Back to Journals » Research and Reports in Urology » Volume 12
Small Ureteral Access Sheath in Treating Paediatric Urolithiasis: A Single Centre Experience
Authors Aljumaiah S, Allubly N, Alshammari A, Alkhamees M ![]() , Bin Hamri S
, Bin Hamri S
Received 24 August 2020
Accepted for publication 30 November 2020
Published 22 December 2020 Volume 2020:12 Pages 663—668
DOI https://doi.org/10.2147/RRU.S277855
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jan Colli
Sahar Aljumaiah,1,2 Nasser Allubly,3 Ahmad Alshammari,1,2,4 Mohammad Alkhamees,5 Saeed Bin Hamri1,2,4
1Division of Urology, Department of Surgery, Ministry of the National Guard – Health Affairs, Riyadh, Saudi Arabia; 2King Abdullah International Medical Research Center (KAIMRC), Riyadh 11426, Saudi Arabia; 3Department of Urology, Department of Surgery, King Fahad Hufof Hospital, Al-Ahsa, Saudi Arabia; 4College of Medicine, King Saud Bin Abdulaziz University for Health Sciences (KSAU-HS), Riyadh 11426, Saudi Arabia; 5Department of Urology, College of Medicine, Majmaah University, Al-Majmaah, Saudi Arabia
Correspondence: Sahar Aljumaiah
Division of Urology, Department of Surgery, Ministry of the National Guard – Health Affairs, Riyadh, Saudi Arabia
Tel +966-551763208
Email [email protected]
Introduction: Urolithiasis is not commonly encountered in the pediatric population. The adoption of ureteral access sheaths (UAS) facilitates the passage to the pediatric ureter and limits the harm and ureteral injury. However, the debate continues regarding whether or not to use UAS in children.
Objective: To assess the safety and outcomes of using UAS in the treatment of pediatric renal and ureteral stones.
Study Design: This was a prospective cohort study of 14 pediatric patients who underwent flexible ureteroscopy (fURS) with the use of UAS for symptomatic renal and ureteric stones.
Results: Of the fourteen enrolled patients, nine (64.3%) were males, and five (35.7%) were females with an average age of 9.5 years. Eleven (78.6%) of the patients were rendered stone-free. The average operative time was 55.7 min. None of the patients developed any complications. The stone-free rate was significantly higher with stone burdens of ≤ 10 mm (p ≤ 0.05).
Conclusion: The use of UAS in children facilitates the passage of a flexible ureteroscope without complications. The procedure is considered to be efficient and safe with minimal morbidity.
Keywords: urolithiasis, UAS, urethral access sheath, pediatric
Introduction
Urolithiasis is not commonly encountered in the pediatric population in which it accounts for only 3% of all stone populations. That being said, the incidence of pediatric urolithiasis has been noted to have increased recently.1 Although the therapeutic approaches for urolithiasis in children are similar to those used in adults, a limited amount of management experience is available.1,2 The available options include extracorporeal shock wave lithotripsy (ESWL), retrograde intra-renal surgery (RIRS), and percutaneous nephrolithotomy (PCNL), and the choice of the most appropriate approach depends on several factors, including patients-related factors, stone factors, and the urologist’s preference.1
ESWL used to be superior to any endourological approach since compared to other available options, it was less invasive with fewer complications and almost the same stone-free rate.3 The success rate of ESWL, however, depends on the stone site, stone burden, and congenital anomalies. ESWL may also require multiple treatment sessions, including potential radiation exposure.3
Introducing endoscopic modalities for the removal of renal stones used to be of great concern because of the small caliber of the pediatric ureter and its fragility, which predisposes it to urethral perforations, strictures, and subsequent vesicoureteral reflux (VUR). However, nowadays, miniaturization in instrumentation, in addition to the evident improvements in endoscopic techniques, have made this technique a safe, feasible, and a less problematic option for treating children.2,4,5
The adoption of urethral access sheaths (UAS) facilitates the passage to the pediatric ureter and reduced the risk of ureteral injury.2,5 However, the debate continues as to whether or not to use UAS in children.3 In fact, little data have shown solid evidence for the use of UAS in the pediatric population. Therefore, we conducted the current investigation to report our single-center experience in order to shed light on the characteristics of using UAS, in terms of safety and outcomes, for treating pediatric urolithiasis. To the best of our knowledge, this is the first report on this topic in the Gulf countries.
Patients and Methods
This prospective cohort study was conducted in accordance with the Declaration of Helsinki on a sample of 14 patients who underwent flexible ureteroscopy (fURS) for symptomatic renal and ureteric stones between March 2018 and December 2019 at King Abdullah Specialist Children’s Hospital, Riyadh, Saudi Arabia. The study included all pediatric patients who underwent fURS with the use of UAS during the study period with no pre-specified exclusion criteria. Prior to conducting this research, our proposal was accepted by the Ethics Committee/Institutional Review Board (IRB) of King Abdullah Specialist Children’s Hospital. The parents and/or the guardians of eligible children signed informed consent prior to their participation in our study.
We reviewed patients’ file, and baseline demographic characteristics of included patients in addition to their previous medical and surgical histories were collected, including previous ESWL, URS, PCNL, or open surgeries. Renal ultrasound and plain kidney, ureter, and bladder (KUB) X-ray were used for preoperative assessment of the stone site and stone burden (using the measurement of the longest diameter) in addition to assessing any associated hydronephrosis or other congenital anomalies. Data regarding operative time, complications, and any additional sessions that were required were also recorded.
UAS (10/12Fr, 35 cm) Biflex® were used in all procedures for active dilatation. Flexible endoscopes (Flex X2 Storz®, Flex XC Storz®, and URF-P5 Olympus®) were used in these surgeries. Fragmentation of the calculi was done with a Holmium: YAG laser, while the calculi were extracted using Rocamed or Coloplast Baskets (Figure 1). All patients had Double-J stents inserted at the conclusion of the procedure. All procedures were carried out by the same surgeon, and all interventions were done at the discretion of the operating interventionist. The follow-up time was determined as the time between the date of surgery and the most recent visit to the clinic. Follow-up was done with renal ultrasound imaging to observe the stone residual and any associated hydronephrosis.
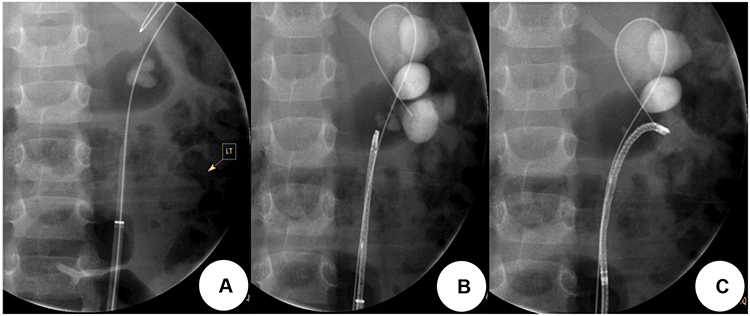 |
Figure 1 Demonstration of retrograde intra-renal surgery (RIRS) procedure steps in one of the cases of a child with a 2 cm renal stone. (A) insertion of ureteral access sheath (UAS). (B, C) insertion of the flexible ureteroscope accessing the lower pole. |
Statistical Analysis
All data were retrieved from participants and entered into a standardized Excel sheet. Complete data were then entered into Statistical Package for Social Science (SPSS-Version 23) for analysis. A simple descriptive statistic was used to define the characteristics of the study variables through counts and percentages for the categorical and nominal variables, while continuous variables were presented by mean and standard deviations. To establish a relationship between categorical variables, we used the chi-square test in this regard. A conventional p-value of <0.05 was considered the cut-off point for statistical significance.
Results
A total of 14 pediatric patients (nine males [64.3%] and five females [35.7%]) were enrolled in this study. The average age was 9.5 years (ranging from 9 months to 17 years). As per the previous relevant medical history of the patients, eight (57.2%) of the patients were either known as stone formers or had a metabolic disease related to stone formation, such as primary oxaluria, three (21.4%) had diseases that were not stone-related, such as bronchial asthma, seizures, and growth hormone deficiency, and three (21.4%) had no known diseases. Four (28.6%) of the patients had not undergone any previous surgical history, whereas five (35.7%) underwent URS, two (14.3%) underwent PCNL, and three (21.4%) had undergone surgeries, such as orchidopexy that were not related to renal stones.
Regarding stone burden, the majority of patients (57.2%) had stones of ≤10 mm, five patients (35.7%) had stone burdens ≥10 mm but ≤20 mm, and one patient (7.1%) had a stone burden ≥20 mm. In terms of stone location, five patients (35.7%) had stones in the lower calyx, four (28.6%) had stones in the renal pelvis, two (14.3%) had staghorn stones, two (14.3%) had ureteric stones, and one (7.1%) had a lower calyx stone and ureteric stone on the same side. The stone analysis showed that eight (57.1%) of the patients had calcium-based stones, and two patients (14.3%) had struvite stones, but this analysis was not done for four (28.6%) patients. All of the baseline demographic characteristics in addition to previous medical and surgical histories of included patients are summarized in Table 1.
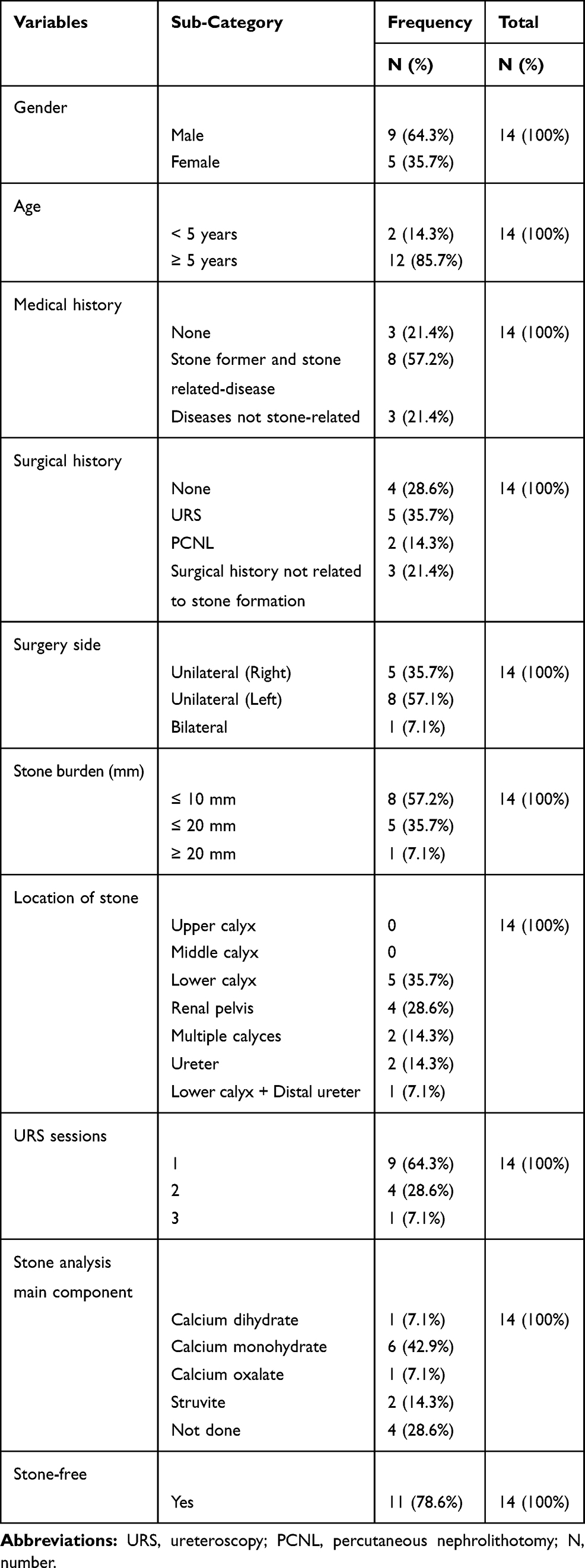 |
Table 1 Demographic Data and Medical Histories of Study Participants (N=14) |
Thirteen (92.9%) out of 14 patients underwent unilateral URS, whereas one (7.1%) patient underwent bilateral URS in the same operative setting. Nine (64.3%) patients underwent only one session of ureteroscopy, four (28.6%) required two sessions, and one (7.1%) patient required three sessions (Table 1). The average operative time was 55.7 min (range: 24 to 120 min). All patients had Double-J stents inserted at the conclusion of the procedure. The Double-J stent was removed within 14 days of the procedure in 42.8% of the patients, within 15–30 days in 28.6% of the patients, and ≥30 days after the procedure in 28.6% of the patients.
Follow-up renal ultrasound scanning was performed in 13 patients (92.9%), whereas one (7.1%) patient did not have the image taken and was lost during follow-up. The average follow-up duration was 17.3 months. The data show that 11 (78.6%) of the patients were stone-free at follow-up, whereas three (21.4%) were not. None of the patients developed any complications, such as ureteric stricture, fistula, avulsion, perforated ureter, rupture fornix, and/or perforated pelvis.
We also investigated whether baseline factors (such as stone burden and location, surgical side, operative time, and number or URS session) were associated with stone-free rate (Table 2). Among the aforementioned factors, only stone burden significantly correlated with stone-free outcome. Patients with stone burden ≤10 mm were significantly more likely to have free-stone outcome compared to patients with high stone burden (≤20 mm, p = 0.026). Similarly, the stone-free rate was observed to be higher in those who underwent unilateral surgery and a single ureteroscopic procedure. However, these differences did not reach statistical significance (P > 0.05).
 |
Table 2 Comparison Between Surgery and Stone Characteristics, and Stone-Free Rate |
Discussion
Since 1980, ESWL used to be the gold standard treatment for pediatric stone disease for stone burdens ≤2 cm and stones located at the proximal ureter with a stone-free rate of up to 95%.6 The recent American Urological Association (AUA) guidelines issued in 2016 for the treatment of pediatric patients with ureteral or renal stones strongly recommend performing URS if the observational trial and medical expulsive therapy failed or if the patient was less likely to pass the stone.7 For patients with total renal stone burdens of ≤20 mm, either ESWL or URS is considered first-line treatment. De Dominicis had randomly distributed the distal ureteral stone patients into two groups (patients received either URS or ESWL) and reported that the URS group had a 94% success rate, whereas the ESWL group had only a 43% success rate.6,8
Recent advancements in endoscopic equipment and technical improvements made the endoscopic option for pediatric stone management more applicable and efficient.6,9 In 1988, Ritchey et al first introduced an 8.5-Fr rigid URS for treating a 1-cm distal ureteral stone in a four-year-old boy and showed no residual stone and zero postoperative complications after URS.10 Multiple case series that used rigid URS for treating distal ureteral stones showed minor complications with a high stone-free rate.11,12
In our cohort study, a total of 14 pediatric patients were included of whom had undergone unilateral surgery and had a stone burden of ≤10 mm, stones located in the lower calyx, and one URS session. In terms of outcomes, the majority of our pediatric population had stone-free outcomes (11/14, 78.6%), after an average follow-up period of 17.3 weeks. No complications were noted during that follow-up period in our population. Furthermore, stone burden was the only significantly associated factor with stone-free outcome, where patients with lower stone burden had significantly higher stone-free rate compared to higher stone burden. Our findings agree with results from the study of Singh et al2 who enrolled eight pediatric patients (average age of 9.3 years) who underwent fURS with the use of UAS. The authors reported a stone-free rate of 100% in their population after a mean follow-up period of 10 months with an average overall stone burden of 9.3 mm. The patients had no intraoperative or postoperative complications during the follow-up period even though the stone-free rate was lower in our population; however, this finding could possibly be attributed to the longer follow-up period of the previous study2. As per the Claviendindo scale for complications ranking, since all patients required postoperative analgesics it considered as Clavien 1. In a similar study, Anbarasan et al13 retrospectively reviewed the data of 21 pediatric patients (mean age of 11.8 years) who underwent fURSL with the use of UAS for the treatment of pediatric renal stones. The majority of their patients had stones at the lower pole (62%) and presented with multiple stones (57%). The overall stone burden of their population was 12 mm (range 5–30 mm). The authors also reported that they had to conduct 31 procedures in order to achieve a stone-free rate of 95%. No complications were noted in the long term over a follow-up period of 37 months (mean 26 months).
Little data are available regarding ureteroscopic procedures for stone treatment in pediatric populations, but even less than that is available regarding UAS use in ureteroscopic surgeries.5 UAS are a technical invention that must facilitate a change in the current protocol.9 Therefore, in our study, we focused on its safety in accordance with the pediatric ureter. Minevich et al8 had performed ureteroscopy in 71 pediatric patients; although they did not use UAS with their patients, they believed that it would protect the ureter from damage, especially when multiple passages of the ureteroscope are expected. A study done in Boston in 2011 involved patients who underwent URS with or without UAS. Their data showed more intraoperative complications in those who underwent URS with UAS.5 Tanaka et al14 documented the use of UAS in ureteroscopic procedures for intrarenal calculi in 25 out of 50 children with no noted intraoperative or postoperative complications. Similarly, our data showed no intraoperative or postoperative complications with a stone-free rate of 78.6%, which was significantly related to stone burden of 10 mm or less.
Different results were observed when correlating the stone-free rate with the use of UAS; in another study, the stone-free rate was either higher or similar to that of patients who underwent URS without UAS.5 A five-year study done in 2007 at the Children’s Hospital of Pittsburgh reported that ureteroscopy was used in a total of 100 children and UAS were used in 47% of their cases. Their successful stone-free rate was 91%, and only six out of 100 patients had ureteral perforation or stricture without any correlation to the use of UAS.6
Even though our study provides helpful insights into the management of renal stones with the use of UAS, particularly, in a pediatric population, our study has several limitations. The most important limitation was the small sample size of included patients and the absence of a control group (no UAS) to determine if UAS was superior to non-UAS ureteroscopy. Therefore, clinical trials of larger sample sizes and longer follow-up durations are warranted in order to provide more robust evidence regarding the efficacy and safety of this procedure in treating renal stones in pediatric patients.
Conclusion
The use of UAS in children was shown to facilitate the passage of a flexible ureterorenoscope with no observed complications. The procedure is considered to be efficient and safe with minimal morbidity.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Schultz-Lampel D, Lampel A. The surgical management of stones in children. BJU Int. 2001;87(8):732–740. doi:10.1046/j.1464-410x.2001.02218.x
2. Singh A, Shah G, Young J, Sheridan M, Haas G, Upadhyay J. Ureteral access sheath for the management of pediatric renal and ureteral stones: a single center experience. J Urol. 2006;175:
3. Tekgül S. Ureteroscopy versus shock wave lithotripsy for renal calculi in children. J Urol. 2011;185(4):1188–1189. doi:10.1016/j.juro.2011.01.047
4. De Dominicis M, Matarazzo E, Capozza N, Collura G, Caione P. Retrograde ureteroscopy for distal ureteric stone removal in children. BJU Int. 2005;95(7):1049–1052. doi:10.1111/j.1464-410X.2005.05464.x
5. Wang HH, Huang L, Routh JC, Kokorowski P, Cilento BG
6. Smaldone MC, Cannon GM
7. Assimos D, Krambeck A, Miller NL, et al. Surgical management of stones: american urological association/endourological society guideline, PART I. J Urol. 2016;196:1153–1160. doi:10.1016/j.juro.2016.05.090
8. Minevich E, Defoor W, Reddy P, et al. Ureteroscopy is safe and effective in prepubertal children. J Urol. 2005;174:
9. Al-Busaidy SS, Prem AR, Medhat M, Al-Bulushi YH. Ureteric calculi in children: preliminary experience with holmium:YAG laser lithotripsy. BJU Int. 2004;93:1318–1323. doi:10.1111/j.1464-410X.2004.04864.x
10. Ritchey M, Patterson DE, Kelalis PP, Segura JW. A case of pediatric ureteroscopic lasertripsy. J Urol. 1988;139:1272–1274. doi:10.1016/S0022-5347(17)42890-4
11. Kucukdurmaz F, Efe E, Sahinkanat T, Amasyalı AS, Resim S. Ureteroscopy with holmium: YAG laser lithotripsy for ureteral stones in preschool children: analysis of the factors affecting the complications and success. Urol. 2018;111:162–167. doi:10.1016/j.urology.2017.09.006
12. Smaldone MC, Corcoran AT, Docimo SG, Ost MC. Endourological management of pediatric stone disease: present status. J Urol. 2009;181:17–28. doi:10.1016/j.juro.2008.09.001
13. Anbarasan R, Griffin SJ, Somani BK. Outcomes and long-term follow-up with the use of ureteral access sheath for pediatric ureteroscopy and stone treatment: results from a tertiary endourology center. J Endourol. 2019;33:79–83. doi:10.1089/end.2018.0448
14. Tanaka ST, Makari JH, Pope J, Adams MC, Brock JW
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.