Back to Journals » Therapeutics and Clinical Risk Management » Volume 18
Single Nucleotide Polymorphism in the 3’ Untranslated Region of PRKAA2 on Cardiometabolic Parameters in Type 2 Diabetes Mellitus Patients Who Received Metformin
Authors Virginia DM ![]() , Patramurti C, Fenty, Setiawan CH
, Patramurti C, Fenty, Setiawan CH ![]() , Julianus J, Hendra P, Susanto NAP
, Julianus J, Hendra P, Susanto NAP
Received 17 November 2021
Accepted for publication 14 March 2022
Published 5 April 2022 Volume 2022:18 Pages 349—357
DOI https://doi.org/10.2147/TCRM.S349900
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Video abstract presented by Dita Maria Virginia.
Views: 189
Dita Maria Virginia,1 Christine Patramurti,2 Fenty,1,3 Christianus Heru Setiawan,1 Jeffry Julianus,2 Phebe Hendra,1 Nicholas Adi Perdana Susanto3
1Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Sanata Dharma University, Yogyakarta, Indonesia; 2Department of Pharmaceutical Analysis and Medicinal Chemistry, Faculty of Pharmacy, Sanata Dharma University, Yogyakarta, Indonesia; 3Bethesda Lempuyangwangi Hospital, Yogyakarta, Indonesia
Correspondence: Dita Maria Virginia, Universitas Sanata Dharma, Mrican, Tromol Pos 29, Yogyakarta, 55281, Indonesia, Tel +62 274 513301, Fax +62 274 562383, Email [email protected]
Purpose: This study aimed to explore the association of rs857148 A>C as 3ʹUTR variants with blood pressure, HbA1c profile, and lipid profiles as cardiometabolic parameters among patients with T2DM receiving metformin.
Patients and Methods: This cross-sectional analytic research was conducted with 114 consecutively selected patients with T2DM. Polymerase chain reaction-restriction fragment length polymorphism was conducted to determine rs857148. A total of 108 patients fulfilled inclusion and exclusion criteria.
Results: Genotype distribution agreed with the Hardy Weinberg Equation for Equilibrium (p> 0.05) but wildtype allele was found as the minor allele. Subjects with CC genotype and C allele had enhanced HbA1c levels (OR=7.12; 95% CI=1.05– 48.26; p=0.04; OR=1.66; 95% CI=1.06– 2.60; p=0.03, respectively). It was confirmed by dominant model whereas subjects with AA tended to have reduced HbA1c compared to AC+CC genotype (OR=0.15; 95% CI=0.02– 0.97; p=0.047). AC genotype had significant correlation to total cholesterol (OR=1.05; 95% CI=1.01– 1.10; p=0.03) compared to AA genotype.
Conclusion: We conclude that polymorphism of rs87148, specifically CC genotype and C allele, has a significant association with HbA1c and total cholesterol after considering oral hypoglycemia agent dose, age, gender, and combination therapy, compared to AA genotype. Future studies that involve a larger sample population and more rigorous selection criteria are required.
Keywords: PRKAA2, rs857148, 3ʹUTR, cardiometabolic, type 2 diabetes mellitus
Introduction
The prevalence of type 2 diabetes mellitus (T2DM) is regarded as a serious public health problem, especially in developing countries.1 Metformin is recommended as a cornerstone for initial therapy of T2DM. However, additional therapy may be added in combination when the target HbA1c has not been achieved.2,3 Remarkably, the T2DM prevalence in Indonesia has been rising in the last two decades,4 especially among the urban population.5 Studies related to metformin efficacy either monotherapy or combination in Indonesian population found that our patients tend to have poor glycemic control.6–8
Several publications have declared glycemic response variations of metformin therapy, either monotherapy or combination therapy.9–11 Furthermore, a group of patients could not tolerate the metformin’s side effects.12 A study among patients with T2DM who were covered national health insurance in Indonesia confirmed that the patients reported metformin side effects in the gastrointestinal tract.13 On the other hand, it is well known that the main pharmacological mechanism of metformin is reducing gluconeogenesis in the liver besides sensitizing insulin and improving GLP-1.14,15 Notably, adenosine monophosphate protein kinase (AMPK) contributed as the main target of the metformin mechanism.16,17
Individual genetic imprints are one of the causes of metformin effectiveness variability. The previous study confirmed that genetic variations affect metformin efficacy regarding pharmacokinetics and pharmacodynamics of metformin.18–21 Recently, AMPK is the focused enzyme related to metformin pharmacodynamic. Xiao et al in 2021 reported that one of the subunits of AMPK, which is PRKAG2, is associated with metformin response among Chinese patients with T2DM.21 AMPK has 3 subunits whereas AMPKα2, encoded by PRKAA2, plays a pivotal role during Thr-172 phosphorylation.22,23
Metformin has been reported to have a beneficial effect on blood pressure and lipid profiles. Hypertension risk could be reduced among metformin users who are newly diagnosed with T2DM.24 Metformin has proven blood pressure reduction in patients with T2DM compared with insulin therapy.25 Monotherapy metformin could significantly reduce triglyceride and low-density lipoprotein cholesterol (LDL-c) levels, and enhance (high-density lipoprotein cholesterol) HDL-c.26 The various international guidelines recommend detecting and monitoring cardiometabolic parameters in addition to HbA1c level in patients with T2DM.2,3 Therefore, it is important to assess cardiometabolic parameters to reduce cardiovascular disease risk in patients with T2DM.27,28 Virginia et al in 2021 demonstrated that the PRKAA2 genetic variation (rs9803799) had a significant association to cardiovascular risk among patients with T2DM receiving monotherapy metformin.29
However, few studies have observed the association of cardiometabolic parameters and AMPK subunit genetic variations. Single nucleotide polymorphism (SNP) rs857148 is a 3’ untranslated region (UTR) of PRKAA2 and located in chromosome 1:5,670,948.30 Although this SNP is not located in the exon area, the 3’ UTR has been confirmed to affect DNA stability and the micro RNA/mRNA interaction, mRNA stability, localization, translation, and degradation.31–33 Therefore, this present study aimed to observe the influence of 3’ UTR PRKAA2 variants, especially rs857148 A>C, on blood pressure, HbA1c profile, and lipid profiles as cardiometabolic parameters among patients with T2DM consuming metformin.
Materials and Methods
This observational analytic research using a cross-sectional study design was conducted at the Bethesda Lempuyangwangi Hospital, Yogyakarta, Indonesia. The study included patients with T2DM who were 35–75 years old using national health coverage and have been consuming metformin either monotherapy or combination therapy for a minimum of 3 months consecutively. We excluded patients with other types of diabetes mellitus, including type 1, monogenic, and gestational, had eGFR<30 mL/min, and refused to sign informed consent. The minimum sample size was 98 participants according to our study design and using type 1 error rate 0.05, power 0.8, predicted risk ratio 2.0, and proportion 0.3. A total of 114 patients with T2DM were consecutively recruited in this study, and only 6 participants were excluded because they did not receive metformin.
Patient’s data related to age, gender, blood pressure, and medication information were collected from medical records. Biochemical and genotyping data were obtained from blood samples were which collected during appointments. This study was approved by the Medical and Health Research Ethics Committee of Faculty of Medicine, Public Health, and Nursing, Universitas Gadjah Mada (KE/FK/0520/EC/2021) and data were complied with the principles established by Declaration of Helsinki and promoted by the Committee on Publication Ethics (COPE). All enrolled participants signed an informed written consent before participating.
Biochemical Analysis
Blood samples were collected in the morning after 8–10 h fasting by venipuncture. Clinical biochemical analyses were performed at the Laboratory of Bethesda Lempuyangwangi Hospital. Laboratory tests included HbA1c and lipid profiles (total cholesterol, HDL-c, LDL-c, and triglycerides), which were measured in fresh samples. HbA1c was assayed using tetradecyl trimethyl ammonium bromide. Total cholesterol levels were determined by cholesterol oxidase method/CHOD PAP. HDL-c and LDL-c were analyzed using direct methods. Glycerol-3-phosphate oxidase was applied to measure triglyceride levels.
DNA Extraction and Genotyping Analysis
Genomic DNA was extracted from peripheral blood in the K3EDTA tube by FavorPrep™ Genomic DNA Extraction Mini Kit following manufacturing procedures. The quality of DNA was evaluated using electrophoresis. Extracted DNA samples were stored at −70°C until genotyping analysis. Single nucleotide polymorphism (SNP) rs857148 was selected according to the International HapMap Project (http://hapmap.ncbi.nlm.nih.gov/). Genotyping was performed using polymerase chain reaction restriction fragment length polymorphism (PCR-RFLP). One set of primers of forward 5’- GACTAAGTTTCTCCTGTGTTAGTGG-3’ and reverse 5’-TTCCCAAAAGAGGTATGGACCC-3’ was applied for the amplification 369 bp. Each individual sample contained 5 μL of DNA which was mixed with 12.5 μL of the GoTaq Green Master Mix® in a PCR tube. Following an initial denaturation step at 95 °C for 5 min. We conducted thirty five cycles of amplification including, denaturation (95°C for 20s), annealing (56.1°C for 30s) and extension (72°C for 30s), with a final extension step at 72°C for 5 min. The PCR products were electrophoresed on a 3% agarose gel to check PCR product size. BSuRI restriction enzyme (ThermoScientific) was applied to detect rs857148 in the PRKAA2. The reaction mixtures were incubated at 37°C for 2 h, were inactivated at 37°C for 20 min, then were electrophoresed on 1.5% agarose gel.
We did PCR condition optimization, including annealing temperature and primer concentration. Incubation duration during the restriction process was also optimized. Validation of genotyping procedure was done through replication of several samples randomly using the same method which was PCR-RFLP.
Statistical Analysis
Data are expressed as frequency (percentage) for categorical variables or as mean±standard deviation (SD) for continuous variables. We performed Anova or Kruskal Wallis as appropriate to compare clinical characteristics between rs857148 genotypes. Multinomial logistic regression analysis was used to determine the association of rs857148 with hypertension, HbA1c level, and lipid profile, where hypertension categorized as blood pressure >130/>80 mmHg. Multiple inherited models including dominant, recessive, and allelic models were applied to estimate the influence of rs857148 on cardiometabolic parameters. A two tailed p-value < 0.05 was considered significant statistically. Two regression models were constructed to adjust potential confounders. Model 1 was adjusted for metformin dose, combination either sulfonylurea or insulin. Additionally, model 2 was adjusted for age, gender, metformin dose, glimepiride dose, and combination either sulfonylurea or insulin. We conducted all statistical procedures using SPSS software version 25.0 (IBM Corp., Armonk, NY)).
Results
Table 1 presents participants’ characteristics with an average age 60.58±8.16 years old and predominately female subjects. Interestingly, the mean of HbA1c was considered poor glycemic control, but the mean of lipid profiles was adequate. Metformin as combination therapy was predominantly prescribed in our study sample.
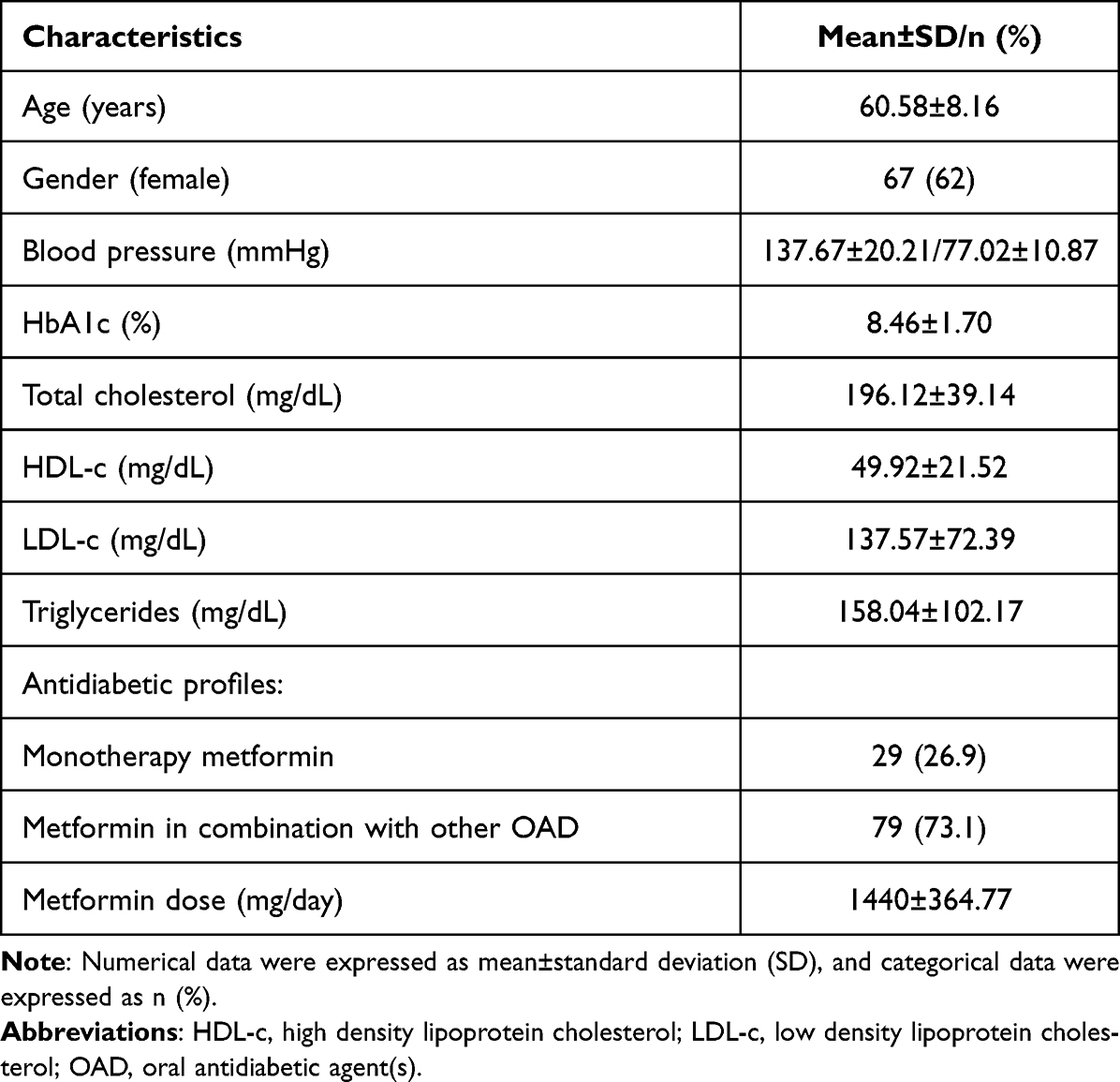 |
Table 1 Participants’ Characteristics |
We obtained different patterns of our PCR products after applying the BSuRI enzyme: wildtype homozygote (AA) indicated by one band of 369 bp, heterozygote (AC) indicated by three bands of 125, 244, and 369 bp, and mutant homozygote (CC) indicated by two bands of 125 bp and 244 bp (Figure 1). The genotype frequencies in our study sample were consistent with the Hardy-Weinberg equilibrium (HWE) equation (p=0.40). Table 2 shows clinical characteristics according to rs857148 genotype. We found that only systolic blood pressure had a significant difference between the rs85714 genotype (p=0.03).
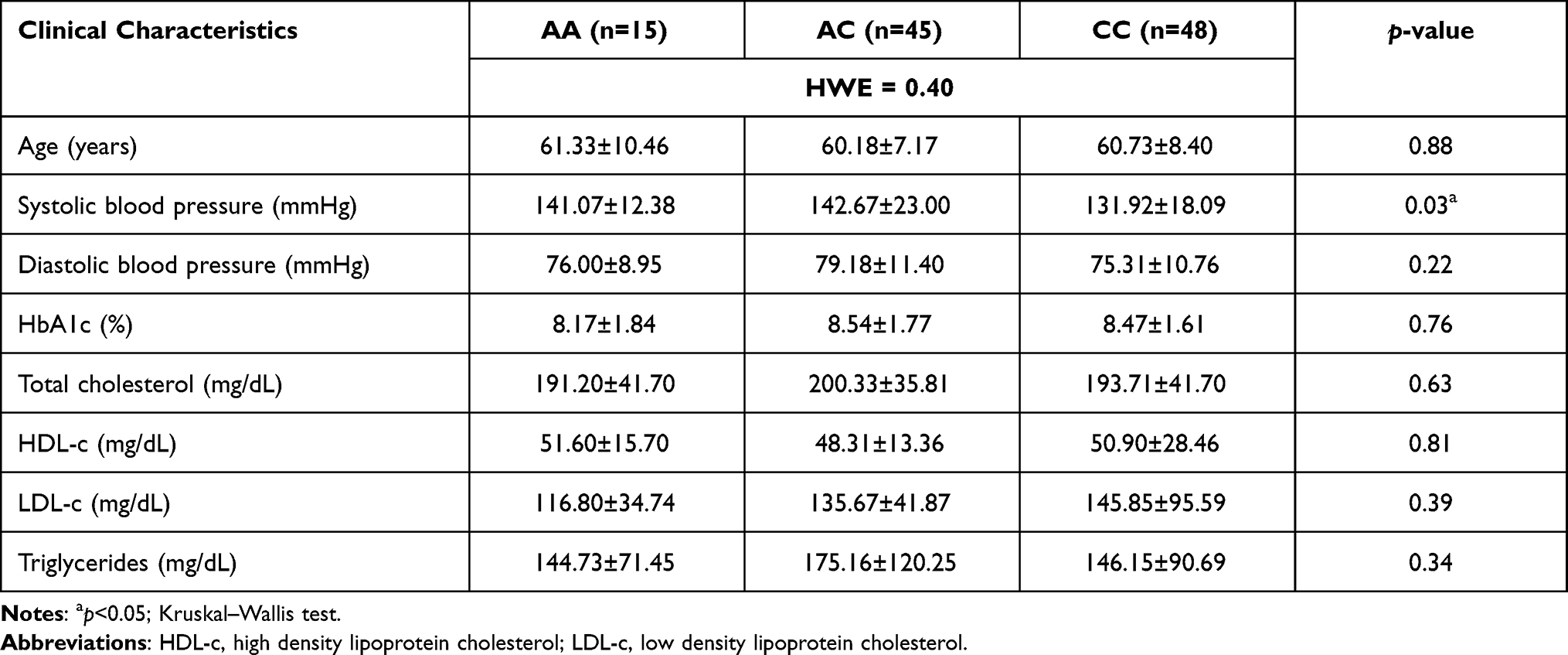 |
Table 2 Patients’ Clinical Characteristics Based on the Genotype of rs857148 |
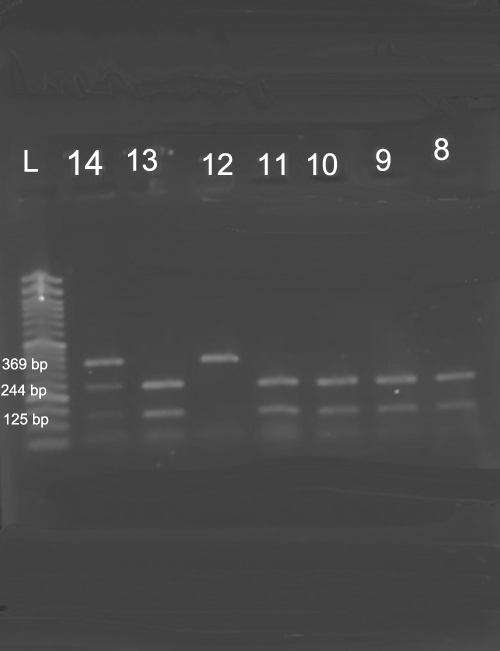 |
Figure 1 The PCR-RFLP results to determine PRKAA2 rs857148 variants. L= ladder (marker 50 bp), 8, 9, 10, 11, 13 are mutant homozygote genotype, 12 is wildtype homozygote genotype, and 14 is heterozygote genotype. |
Table 3 displays the results of multiple regression analysis to detect any relationship between genotype model and cardiometabolic parameters. Overall, we discovered a significant relationship between SNP rs857148 and HbA1c level in model 2. Subjects with CC genotype were detected to have significantly increased HbA1c levels (OR=7.12; 95% CI=1.05–48.26; p=0.04). It was asserted through recessive and allelic models where subjects with AA tended to have reduced HbA1c lower than those with AC+CC genotype, and subjects with C allele tended to have increased HbA1c levels (OR=0.15; 95% CI=0.02–0.97; p=0.047, OR=1.66; 95% CI=1.06–2.60; p=0.03, respectively). For the other cardiometabolic parameters, only total cholesterol was correlated with rs857148 calculated using model 2 (OR=1.05; 95% CI=1.01–1.10; p=0.03).
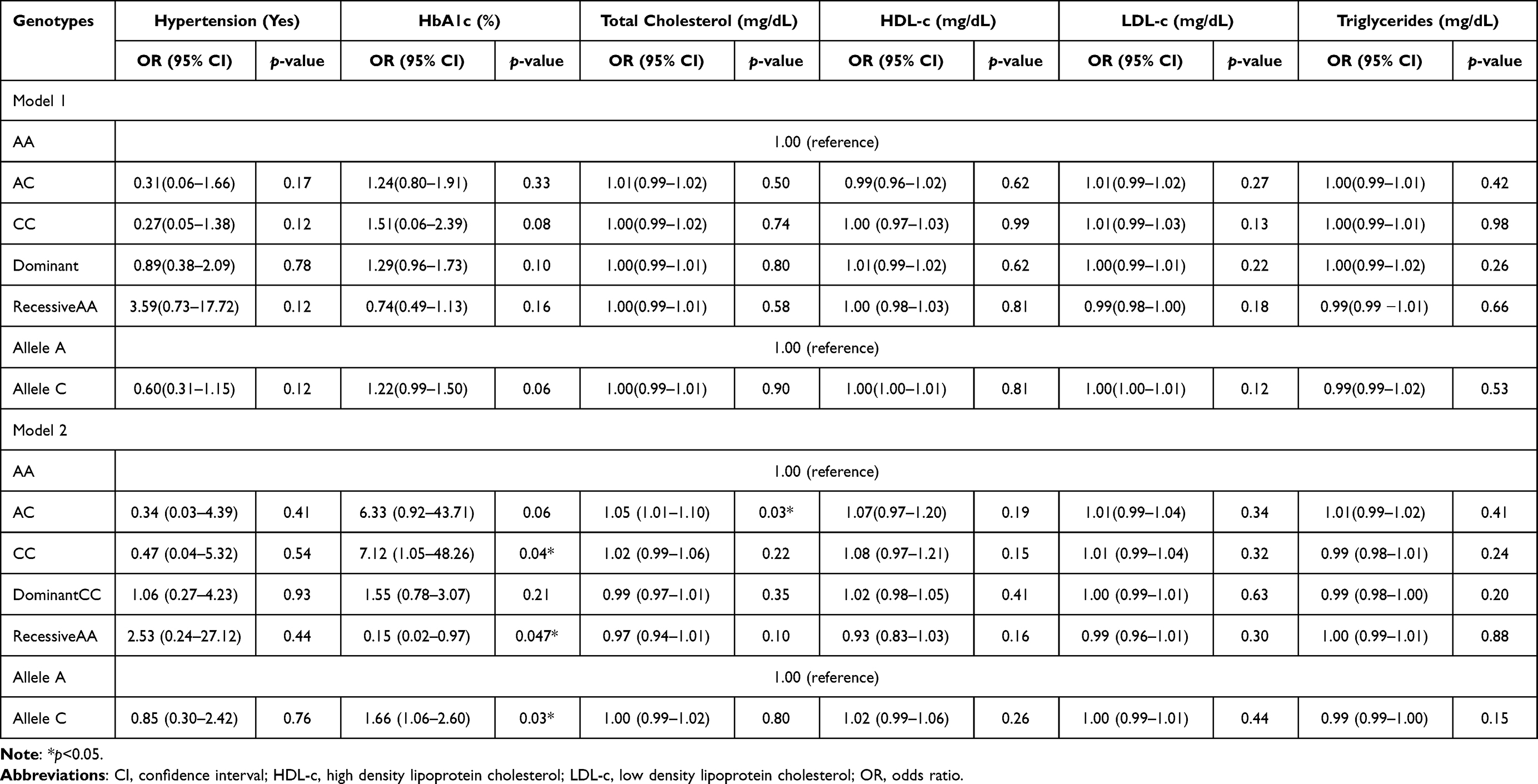 |
Table 3 Multiple Regression Analysis of rs857148 and Cardiometabolic Parameters |
Discussion
A number of studies have explored the association between a list of genetic variants and cardiometabolic parameters.34–36 To our knowledge, our study is the first study that observed the 3’ UTR variant, especially rs857148 related to cardiometabolic parameters, within the Yogyakarta population. This was the initial study related to personalized, patient-centered medicine, and we could only recruit a small number of participants. Cardiometabolic parameters in detail in this study include hypertension, HbA1c, and lipid profiles.
The association between hypertension and rs857148 in our study is not well concluded yet. This is because we found significant statistical difference only in systolic blood pressure among the rs857148 genotype, but not in diastolic blood pressure. Some studies have revealed the molecular explanation of AMPK and hypertension. AMPK activates sarcoplasmic/endoplasmic Ca2+-ATPase (SERCA), thus reducing ion Ca2+ devaluated, and the result is directly vascular smooth muscle relaxation.37 Enhancing phosphorylated AMPK could suppress the expression of the angiotensin II type 1 receptor. Therefore, AMPK activation affects blood pressure.38
Our study has observed that subjects with CC genotype and C allele tended to have increased HbA1c levels after adjusted for metformin and glimepiride dose, age, gender, and considering combination therapy. Remarkably, there are limited association studies related to rs857148. We found a study that investigated the effect of rs857148 variants on non-lung small cancer prognosis,39 but no study that discussed the effect of HbA1c, previously. However, three SNPs of PRKAA2 have been demonstrated in the previous study and it revealed no association to HbA1c.40 These discrepancies could be due to the difference in the participants’ selection. We recruited T2DM patients with less rigorous criteria than the previous study who engaged only newly diagnosed T2DM patients. Therefore, further studies are required focusing on rs857148 with a larger sample population and applying more rigorous criteria to confirm the association that we found in our study.
A study among patients with T2DM performed by Sokolova et al in 2019 reported that phosphorylated AMPK was decreasing when the blood HbA1c level was increasing.41 Luo et al in 2020 conducted a Mendelian randomization study and found that HbA1c reduction was instrumented by AMPK variants.42 AMPK activation through phosphorylation induced by ATP/AMP changes and induced by metformin. Notably, AMPK controls energy metabolism in the whole body. Biologic functions of AMPK related to HbA1c include glycolysis promotion, glucose transport enhancing, and gluconeogenesis inhibition.43,44 Therefore, it requires further investigations to confirm our findings, whether as the impact of T2DM or the effect of metformin.
Concerning the lipid profiles, no significant associations were found between rs857148 and total cholesterol, HDL-c, LDL-c, and triglyceride in model 1. Nonetheless, model 2 showed that the AC genotype had a significant correlation to total cholesterol level compared to the AA genotype. Nevertheless, only a little effect of AC was detected to total cholesterol level where the odds ratio was only 1.05. This agrees with the study conducted by Jones et al in 2006, 5 SNPs of PRKAA2 (rs1124900, rs2796516, rs2746342, rs2796498 and rs1418442) were significantly correlated to total cholesterol in a Caucasian population.45
The synthesis and disposal of cholesterol are coregulated through phosphorylation of key enzymes activated by AMPK. Those activated via sterol-regulatory element-binding protein (SREBP) and acetyl-CoA carboxylase (ACC) as the AMPK downstream.46–48 An in vivo study revealed that AMPK influence the signalling of the mevalonate pathway 3-hydroxy-3-methylglutaryl (HMG) coenzyme A (CoA) reductase (HMGCR), thus regulating the cholesterol biosynthesis.49
As mentioned above, rs857148 have not been observed related to cardiometabolic parameters, especially among T2DM patients, yet. We found one study that reported the frequency of the genotypes among health participants (as control of pancreatic cancer). The percentages of AA vs AC vs CC were 15.5%, 25.6%, and 11.3% respectively, among non-Hispanic whites as a control group.50
The clinical importance explained to us that the homozygote mutant of rs857148 could increase HbA1c than wildtype, even heterozygotes tend to increase total cholesterol. Since it is a pilot study among Indonesian subjects, it requires a larger sample to clarify our findings. However, these findings could indicate that rs857148 is worth considering as one of SNP contributing to cardiometabolic parameters, especially among patients with T2DM.
Notably, several limitations have been detected in our study. First, we could not explore whether the effect of SNP is influenced by pathologic conditions or metformin therapy because we did not collect HbA1c baseline and the information related to metformin as monotherapy or as combination therapy. Second, we did not measure physical activities, diet habits, and coexisting diseases that contribute to cardiometabolic physiologic. We have tried to minimalize these effects through multinomial logistical regression analyses. However, it would be better to apply more rigorous criteria during data collection.
Conclusions
In summary, CC genotype and C allele of rs857148 had a significant correlation to HbA1c level. Our study gives evidence that AC genotype could significantly increase total cholesterol compared to AA genotype. Since our results as a preliminary study showed significant findings, it requires further investigation with a larger sample and more rigorous criteria to determine the effect of metformin on PRKAA2 variants accurately.
Abbreviations
T2DM, type 2 diabetes mellitus; AMPK, adenosine monophosphate protein; LDL-c, low-density lipoprotein cholesterol; HDL-c, high-density lipoprotein cholesterol; SNP, single nucleotide polymorphism; UTR, untranslated region; SERCA, sarcoplasmic/endoplasmic Ca2+-ATPase; SREBP, sterol-regulatory element-binding protein; ACC, acetyl-CoA carboxylase; HMGCR, mevalonate pathway 3-hydroxy-3-methylglutaryl (HMG) coenzyme A (CoA) reductase.
Acknowledgments
We would like to thank the health care professionals at Bethesda Lempuyangwangi Hospital for assistance during data collection. This work was fully funded by The Ministry of Education, Culture, Research, and Technology of the Republic of Indonesia through the Kampus Merdeka grant (No. 50/E1/KM.05.03/2021).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rowley WR, Bezold C, Arikan Y, Byrne E, Krohe S. Diabetes 2030: insights from yesterday, today, and future trends. Popul Health Manag. 2017;20(1):6–12. doi:10.1089/pop.2015.0181
2. American Diabetes Association. Standards of medical care in diabetes. J Clin Appl Res Educ. 2020;43(1):1–212.
3. Cosentino F, Grant PJ, Aboyans V, et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J. 2020;41(2):255–323. doi:10.1093/eurheartj/ehz486
4. Khan MAB, Hashim MJ, King JK, Govender RD, Mustafa H, Al Kaabi J. Epidemiology of type 2 diabetes – global burden of disease and forecasted trends. J Epidemiol Glob Health. 2019;10(1):107. doi:10.2991/jegh.k.191028.001
5. Mihardja L, Soetrisno U, Soegondo S. Prevalence and clinical profile of diabetes mellitus in productive aged urban Indonesians. J Diabetes Invest. 2014;5(5):507–512. doi:10.1111/jdi.12177
6. Maifitrianti M, Wulandari N, Haro M, Lestari SF, Fitriani A. Glycemic control and its factor in type 2 diabetic patients in Jakarta. Indones J Clin Pharm. 2020;9(3):198–204. doi:10.15416/ijcp.2020.9.3.198
7. Cholil AR, Lindarto D, Pemayun TGD, Wisnu W, Kumala P, Puteri HHS. DiabCare Asia 2012: diabetes management, control, and complications in patients with type 2 diabetes in Indonesia. Med J Indones. 2019;28(1):47–56. doi:10.13181/mji.v28i1.2931
8. Pamungkas RA, Hadijah S, Mayasari A, Nusdin N. Factors associated with poor glycemic control among type 2 diabetes mellitus in Indonesia. Belitung Nurs J. 2017;3(3):272–280. doi:10.33546/bnj.61
9. Rashid M, Shahzad M, Mahmood S, Khan K. Variability in the therapeutic response of metformin treatment in patients with type 2 diabetes mellitus. Pakistan J Med Sci. 2019;35(1):71–76.
10. Zhou K, Donnelly L, Yang J, et al. Heritability of variation in glycaemic response to metformin: a genome-wide complex trait analysis. Lancet Diabetes Endocrinol. 2014;2(6):481–487. doi:10.1016/S2213-8587(14)70050-6
11. Bankura B, Das M, Kumar Pattanayak A, et al. Inter-patient variability in clinical efficacy of metformin in type 2 diabetes mellitus patients in West Bengal, India. J Metab Synd. 2016;5(2):198–202. doi:10.4172/2167-0943.1000198
12. Mccreight LJ, Bailey CJ, Pearson ER. Metformin and the gastrointestinal tract. Diabetologia. 2016;2016(59):426–435. doi:10.1007/s00125-015-3844-9
13. Riwu M, Subarnas A, Lestari K. The correlation of age factor, administration, and metformin dose against risk of side effect on type 2 diabetes mellitus. Indones J Clin Pharm. 2015;4(3):151–161. doi:10.15416/ijcp.2015.4.3.151
14. Minamii T, Nogami M, Ogawa W. Mechanisms of metformin action: in and out of the gut. J Diabetes Investig. 2018;9(4):701–703. doi:10.1111/jdi.12864
15. Zilov AV, Abdelaziz SI, AlShammary A, et al. Mechanisms of action of metformin with special reference to cardiovascular protection. Diabetes Metab Res Rev. 2019;35(7):e3173. doi:10.1002/dmrr.3173
16. Foretz M, Guigas B, Bertrand L, Pollak M, Viollet B. Metformin: from mechanisms of action to therapies. Cell Metab. 2014;20(6):953–966. doi:10.1016/j.cmet.2014.09.018
17. Rena G, Hardie DG, Pearson ER. The mechanisms of action of metformin. Diabetologia. 2017;60(9):1577–1585. doi:10.1007/s00125-017-4342-z
18. Mato EPM, Guewo-Fokeng M, Faadiel Essop M, Owira PMO. Genetic polymorphisms of organic cation transporters 1 (OCT1) and responses to metformin therapy in individuals with type 2 diabetes mellitus: a systematic review protocol. Syst Rev. 2018;7(1):105. doi:10.1186/s13643-018-0773-y
19. Masilela C, Pearce B, Ongole JJ, Adeniyi OV, Benjeddou M. Single nucleotide polymorphisms associated with metformin and sulphonylureas’ glycaemic response among South African adults with type 2 diabetes mellitus. J Pers Med. 2021;11(2):1–14. doi:10.3390/jpm11020104
20. Li Q, Li C, Li H, et al. STK11 rs2075604 polymorphism is associated with metformin efficacy in Chinese type 2 diabetes mellitus. Int J Endocrinol. 2017;2017:3402808. doi:10.1155/2017/3402808
21. Xiao D, Liu J-Y, Zhang S-M, et al. A two-stage study identifies two novel polymorphisms in PRKAG2 affecting metformin response in Chinese type 2 diabetes patients. Pharmgenomics Pers Med. 2021;14:745–755. doi:10.2147/PGPM.S305020
22. Kim J, Yang G, Kim Y, Kim J, Ha J. AMPK activators: mechanisms of action and physiological activities. Exp Mol Med. 2016;48(4):e224–12. doi:10.1038/emm.2016.16
23. Steinberg GR, Carling D. AMP-activated protein kinase: the current landscape for drug development. Nat Rev Drug Discov. 2019;18(7):527–551. doi:10.1038/s41573-019-0019-2
24. Tseng CH. Metformin and risk of hypertension in Taiwanese patients with type 2 diabetes mellitus. J Am Heart Assoc. 2018;7(13):e008860. doi:10.1161/JAHA.118.008860
25. Hansen CS, Lundby-Christiansen L, Tarnow L, et al. Metformin may adversely affect orthostatic blood pressure recovery in patients with type 2 diabetes: substudy from the placebo-controlled Copenhagen Insulin and Metformin Therapy (CIMT) trial. Cardiovasc Diabetol. 2020;19(1):1–10. doi:10.1186/s12933-020-01131-3
26. Lin SH, Cheng PC, Te TS, Hsu SR, Cheng YC, Liu YH. Effect of metformin monotherapy on serum lipid profile in statin-naïve individuals with newly diagnosed type 2 diabetes mellitus: a cohort study. Peer J. 2018;2018(4):e4578. doi:10.7717/peerj.4578
27. Rosenzweig JL, Bakris GL, Berglund LF, et al. Primary prevention of ASCVD and T2DM in patients at metabolic risk: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2019;104(9):3939–3985.
28. Einarson TR, Acs A, Ludwig C, Panton UH. Prevalence of cardiovascular disease in type 2 diabetes: a systematic literature review of scientific evidence from across the world in 2007–2017. Cardiovasc Diabetol. 2018;17(1):83. doi:10.1186/s12933-018-0728-6
29. Virginia DM, Wahyuningsih MSH, Nugrahaningsih DAA. Association between three variants in the PRKAA2 gene, rs2796498, rs9803799, and rs2746342, with 10-year ASCVD risk on newly diagnosed T2DM in Yogyakarta, Indonesia. Open Access Maced J Med Sci. 2021;9(A):541–547. doi:10.3889/oamjms.2021.6213
30. NCBI [homepage on the Internet]. rs857148 RefSNP Report - dbSNP - NCBI. Available from: https://www.ncbi.nlm.nih.gov/snp/rs857148#frequency_tab.
31. Zhou S, Li M, Zeng D, et al. A single nucleotide polymorphism in 3’ untranslated region of epithelial growth factor receptor confers risk for pulmonary hypertension in chronic obstructive pulmonary disease. Cell Physiol Biochem. 2015;36(1):166–178. doi:10.1159/000374061
32. Silva NNT, Santos ACS, Nogueira VM, Carneiro CM, Lima AA. 3ʹUTR polymorphism of thymidylate synthase gene increased the risk of persistence of pre-neoplastic cervical lesions. BMC Cancer. 2020;20(1):1–9. doi:10.1186/s12885-020-06811-7
33. Matoulkova E, Michalova E, Vojtesek B, Hrstka R. The role of the 3' untranslated region in post-transcriptional regulation of protein expression in mammalian cells. RNA Biol. 2012;9(5):563–576. doi:10.4161/rna.20231
34. Vardarlı AT, Harman E, Çetintaş VB, et al. Polymorphisms of lipid metabolism enzyme-coding genes in patients with diabetic dyslipidemia. Anatol J Cardiol. 2017;17(4):313–321. doi:10.14744/AnatolJCardiol.2016.7142
35. Vimaleswaran KS, Bodhini D, Jiang J, et al. Circulating adiponectin mediates the association between omentin gene polymorphism and cardiometabolic health in Asian Indians. PLoS One. 2021;16(5):e0238555. doi:10.1371/journal.pone.0238555
36. Li C, Yang Y, Liu X, Li Z, Liu H, Tan Q. Glucose metabolism-related gene polymorphisms as the risk predictors of type 2 diabetes. Diabetol Metab Syndr. 2020;12(1):1–6. doi:10.1186/s13098-020-00604-5
37. Schneider H, Schubert KM, Blodow S, et al. AMPK dilates resistance arteries via activation of SERCA and BK Ca channels in smooth muscle. Hypertension. 2015;66(1):108–116. doi:10.1161/HYPERTENSIONAHA.115.05514
38. Wei M, Gan L, Liu Z, et al. Mitochondrial-derived peptide mots-c attenuates vascular calcification and secondary myocardial remodeling via adenosine monophosphate-activated protein kinase signaling pathway. Cardiorenal Med. 2020;10(1):42–50. doi:10.1159/000503224
39. Lee YH, Do SK, Lee SY, et al. TSC2 genetic variant and prognosis in non-small cell lung cancer after curative surgery. Thorac Cancer. 2019;10(2):335–340. doi:10.1111/1759-7714.12951
40. Virginia DM, Wahyuningsih MSH, Nugrahaningsih DAA. PRKAA2 variation and the clinical characteristics of patients newly diagnosed with type 2 diabetes mellitus in Yogyakarta, Indonesia. Asian Biomed. 2021;15(4):161–170. doi:10.2478/abm-2021-0021
41. Sokolova LK, Pushkarev VM, Belchina YB, Pushkarev VV, Vatseba TS, Tronko ND. Association of 5ʹAMP-activated protein kinase activity with disease duration and HbA1c content in leukocytes in diabetic patients. Int J Endocrinol. 2019;15(1):23–26.
42. Luo S, Schooling CM, Wong ICK, Au Yeung SL. Evaluating the impact of AMPK activation, a target of metformin, on risk of cardiovascular diseases and cancer in the UK Biobank: a Mendelian randomisation study. Diabetologia. 2020;63(11):2349–2358. doi:10.1007/s00125-020-05243-z
43. Dutta D, Kalra S, Sharma M. Adenosine monophosphate-activated protein kinase-based classification of diabetes pharmacotherapy. J Postgrad Med. 2017;63(2):114–121. doi:10.4103/0022-3859.191007
44. Coughlan KA, Valentine RJ, Ruderman NB, Saha AK. AMPK activation: a therapeutic target for type 2 diabetes? Diabetes Metab Syndr Obes Targets Ther. 2014;7:241–253.
45. Spencer-Jones NJ, Ge D, Snieder H, et al. AMP-kinase α2 subunit gene PRKAA2 variants are associated with total cholesterol, low-density lipoprotein-cholesterol and high-density lipoprotein-cholesterol in normal women. J Med Genet. 2006;43(12):936–942. doi:10.1136/jmg.2006.041988
46. Kinaan M, Ding H, Triggle CR. Metformin: an old drug for the treatment of diabetes but a new drug for the protection of the endothelium. Med Princ Pract. 2015;24(5):401–415. doi:10.1159/000381643
47. Fullerton MD. AMP-activated protein kinase and its multifaceted regulation of hepatic metabolism. Curr Opin Lipidol. 2016;27(2):172–180. doi:10.1097/MOL.0000000000000273
48. Han Y, Hu Z, Cui A, et al. Post-translational regulation of lipogenesis via AMPK-dependent phosphorylation of insulin-induced gene. Nat Commun. 2019;10(1):1–13.
49. Loh K, Tam S, Murray-Segal L, et al. Inhibition of adenosine monophosphate-activated protein kinase-3-hydroxy-3-methylglutaryl coenzyme a reductase signaling leads to hypercholesterolemia and promotes hepatic steatosis and insulin resistance. Hepatol Commun. 2019;3(1):84–98. doi:10.1002/hep4.1279
50. Tang H, Dong X, Hassan M, Abbruzzese JL, Li D. Body mass index and obesity- and diabetes-associated genotypes and risk for pancreatic cancer. Cancer Epidemiol Biomarkers Prev. 2011;20(5):779–792. doi:10.1158/1055-9965.EPI-10-0845
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.