Back to Journals » Cancer Management and Research » Volume 11
Single-Fraction Radiotherapy (SFRT) For Bone Metastases: Patient Selection And Perspectives
Authors Loi M, Nuyttens JJ, Desideri I ![]() , Greto D, Livi L
, Greto D, Livi L
Received 16 July 2019
Accepted for publication 22 October 2019
Published 5 November 2019 Volume 2019:11 Pages 9397—9408
DOI https://doi.org/10.2147/CMAR.S186630
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Antonella D'Anneo
Mauro Loi,1 Joost J Nuyttens,2 Isacco Desideri,1 Daniela Greto,1 Lorenzo Livi1
1Radiotherapy Department, University of Florence, Florence, Italy; 2Radiotherapy Department, Erasmus MC Cancer Center, Rotterdam, The Netherlands
Correspondence: Mauro Loi
Radiotherapy Department, University of Florence, L.go Brambilla 3, Florence 50100, Italy
Email [email protected]
Abstract: Bone metastases are a frequent and important source of morbidity in cancer patients. Stereotactic body radiation therapy (SBRT) is an established treatment option for local control and pain relief of bone metastases, and it is increasingly used as upfront treatment, postoperative consolidation or salvage treatment after prior RT. However, heterogeneity of dose schedules described in literature represents a severe limitation in the definition of the role of SBRT as a standard of care. No consensus is available on the use of single versus multiple fraction SBRT for bone metastases. Advantages of single-fraction SBRT include shorter overall duration of treatment, absence of inter-fraction uncertainty, improved compliance, theoretical increased efficacy, and lower costs. However, caution has been advised due to reports of severe late toxicities, in particular, vertebral collapse fracture (VCF). The aim of this paper is to review dose fractionation and indications for the management of bone metastases using SBRT.
Keywords: SBRT, stereotactic radiotherapy, radiosurgery, bone metastases, spine, non-spine
Introduction
Metastatic bone involvement is a frequent occurrence in cancer patients. It is present in approximately 15 to 70% of advanced stage cancer patients according to primary tumor localization, with an estimated incidence of 100,000 cases per year only in the United States.1,2 Refractory pain is found in 70% of patients with bone metastases.1 Uncontrolled bone metastases (BM) are an important source of morbidity in cancer patients, resulting in pathologic fractures, hypercalcemia, and neurologic impairment.3 Bone metastases-related complications, collectively defined as Skeletal-Related Events (SRE), represent a serious threat to well-being and quality of life in cancer patients.4 Moreover, the socio-economic burden of this condition is also of primary concern, since monthly treatment cost raised from €190 in asymptomatic patients to €4672 in patients with SRE in a prospective multicentric cohort.5 Conventional radiotherapy (CRT), delivering a range of radiation doses between 8 Gy in 1 fraction to 30 Gy in 10 fractions, is a mainstay of BM management, providing prompt symptom palliation with a benign toxicity profile, and resort to other surgical or medical treatment modalities does not obviate the use of radiotherapy.6 However, long-term results are often disappointing, showing complete pain response only in 24% of patients, with no particular benefit of one dose schedule over the other.7 Lack of symptom control may also lead to high retreatment rates, in particular following single fraction radiotherapy, though no benefit was found in over 40% of patients regardless of initial response to treatment or dose schedule.8 Achievement of durable disease and symptom control is of particular interest, due to constant improvement in survival among cancer patients,9 most notably in specific subsets such as oligometastatic patients who experience extended survival compared to polymetastatic patients.10 Stereotactic body radiation therapy (SBRT), defined as delivery of high dose per fraction in a short treatment course, allows the administration of potentially ablative radiation doses to the core of target metastases with a steep dose gradient that minimizes radiation exposure of neighboring critical organs. For these reasons, SBRT is an established treatment option for bone metastases as primary treatment, and, particularly in case of spinal involvement, as postoperative consolidation or salvage treatment after prior RT.6 In comparison with conventional palliative radiotherapy, delivery of highly biologically effective radiation doses with SBRT may result in improved tumor control and fast symptom palliation.11 Results from the exploratory trial IRON-1 favors 24 Gy single-fraction SBRT over 30 Gy in 10 fractions three-dimensional radiotherapy (3DRT) in terms of pain relief,11 and randomized phase III studies12,13 are ongoing to assess superiority of SBRT over CRT in terms of tumor control, palliation of symptoms, and quality of life. Of note, SBRT could be of particular interest in oligometastatic patients, who may draw further benefit in survival and systemic therapy-free survival from reduction of disease burden with the use of locally ablative therapies:14 pathologic assessment of operated tumor specimen after SBRT proved the absence of residual viable tumor in over 80% of cases, thus confirming the reliability of instrumental assessment and demonstrating that SBRT is an ablative procedure in the majority of cases.15 However, heterogeneity of dose schedules described in literature represents a severe limitation in the definition of the role of SBRT as a standard of care. Comparable to CRT, no consensus is available on the use of single versus multiple fraction SBRT for bone metastases. Theoretical advantages of single-fraction radiotherapy over multifractionated SBRT include shorter overall duration of treatment, absence of inter-fraction uncertainty, improved compliance, and lower costs.16 However, while historical series mainly reported promising results following single fraction irradiation, late occurrence of severe toxicities (particularly in spinal treatment) motivated an increasingly widespread use of multi-fractionated schedules in an attempt to dampen toxicity. It is unclear whether fractionation may influence clinical outcome of patients treated with SBRT with regard to time to symptom palliation, duration of pain control, need for a second radiotherapy course, and risk of treatment-induced toxicities. This has important implications in clinical practice, since appropriate choice of treatment schedule should be warranted in function of clinical presentation of patients eligible for SBRT. The aim of this paper is to review dose fractionations and indications for the management of bone metastases using SBRT. A PubMed search was performed on March 7th, 2019 using the terms ‹‹‹(stereotactic OR SBRT OR radiosurgery) AND (bone OR spinal OR spine OR vertebral OR osseous) AND metastases››, resulting in the identification of 767 records. Screening for appropriateness was carried out by 2 independent author teams (ML/ID, DG/LL) in order to identify relevant papers. For the purpose of this study, reviews, dose planning studies or case reports were excluded, and articles focusing on unrelated topics (including re-irradiation following prior conformal/stereotactic radiotherapy, post-surgery consolidation radiotherapy, miscellaneous sites including extraosseous localizations) were, likewise, removed. In case of disagreement, a final decision was formulated with a third author (JJN). Full-text papers assessed for eligibility and included for review are listed in Tables 1 and 2.
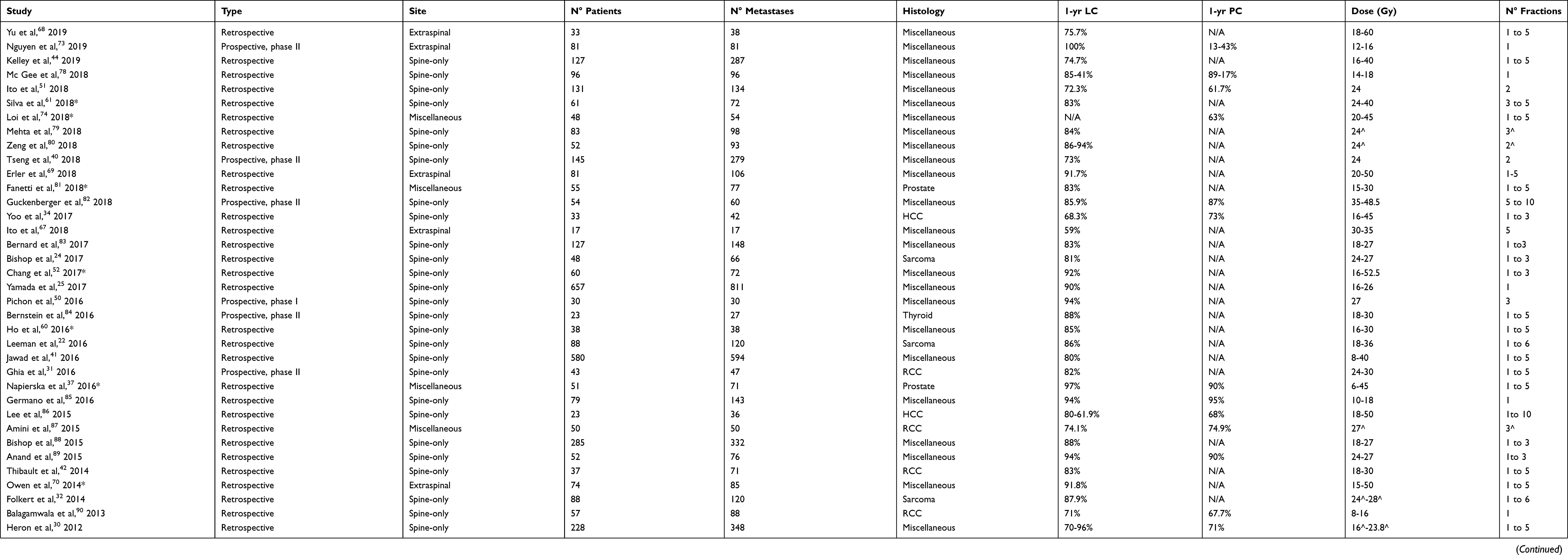 |
Table 1 Selected Studies On The Use Of Stereotactic Radiotherapy For Bone Metastases, Reporting Data On Efficacy Endpoints |
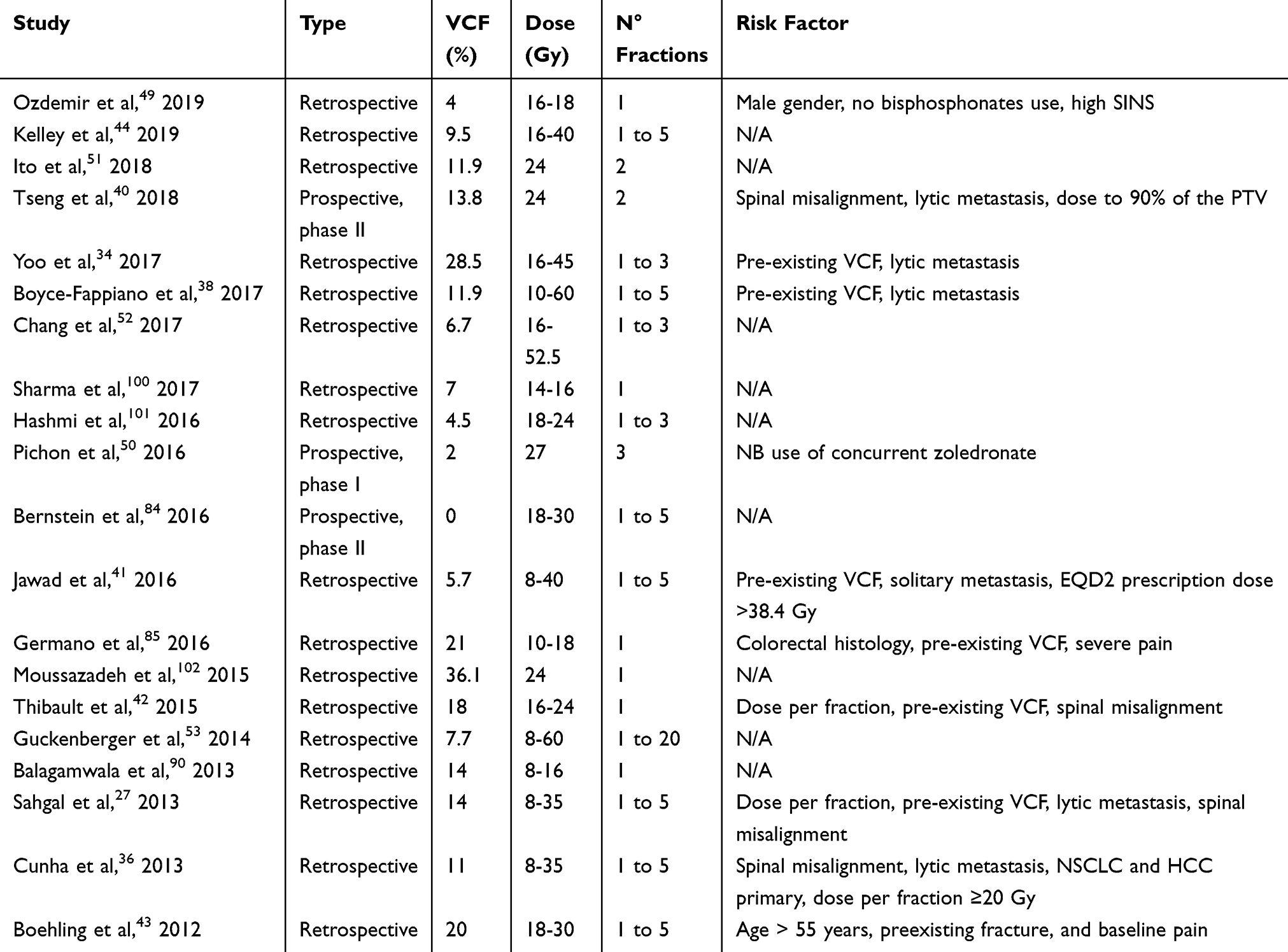 |
Table 2 Selected Studies On The Use Of Stereotactic Radiotherapy For Bone Metastases, Reporting Data On VCF Incidence And Predictors |
Spinal Metastases
General Considerations
Axial skeleton is the most common site of secondary localization, accounting for 40% of metastatic bone sites.17 Use of SBRT in the management of painful spinal metastases was tested as early as the mid-1990s.18 SBRT was initially intended as a single 8-Gy boost to the gross tumor volume following conventional palliative radiotherapy, in order to maximize dose to the tumor while respecting dose constraints to the spinal cord: this resulted in promising rates of pain palliation with no additional acute toxicity.19 Upfront use of SBRT in previously non-irradiated lesions was prospectively validated by Garg et al.20 Feasibility of dose escalation to 16 Gy was confirmed in the phase II trial RTOG 0631.13 Interestingly, precise tumor targeting did not result in increased rate of marginal failures: since one of the major arguments against the use of SBRT was the omission of the adjacent vertebral level, this finding justified the treatment of the involved spine only as previously reported by Ryu et al,21 who reported a relapse rate of <5% in the immediately adjacent vertebrae. This was confirmed by Leeman et al, who showed involvement of the adjacent vertebra in 2% of cases.22 A subsequent, large prospective cohort study23 investigated the clinical outcome of single-fraction (20–25 Gy) SBRT in 500 spinal metastases from mixed primary tumors, confirming excellent pain control in symptomatic tumors (290/336, 86%) and neurologic impairment relief (27/32, 84%) at a median follow-up of 21 (3–53) months. Modern series of SBRT shows promising rates of 1-year local control between 60 and 95% and 1-year symptom control in 43 to 90% of patients (Table 1 and Figure 1). Irrespective of the use of single or multifractionated SBRT, a dose-response relationship has been highlighted: superior local control was found in sarcoma metastases receiving a BED > 48 Gy,24 while, in another report on spinal metastases of miscellaneous histology, local failure rate did not exceed 2% in patients receiving a dose of at least 23.56 Gy EQD2 to 95% of the Gross Tumor Volume.25 Similar considerations also apply to symptom relief: in the study by Jahaveri et al, renal cell carcinoma patients (RCC) treated with a fractionated schedule delivering a BED > 85 Gy achieved faster and more durable pain control26 than patients receiving inferior cumulative doses.
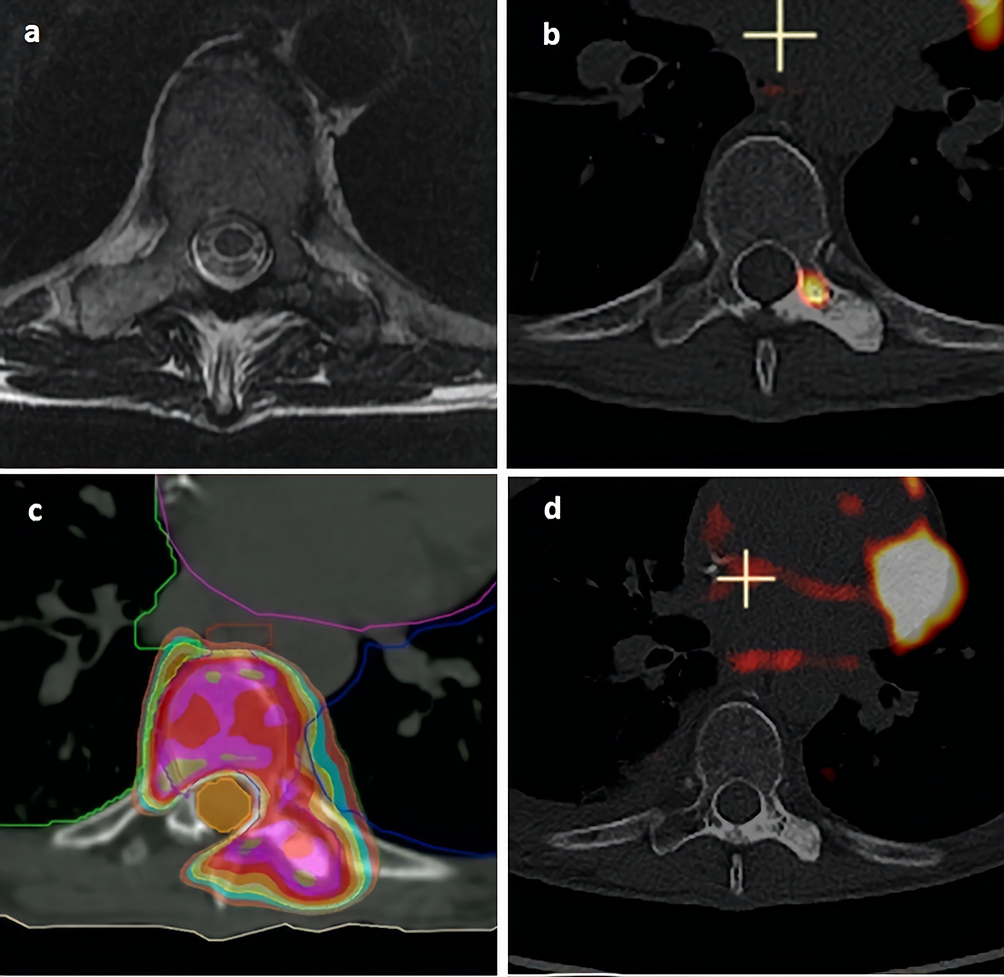 |
Figure 1 A 68 year old woman affected by metastatic breast cancer was referred for SBRT of a painful metastasis of the left transverse pedicle of the 8th thoracic vertebra. Notes: (A) MRI view prior to SBRT. (B) 18FDG-PET view prior to SBRT. (C) Dose planning prior to administration of a single fraction of 18 Gy to the 80% isodose line (color wash deep orange, light blue, yellow, gold, purple, red and olive corresponding respectively to 14, 15, 16, 17, 18, 19, 20 and 21 Gy), resulting in conformal dose distribution sparing the spinal canal (light orange). (D) 18FDG-PET view 6 months after SBRT, showing stable mineralization of the treated area and metabolic complete response. Acute toxicity consisted of G2 dysphagia due to proximity of the esophagus. No late toxicity was observed at 1 year, while complete pain control was obtained. |
Single Or Multifractionated Spine SBRT?
While dose escalation might prove beneficial, careful attention has been paid to attain clinically active doses while respecting healthy tissues' tolerance constraints. In particular, use of single fraction SBRT, the historical treatment modality, has been questioned due to reported incidence of vertebral collapse fracture (VCF) in up to 39% of cases after a single dose of 24 Gy or higher,27 thus advocating for the use of fractionated schedules in an attempt to reduce severe adverse events while maintaining effective cumulative dose. However, optimal fractionation schedule allowing acceptable trade-off between efficacy and safety is a matter of debate. It has been speculated that radiobiological effects of a single radiation dose >15-20Gy may involve additional biological activity compared to lower fractionated dose, including asmase/ceramide pathway-related endothelial damage.28 Pathologic assessment of resected metastases, preoperatively treated with a single 18 Gy fraction, showed significant onset of tumor necrosis and decrease in vessel density within 24 hrs.29 This observation supports the hypothesis that more pronounced tumoricidal action, as well as osteoradionecrosis, may occur after single fraction SBRT following microvascular damage: hence, theoretical superior efficacy of single-fraction SBRT and increased risk of local adverse events may represent two sides of the same coin. However, in clinical practice no formal evidence is available.
On one hand, several papers comparing different SBRT dose schedules suggest significantly higher pain control rates30 and local control rates31,32 for single-fraction SBRT compared to multiple fraction. Nevertheless, fractionated regimens employed in these studies may not be as dose-intensive as single fraction SBRT. For example, in the study by Ghia et al,31 24 Gy in a single fraction proved superior to 27 Gy in 3 fractions and 30 Gy in 5 fractions in terms of local control in spinal metastases from RCC: however, using an alpha/beta ratio of 10, this translated into very different corresponding BED of 81.6, 51.3, and 48 Gy, respectively. Hence, use of single fraction was associated with a nearly 1.5–2 fold BED increase as compared to multifractionated schedules, which may possibly explain superior outcome in this group of patients; of note, follow-up at 5 years did not show increased toxicity in patients receiving single-fraction SBRT, and global incidence of VCF was 14%.33 Interestingly, in the paper by Heron et al,30 a median single dose of 16 Gy (corresponding to a BED=41.6 Gy), while providing faster pain relief, resulted in inferior local control as compared to a median 23.8–25 Gy in 4–5 fractions (corresponding to BED 37.1–38.4). In a large cohort by Bishop et al, local relapse was correlated to inadequate tumor coverage independently of the fractionation, advising a GTV Dmin above 14 Gy in 1 fraction and 21 Gy in 3 fractions.24 It should be eventually pointed out that, among the previously cited studies, superior tumor control of single fraction schedule was assessed in subsets of patients affected by radio-resistant primary tumors such as sarcoma and RCC,31,32 while a single fraction of 14–18 Gy was insufficient to overcome radioresistance in hepatocellular carcinoma compared to other histotypes:34 therefore, though tantalizing, the hypothesis of superior activity of single-fraction SBRT according to tumor histology cannot be definitely ruled out.
On the other hand, dose per fraction to the vertebral body has been correlated to VCF and, most interestingly, the use of single fraction doses as high as ≥20 Gy have been questioned as a major risk factor. Incidence of VCF (de novo or progression of existing fracture) varies greatly among different authors (Table 2), and may occur within 5 years from the treatment.35 Following reports by Sahgal et al, showing dose per fraction ≥20 and as ≥24 as an independent risk factor for VCF (HR: 4.9 and 5.2, respectively), caution has been advised concerning the use of single fraction SBRT for spinal metastases.36 Since SBRT schedules are not dose-equivalent, it is unclear whether VCF risk is strictly dependent on dose per fraction rather than cumulative dose: Jawad et al reported higher VCF incidence for a 2-Gy equivalent dose (EQD2) >38.4 Gy (corresponding approximately to 17, 24, and 29 Gy in 1, 3 and 5 fractions, respectively) independently of the use of a single or multiple fraction.37 However, to avoid oversimplification, it should be pointed out that VCF is a complex entity, that may result from a certain number of predisposing factors other than dose schedule. Lytic metastases show higher risk of VCF,27,34,36,38 and automatic calculation of the lytic component volume has been tested to predict the risk of VCF.39 Spinal misalignment has also been frequently found in patients experiencing VCF,27,36,40 as well as pre-existing VCF.27,34,40–43 Put together, all these factors may participate in global mechanical instability of the vertebra, that is of particular concern since it has been correlated both to VCF onset and to local failure: interestingly, Kelley et al reported superior local control after single-fraction SBRT with a median dose of 16 (16–20) Gy as compared to hypofractionated SBRT.44 Mechanical instability of vertebra should be constantly addressed in patients potentially eligible for SBRT in order to select candidates for this option and predict the risk of complications. Consensus statement led to the development of the Spinal Instability Neoplastic Score (SINS),45 encompassing both clinical and radiological findings: a subset analysis from a prospective phase II trial confirmed the performance of SINS in predicting the onset of VCF after spine SBRT, showing a 2 year-VCF rate of 31.6% in patients with high (7–12) SINS score compared to 7.1% in patients with low (<7) SINS score.46 Careful spinal instability assessment may guide the choice to consider prophylactic surgical stabilization or cement augmentation after SBRT, that has been successfully practised in CRT47 and prospectively evaluated in a phase II trial.48 Besides mechanical instability, other predictors of VCF have been analyzed. Concurrent or prior biphosphonate administration, in particular for a treatment interval of at least 6 months, may prevent the onset of VCF:49 use of prophylactic zoledronic acid injection before hypofractionated SBRT has been tested in a phase I trial, reporting a 2% incidence of VCF.50 A protective effect of obesity27 and prior irradiation42 has also been suggested.
Apart from VCF, no other toxicity seems to be influenced by SBRT schedule and few data are available due to low incidence of late complications. In particular, radiation myelopathy is exceedingly rare, presenting in less than 1% of cases in current literature:35,51–53 interestingly, only a maximum point dose (Dmax) corresponding to a BED> 110 Gy to spinal cord or cauda equina was correlated to neurologic impairment, independently of the dose per fraction.35 Conversely, esophageal toxicity is a frequent occurrence following chest SBRT and may be life-threatening in a small but significant fraction of patients,54 leading to fatal outcome in rare cases due to massive bleeding or fistula.55–57 Interestingly, multiple dose constraints have been proposed, showing significant inconsistencies among authors: for example, suggested Dmax extrapolated from clinical studies for esophagus single-fraction SBRT ranged between 15.4 and 22 Gy.55,56 It is likely that other variables, including organ motion, individual radiosensitivity, prior chemotherapy and iatrogenic manipulation may influence the incidence of esophageal toxicity.54
Spine SBRT In Oligometastatic Disease
Oligometastatic patients represent a subset of metastatic patients with low disease burden (inferior or equal to 3–5 metastases) potentially suitable for focal treatment in order to obtain control of the macroscopic site of disease and theoretically prolong survival.58 Focusing on metastatic spinal involvement, a recent prospective cohort confirmed a significant survival advantage (+22% at 6 months) in patients with oligometastatic versus polymetastatic (>5 lesions) involvement, regardless of treatment modalities. SBRT has been widely applied in this setting in order to maximize disease control and symptom relief.59 In all the available experiences (Table 1), the authors report excellent local control rates in oligometastatic patients with spinal involvement treated by SBRT, translating to 62–67% of patients achieving durable systemic-progression free survival at 1-year with modest incidence of severe adverse events.52,60 Interestingly, superior local control was shown in oligometastatic patients receiving hypofractionated (3 to 5 fractions) SBRT to spinal metastases as compared to polymetastatic patients. This may be explained by elicitation of background immune response toward tumor cells, or by retention of a less aggressive phenotype in oligometastases.61 Therefore, it could be speculated that dose fractionation may be involved in the modulation of the local effect of SBRT through interaction with tumor-host synergy;62 however, use of heterogeneous dose schedule in these limited experiences do not allow further analysis. Hence, no data are available concerning the optimal dose schedule in oligometastatic patients, though longer expected survival implies a more stringent trade-off between risk of late toxicity and need for durable local control. In order to guide the choice of the clinician, multiple prognostic tools integrating clinical variables (PRISM, NOMS) in a decision framework are currently available.63-65
Extra-Spinal Bone Metastases
General Considerations
Use of SBRT in non-spinal bone metastases has been inconsistently described. First, there is a scarcity of literature specifically addressing SBRT for extra-spinal disease, since most studies report miscellaneous data from spinal and non-spinal treatment: however, treatment efficacy seems comparable with 1-year LC and pain control rate of 75–100% and 13–100% (Table 1). Secondly, studies addressing extra-spinal bone SBRT frequently include heterogeneous bone location: hence, choice of cumulative dose and schedule fractionation may be influenced to a variable degree by dose tolerance of neighboring critical structures as compared to spinal SBRT, where radiation myelopathy is commonly accepted as the main dose-limiting toxicity.
Consensual definition of target volume is still lacking in extraspinal metastases delineation, as opposed to spinal SBRT where a consensus statement has been reached following reports on pattern of failure and integration of MRI.66 To our knowledge, only a recent paper by Ito et al67 examined pattern of failure in 17 coxal metastases treated with a hypofractionated schedule (30–35 Gy in 5 fractions) on an MRI-delineated Gross Treatment Volume (GTV) plus a 5–10 mm expansion to a Clinical Treatment Volume, showing a 41% marginal/out of field relapse incidence occurring at an average 3.4 cm distance (range 1.5–5.5) from the closer edge of the treated tumor: hence, use of a Clinical Target Volume expansion has been questioned.
Finally, heterogeneity in the study end-points (symptom relief or local control) may indirectly reflect use of different criteria for patient selection, in particular with regard to the decision to allocate patients to SBRT rather than conventionally fractionated radiotherapy: for example, SBRT irradiation of oligometastatic or oligoprogressive non-symptomatic metastasis may underlie a positive bias due to inclusion of a population subset characterized by a more favorable outcome. Interestingly, only a recent retrospective cohort by Yu et al68 identified patients according to the treatment intent: despite evident differences in overall survival, no difference in local control was found between oligometastatic, oligoprogressive, and polymetastatic patients treated at the dominant site of progression, showing a 1-year LC rate of 75.7%. It is noteworthy that local control rate differed according to criteria for response assessment, resulting in a 11.1% discrepancy between MDA and RECIST criteria, and a more specific correlation between local control rate according to MDA and improved survival was found.
Single Or Multifractionated Bone SBRT?
Since most studies on extra-spinal SBRT delivered miscellaneous dose regimens, dose fractionation has not been specifically addressed in current literature either in regard to tumor and pain control or expected toxicity. Interestingly, use of single fraction SBRT (15–24 Gy) varies between 1.869 and 52%70 in retrospective cohorts.
Underutilization of single fraction SBRT in this setting may result from reluctance among praticians to prescribe single-fraction CRT in particular in long-surviving patients, following widespread opinion that single fraction would expose to increased toxicity, inadequate efficacy, and higher retreatment rate. However, it is currently accepted that single fraction radiotherapy yields the same efficacy as multiple fraction CRT even in patients with favorable expected survival.71 Moreover, delivering higher dose to the target may further improve the therapeutic ratio of single fraction CRT.72 Most interestingly, a recent phase II trial73 comparing single-fraction SBRT to multifraction CRT, reported significantly higher rates of pain response both at early (2 weeks) and late (9 months) evaluation. Interestingly, according to a recent study from our group, no specific SBRT dose fractionation was correlated to pain control, that was mostly influenced by patient-related features identified with the use of validated tools such as the ECS‐CP.74 Concerning toxicity, severe adverse events correlated with bone irradiation included fracture and pain flare (defined as acute onset or exacerbation of pain in relation to radiotherapy).75 Cumulative incidence of pain flare ranging between 10 and 68%70,75,76 has been reported, with single‐fraction dose regimen76 and lack of steroid pretreatment77 being the main predictors. In our experience, pain flare occurred following 34% of SBRT treatments74 but no variable was associated with its onset.
Owen et al described the occurrence of pain flare and fractures in 10% and 2% of 7 cases with a median dose of 24 Gy in one fraction.70 Erler et al69 reported an overall fracture incidence of 8.5%, significantly affecting female patients and lytic metastases: however single-fraction SBRT accounted only for 1.8% of treatment.
Regarding the previously cited prospective trial, no differences in toxicity were shown in particular concerning bone fracture, occurring in 1.2% of patients in the single-fraction SBRT arm.
Conclusion
Stereotactic Body Radiotherapy (SBRT) is established as a safe and effective treatment option for metastatic bone disease, resulting in prompt pain relief and excellent disease control with acceptable toxicity: its applications range from upfront treatment of painful metastases to re-irradiation of previously treated sites in proximity to dose-limiting organs, and to extend disease remission in oligometastatic patients. Despite extensive literature, no definitive conclusion can be drawn on the superiority of one regimen over another: in particular it is unclear whether the use of multifractionated versus single fraction SBRT schedule might ensure a better therapeutic ratio between disease control and adverse event risk.
In spinal metastases, while satisfying clinical efficacy is found with doses as low as 12–16 Gy in a single fraction, a dose-response relationship has been highlighted that may favor single-fraction schedules (in particular in radioresistant histotypes), possibly through theoretical exploitation of alternative radiobiological effects involving vascular apoptosis, occurring at >10-15 Gy/fraction. However, the use of doses per fraction ≥ 20 Gy may increase the risk of severe adverse events such as vertebral collapse fracture, in particular in high risk patients (extended lytic component, spinal misalignment, prior fracture): caution is advised in the use of single fractions, that may be of interest in patients with low spinal instability (SINS) score and/or in combination with vertebroplasty. Conversely, myelopathy is an infrequent event that may occur at high total doses (BED> 110 Gy) independently from fractionation scheme. In extra-spinal bone SBRT, scarce data are available: however, a recent prospective trial suggests that, despite relative underutilization, single fraction SBRT may not be burdened by higher toxicity rates and proved prospectively superior to multifractionated CRT in terms of pain relief. Multiple randomized trials (NCT02608866; NCT03028337) are currently comparing single versus multifraction SBRT.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bruera ED, Portenoy RK, eds, Cancer Pain: Assessment and Management. New York (NY): Cambridge University Press; 2003:413–428.
2. Smith HS. Painful osseous metastases. Pain Physician. 2011;14(4):E373–403.
3. Mundy GR. Metastasis to bone: causes, consequences and therapeutic opportunities. Nat Rev Cancer. 2002;2(8):584–593. doi:10.1038/nrc867
4. Weinfurt KP, Li Y, Castel LD, et al. The significance of skeletal-related events for the health-related quality of life of patients with metastatic prostate cancer. Ann Oncol. 2005;16(4):579–584. doi:10.1093/annonc/mdi122
5. Decroisette C, Monnet I, Berard H, et al. Epidemiology and treatment costs of bone metastases from lung cancer: a French prospective, observational, multicentre study (GFPC 0601). J Thorac Oncol. 2011;6(3):576–582. doi:10.1097/JTO.0b013e318206a1e3
6. Lutz S, Balboni T, Jones J, et al. Palliative radiation therapy for bone metastases: update of an ASTRO evidence-based guideline. Pract Radiat Oncol. 2017;7(1):4–12. doi:10.1016/j.prro.2016.08.001
7. Rich SE, Chow R, Raman S, et al. Update of the systematic review of palliative radiation therapy fractionation for bone metastases. Radiother Oncol. 2018;126(3):547–557. doi:10.1016/j.radonc.2018.01.003
8. Huisman M, van Den Bosch MA, Wijlemans JW, et al. Effectiveness of reirradiation for painful bone metastases: a systematic review and meta-analysis. Int J Radiat Oncol Biol Phys. 2012;84(1):8–14. doi:10.1016/j.ijrobp.2011.10.080
9. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69(1):7–34. doi:10.3322/caac.v69.1
10. Barzilai O, Versteeg AL, Sahgal A, et al. Survival, local control, and health-related quality of life in patients with oligometastatic and polymetastatic spinal tumors: a multicenter, international study. Cancer. 2019;125(5):770–778. doi:10.1002/cncr.31870
11. Sprave T, Verma V, Förster R, et al. Randomized phase II trial evaluating pain response in patients with spinal metastases following stereotactic body radiotherapy versus three-dimensional conformal radiotherapy. Radiother Oncol. 2018;128(2):274–282. doi:10.1016/j.radonc.2018.04.030
12. van der Velden JM, Verkooijen HM, Seravalli E, et al. Comparing conVEntional radiotherapy with stereotactIC body radiotherapy in patients with spinAL metastases: study protocol for an randomized controlled trial following the cohort multiple randomized controlled trial design. BMC Cancer. 2016;16(1):909. doi:10.1186/s12885-016-2947-0
13. Ryu S, Pugh SL, Gerszten PC, et al. RTOG 0631 phase 2/3 study of image guided stereotactic radiosurgery for localized (1-3) spine metastases: phase 2 results. Pract Radiat Oncol. 2014;4(2):76–81. doi:10.1016/j.prro.2013.05.001
14. Palma DA, Olson R, Harrow S, et al. Stereotactic ablative radiotherapy versus standard of care palliative treatment in patients with oligometastatic cancers (SABR-COMET): a randomised, phase 2,open-label trial. Lancet. 2019;393(10185):2051–2058. doi:10.1016/S0140-6736(18)32487-5
15. Katsoulakis E, Laufer I, Bilsky M, et al. Pathological characteristics of spine metastases treated with high-dose single-fraction stereotactic radiosurgery. Neurosurg Focus. 2017;42(1):E7. doi:10.3171/2016.10.FOCUS16368
16. van Den Hout WB, van der Linden YM, Steenland E. Single- versus multiple-fraction radiotherapy in patients with painful bone metastases: cost-utility analysis based on a randomized trial. J Natl Cancer Inst. 2003;95(3):222–229. doi:10.1093/jnci/95.3.222
17. Klimo P
18. Hamilton AJ, Lulu BA, Fosmire H, Stea B, Cassady JR. Preliminary clinical experience with linear accelerator-based spinal stereotactic radiosurgery. Neurosurgery. 1995;36(2):311–319. doi:10.1227/00006123-199502000-00010
19. Ryu S, Fang Yin F, Rock J, et al. Image-guided and intensity-modulated radiosurgery for patients with spinal metastasis. Cancer. 2003;97(8):2013–2018. doi:10.1002/cncr.11296
20. Garg AK, Shiu AS, Yang J, et al. Phase 1/2 trial of single-session stereotactic body radiotherapy for previously unirradiated spinal metastases. Cancer. 2012;118(20):5069–5077. doi:10.1002/cncr.27530
21. Ryu S, Rock J, Rosenblum M, Kim JH. Patterns of failure after single-dose radiosurgery for spinal metastasis. J Neurosurg. 2004;101(S3):402–405. doi:10.3171/sup.2004.101.supplement3.0402
22. Leeman JE, Bilsky M, Laufer I, et al. Stereotactic body radiotherapy for metastatic spinal sarcoma: a detailed patterns-of-failure study. J Neurosurg Spine. 2016;25(1):52–58. doi:10.3171/2015.11.SPINE151059
23. Gerszten PC, Burton SA, Ozhasoglu C, Welch WC. Radiosurgery for spinal metastases: clinical experience in 500 cases from a single institution. Spine (Phila Pa 1976). 2007;32(2):193–199. doi:10.1097/01.brs.0000251863.76595.a2
24. Bishop AJ, Tao R, Guadagnolo BA, et al. Spine stereotactic radiosurgery for metastatic sarcoma: patterns of failure and radiation treatment volume considerations. J Neurosurg Spine. 2017;27(3):303–311. doi:10.3171/2017.1.SPINE161045
25. Yamada Y, Katsoulakis E, Laufer I, et al. The impact of histology and delivered dose on local control of spinal metastases treated with stereotactic radiosurgery. Neurosurg Focus. 2017;42(1):E6. doi:10.3171/2016.9.FOCUS16369
26. Jahaveri PM, Teh BS, Paulino AC, et al. A dose-response relationship for time to bone pain resolution after stereotactic body radiotherapy (SBRT) for renal cell carcinoma (RCC) bony metastases. Acta Oncol. 2012;51(5):584–588. doi:10.3109/0284186X.2011.652741
27. Rose PS, Laufer I, Boland PJ, et al. Risk of fracture after single fraction image-guided intensity-modulated radiation therapy to spinal metastases. J Clin Oncol. 2009;27(30):5075–5079. doi:10.1200/JCO.2008.19.3508
28. Garcia-Barros M, Paris F, Cordon-Cardo C, et al. Tumor response to radiotherapy regulated by endothelial cell apoptosis. Science. 2003;300(5622):1155–1159. doi:10.1126/science.1082504
29. Steverink JG, Willems SM, Philippens MEP, et al. Early tissue effects of stereotactic body radiation therapy for spinal metastases. Int J Radiat Oncol Biol Phys. 2018;100(5):1254–1258. doi:10.1016/j.ijrobp.2018.01.005
30. Heron DE, Rajagopalan MS, Stone B, et al. Single-session and multisession CyberKnife radiosurgery for spine metastases-University of Pittsburgh and Georgetown University experience. J Neurosurg Spine. 2012;17(1):11–18. doi:10.3171/2012.4.SPINE11902
31. Ghia AJ, Chang EL, Bishop AJ, et al. Single-fraction versus multifraction spinal stereotactic radiosurgery for spinal metastases from renal cell carcinoma: secondary analysis of Phase I/II trials. J Neurosurg Spine. 2016;24(5):829–836. doi:10.3171/2015.8.SPINE15844
32. Folkert MR, Bilsky MH, Tom AK, et al. Outcomes and toxicity for hypofractionated and single-fraction image-guided stereotactic radiosurgery for sarcomas metastasizing to the spine. Int J Radiat Oncol Biol Phys. 2014;88(5):1085–1091. doi:10.1016/j.ijrobp.2013.12.042
33. Ning MS, Deegan BJ, Ho JC, et al. Low incidence of late failure and toxicity after spine stereotactic radiosurgery: secondary analysis of phase I/II trials with long-term follow-up. Radiother Oncol. 2019;138:80–85. doi:10.1016/j.radonc.2019.06.003
34. Yoo GS, Park HC, Yu JI, et al. Stereotactic ablative body radiotherapy for spinal metastasis from hepatocellular carcinoma: its oncologic outcomes and risk of vertebral compression fracture. Oncotarget. 2017;8(42):72860–72871. doi:10.18632/oncotarget.v8i42
35. Ling DC, Flickinger JC, Burton SA, et al. Long-term outcomes after stereotactic radiosurgery for spine metastases: radiation dose-response for late toxicity. Int J Radiat Oncol Biol Phys. 2018;101(3):602–609. doi:10.1016/j.ijrobp.2018.02.035
36. Sahgal A, Atenafu EG, Chao S, et al. Vertebral compression fracture after spine stereotactic body radiotherapy: a multi-institutional analysis with a focus on radiation dose and the spinal instability neoplastic score. J Clin Oncol. 2013;31(27):3426–3431. doi:10.1200/JCO.2013.50.1411
37. Napieralska A, Miszczyk L, Stapor-Fudzinska M. CyberKnife stereotactic radiosurgery and stereotactic ablative radiation therapy of patients with prostate cancer bone metastases. Neoplasma. 2016;63(2):304–312. doi:10.4149/218_150807N435
38. Boyce-Fappiano D, Elibe E, Schultz L, et al. Analysis of the factors contributing to vertebral compression fractures after spine stereotactic radiosurgery. Int J Radiat Oncol Biol Phys. 2017;97(2):236–245. doi:10.1016/j.ijrobp.2016.09.007
39. Thibault I, Whyne CM, Zhou S, et al. Volume of lytic vertebral body metastatic disease quantified using computed tomography-based image segmentation predicts fracture risk after spine stereotactic body radiation therapy. Int J Radiat Oncol Biol Phys. 2017;97(1):75–81. doi:10.1016/j.ijrobp.2016.09.029
40. Tseng CL, Soliman H, Myrehaug S, et al. Imaging-based outcomes for 24 Gy in 2 daily fractions for patients with de novo spinal metastases treated with spine stereotactic body radiation therapy (SBRT). Int J Radiat Oncol Biol Phys. 2018;102(3):499–507. doi:10.1016/j.ijrobp.2018.06.047
41. Jawad MS, Fahim DK, Gerszten PC, et al. Vertebral compression fractures after stereotactic body radiation therapy: a large, multi-institutional, multinational evaluation. J Neurosurg Spine. 2016;24(6):928–936. doi:10.3171/2015.10.SPINE141261
42. Thibault I, Al-Omair A, Masucci GL, et al. Spine stereotactic body radiotherapy for renal cell cancer spinal metastases: analysis of outcomes and risk of vertebral compression fracture. J Neurosurg Spine. 2014;21(5):711–718. doi:10.3171/2014.7.SPINE13895
43. Boehling NS, Grosshans DR, Allen PK, et al. Vertebral compression fracture risk after stereotactic body radiotherapy for spinal metastases. J Neurosurg Spine. 2012;16(4):379–386. doi:10.3171/2011.11.SPINE116
44. Kelley KD, Racareanu R, Sison CP, et al. Outcomes in the radiosurgical management of metastatic spine disease. Adv Radiat Oncol. 2018;4(2):283–293. doi:10.1016/j.adro.2018.10.007
45. Fisher CG, DiPaola CP, Ryken TC, et al. A novel classification system for spinal instability in neoplastic disease: an evidence-based approach and expert consensus from the Spine Oncology Study Group. Spine (Phila Pa 1976). 2010;35(22):E1221–9. doi:10.1097/BRS.0b013e3181e16ae2
46. Lee SH, Tatsui CE, Ghia AJ, et al. Can the spinal instability neoplastic score prior to spinal radiosurgery predict compression fractures following stereotactic spinal radiosurgery for metastatic spinal tumor?: a post hoc analysis of prospective phase II single-institution trials. J Neurooncol. 2016;126(3):509–517. doi:10.1007/s11060-015-1990-z
47. Kassamali RH, Ganeshan A, Hoey ET, Crowe PM, Douis H, Henderson J. Pain management in spinal metastases: the role of percutaneous vertebral augmentation. Ann Oncol. 2011;22(4):782–786. doi:10.1093/annonc/mdq605
48. Wardak Z, Bland R, Ahn C, et al. A phase 2 clinical trial of SABR followed by immediate vertebroplasty for spine metastases. Int J Radiat Oncol Biol Phys. 2019;104(1):83–89. doi:10.1016/j.ijrobp.2019.01.072
49. Ozdemir Y, Torun N, Guler OC, et al. Local control and vertebral compression fractures following stereotactic body radiotherapy for spine metastases. J Bone Oncol. 2019;15:100218. doi:10.1016/j.jbo.2019.100218
50. Pichon B, Campion L, Delpon G, et al. High-dose hypofractionated radiation therapy for noncompressive vertebral metastases in combination with zoledronate: a phase 1 study. Int J Radiat Oncol Biol Phys. 2016;96(4):840–847. doi:10.1016/j.ijrobp.2016.07.027
51. Ito K, Ogawa H, Shimizuguchi T, et al. Stereotactic body radiotherapy for spinal metastases: clinical experience in 134 cases from a single Japanese institution. Technol Cancer Res Treat. 2018;17:1533033818806472. doi:10.1177/1533033818806472
52. Chang JH, Gandhidasan S, Finnigan R, et al. Stereotactic ablative body radiotherapy for the treatment of spinal oligometastases. Clin Oncol (R Coll Radiol). 2017;29(7):e119–e125. doi:10.1016/j.clon.2017.02.004
53. Guckenberger M, Mantel F, Gerszten PC, et al. Safety and efficacy of stereotactic body radiotherapy as primary treatment for vertebral metastases: a multi-institutional analysis. Radiat Oncol. 2014;9:226. doi:10.1186/s13014-014-0226-2
54. Nuyttens JJ, Moiseenko V, McLaughlin M, Jain S, Herbert S, Grimm J. Esophageal dose tolerance in patients treated with stereotactic body radiation therapy. Semin Radiat Oncol. 2016;26(2):120–128. doi:10.1016/j.semradonc.2015.11.006
55. Abelson JA, Murphy JD, Loo BW
56. Cox BW, Jackson A, Hunt M, Bilsky M, Yamada Y. Esophageal toxicity from high-dose, single-fraction paraspinal stereotactic radiosurgery. Int J Radiat Oncol Biol Phys. 2012;83(5):e661–7. doi:10.1016/j.ijrobp.2012.01.080
57. Onimaru R, Shirato H, Shimizu S, et al. Tolerance of organs at risk in small-volume, hypofractionated, image-guided radiotherapy for primary and metastatic lung cancers. Int J Radiat Oncol Biol Phys. 2003;56(1):126–135. doi:10.1016/S0360-3016(03)00095-6
58. Hellman S, Weichselbaum RR. Oligometastases. J Clin Oncol. 1995;13(1):8–10. doi:10.1200/JCO.1995.13.1.8
59. Salama JK, Hasselle MD, Chmura SJ, et al. Stereotactic body radiotherapy for multisite extracranial oligometastases: final report of a dose escalation trial in patients with 1 to 5 sites of metastatic disease. Cancer. 2012;118(11):2962–2970. doi:10.1002/cncr.26611
60. Ho JC, Tang C, Deegan BJ, et al. The use of spine stereotactic radiosurgery for oligometastatic disease. J Neurosurg Spine. 2016;25(2):239–247. doi:10.3171/2016.1.SPINE151166
61. Silva SR, Gliniewicz A, Martin B, et al. Oligometastatic disease state is associated with improved local control in patients undergoing three or five fraction spine stereotactic body radiotherapy. World Neurosurg. 2019;122:e342–e348. doi:10.1016/j.wneu.2018.10.044
62. Loi M, Desideri I, Greto D, et al. Radiotherapy in the age of cancer immunology: current concepts and future developments. Crit Rev Oncol Hematol. 2017;112:1–10. doi:10.1016/j.critrevonc.2017.02.002
63. Laufer I, Rubin DG, Lis E, et al. The NOMS framework: approach to the treatment of spinal metastatic tumors. Oncologist. 2013;18(6):744–751. doi:10.1634/theoncologist.2012-0293
64. Tang C, Hess K, Bishop AJ, et al. Creation of a prognostic index for spine metastasis to stratify survival in patients treated with spinal stereotactic radiosurgery: secondary analysis of mature prospective trials. Int J Radiat Oncol Biol Phys. 2015;93(1):118–125. doi:10.1016/j.ijrobp.2015.04.050
65. Spratt DE, Beeler WH, de Moraes FY, et al. An integrated multidisciplinary algorithm for the management of spinal metastases: an International Spine Oncology Consortium report. Lancet Oncol. 2017;18(12):e720–e730. doi:10.1016/S1470-2045(17)30612-5
66. Cox BW, Spratt DE, Lovelock M, et al. International Spine Radiosurgery Consortium consensus guidelines fortarget volume definition in spinal stereotactic radiosurgery. Int J Radiat Oncol Biol Phys. 2012;83(5):e597–e605. doi:10.1016/j.ijrobp.2012.03.009
67. Ito K, Shimizuguchi T, Nihei K, et al. Patterns of intraosseous recurrence after stereotactic body radiation therapy for coxal bone metastasis. Int J Radiat Oncol Biol Phys. 2018;100(1):159–161. doi:10.1016/j.ijrobp.2017.08.045
68. Yu T, Choi CW, Kim KS. Treatment outcomes of stereotactic ablative radiation therapy for non-spinal bone metastases: focus on response assessment and treatment indication. Br J Radiol. 2019;92(1099):20181048. doi:10.1259/bjr.20181048
69. Erler D, Brotherston D, Sahgal A, et al. Local control and fracture risk following stereotactic body radiation therapy for non-spine bone metastases. Radiother Oncol. 2018;127(2):304–309. doi:10.1016/j.radonc.2018.03.030
70. Owen D, Laack NN, Mayo CS. Outcomes and toxicities of stereotactic body radiation therapy for non-spine bone oligometastases. Pract Radiat Oncol. 2014;4(2):e143–e149. doi:10.1016/j.prro.2013.05.006
71. van der Linden YM, Steenland E, van Houwelingen HC, et al. Patients with a favourable prognosis are equally palliated with single and multiple fraction radiotherapy: results on survival in the Dutch Bone Metastasis Study. Radiother Oncol. 2006;78(3):245–253. doi:10.1016/j.radonc.2006.02.007
72. Gaze MN, Kelly CG, Kerr GR, et al. Pain relief and quality of life following radiotherapy for bone metastases: a randomised trial of two fractionation schedules. Radiother Oncol. 1997;45(2):109–116. doi:10.1016/S0167-8140(97)00101-1
73. Nguyen QN, Chun SG, Chow E, et al. Single-fraction stereotactic vs conventional multifraction radiotherapy for pain relief in patients with predominantly nonspine bone metastases: a randomized phase 2 trial. JAMA Oncol. 2019;5:872. doi:10.1001/jamaoncol.2019.0192
74. Loi M, Klass ND, De Vries KC, et al. Pain flare, complexity and analgesia in bone oligometastases treated with stereotactic body radiation therapy. Eur J Cancer Care (Engl). 2018;27(6):e12915. doi:10.1111/ecc.12915
75. Chiang A, Zeng L, Zhang L, et al. Pain flare is a common adverse event in steroid-naïve patients after spine stereotactic body radiation therapy: a prospective clinical trial. Int J Radiat Oncol Biol Phys. 2013;86(4):638–642. doi:10.1016/j.ijrobp.2013.03.022
76. Pan HY, Allen PK, Wang XS, et al. Incidence and predictive factors of pain flare after spine stereotactic body radiation therapy: secondary analysis of phase 1/2 trials. Int J Radiat Oncol Biol Phys. 2014;90(4):870–876. doi:10.1016/j.ijrobp.2014.07.037
77. Khan L, Chiang A, Zhang L, et al. Prophylactic dexamethasone effectively reduces the incidence of pain flare following spine stereotactic body radiotherapy (SBRT): a prospective observational study. Support Care Cancer. 2015;23(10):2937–2943. doi:10.1007/s00520-015-2659-z
78. McGee HM, Carpenter TJ, Ozbek U, et al. Analysis of local control and pain control after spine stereotactic radiosurgery reveals inferior outcomes for hepatocellular carcinoma compared with other radioresistant histologies. Pract Radiat Oncol. 2019;9(2):89–97. doi:10.1016/j.prro.2018.11.009
79. Mehta N, Zavitsanos PJ, Moldovan K, et al. Local failure and vertebral body fracture risk using multifraction stereotactic body radiation therapy for spine metastases. Adv Radiat Oncol. 2018;3(3):245–251. doi:10.1016/j.adro.2018.04.002
80. Zeng KL, Myrehaug S, Soliman H, et al. Stereotactic body radiotherapy for spinal metastases at the extreme ends of the spine: imaging-based outcomes for cervical and sacral metastases. Neurosurgery. 2018. doi:10.1093/neuros/nyy393
81. Fanetti G, Marvaso G, Ciardo D, et al. Stereotactic body radiotherapy for castration-sensitive prostate cancer bone oligometastases. Med Oncol. 2018;35(5):75. doi:10.1007/s12032-018-1137-0
82. Guckenberger M, Sweeney RA, Hawkins M, et al. Dose-intensified hypofractionated stereotactic body radiation therapy for painful spinal metastases: results of a phase 2 study. Cancer. 2018;124(9):2001–2009. doi:10.1002/cncr.v124.9
83. Bernard V, Bishop AJ, Allen PK, et al. Heterogeneity in treatment response of spine metastases to spine stereotactic radiosurgery within “radiosensitive” subtypes. Int J Radiat Oncol Biol Phys. 2017;99(5):1207–1215. doi:10.1016/j.ijrobp.2017.08.028
84. Bernstein MB, Chang EL, Amini B, et al. Spine stereotactic radiosurgery for patients with metastatic thyroid cancer: secondary analysis of phase I/II trials. Thyroid. 2016;26(9):1269–1275. doi:10.1089/thy.2016.0046
85. Germano IM, Carai A, Pawha P, et al. Clinical outcome of vertebral compression fracture after single fraction spine radiosurgery for spinal metastases. Clin Exp Metastasis. 2016;33(2):143–149. doi:10.1007/s10585-015-9764-8
86. Lee E, Kim TG, Park HC, et al. Clinical outcomes of stereotactic body radiotherapy for spinal metastases from hepatocellular carcinoma. Radiat Oncol J. 2015;33(3):217–225. doi:10.3857/roj.2015.33.3.217
87. Amini A, Altoos B, Bourlon MT, et al. Local control rates of metastatic renal cell carcinoma (RCC) to the bone using stereotactic body radiation therapy: is RCC truly radioresistant? Pract Radiat Oncol. 2015;5(6):e589–e596. doi:10.1016/j.prro.2015.05.004
88. Bishop AJ, Tao R, Rebueno NC, et al. Outcomes for spine stereotactic body radiation therapy and an analysis of predictors of local recurrence. Int J Radiat Oncol Biol Phys. 2015;92(5):1016–1026. doi:10.1016/j.ijrobp.2015.03.037
89. Anand AK, Venkadamanickam G, Punnakal AU, et al. Hypofractionated stereotactic body radiotherapy in spinal metastasis - withor without epidural extension. Clin Oncol (R Coll Radiol). 2015;27(6):345–352. doi:10.1016/j.clon.2015.01.035
90. Balagamwala EH, Angelov L, Koyfman SA, et al. Single-fraction stereotactic body radiotherapy for spinal metastases from renal cell carcinoma. J Neurosurg Spine. 2012;17(6):556–564. doi:10.3171/2012.8.SPINE12303
91. Ahmed KA, Stauder MC, Miller RC, et al. Stereotactic body radiation therapy in spinal metastases. Int J Radiat Oncol Biol Phys. 2012;82(5):e803–e809. doi:10.1016/j.ijrobp.2011.11.036
92. Wang XS, Rhines LD, Shiu AS, et al. Stereotactic body radiation therapy for management of spinal metastases in patients without spinal cord compression: a phase 1-2 trial. Lancet Oncol. 2012;13(4):395–402. doi:10.1016/S1470-2045(11)70384-9
93. Martin AG, Cowley IR, Taylor BA, et al. (Stereotactic) radiosurgery XIX: spinal radiosurgery–two year experience in a UK centre. Br J Neurosurg. 2012;26(1):53–58. doi:10.3109/02688697.2011.603857
94. Muacevic A, Kufeld M, Rist C, Wowra B, Stief C, Staehler M. Safety and feasibility of image-guided robotic radiosurgery for patients with limited bone metastases of prostate cancer. Urol Oncol. 2013;31(4):455–460. doi:10.1016/j.urolonc.2011.02.023
95. Nguyen QN, Shiu AS, Rhines LD, et al. Management of spinal metastases from renal cell carcinoma using stereotactic body radiotherapy. Int J Radiat Oncol Biol Phys. 2010;76(4):1185–1192. doi:10.1016/j.ijrobp.2009.03.062
96. Amdur RJ, Bennett J, Olivier K, et al. A prospective, phase II study demonstrating the potential value and limitation of radiosurgery for spine metastases. Am J Clin Oncol. 2009;32(5):515–520. doi:10.1097/COC.0b013e318194f70f
97. Tsai JT, Lin JW, Chiu WT, Chu WC. Assessment of image-guided CyberKnife radiosurgery for metastatic spine tumors. J Neurooncol. 2009;94(1):119–127. doi:10.1007/s11060-009-9814-7
98. Chang EL, Shiu AS, Mendel E, et al. Phase I/II study of stereotactic body radiotherapy for spinal metastasis and its pattern of failure. J Neurosurg Spine. 2007;7(2):151–160. doi:10.3171/SPI-07/08/151
99. Gibbs IC, Kamnerdsupaphon P, Ryu MR, et al. Image-guided robotic radiosurgery for spinal metastases. Radiother Oncol. 2007;82(2):185–190. doi:10.1016/j.radonc.2006.11.023
100. Sharma M, Bennett EE, Rahmathulla G, et al. Impact of cervicothoracic region stereotactic spine radiosurgery on adjacent organs at risk. Neurosurg Focus. 2017;42(1):E14. doi:10.3171/2016.10.FOCUS16364
101. Hashmi A, Guckenberger M, Kersh R, et al. Re-irradiation stereotactic body radiotherapy for spinal metastases: a multi-institutional outcome analysis. J Neurosurg Spine. 2016;25(5):646–653. doi:10.3171/2016.4.SPINE151523
102. Moussazadeh N, Lis E, Katsoulakis E, et al. Five-year outcomes of high-dose single-fraction spinal stereotactic radiosurgery. Int J Radiat Oncol Biol Phys. 2015;93(2):361–367. doi:10.1016/j.ijrobp.2015.05.035
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.