobile app. These findings support further research into clinical populations and long-term implementation studies.
Keywords: smart packaging, medication adherence, digital health, usability, mobile app, mHealth
Introduction
Medication non-adherence remains a major and costly challenge in the management of long-term conditions. Despite the availability of effective pharmacological therapies, many patients do not take their medication as prescribed, leading to suboptimal health outcomes, disease progression, and increased healthcare utilization. The World Health Organization estimates that approximately 50% of patients with chronic conditions are non-adherent, underscoring the need for effective adherence support strategies.1–4 Improving medication adherence may yield greater benefits than many current medical interventions.1,3,4 National policies emphasize the importance of digital innovations that promote self-management and reduce unnecessary healthcare utilization.5
Medication non-adherence also affects the conduct and interpretation of clinical research, as protocol deviations related to medication use can bias trial outcomes.2,6 However, accurate adherence measurement remains challenging. Traditional methods such as pill counts and self-reports are prone to recall bias and overestimation, while patients often receive limited feedback on their adherence behavior.2,7–10
Digital health technologies offer novel opportunities to monitor and support medication adherence.11–13 Electronic medication packaging systems, including smart blister packs, can record medication-taking events but often lack integration with mobile applications that provide real-time feedback and self-management support.14–16
Previous research shows that blister-based packaging interventions can improve medication adherence across chronic conditions, although effects vary by population and intervention complexity.2,9 Studies of smart blister packaging generally report good usability and acceptability, including among older adults, while also identifying design-related challenges requiring further optimization.5–8 Electronic blister monitoring has additionally been shown to provide a more objective and conservative estimate of medication-taking behavior than self-report.10
Despite these promising findings, most smart blister systems have been evaluated in observational or feasibility studies. Evidence from randomized controlled trials, particularly those comparing use with and without mobile app support, remains limited.10,17–21 Therefore, studies that use a randomized controlled trial design to compare smart blister packaging with and without mobile app support are required to fill this gap in evidence.
In this study, we aimed to evaluate the usability and feasibility of a novel smart blister pack, with and without mobile app support, using quantitative usability scores, adherence measures, and qualitative user feedback. Because this study focused on usability and feasibility rather than clinical effectiveness, it was conducted in a healthy adult population, a common approach in early-phase usability research to enable controlled evaluation of user–technology interaction and avoid exposing a clinical population to a suboptimal device.
Methods
Study Design
This two-arm randomized controlled trial (RCT) evaluated the usability and feasibility of a smart blister pack, with and without a mobile medication adherence app. Participants were randomly assigned to either the intervention group (smart blister pack + app) or the control group (smart blister pack only). Blinding was not feasible due to app installation and instruction requirements. The study followed the FDA and Digital Medicine Society’s Verification, Analytical Validation, and Clinical Validation (DiMe) V3 framework.22,23
Participants
Participants were recruited in February-March of 2024 in the Netherlands through convenience sampling across healthcare, academic, and community settings. Eligible participants were at least 18 years old, English literate, and generally healthy. Chronic conditions or medication use were allowed if participants were clinically stable. Clinical stability was defined as no self-reported acute exacerbations, hospital admissions, or major changes in chronic medication regimen over the last year. All required a compatible smartphone (Android 8+ or iPhone 7+ with iOS 13+). Participants with diverse demographics were actively recruited for FDA recommendations.22
Randomization
Participants were stratified by age and prior chronic medication use and randomized 1:1 using REDCap (version 15.0.15).
Intervention and Procedures
The smart blister pack technology used (Cerepak®) integrates an inner electronically fitted drug blister card component with an outer paperboard component. The system uses a 28-unit format to log blister openings and, when combined with a mobile app (MEMS® Mobile), allows reminder delivery and manual correction of dosing events, and support of self-management.
Participants in the intervention group used the application, which provided scheduled intake reminders via smartphone push notifications (snoozing or repeated reminder alerts were not enabled) and access to a calendar-based medication history. Users had access to a medication history screen displaying date- and time-stamped blister opening events in a calendar overview and could manually edit dosing events in case of missed or duplicate recordings. Control participants used the smart blister pack without app access.
Participants received four 28-unit smart blister packs containing placebo tablets and were instructed to expel one tablet twice daily for eight weeks without ingestion, discarding tablets immediately after removal. Tablet use was unsupervised to simulate real-world medication handling. This procedure was explained verbally and in written instructions at baseline to ensure consistent execution across participants. After eight weeks, participants completed usability questionnaires and a semi-structured interview. Study materials are provided in Supplementary Material A. The end-of-study questionnaires are provided in Supplementary materials A1–A4 (Figure S1–S4), and the semi-structured interview questions are presented in Supplementary materials A5 and A6. Figures 1A and B illustrate the smart blister pack, and Figures 2A and B show the mobile app interface.
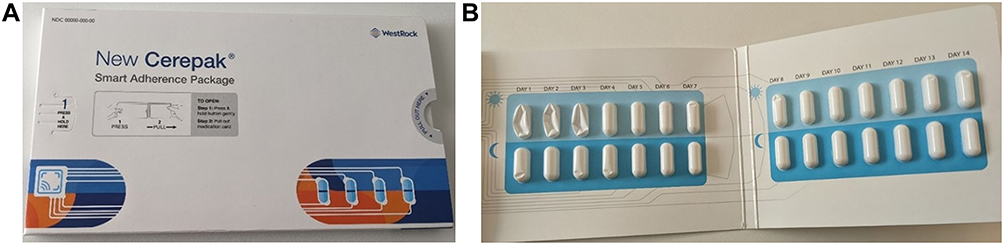 |
Figure 1 Smart blister packaging. (A) Exterior of the smart blister package and (B) Interior of the smart blister package showing the medication blisters. Pictures are used with permission from Westrock Healthcare Packaging (Atlanta, US) and AARDEX Group (Belgium). |
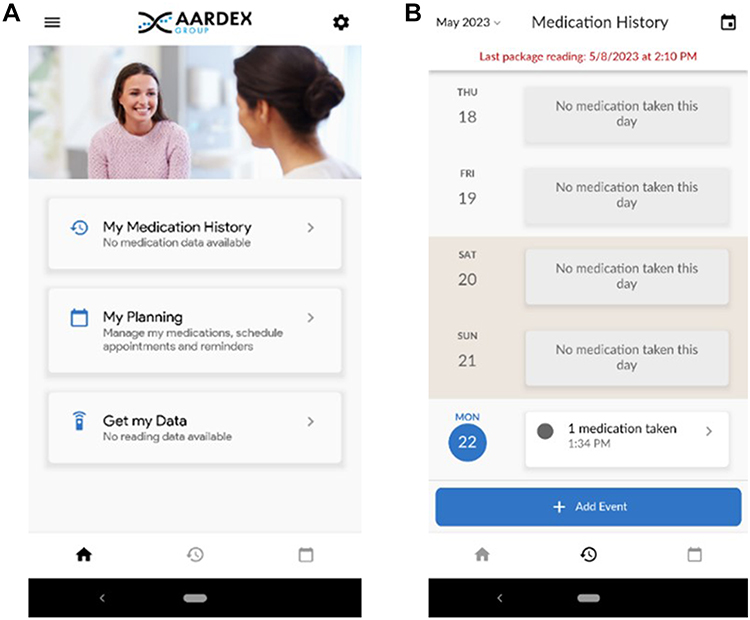 |
Figure 2 Adherence monitoring smartphone application. (A) Home screen of the adherence monitoring smartphone application. (B) Medication history overview in the adherence monitoring smartphone application. Pictures are used with permission from Westrock Healthcare Packaging (Atlanta, US) and AARDEX Group (Belgium). |
Outcome Measures
The primary outcome was usability, assessed using the System Usability Scale (SUS; score range 0–100).24 Additional Likert-scale items assessed user satisfaction. Semi-structured interviews explored user experiences, barriers, and suggestions for improvement.
Medication adherence was a secondary outcome, assessed electronically and manually. Electronic adherence was defined as the proportion of study days with two recorded blister openings. Electronic adherence data were reviewed for technical irregularities, including confirmed packaging damage or persistent connectivity failures that resulted in missed recordings. A technical malfunction was defined as a failure to record blister opening events due to such issues. Days affected by confirmed technical malfunctions were excluded from adherence calculations to prevent misclassification of participant behavior; no imputation methods were applied. Adjudication of technical issues was performed prior to analysis and was not influenced by study group allocation. All adjustments were applied consistently across both study arms. Manual adherence was assessed via end-of-study pill counts, corrected for returned medication and participant-reported deviations.
Sample Size
Thirty-six participants were aimed for, meeting the target range of 30–40, based on prior evidence that 15–20 users identify ~98% of usability issues.25
Statistical Analysis
Descriptive statistics summarized participant characteristics, usability scores, and adherence outcomes. Between-group comparisons used Mann–Whitney U or t-tests for continuous variables and chi-square or Fisher’s exact tests for categorical variables. Post-hoc exploratory subgroup analyses were conducted using non-parametric tests. Statistical significance was set at p < 0.05. Analyses were performed in R (version 4.4.1).
Interview transcripts were thematically analyzed using an inductive approach. Coding was performed in Atlas.ti (version 25) and iteratively discussed within the research team to ensure analytical rigor.
Ethics
The Medical Ethics Review Board of the University Medical Center Groningen (METc UMCG; reference number 2023/163) reviewed the study and determined that it did not fall under the Dutch Medical Research Involving Human Subjects Act (WMO), as no health-related interventions or risks were involved and only healthy volunteers participated. Therefore, formal medical ethics approval and prospective trial registration were not legally required.
For transparency, the study was voluntarily registered at ClinicalTrials.gov (NCT07099612). Written informed consent was obtained from all participants before the initiation of the study. The study was conducted in accordance with the Declaration of Helsinki and the EU General Data Protection Regulation (GDPR).
Results
Study Population
A total of 36 participants were randomized. Due to a system-related irregularity during the final allocation step, the resulting group sizes were slightly imbalanced (19 intervention vs 17 control participants), despite the intended 1:1 randomization ratio. The allocation sequence remained random and was not influenced by researchers. One control participant dropped out after three days and was excluded from follow-up analyses. Baseline characteristics were balanced, with a median age of 41.5 years, a female proportion of 63.9%, and 50% reporting prior chronic medication use (Table 1).
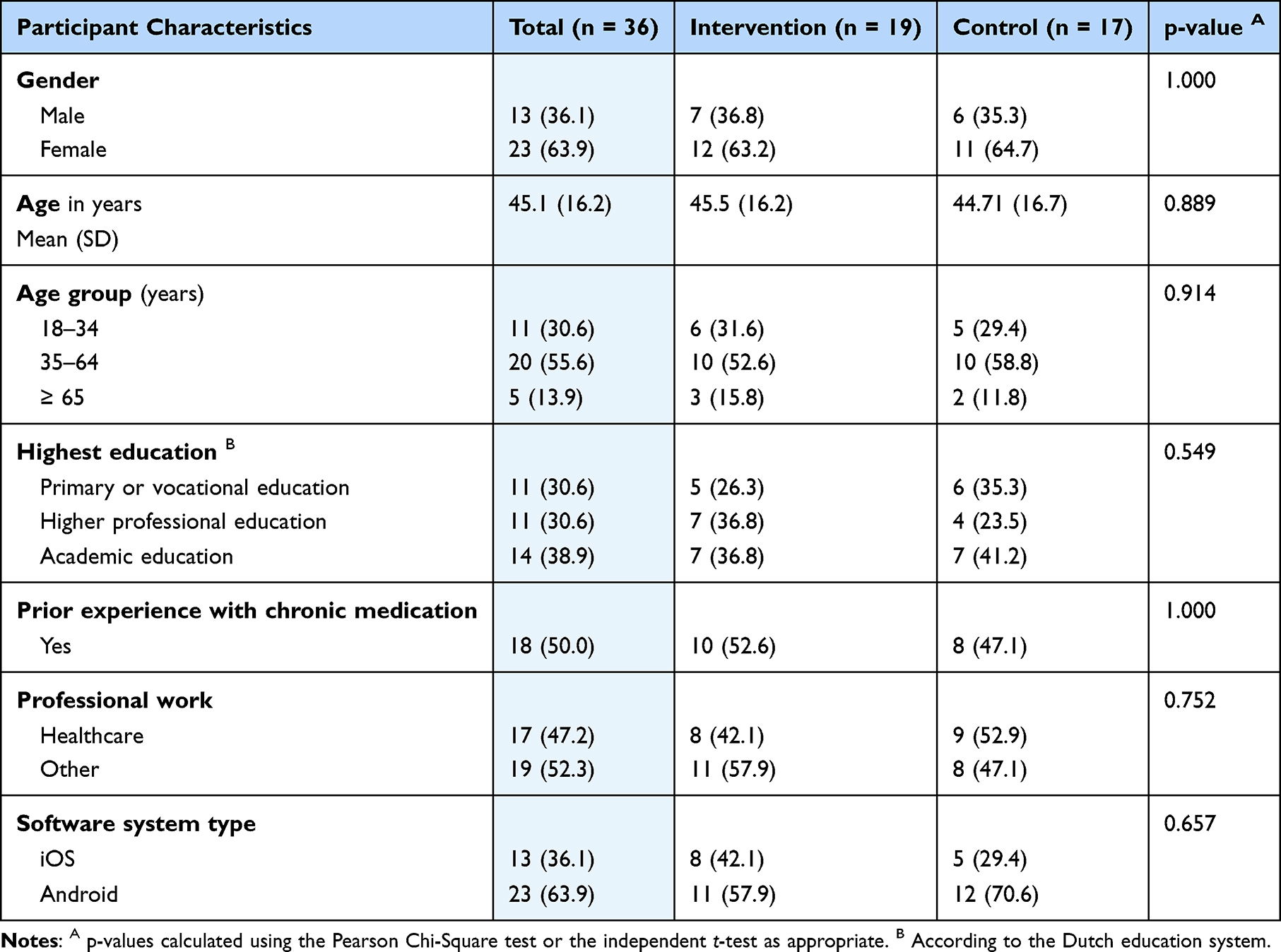 |
Table 1 Baseline Characteristics of Study Participants, Overall and by Study Arm. All Values are Presented as Numbers (Percentages) Unless Otherwise Indicated |
Usability
Both study arms completed the SUS. The intervention group evaluated the smart blister pack used with the mobile medication adherence app, reporting a median score of 80.0 [IQR 73.8–82.5], indicating good to excellent usability. Usability scores were significantly higher in the intervention group compared to the control group (p = 0.0007). The control group assessed the smart blister pack without the app, scoring a median of 67.5 [IQR 55.0–70.6], which reflects average usability. Figure 3 presents the comparative usability outcomes from the SUS, offering a visual summary of overall participant ratings. While Figure 3 summarizes overall usability scores, Figures S5 and S6 (in Supplementary Material B) present the item-level distribution of responses to the SUS questions for the intervention and control groups, respectively. Item-level responses that detail specific aspects, such as ease of use and integration, are visualized in Supplementary Material B.
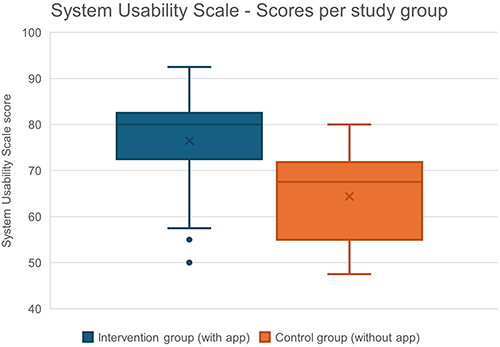 |
Figure 3 System Usability Scale (SUS) scores for the intervention group (with app) and control group (without app). |
Subgroup Analysis
Subgroup analyses were conducted on an exploratory, post hoc basis and were not powered for between-subgroup comparisons. Within the control group (n=16), female participants rated the usability of the smart blister pack used without the app lower than male participants (median SUS: 62.5 vs 72.5; p = 0.017). Given the small sample size and multiple subgroup comparisons, this finding should be interpreted cautiously as a hypothesis-generating result. No other subgroup differences were observed (see Supplementary Material C: Table S1).
User Experience and Thematic Analysis of Semi-Structured Interviews
To explore user experience in depth, we performed a thematic analysis of the interviews and integrated relevant user satisfaction data. This resulted in six overarching themes: usability and technology, technical obstacles, structure and routine, motivation and positive experience, suggestions for improvement, and physical challenges with packaging.
Usability & Technology
Participants in both groups reported high satisfaction with the smart blister pack. Nearly all found the printed instructions clear and appreciated the calendared blister card layout printed with sun and moon icons (Figure 1B), which supported dose tracking and daily structure. Some recommended replacing generic “Day 1–7” labeling with actual weekdays (eg, “Monday”) for better alignment with routines. Participants in the intervention group generally found the mobile adherence app intuitive and easy to use. This aligns with the quantitative finding that 84.2% of users rated the interface as easy to use, and 73.7% reported that it met their expectations (based on the additional questionnaire, Supplementary Material A, Figure S3). Some participants suggested including a short onboarding video in the app to further improve accessibility.
Technical Obstacles
Despite overall positive experiences, users reported technical issues with a proportion of packages (10.4%), including delayed scan recognition and difficulties with NFC connectivity. Feedback was provided after scanning, but occasional delays led some users to double-scan out of uncertainty, which raised concerns about duplicate entries. In total, 31.6% of users manually edited at least one dosing event (178 edits in total, accounting for 5.1% of all entries), primarily to correct missed or duplicate scans or to reflect pocket dosing (ie, when patients take their medication out of its packaging to keep in a pocket or bag for later use, which may prevent the dose from being registered at the actual intake moment). This helps contextualize the prevalence of manual edits observed in the quantitative adherence data.
Structure & Routine
Many participants in both the control and intervention arms reported that using the smart blister pack, particularly when paired with the mobile adherence app, helped establish a daily rhythm. Users described the act of scanning and taking the mock medication as a “task” or even a “ritual”, which provided structure and reinforced routine behavior. This was especially appreciated by individuals without prior experience with regular medication use.
Motivation & Positive Experience
Several users from the intervention group described the app as a “silent coach” that subtly encouraged adherence without being intrusive. Even though the medication was a placebo, participants reported feeling accountable and motivated to maintain the routine. This sense of involvement and “doing something good” was particularly strong among digitally engaged users. App usage patterns varied: while some participants explored nearly all features, others used the system more selectively, relying primarily on reminders and visual dose tracking.
Suggestions for Improvement
Participants in the intervention arm noted that while the scanning function was accessible from the home screen, certain actions required multiple steps within the app. They suggested that a redesigned home screen with more direct access to key features could improve usability. Additionally, participants expressed interest in enhanced motivational feedback to support adherence. Some also requested a more flexible way to log missed doses, to avoid being penalized for technical issues or accidental omissions.
Physical Challenges with Packaging
A recurring barrier was the stiffness of the inner blister card component of the smart blister pack. Older participants and those with reduced hand strength (eg, due to tremors or arthritis) reported difficulties pressing out tablets. Recommendations included softer materials, larger Child Resistance/Senior Friendly (CR/SF) opening button pressure zones, and a more ergonomic design. For mobility, some users suggested a slimmer or more portable format. Sustainability was also a concern, with several participants advocating for eco-friendly or reusable packaging options.
These themes reflect a generally positive but nuanced user experience, highlighting both the potential and the areas for optimization of this early-phase digital health innovation.
Medication Adherence
After excluding days affected by confirmed technical malfunctions, electronically measured adherence was 91.7% in the intervention group and 86.1% in the control group (p = 0.1835). Manual pill counts showed median adherence of 96.4% in the intervention group and 88.0% in the control group (p = 0.0666; Table 2). No statistically significant differences in adherence were observed between study arms.
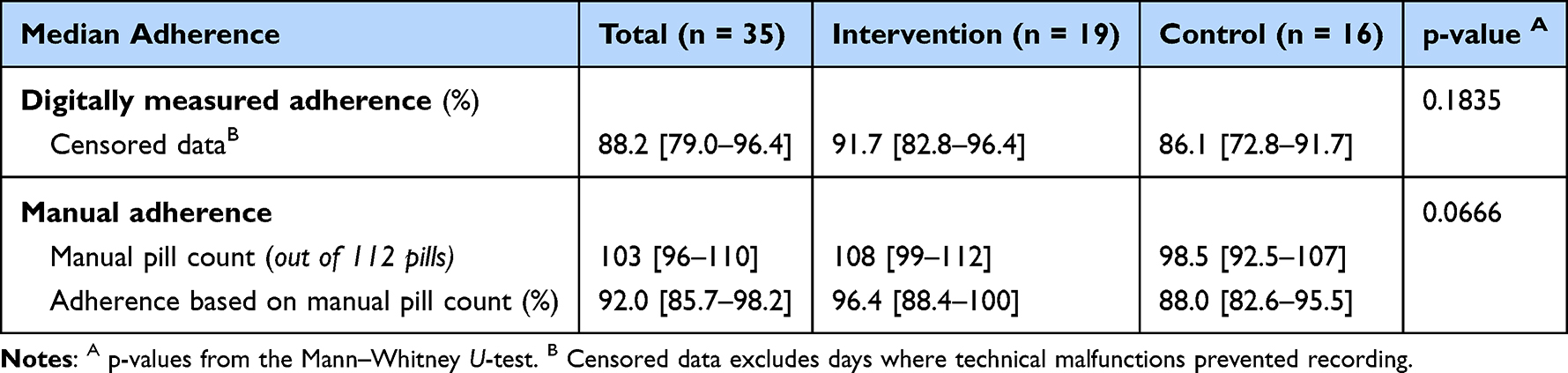 |
Table 2 Median Adherence Measured by Electronic Monitoring and Manual Pill Count, Overall and by Study Arm. Values are Presented as Median [Interquartile Range], Unless Otherwise Noted |
Discussion
This study evaluated the usability and feasibility of a smart blister pack, both with and without a mobile adherence app, in a healthy adult population. Overall usability was rated positively in both study arms, with significantly higher usability scores observed in the app-supported group. No statistically significant differences in adherence outcomes were detected. Qualitative findings provided important context for these results by elucidating user experiences, perceived benefits, and technical barriers.
Participants described the smart blister pack as intuitive and easy to integrate into daily routines. While the standalone smart blister pack provided structure, the addition of the mobile adherence app was particularly valued for offering reminders, feedback, and engagement. These findings align with prior research demonstrating that simple, visually intuitive, and user-centered digital adherence technologies can enhance user satisfaction and support medication routines.10,26,27 The visual design of the smart blister pack, particularly the calendar layout featuring sun/moon icons, was appreciated for promoting daily structure, aligning with earlier evidence on the role of visual cues in adherence behavior.10
The mobile application was generally well-received, with users reporting that reminders and dose history visualization improved awareness of medication intake. Engagement with optional features varied, which is consistent with previous research indicating that sustained use of mHealth tools depends on perceived usefulness and personalization.18,28,29 Suggestions for interface improvement further underline the importance of user-centered designs in tailoring digital adherence tools to user preferences.13,28
Exploratory subgroup analyses suggested lower usability ratings among female participants in the control group compared with males. Given the small subgroup sizes, this post hoc finding should be interpreted with extreme caution and considered hypothesis-generating only. Nonetheless, it is consistent with prior studies reporting gender differences in perceived ease of use and confidence with digital health technologies.30 Importantly, this difference was not observed in the app-supported group.30,31
The system demonstrated good feasibility for unsupervised daily use. Most participants incorporated scanning into their routines with minimal effort, and technical issues were infrequent and generally resolved independently. These findings support the practicality of implementing smart blister systems outside clinical settings and are consistent with previous research on digital adherence technologies designed for real-world use.26,32,33 Interestingly, even participants in the control group expressed interest in app-based features after learning about them, suggesting broader receptiveness to digital adherence support when tools are intuitive and well integrated.12
Participant feedback identified several opportunities for system optimization, particularly regarding physical aspects of the blister pack, clarity of labeling, and visibility of key app functions. Difficulties expelling tablets, preferences for weekday-aligned labeling, and interest in more prominent app navigation features were recurrent themes. Sustainability considerations, including interest in reusable or eco-friendly packaging, further emphasize the importance of incorporating user feedback into future hardware and software refinements.
Strengths and Limitations
This study has several strengths. First, the mixed-methods approach, which combines usability scores, objective adherence data, and qualitative feedback, provided a well-rounded understanding of user experience and system performance.34 Second, by including both an app-supported and a standalone version of the smart blister pack, we were able to assess the added value of digital support. The use of electronic monitoring alongside manual pill counts also allowed for internal validation of adherence outcomes. Notably, adherence percentages derived from manual pill counts were higher than those measured by smart packaging. This difference can be explained by the fact that electronic monitoring accounts for the exact date and time of pill intake, thereby assessing whether patients adhered to the prescribed dosing regimen (eg, taking one pill twice daily). In contrast, manual pill counting was conducted retrospectively, which means that, at least hypothetically, participants could have expelled multiple pills at once. While this would still appear as full adherence in a manual count, it does not necessarily reflect true adherence to the prescribed dosing schedule.
However, several limitations should be acknowledged. This study was conducted in a healthy, motivated adult population, which may limit the generalizability of findings to clinical populations. Participants were generally well-functioning, digitally literate, and willing to engage with adherence technologies, which may lead to higher usability and adherence scores compared to patients with chronic conditions, cognitive impairments, or limited digital access.35 Convenience sampling may also have affected representativeness, despite efforts to include participants with diverse backgrounds.36 Secondly, the modest sample size limited statistical power to detect small adherence differences, and the 8-week duration precluded evaluation of long-term engagement, alert fatigue, and sustainability. Finally, although technical performance was generally reliable, occasional malfunctions indicate the need for further hardware optimization.
Implications for Future Research and Practice
These findings demonstrate that smart blister packaging is usable and feasible for short-term, unsupervised medication handling, particularly when combined with mobile app support. App-based reminders, feedback, and visualization appear to enhance engagement and perceived usability. Future studies should evaluate smart blister systems in clinical populations, with longer follow-up and sufficient power to assess sustained use, adherence outcomes, and real-world effectiveness. User feedback should continue to inform iterative refinement of both packaging and app design prior to large-scale implementation.
Conclusion
This study demonstrated that a smart blister package is usable and feasible for short-term medication handling in healthy adults, with higher usability observed when combined with mobile app support. Although no significant differences in adherence were found, qualitative findings highlighted user experiences, technical barriers, and features that may support engagement with medication routines.
These findings suggest that smart blister packaging, particularly when paired with a mobile application, has potential as a user-friendly adherence support tool. Further research in clinical populations with longer follow-up is needed to assess real-world effectiveness and inform optimization for diverse user needs.
Data Sharing Statement
Individual de-identified participant data underlying the results reported in this article will be available from the corresponding author upon reasonable request. The data to be shared include anonymized quantitative study data (eg, usability scores and adherence measures). Additional study documents, including the study protocol and statistical analysis code, will be made available upon request.
Data will be shared for academic research purposes, subject to approval of a methodologically sound proposal and execution of a data sharing agreement. Requests should be directed to the corresponding author, Dr Job F M Van Boven ([email protected]). Data will be available beginning 3 months after publication and for a period of 5 years.
Acknowledgments
We want to thank the study participants for their time and valuable feedback.
Funding
This study was financially supported by AARDEX Group, which provided a financial contribution to the University Medical Center Groningen (UMCG). Smurfit WestRock provided the smart blister packages used in the study, and AARDEX Group provided access to the digital adherence software. The funders had no role in the study design, data collection, data analysis, data interpretation, or the decision to submit the manuscript for publication.
Disclosure
Dr Amy Chan reports grants from Health Research Council, grants from Auckland Medical Research Foundation, grants from CMDT Med Tech, outside the submitted work; and Clinical Director - Asthma NZ.
Chair - REG adherence working group.
ERS CONNECT CRC - working group lead.
Dr Job Van Boven reports grants from Aardex, during the conduct of the study; grants, personal fees from Aardex, ALK, AstraZeneca, Chiesi, European Commission, COST (COST Action 19132), GSK, Novartis, Pfizer, Pill Connect, Sanofi, Teva, Trudell Medical, Vertex, outside the submitted work, and paid to his employer, the UMCG. The authors declare that this study received financial and in-kind support as described in the Funding section.
The UMCG has received several other grants and/or consultancy fees from other companies (AstraZeneca, Chiesi, Novartis, Sanofi, Pfizer, Pill Connect, Teva, Trudell Medical and Vertex) to provide advice and/or perform research studies with digital adherence technologies. The authors report no other conflicts of interest in this work.
References
1. World Health Organization. Adherence to Long-Term Therapies: evidence for Action; 2003. Available from: https://iris.who.int/handle/10665/42682.
2. Blaschke TF, Osterberg L, Vrijens B, Urquhart J. Adherence to medications: insights arising from studies on the unreliable link between prescribed and actual drug dosing histories. Annu Rev Pharmacol Toxicol. 2012;52(1):275–10. doi:10.1146/annurev-pharmtox-011711-113247
3. Cutler RL, Fernandez-Llimos F, Frommer M, Benrimoj SI, Garcia-Cardenas V. Economic Impact of Medication Nonadherence by Disease Groups: A Systematic Review Authors. 2018.
4. van Boven JFM, Lavorini F, Agh T, Sadatsafavi M, Patino O, Muresan B. Cost-effectiveness and impact on health care utilization of interventions to improve medication adherence and outcomes in asthma and chronic obstructive pulmonary disease: a systematic literature review. J Allergy Clin Immunol Pract. 2024;12(5):1228–1243. doi:10.1016/j.jaip.2023.12.049
5. Government of the Netherlands. More sustainability in the health and care sector. Ministry of Health Welfare and Sport. March 2023. Available from: https://www.government.nl/topics/sustainable-healthcare/more-sustainability-in-the-care-sector.
6. Davis C, Abraham J. Unhealthy Pharmaceutical Regulation. Palgrave Macmillan UK; 2013. Available from: https://www.perlego.com/book/3486190/unhealthy-pharmaceutical-regulation-innovation-politics-and-promissory-science-pdf.
7. Dima AL, Dediu D. Computation of adherence to medication and visualization of medication histories in R with AdhereR: towards transparent and reproducible use of electronic healthcare data. PLoS One. 2017;12(4). doi:10.1371/journal.pone.0174426
8. Vrijens B, Urquhart J. Patient adherence to prescribed antimicrobial drug dosing regimens. J Antimicrob Chemother. 2005;55(5):616–627. doi:10.1093/jac/dki066
9. Mantila KM, Pasmooij AMG, Hallgreen CE, mol PGM, van Boven JFM. Medication adherence measurement methods in registration trials supporting the approval of new medicines: a cross-sectional analysis of centralized procedures in the european union 2010–2020. Clin Pharmacol Ther. 2022;112(5):1051–1060. doi:10.1002/cpt.2709
10. Izzah Z, Zijp TR, Åberg C, Touw DJ, van Boven JF. Electronic smart blister packages to monitor and support medication adherence: a usability study. Patient Prefer Adherence. 2022;16:2543–2558. doi:10.2147/PPA.S374685
11. van Boven JFM, Dima AL, Wettermark B, Potocnjak I, Ágh T. Leveraging Digital Medication Adherence Technologies to Enhance Sustainability of European Health Systems: ENABLE’s Key Recommendations. Vol. 105. 2018. doi:10.1787/8178962c-en
12. Chan AHY, Reddel HK, Apter A, Eakin M, Riekert K, Foster JM. Adherence monitoring and E-health: how clinicians and researchers can use technology to promote inhaler adherence for asthma. J Allergy Clin Immunol Pract. 2013;1(5):446–454. doi:10.1016/j.jaip.2013.06.015
13. Marcolino MS, Oliveira JAQ, D’Agostino M, Ribeiro AL, Alkmim MBM, Novillo-Ortiz D. The impact of mhealth interventions: systematic review of systematic reviews. JMIR mHealth uHealth. 2018;6(1). doi:10.2196/mhealth.8873
14. Cramer JA, Scheyer RD, Mattson RH. Compliance declines between clinic visits. Arch Intern Med. 1990;150(7):1509–1510.
15. Vrijens B, Urquhart J. Methods for measuring, enhancing, and accounting for medication adherence in clinical trials. Clin Pharmacol Ther. 2014;95(6):617–626. doi:10.1038/clpt.2014.59
16. Arnet I, Walter PN, Hersberger KE. Polymedication Electronic Monitoring System (POEMS) – a new technology for measuring adherence. Front Pharmacol. 2013;4. doi:10.3389/fphar.2013.00026
17. Zullig LL, Blalock D, Dougherty S, et al. The new landscape of medication adherence improvement: where population health science meets precision medicine. Patient Prefer Adherence. 2018;12:1225–1230. doi:10.2147/PPA.S165404
18. Zijp T, Touw D, van Boven J. User acceptability and technical robustness evaluation of a novel smart pill bottle prototype designed to support medication adherence. Patient Prefer Adherence. 2020;14:625–634. doi:10.2147/PPA.S240443
19. Ghimire S, Iskandar D, van der Borg-Boekhout R, et al. Combining digital adherence technology and therapeutic drug monitoring for personalised tuberculosis care. Eur Resp J Eur Resp Soc. 2022;60(6). doi:10.1183/13993003.01690-2022
20. Chan AHY, De Keyser HH, Horne R, Szefler SJ. Viewpoint: defining adherence phenotype and endotypes to personalise asthma management. Eur Resp J Eur Resp Soc. 2025;65(1). doi:10.1183/13993003.01357-2024
21. Chan AHY, Foot H, Pearce CJ, Horne R, Foster JM, Harrison J. Effect of electronic adherence monitoring on adherence and outcomes in chronic conditions: a systematic review and meta-analysis. PLoS One. 2022;17(3):e0265715. doi:10.1371/journal.pone.0265715
22. U.S. Food and Drug Administration. Digital Health Technologies for Remote Data Acquisition in Clinical Investigations: guidance for Industry, Investigators, and Other Stakeholders. January 2023. Available from: https://www.fda.gov/media/155022/download.
23. Goldsack JC, Coravos A, Bakker JP, et al. Verification, analytical validation, and clinical validation (V3): the foundation of determining fit-for-purpose for Biometric Monitoring Technologies (BioMeTs). NPJ Digit Med. 2020;3(1):55. doi:10.1038/s41746-020-0260-4
24. Lewis JR. The system usability scale: past, present, and future. Int J Hum Comput Interact. 2018;34(7):577–590. doi:10.1080/10447318.2018.1455307
25. Nielsen J, Landauer TK. A Mathematical Model of the Finding of Usability Problems. In: Association for Computing Machinery; 1993:206–213. doi:10.1145/169059.169166
26. Vrijens B, De Geest S, Hughes DA, et al. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol. 2012;73(5):691–705. doi:10.1111/j.1365-2125.2012.04167.x
27. Baumgartner SL, Buffkin JDE, Rukavina E, Jones J, Weiler E, Carnes TC. A novel digital pill system for medication adherence measurement and reporting: usability validation study. JMIR Hum Factors. 2021;8(4):e30786. doi:10.2196/30786
28. Kumar S, Nilsen WJ, Abernethy A, et al. Mobile health technology evaluation. Am J Prev Med. 2013;45(2):228–236. doi:10.1016/j.amepre.2013.03.017
29. Thakkar J, Kurup R, Laba TL, et al. Mobile telephone text messaging for medication adherence in chronic disease. JAMA Intern Med. 2016;176(3):340. doi:10.1001/jamainternmed.2015.7667
30. van Elburg FRT, Klaver NS, Nieboer AP, Askari M. Gender differences regarding intention to use mHealth applications in the Dutch elderly population: a cross-sectional study. BMC Geriatr. 2022;22(1):449. doi:10.1186/s12877-022-03130-3
31. Luo Y, Mou J. Understanding gender differences in mHealth apps continuance: a modified protection motivation theory. J Electr Bus Dig Econ. 2022;1(1/2):225–247. doi:10.1108/JEBDE-09-2022-0032
32. Faisal S, Samoth D, Aslam Y, et al. Key features of smart medication adherence products: updated scoping review. JMIR Aging. 2023:6:e50990. 10.2196/50990.
33. Mason M, Cho Y, Rayo J, Gong Y, Harris M, Jiang Y. Technologies for medication adherence monitoring and technology assessment criteria: narrative review. JMIR mHealth uHealth. 2022;10(3):e35157. doi:10.2196/35157
34. Creswell JW, Plano Clark VL. Designing and Conducting Mixed Methods Research. SAGE Publications, Inc; 2017.
35. Kardas P, Lewek P, Matyjaszczyk M. Determinants of patient adherence: a review of systematic reviews. Front Pharmacol. 2013;4. doi:10.3389/fphar.2013.00091
36. Manton KJ, Gauld CS, White KM, Griffin PM, Elliott SL. Qualitative study investigating the underlying motivations of healthy participants in Phase I clinical trials. BMJ Open. 2019;9(1):e024224. doi:10.1136/bmjopen-2018-024224
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.