Back to Journals » Journal of Asthma and Allergy » Volume 18
Skin Prick Test and Patch Test: Environmental and Chemical Allergen Reactivity Pattern Among Yemeni Patients in Sana’a City, Yemen
Authors Al-Ghoury AA ![]() , Obaid JMAS
, Obaid JMAS ![]() , Ali WA, Al-Shaybani MA
, Ali WA, Al-Shaybani MA
Received 23 May 2025
Accepted for publication 15 October 2025
Published 22 October 2025 Volume 2025:18 Pages 1413—1424
DOI https://doi.org/10.2147/JAA.S538601
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Luis Garcia-Marcos
Abdulbasit A Al-Ghoury,1,2 Jamil MAS Obaid,1,3 Waheed A Ali,4 Mohammed A Al-Shaybani5
1Laboratory Medicine Department, Faculty of Medicine and Health Sciences, Emirates International University, Sana’a, Yemen; 2Laboratory Medicine Department, Faculty of Medicine and Health Sciences, Amran University, Amran, Yemen; 3Medical Laboratory Sciences Department, Faculty of Medicine and Health Sciences, Ibb University, Ibb, Yemen; 4Department of Microbiology and Immunology, Faculty of Medicine and Health Sciences, Taiz University, Taiz, Yemen; 5Elaj Medical Center, Sana’a, Yemen
Correspondence: Jamil MAS Obaid, Department of Medical Laboratory Sciences, Ibb University, B.O.Box: 70270, Asalaba, Ibb City, Yemen, Tel +00967773979848, Email [email protected]; [email protected]
Background: The prevalence of hypersensitivity reactions to different allergens varies according to the population studied and is subject to environmental and lifestyle factors. Early and delayed hypersensitivity are diagnosed with skin prick test and patch test.
Objective: This study aimed to identify the common environmental and chemical allergens sensitizing Yemeni allergic patients.
Subjects and Methods: A retrospective study was conducted using registries of patients who attended Elaj Medical Center in Sana’a city, Yemen, from January 1st to December 31st 2023. The collected data included sex, age, and the clinical laboratory test results of the skin prick test and the patch test.
Results: The skin prick test was performed on sixty-five patients compared to twenty-two who were tested with a patch test. Most of the positive participants were male, aged between 18 and 40 years. The most frequent environmental allergens causing immediate hypersensitivity were Dermatophagoides farinae and Dermatophagoides pteronyssinus mites (64.6% and 69.2%, respectively), Aspergillus (47.7%), cat dander and dog dander (43.1% and 35.4%, respectively). Dermatophagoides farinae mites mostly sensitized females with an odds ratio of 3.43 (95% CI, 1.13– 10.42, p=0.05). The most common chemical allergens that caused delayed hypersensitization were paraphenylenediamine (45.5%), potassium bichromate (45.5%), cobalt sulfate (36.4%), thiuram mix (27.3%), Vaseline (27.3%), and nickel sulfate (27.3%). Polysensitization was more frequent. The age of patients was directly proportional to the number of allergens responsible for immediate hypersensitivity (r-0.298, p=0.016).
Conclusion: Yemeni patients exhibited high sensitization to aeroallergens and chemical allergens. Females showed a higher propensity for polysensitization. The pattern of sensitization to environmental and chemical allergens in Yemen differs somewhat from neighboring Arab and Asian countries. Further multi-center studies are needed to support and establish a standard country-specific allergens panel for testing.
Keywords: skin prick test, patch test, allergens, atopy, immediate hypersensitivity, delayed hypersensitivity, Yemen
Introduction
Allergic diseases are prevalent among all populations globally, and their rates have increased over time.1 The etiology of these diseases comprises genetic and environmental factors that affect the exacerbated immune response characteristics of hypersensitivity. Allergic diseases, including allergic rhinitis, allergic asthma, atopic dermatitis, food allergy, and contact dermatitis, are all triggered by certain environmental and chemical allergens. Clinical features of allergies range from local mild manifestations to life-threatening condition.2 Allergies have a significant impact on the quality of life. Therefore, the identification of the responsible allergen is central for the treatment and preventive measures of allergies. Every population needs to identify the most common allergens in their environment.
Immediate hypersensitivity reactions are mediated by IgE antibodies that sensitize mast cells. Allergen crosslinking of IgE leads to mast cell activation and rapid degranulation of mediators such as histamine, serotonin, and other inflammatory mediators. These mediators cause vasodilation, smooth muscle contraction, decreased blood pressure, bronchoconstriction and, in severe cases, anaphylactic shock.2,3 Environmental allergens, both indoor and outdoor allergens, cause immediate hypersensitivity. These include pollen, mold, pets, dust mites, and cockroaches.4,5 The skin prick test is a standard and recommended test for the diagnosis of immediate type I hypersensitivity reactions even in modern allergy practice. It investigates and identifies the potential cause of allergy in a given patient from different allergen panels tested.6
Allergic contact dermatitis is a delayed-type hypersensitivity that develops 48–72 hours after contact with an allergen. Contact with an offending chemical or allergen enables it to penetrate the skin and conjugate with a protein, then activate CD4+ T-cells. Activated T cells release cytokines, enhancing further immune reactions that lead to the development of dermatitis. Clinical manifestations present with erythema, swelling, pruritus and vesicle development.7 Responsible allergens differ greatly among populations based on geography, cultural and personal habits.8 The most prevalent allergens that induce contact dermatitis are poison ivy, rubber, nickel, fragrances, and cosmetics9 A patch test has a high diagnostic efficacy for delayed-type allergy dermatitis and identification of the responsible allergen.10
The global burden of asthma and atopic dermatitis rose in 2021 to be 260 million (95% UI 227–298) patients and 129 million (95% UI 124–134) respectively. While that of allergic rhinitis was 400 million, contact dermatitis was 253 million (95% UI 204–314).11–13 Yemen lacks the exact data about allergic diseases; however, it was reported that the prevalence of asthma and hay fever was 14.4% and 12%, respectively.14,15 In addition, published data on the allergens responsible for hypersensitivity among Yemeni patients is limited, except for one carried out in Taiz City.16
Yemen, like all low-income countries, until recently lacked the specialized centers for allergen identification in hypersensitivity patients. Consequently, immunotherapy treatment with hyposensitization cannot be pursued. Elaj Medical Center, in the capital Sana’a City, is the first specialized center for hypersensitivity diagnosis and immunotherapy. Therefore, the objective of the current study was to identify the pattern of allergens implicated in immediate and delayed hypersensitivity reactions among Yemeni patients. We retrospectively analyzed the registry of patients who had attended Elaj Medical Center in Sana’a City, Yemen, and were investigated using the skin prick test and the patch test.
Subjects and Methods
The study was conducted as a retrospective study using registries for patients who attended Elaj Medical Center in Sana’a city, Yemen, from January 1st to December 31st 2023. The data of patients included demographic information such as sex and age. The laboratory test results of both the skin prick test and the patch test for patients were collected from the registry of Elaj Medical Center. The protocol of this study and its ethical considerations had been approved by the ethical committee at the Faculty of Medicine and Health Sciences, Emirates International University, and by the administration of Elaj Medical Centre in accordance with the ethical standards established in the Declaration of Helsinki 2013.
Analyses were requested by dermatologists based on clinical symptoms. The inclusion criteria included suspicion of any type of allergies, while the exclusion criteria included the use of drugs like antihistamines, anti-inflammatories, corticosteroids and immunosuppressants unless stopped one week before.
Skin prick testing is a skin test for immediate IgE-mediated allergy. A set of 30 allergens with positive and negative controls were used (Inmuotek, Madrid, Spain). Skin prick tests were performed on the inner forearm or the back using the standard protocol.17 The selected area was cleaned with soap and water then alcohol, and marked with each allergen placed 2 cm apart. A drop of allergen solution was placed on mark, and a small prick through the drop was made using a sterile prick lancet. A new lancet was used for each allergen tested. Excess allergen solution was dabbed off with tissue. The skin reaction was observed within 20–30 minutes with a wheel and flare. Wheel diameter greater than 3 mm compared to negative control was recorded as a positive reaction. Histamine was used as a positive control, and saline was used as a negative control. The allergens used in the skin prick test were: mites (Dermatophagoides farinae, Dermatophagoides pteronyssinus and storage mites); mold and Yeast (Alternaria, Aspergillus mix, Candida albicans, penicillium mix, and Cladosporium herbarum); grass pollens (cocksfoot, rye, timothy mix, timothy, and Bermuda grasses); tree pollens (date palm, mimosa, and rough pigweed); weed pollens (fat hen, mugwort, plantain, sorrel, chenopodiaceae mix, compositae, pellitory of the wall, Amaranthus spinosus, Xanthium strumarium, salsola kali, and dandelion); epithelia (cat, horse, and dog); and insects (cockroach Blattella germanica and mesquite).
Patch testing investigates contact hypersensitivity or delayed-type hypersensitivity using a panel of 20 allergens recommended as an Indian standard series (Credisol, Creative Diagnostic Medicare Pvt. Ltd., Mumbai, India). The analyzed allergens were paraphenylenediamine, formaldehyde, epoxy resins, benzocaine, balsam of Peru, parabens mix, chlorocresol, cobalt sulfate, 2-mercaptobenzothiazole, potassium bichromate, parthenium, black rubber mix, thiuram mix, wool alcohol (lanolin), Vaseline, colophony, nickel sulfate, neomycin sulfate, nitrofurazone, and fragrance mix. The tests were performed on the back skin according to the standard procedure using a hypoallergenic adhesive paper with chambers.18 A small amount of each allergen was carefully squeezed onto a filter paper and placed in the test chamber, then labeled with correct identification. Readings were taken at 48 and 96 hours after removal of the adhesive paper. The development of erythematous papular or vesicular lesions indicating a positive reaction and interpreted according to the manufacturer’s instructions: +1 is a weak positive reaction with non-vesicular erythema, infiltration, and possible papules; +2 is a strong positive reaction with vesicular erythema, infiltration and papules; and +3 is an extreme positive reaction with intense erythema infiltration, coalescing vesicles, and a bullous reaction.
Data was entered into a Microsoft Excel version 2021 extraction sheet and analyzed using IBM SPSS version 19 software (IBM). Qualitative variables were presented using frequency and percentage. Association and comparison of frequencies were analyzed using X2 test and Fisher’s exact test. The difference for quantitative variables was analyzed using the nonparametric Mann–Whitney U-test. Results were considered statistically significant if the p value was ≤.0.05.
Results
The patients analyzed with the skin prick test were sixty-five (74.4%), and those analyzed for the patch test were twenty-two (25.6%). Most of the positive participants were males aged between 18 and 40 years (Table 1). Analyses were requested by dermatologists based on clinical symptoms. Both groups were tested separately, i.e., no one was tested for both analyses.
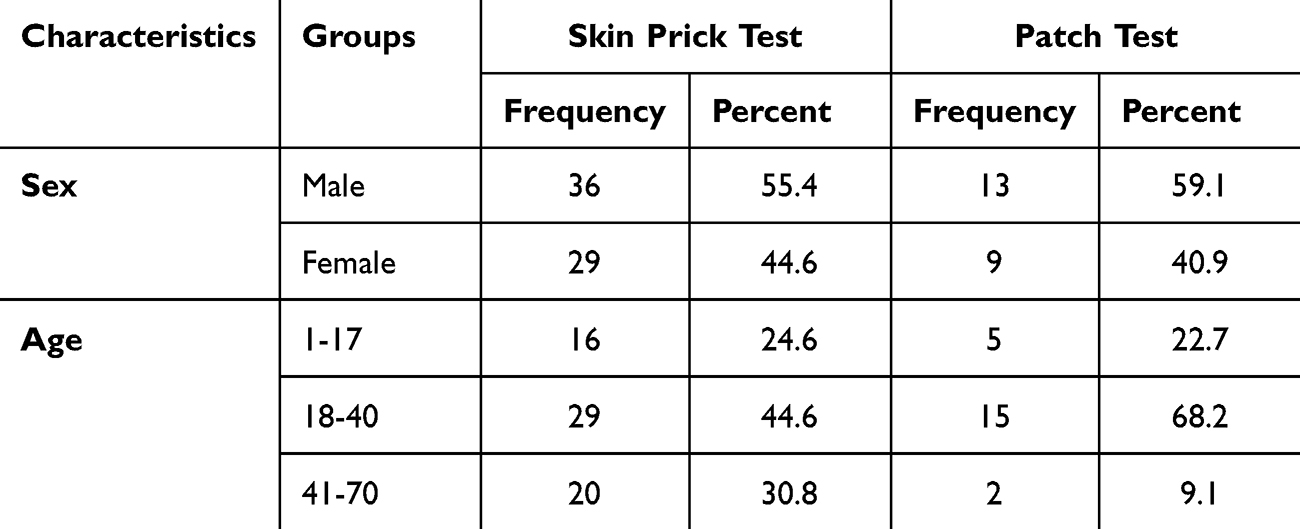 |
Table 1 Demographic Data of Yemeni Patients Attending the Elaj Center Were Tested with Skin Prick Tests and Patch Tests |
Table 2 lists the total and gender distribution of the immediately sensitized patients according to individual allergens. The most frequent environmental allergens causing immediate hypersensitivity were Dermatophagoides farinae and Dermatophagoides pteronyssinus mites (64.6% and 69.2%, respectively), followed by Aspergillus (47.7%) cat dander and dog dander (43.1% and 35.4%, respectively). The prevalence of these allergens among both sexes showed close percentages, but the highly prevalent allergen among females was Dermatophagoides farinae mites (79.3%).
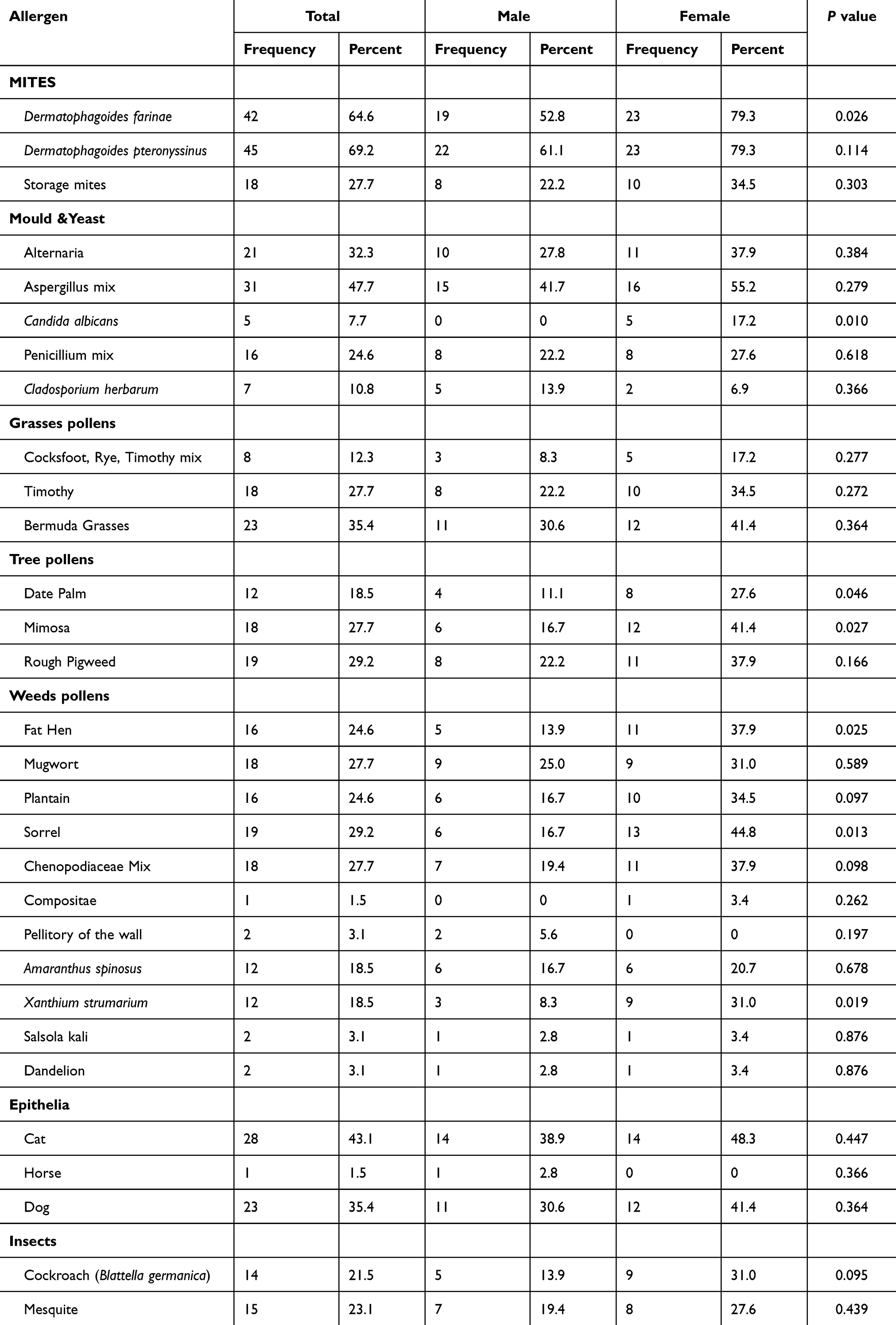 |
Table 2 Distribution of Positive Skin Prick Tests Among Participants by Sex and Allergen |
The allergens exhibiting more female predominance with statistically different results compared to males are Candida albicans, Dermatophagoides farinae mites, and pollens of date palm, mimosa, rough pigweed, sorrel, and Xanthium strumarium. The calculated odds ratio at 95% confidence intervals for them reveals statistical significance for only Dermatophagoides farinae (OR=3.43, 95% CI, 1.13–10.42, p=0.05), Sorrel (OR=4.06, 95% CI, 1.30–12.73, p=0.027), and Xanthium strumarium (OR=4.95, 95% CI, 1.20–20.47, p=0.043) as shown in Table 3.
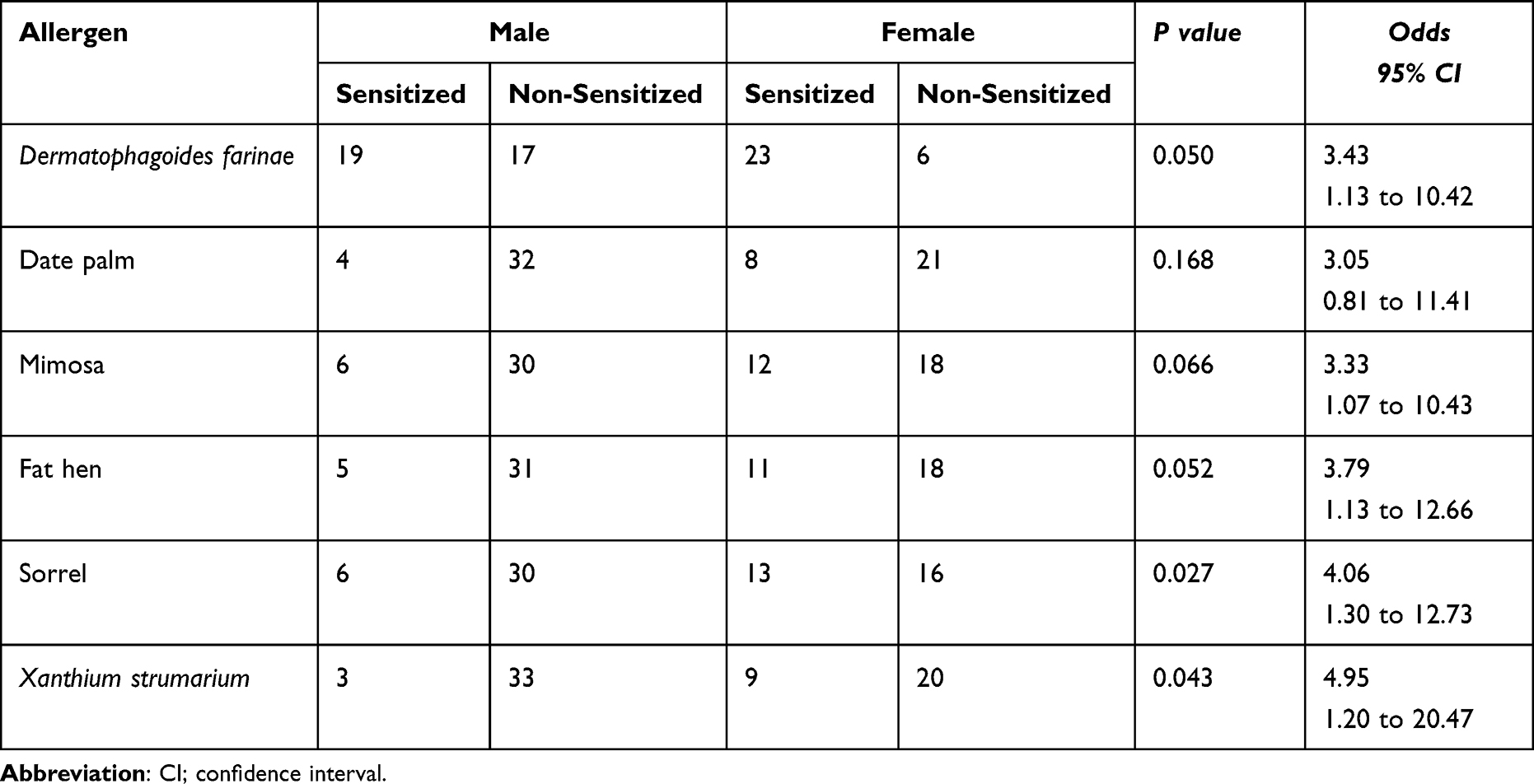 |
Table 3 Odds of Sensitization Risk by Sex for Statistically Significant Distributed Allergens in Skin Prick Tests |
The sensitized patients with skin prick test allergens are mostly adults belonging to the middle age group (18–40 years) compared to other age groups. The difference was statistically significant with allergens, pathogens (Candida albicans and Penicillium mix), plants (mimosa, rough pigweed, and fat hen), animals (cats and dogs), and insects (cockroaches and mosquitoes), as listed in Table 4.
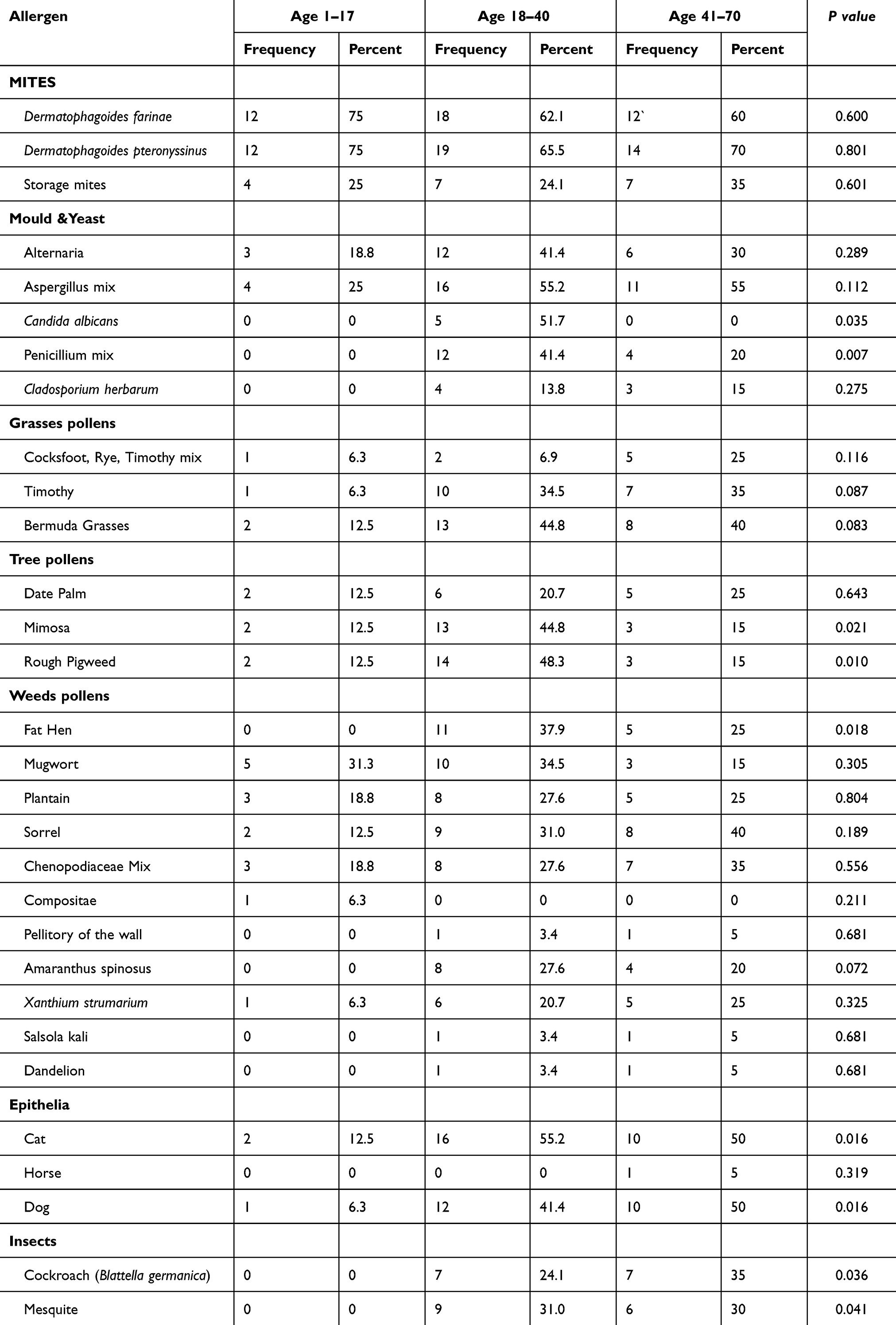 |
Table 4 Distribution of Sensitized Individuals by Age Group and Responsible Allergen Skin Prick Tests |
The high number of patients sensitized to chemical allergens caused delayed hypersensitization, reported with paraphenylenediamine (45.5%), potassium bichromate (45.5%), cobalt sulfate (36.4%), thiuram mix (27.3%), Vaseline (27.3%), and nickel sulfate (27.3%), as listed in Table 5. The statistically significant difference between sexes with male predominance was reported for formaldehyde and Vaseline only (p<0.05). Meanwhile, the difference according to age groups showed no statistical significance, despite the predominance of the Middle Ages (18–40 years) as reported in Table 6.
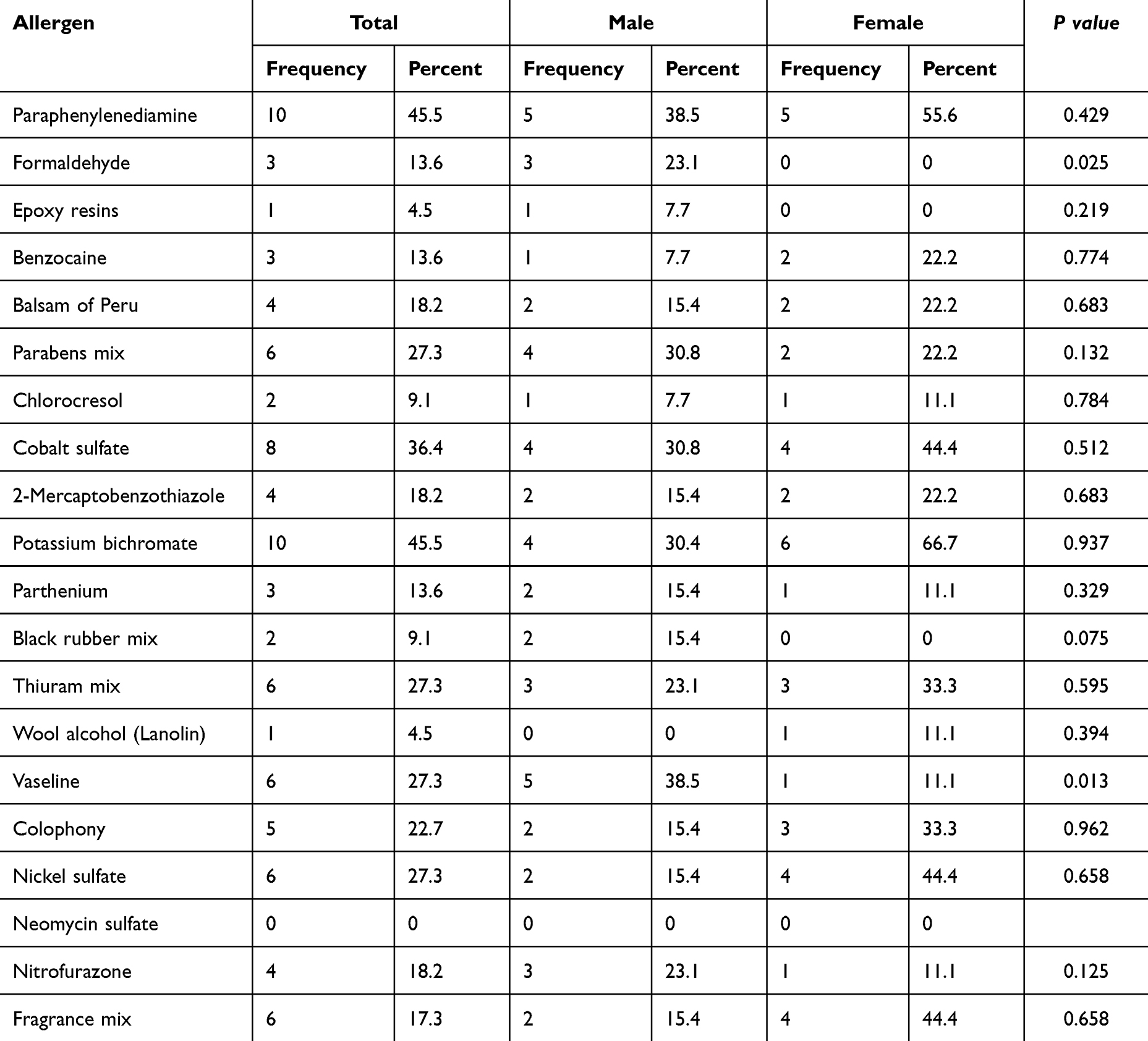 |
Table 5 Distribution of Positive Patch Test Results Among Yemeni Patients by Sex |
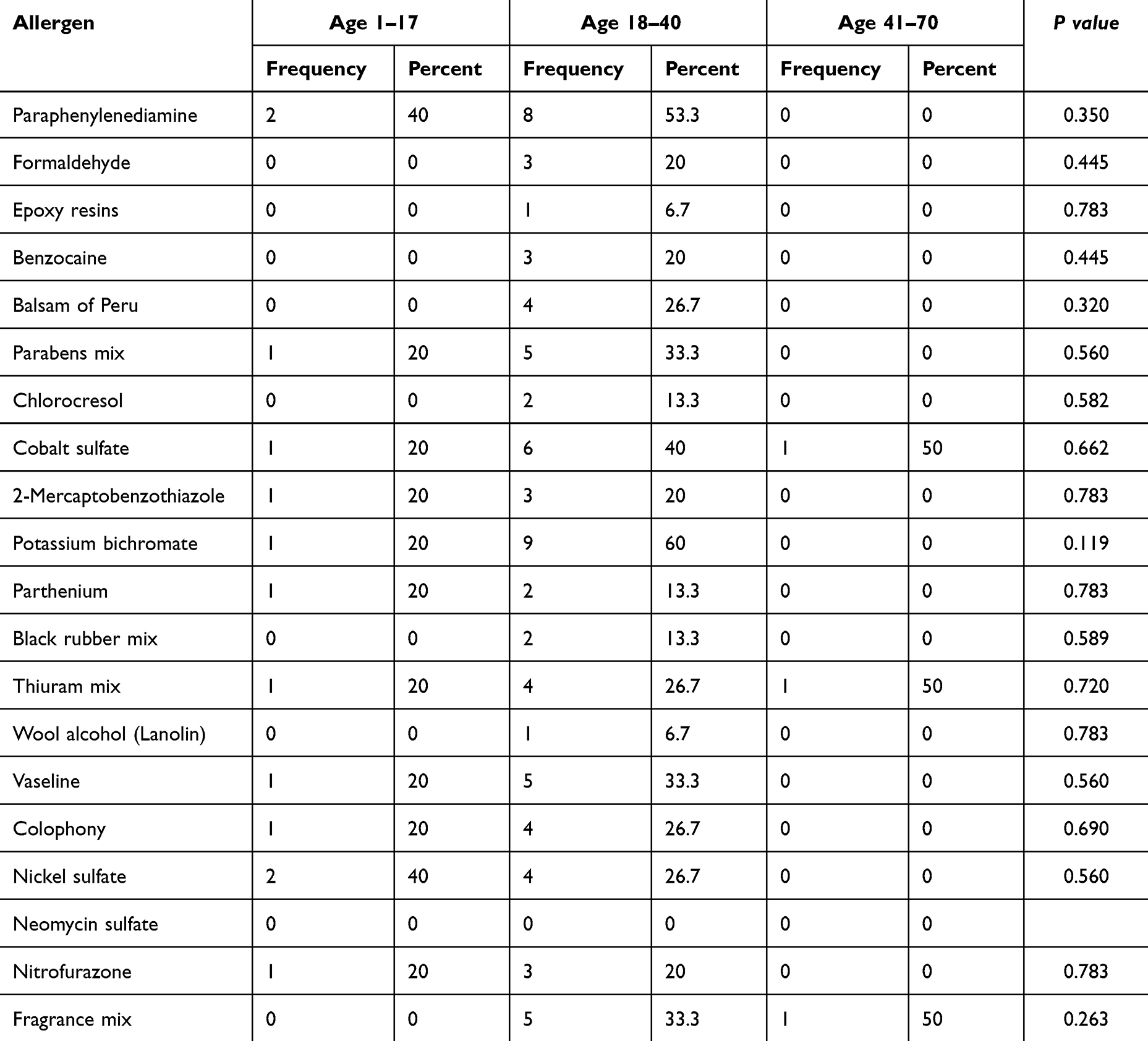 |
Table 6 Distribution of Sensitized Individuals by Age Group and Responsible Allergen in Patch Tests |
Figure 1 depicts the polysensitization by different numbers of allergens. Most patients were sensitized to 6–8 allergens in the skin prick test (23.1%) and 3–5 allergens in the patch test (36.4%); very few patients were sensitized by more than twelve allergens (about 4.5%). The age of patients was directly proportional to the cumulative number of allergens to which patients were sensitized by immediate hypersensitivity; the correlation coefficient was r=0.298, and p=0.016 (Figure 2).
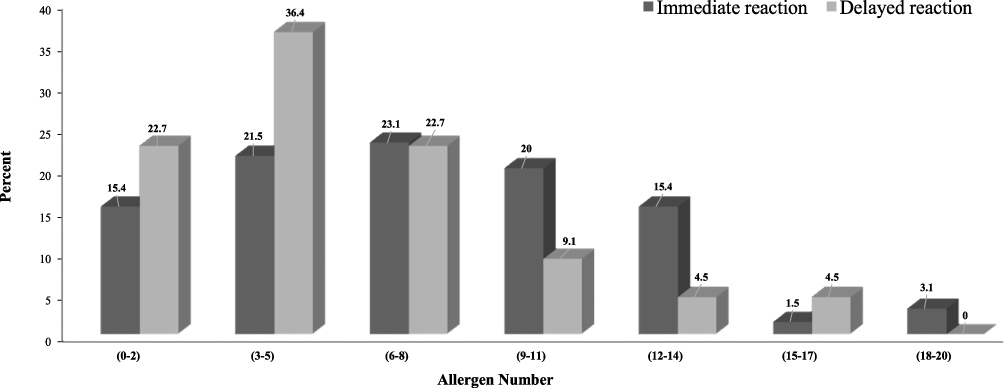 |
Figure 1 Distribution of polysensitization allergens for immediate and delayed hypersensitivity among different age groups. |
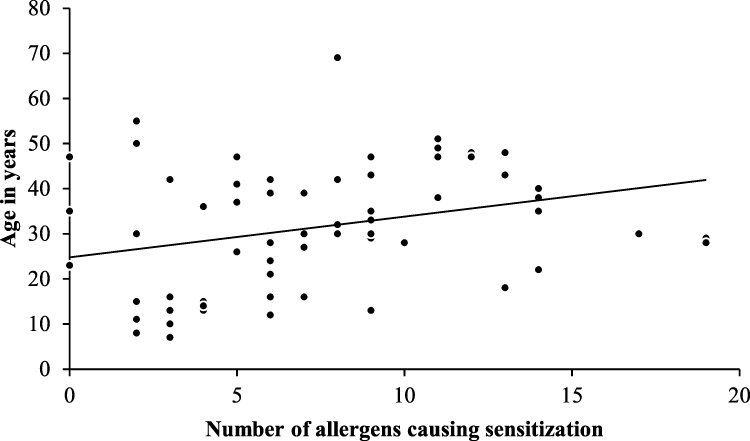 |
Figure 2 Correlation between age and the cumulative number of allergens causing immediate hypersensitivity in Yemeni patients. |
Discussion
This study identified the most prevalent allergens responsible for sensitivity in Yemeni patients. The most frequent allergens in the skin prick test were Dermatophagoides farinae, Dermatophagoides pteronyssinus, Aspergillus, cat dander, and dog dander. The most frequent allergens in the patch test were paraphenylenediamine, potassium bichromate, cobalt sulfate, thiuram mix, Vaseline, and nickel sulfate. Polysensitization was noted and correlated with the age of patients.
The type of allergy and allergen profiling are region-specific and may change continuously due to changes in the environment, climate, and lifestyle.19,20 Allergen identification in each population suffering from hypersensitivity is essential for epidemiological aspects to provide comprehensive knowledge of locally prevalent allergens, which should be helpful in disease management and prevention planning. Therefore, this study constitutes one of the allergy studies involving the determination of common allergen affecting Yemeni patients. All thirty allergens selected for testing are found in the Yemeni environment.
A higher prevalence of immediate allergy than delayed allergy was reported globally,21 in agreement with the proportions of allergic patients tested with the skin prick test to those tested with the patch test in this study (3:1). A similar proportion (4:1) was reported in Saudi Arabia.22 The variations in prevalence across different regions may be attributed to differences in environmental exposures, genetic predispositions, and lifestyle factors. This highlights the need for regional epidemiological studies responsible for that difference.23
Gender specific prevalence showed a higher predominance in males than females in accordance with previous data from Taiz city in Yemen11 and Poland.24 The age group showing the highest positive rate was the age group of 20–44 years, followed by older individuals, in agreement with our data (18–40 years).24 Age accumulates polysensitization for patients as indicated by the direct correlation between age and the number of allergens reported in allergic Yemeni patients (r=0.298, p=0.016) in agreement with results reported early.25 Polysensitization by >6 allergens in the skin prick test and >3 allergens in the patch test were reported in about 80% of patients in concordance with another study. The alarm of polysensitization lies in its association with more severe disease.26
This gender difference indicates a potential gender-specific susceptibility to certain allergens to be reported as a risk factor with profound studies. Gender effect may be attributed to cultural habits in Yemen that may prohibit female treatment, sex hormonal differences and barriers efficiency. Meanwhile, the age difference is mainly attributed to immunological maturation in middle age compared to early development in childhood and decline in elder hood. Another factor of age is physical activity that exposes the patient to allergens mainly outdoor allergens. However, middle-aged patients exhibited high sensitization to Candida albicans, Penicillium mix, mimosa, rough pigweed, fat hen, cats and dogs’ dander, cockroaches and mosquitoes.
The skin prick test revealed different allergen frequencies; the most prevalent were Dermatophagoides farinae mite (64.6%), Dermatophagoides pteronyssinus mite (69.2%), Aspergillus (47.7%), cat hairs (43.1%), and dog hair (35.4%), resembling results obtained before in Taiz city, Yemen.16 The rate of dust mite prevalence in Egypt was 51.2% and 72.6%, respectively.27 Lower rates (16%, 33%) were reported in Bahrain, a country with a high-income level.28 In Thailand, the cat dander frequency was 11.77%, and the dog dander was 1.89%; contrary to our result.29 This is due to poor hygiene, vet services, and low prevention measures. Dermatophagoides farinae mite was mostly prevalent among females because it is the most common dust mite. Females accept this indoor allergen during daily house cleaning. The odds of occurrence among females were 3.43 times that for males (OR=3.43, 95% CI, 1.13–10.42, p=0.05). Females also experience candidal infections during their life in the form of vaginal thrush.
The patch test of delayed hypersensitivity among Yemeni patients reported that the most prevalent contact allergens were paraphenylenediamine (45.5%), potassium bichromate (45.5%), cobalt sulfate (36.4%), thiuram mix (27.3%), Vaseline (27.3%) and nickel sulfate (27.3%). In comparison, the most common allergens in China were nickel sulfate, fragrance mix, thiuram mix, ammoniated mercury, and P-phenylenediamine.30 In Turkey, nickel sulfate, cobalt chloride, potassium dichromate, thiuram mix, P-phenylenediamine, and formaldehyde were the most prevalent contact allergens.31
Contrary to data published from India,32 this study showed that the contact allergens were more prevalent among females than males, consistent with data on Spanish patients.33 This may be due to their prevalent use by females in the local environment. Contact allergens may be found in cosmetics (paraphenylenediamine, cobalt sulfate, and Vaseline), jewelry (nickel sulfate), or household items (potassium bichromate and thiuram mix).
Despite no statistically significant difference, the middle-age group (18–40 years) participants had more sensitized by contact allergens. This is mainly attributed to the high activity of humans at this age. A slight elevation of age was reported among delayed hypersensitivity patients in Spain; the elevation of sensitization also increased with age advances.33
This study is limited by constraints of resources, funding, and being a single-center study. The generalization of results will be out of ideal inferences. It threw a stone in this field. Expanding this study to include larger and more diverse populations across the area of Yemen, as well as conducting longitudinal studies, would provide a more comprehensive understanding of the epidemiology and trajectories of atopic and contact allergies. An expanded survey with more allergens and correlation with clinical and environmental data will enrich this topic and improve the management and prevention outputs. The data of allergen patterns in this study can also help the physician and local health authorities in planning effective protection and management strategies. For instance, immunotherapy was established in Elaj Center for the most common allergens by hyposensitization for many patients. Governmental support is needed to expand testing and immunotherapy.
Conclusion
This study provides a comprehensive analysis of allergens responsible for hypersensitivity in Yemen. It reveals a unique pattern of sensitivity for eleven most common environmental and chemical allergens prevalent in the Yemeni environment: Dermatophagoides farinae, Dermatophagoides pteronyssinus, Aspergillus, cat dander, dog dander, paraphenylenediamine, potassium bichromate, cobalt sulfate, thiuram mix, Vaseline, and nickel sulfate. This data will provide a guide for physicians, patients and health authorities for planning a strategy for the protection and management of allergic diseases.
Data Sharing Statement
All data are available in this manuscript.
Ethics Standards and Consent to Participate
The protocol of this study and its ethical consideration had been approved by the ethical committee at the Faculty of Medicine and Health Sciences, Emirates International University, and by the administration of Elaj Medical Centre. The patient informed consent for this study was waived by the Ethics Committee of the Faculty of Medicine and Health Sciences, Emirates International University, because of the retrospective nature of this study. All patients’ data included in this study were anonymized to protect participants’ privacy and confidentiality. This work met the international ethical guidelines, mainly the WMA Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects, 2013.
Acknowledgment
Thank you to Laith Al-Shibani, Aya Al-Assouli, Doaa Al-Faqih, Ghadeer Al-Attab, Hana’a Al-Halek, Rasha Al-Qawdari, Walaa Saboona, Ayat Al-Mashdli, Eman Al-Gurbani, Hajar Homed, Johara Babaer, Sameh Al-Adeeb, and Lola Al-Ameri for their assistance.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors did not receive any funds.
Disclosure
The authors declare that they have no competing interests.
References
1. GBD 2019 Allergic Disorders Collaborators, Shin YH, Hwang J, Kwon R, et al. Global, regional, and national burden of allergic disorders and their risk factors in 204 countries and territories, from 1990 to 2019: a systematic analysis for the Global Burden of Disease Study 2019. Allergy. 2023;78(8):2232–2254. doi:10.1111/all.15807.
2. Owen JA, Punt J, Stranford SA, Jones PP. Kuby Immunology.
3. Justiz Vaillant AA, Vashisht R, Zito PM. Immediate Hypersensitivity Reactions. In: StatPearls. In: StatPearls Publishing, Treasure Island (FL); 2023.
4. Thibaudon M, Besancenot J. Outdoor aeroallergens and climate change. Rev Mal Respir. 2021;38(10):1025–1036. doi:10.1016/j.rmr.2021.08.007
5. Ahluwalia SK, Matsui EC. Indoor environmental interventions for furry pet allergens, pest allergens, and mold: looking to the future. J Allergy Clin Immunol Pract. 2018;6(1):9–19. doi:10.1016/j.jaip.2017.10.009
6. Malling HJ, Allesen-Holm P, Karved LS, Poulsen LK. Proficiency testing of skin prick testers as part of a quality assurance system. Clin Transl Allergy. 2016;6:36. doi:10.1186/s13601-016-0126-7
7. Aquino M, Rosner G. Systemic Contact Dermatitis. Clin Rev Allergy Immunol. 2019;56(1):9–18. doi:10.1007/s12016-018-8686-z
8. Lazzarini R, Mendonça RF, Hafner MFS. Allergic contact dermatitis to shoes: contribution of a specific series to the diagnosis. An Bras Dermatol. 2018;93(5):696–700. doi:10.1590/abd1806-4841.20187370
9. M.c D. Classification of hypersensitivity reactions. Allergy Asthma Proc. 2019;40:470–473. doi:10.2500/aap.2019.40.4274
10. Garg V, Brod B, Gaspari AA. Patch testing: uses, systems, risks/benefits, and its role in managing the patient with contact dermatitis. Clin Dermatol. 2021;39(4):580–590. doi:10.1016/j.clindermatol.2021.03.005
11. Oh J, Kim S, Kim MS, GBD 2021 Asthma and Allergic Diseases Collaborators. Global, regional, and national burden of asthma and atopic dermatitis, 1990-2021, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021. Lancet Respir Med. 2025;13(5):425–446. doi:10.1016/S2213-2600(25)00003-7
12. Nur Husna SM, Tan HT, Md Shukri N, Mohd Ashari NS, Wong KK. Allergic Rhinitis: a Clinical and Pathophysiological Overview. Front Med Lausanne. 2022;9:874114. doi:10.3389/fmed.2022.874114
13. Tang X, Lin L, Yu F, Ma Y, Liu Z, Xu X. Allergic-related skin diseases: global disease burden from 1990 to 2021 and future trends. World Allergy Organ J. 2025;18(7):101072.
14. Bahaj S, Moharem A, Kaid A. Prevalence of asthma and allergic diseases among high school students in urban and rural communities, Yemen. Egypt J Med Microbiol. 2012;38:1–5.
15. Masjedi M, Ainy E, Zayeri F, Paydar R. Assessing the prevalence and incidence of asthma and chronic obstructive pulmonary disease in the Eastern Mediterranean Region. Turk Thorac J. 2018;19:56–60. doi:10.5152/TurkThoracJ.2018.17051
16. Ali WAM, Obaid JMAS. Sensitization Pattern to common Inhalant allergens among patients with Allergic Rhinitis in Taiz, Yemen. AL - Saeed J Humanities Appl Sci. 2019;3(2):15–23.
17. Heinzerling L, Mari A, Bergmann KC, et al. The skin prick test - European standards. Clin Transl Allergy. 2013;3(1):3. doi:10.1186/2045-7022-3-3
18. Lazzarini R, Duarte I, Ferreira AL. Patch tests. An Bras Dermatol. 2013;88(6):879–888. doi:10.1590/abd1806-4841.20132323
19. Hong SJ. Report of Korean ISAAC epidemiologic study for asthma and allergic diseases in children. Pediatr Allergy Respir Dis. 2007;17(Suppl 1):S55–S66.
20. Ariano R, Canonica GW, Passalacqua G. Possible role of climate changes in variations in pollen seasons and allergic sensitizations during 27 years. Ann Allergy Asthma Immunol. 2010;104:215–222. doi:10.1016/j.anai.2009.12.005
21. Momtazmanesh S, Rezaei N. Hypersensitivity. In: Rezaei N, editor. Encyclopedia of Infection and Immunity. Elsevier; 2022:243–258.
22. Almohideb M. Epidemiological Patterns of Skin Disease in Saudi Arabia: a Systematic Review and Meta-Analysis. Dermatol Res Pract. 2020;2020:5281957. doi:10.1155/2020/5281957
23. Aldakheel FM. Allergic Diseases: a Comprehensive Review on Risk Factors, Immunological Mechanisms, Link with COVID-19, Potential Treatments, and Role of Allergen Bioinformatics. Int J Environ Res Public Health. 2021;18(22):12105. doi:10.3390/ijerph182212105
24. Dor-Wojnarowska A, Liebhart J, Miecielica J, et al. The Impact of Sex and Age on the Prevalence of Clinically Relevant Sensitization and Asymptomatic Sensitization in the General Population. Arch Immunol Ther Exp. 2017;65:253–261. doi:10.1007/s00005-016-0425-7
25. Silvestri M, Rossi GA, Cozzani S, Pulvirenti G, Fasce L. Age-dependent tendency to become sensitized to other classes of aeroallergens in atopic asthmatic children. Ann Allergy Asthma Immunol. 1999;83(4):335–340. doi:10.1016/S1081-1206(10)62674-9
26. Cacheiro-Llaguno C, Mösges R, Calzada D, González-de la Fuente S, Quintero E, Carnés J. Polysensitisation is associated with more severe symptoms: the reality of patients with allergy. Clin Exp Allergy. 2024;54(8):607–620. doi:10.1111/cea.14486
27. Abou Galal DIM, Hany HM, El Sobky MMK, Harbahr NM, El Kerash WM. Morphological identification of house dust mite species in Menoufia Governorate and their antigen effect in immunoglobulin E response in allergic patients. Menoufia Med J. 2019;32:1,14.
28. Hasan HY, Rizwan MA. Prevalence of Inhalant and Food Allergies after Skin Prick Testing in Patients with Resistant Allergic Rhinitis in Warm Humid Weather. Bahrain Med Bull. 2015;37:2. doi:10.12816/0014420
29. Kulalert P, Poachanukoon O, Nanthapisal S, et al. Minimum number and types of allergens for a skin prick test panel in Thai children with allergic respiratory diseases. Allergy Asthma Clin Immunol. 2022;18(1):77. doi:10.1186/s13223-022-00718-7
30. Dou X, Zhao Y, Ni C, Zhu X, Liu L. Prevalence of contact allergy at a dermatology clinic in China from 1990-2009. Dermatitis. 2011;22(6):324–331. doi:10.2310/6620.2011.11051
31. Tunca M, Çalışkan E, Yürekli A. Frequent contact allergens in Ankara/Turkey: a retrospective study of patch test results. Turk Arch Dermatol Venereol. 2019;53(2):49–52.
32. Gopinath VPK, Simi VM, Ahammed KB, Rishad CMA, Farisa PM. Common allergens in patients with contact dermatitis identified using patch test in a tertiary care centre in North Kerala. Int J Res Dermatol. 2019;5(1):78–87. doi:10.18203/issn.2455-4529.IntJResDermatol20185054
33. Aguilar- Bernier M, Bernal-Ruiz AI, Rivas-Ruiz F, Fernández-Morano MT, de Troya-Martín M. Contact Sensitization to Allergens in the Spanish Standard Series at Hospital Costa del Sol in Marbella, Spain: a Retrospective Study (2005–2010). Actas Dermo-Sifiliográficas. 2012;103(3):223–228. doi:10.1016/j.adengl.2011.07.008
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.