Back to Journals » Local and Regional Anesthesia » Volume 18
Single-Entry Selective Trunk Block (S-SeTB): An Innovative Approach to Complete Upper Extremity Anesthesia in Weapon-Wounded Patients in Low-Resource Settings
Authors Shabani M ![]() , Crespo S, Raingeval X
, Crespo S, Raingeval X ![]()
Received 24 February 2025
Accepted for publication 22 July 2025
Published 26 July 2025 Volume 2025:18 Pages 45—55
DOI https://doi.org/10.2147/LRA.S524347
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Stefan Wirz
Video abstract of “Single-entry selective trunk block” [524347].
Views: 142
Majaliwa Shabani,1,* Sophie Crespo,2,* Xavier Raingeval3,*
1Health_unit, International Committee of the Red Cross, Bamako, Mali; 2Health Unit, International Committee of the Red Cross, Geneva, Switzerland; 3Association de Développement et de Recherche en Anesthésie Locorégionale Echoguidée (ADRALE), Paris, France
*These authors contributed equally to this work
Correspondence: Majaliwa Shabani, Health Unit, International Committee of the Red Cross, HAMDALLAYE RUE 239, Postal Office Box: 58, Bamako, Mali, Email [email protected]
Background: Regional anesthesia for upper extremity surgery in weapon-wounded patients is challenging, particularly in low-resource settings. Existing techniques often require multiple needle entries and ultrasound probe repositioning, increasing complexity and risk. There is a need for a simpler, effective technique providing complete anesthesia from the shoulder to the hand.
Methods: We developed a novel ultrasound-guided regional anesthesia technique—the Single-entry Selective Trunk Block (S-SeTB)—which targets the superior trunk (ST), middle trunk (MT), and C8 ventral ramus (C8VR) with local anesthetic diffusion to the inferior trunk (IT). The procedure uses one skin entry point to deliver three injections and is combined with a superficial cervical plexus (SCP) block using the same entry and ultrasound plane. Over 600 procedures were performed in field hospitals operated by the International Committee of the Red Cross, with observations documented.
Results: The S-SeTB consistently achieved full anesthesia of the upper extremity, including the shoulder and clavicle, without the need for conversion to general anesthesia. The technique was well tolerated and effective in complex trauma cases. No major complications were reported. Compared to conventional selective trunk blocks or hybrid brachial plexus approaches, the S-SeTB required lower anesthetic volumes (20– 25 mL) and demonstrated reduced procedural complexity and risks (eg, pneumothorax, vascular puncture).
Conclusion: The S-SeTB, combined with SCP and intercostobrachial nerve blocks, offers a reliable, resource-efficient, and safer alternative to traditional brachial plexus block techniques. It is particularly well-suited for austere environments where anesthesia resources and safety margins are limited. Further prospective studies are ongoing to evaluate block dynamics and confirm efficacy.
Keywords: selective trunk block, SeTB, ultrasound-guided regional anesthesia, brachial plexus anesthesia, conflict-zone anesthesia, low-resource anesthesia
Introduction
Background
In low-resource settings, effective anesthesia, and pain management for weapon-wounded are critical components of comprehensive surgical care.1–3 Traditionally, potent opioids have been central to managing post-injury pain; however, their use poses significant challenges in these environments. A key concern is the heightened risk of addiction, particularly in populations already struggling with the widespread misuse of weaker opioids, such as tramadol.4,5 Furthermore, the procurement and availability of strong intravenous opioids such as fentanyl and morphine, are severely hindered by strict regulatory controls, especially in conflict zones.6 These barriers underscore the urgent need for alternative pain management and anesthesia strategies that are both effective and feasible in resource-limited settings.7
Upper extremity injuries from weapon wounds are common and pose unique anesthesia challenges due to extensive debridement and frequent use of external fixation for immobilization.8
The brachial plexus, recognized as one of the most anatomically complex components of the peripheral nervous system, extends from the cervical intervertebral foramina to the axilla. This extensive and intricate course poses a significant challenge to achieving complete anesthesia of the upper extremity through a single nerve block.9
Rationale
No single brachial plexus blockade technique achieves comprehensive anesthesia for surgical procedures involving the entire upper limb including the clavicle and shoulder. To address this limitation, a hybrid brachial plexus block techniques — combining an interscalene block and a supraclavicular block — and the selective trunk block (SeTB) with double needle insertion have been proposed.10–13 Additionally, when the clavicle is involved, a supplementary superficial cervical plexus (SCP) block is necessary.14,15
Combining the SeTB and SCP block through a single-entry point to achieve anesthetic coverage equivalent to the combination of interscalene, supraclavicular, and superficial cervical plexus blocks is theoretically complex and sparsely documented in the medical literature.10–15
The intercostobrachial nerve (ICBN) is a purely sensory nerve arising from the lateral cutaneous branch of the second intercostal nerve (T2 spinal level). It provides sensory innervation to the axilla and the posteromedial aspect of the upper arm. Since the ICBN is not part of the brachial plexus, it must be blocked separately for surgical procedures involving these regions.16
Hypothesis
We hypothesize that targeting the brachial plexus midway between the interscalene groove and supraclavicular fossa will selectively block the C8 ventral ramus (C8VR), middle trunk (MT), and superior trunk (ST). Advancing the needle between the deep investing cervical fascia and the prevertebral fascia, will achieve an effective SCP block. This combined technique, using a single skin entry point, aims to provide comprehensive anesthesia of the upper extremity, including the shoulder and clavicle.
At the midpoint between the scalene groove and the supraclavicular fossa along the brachial plexus course, the C8VR appears hypoechoic, follows the shortest course among C5–C8, and is positioned above the first rib–T1 transverse process complex (1st Rib-T1TP) before merging with T1 to form the inferior trunk (IT).17 The T1 ventral ramus emerges from beneath the first rib and joins the C8VR more anteriorly, overlying the rib. Injection of local anesthetic (LA) between the C8VR and the first rib–T1TP complex may facilitate its spread to the T1 ventral ramus and IT, which are located above the first rib.
Objective
The primary objective of this manuscript is to introduce and describe the single-entry selective trunk block (S-SeTB), a novel ultrasound-guided regional anesthesia technique designed to selectively anesthetize the ST, MT, and IT of the brachial plexus. When combined with a SCP block, this approach provides comprehensive anesthesia for the entire upper extremity—including the shoulder and clavicle—through a single skin entry point. Additionally, we present initial clinical experiences demonstrating the efficacy and feasibility of this innovative technique in low-resource and conflict-affected settings.
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. All videos and images included for illustrative purposes were obtained with informed patient consent and approved by the Institutional Ethical Review Board of the International Committee of the Red Cross.
Technique Description
Equipment, Patient Positioning, and Sonoanatomy
An ultrasound machine equipped with a high-frequency linear transducer is used. Patient is positioned supine, with the ipsilateral arm in a neutral position and the head slightly rotated contralaterally to optimize the ultrasound view (Figure 1A).
 |
Figure 1 Sonographic anatomy of the superior trunk, middle trunk, and C8 ventral ramus at the midpoint between the scalene groove and the supraclavicular fossa. (A) Patient position and ultrasound probe placement; (B) sonoanatomy of the trunks and C8 ventral ramus for the single-entry selective block; (C) the anatomy illustration demonstrates the ultrasound beam’s position (plane) and the neural structures visible at a level between the supraclavicular fossa and interscalene groove. Abbreviations: ASM, anterior scalene muscle; MSM, middle scalene muscle; ss, suprascapular nerve; PL, pleural line; SA, Subclavian artery; C8VR, C8 ventral ramus; MT, middle trunk; ST, superior trunk. |
The sonoanatomy of the S-SeTB is characterized by clear visualization of two distinct brachial plexus trunks—the ST and MT — along with the C8VR. These structures are situated between the anterior and middle scalene muscles (Figure 1B and C).
The C8VR, appearing hypoechoic, is positioned laterally on the first rib–T1 transverse process complex, with the pleural dome medially adjacent. The subclavian artery lies medial to the C8VR.
Anatomical variations in the distribution of the superior and middle trunks are common, necessitating an extended ultrasound scan from the supraclavicular fossa to the scalene groove to accurately trace each trunk and adjust the technique accordingly.18 Additionally, a muscular bridge between the MT and C8VR may hinder local anesthetic (LA) spread from a scalene groove to the C8VR19 (Figure 2).
 |
Figure 2 Anatomical variation with middle trunk located within the middle scalene muscle and muscular bridge separating the middle trunk to C8 ventral ramus. Abbreviations: ST, superior trunk; MT, middle trunk; C8VR, C8 ventral ramus; sa, Subclavian artery; asm, anterior scalene muscle; msm, middle scalene muscle. |
Detailed Procedural Steps
- The ultrasound sequence starts by positioning the ultrasound transducer in the supraclavicular fossa region, parallel to the clavicle (Figure 3A), to obtain the classic image of supraclavicular nerve block (Figure 3B).

Figure 3 Sequential ultrasound technique for single-entry selective trunk block. (A) Patient positioning and ultrasound screening technique using three key scanning points: the supraclavicular fossa (1), the scalene groove (2), and a midpoint between these two locations (3). (B) Sonographic view at supraclavicular fossa, illustrating the brachial plexus. (C) Sonographic view at the midpoint between the supraclavicular fossa and the scalene groove, illustrating C8Vr, MT, and ST. (D) Sonographic view of the scalene groove, illustrating the C5, C6, and C7 nerve roots.
Abbreviations: SA, Subclavian artery; C7TP, transverse process of C7 cervical vertebrae, VA, vertebral artery; ST, superior trunk; MT, middle trunk; C8VR, C8 ventral ramus.
- The ultrasound transducer is slowly moved cranially, with sweeping motion in scalene groove to have C7, C6, and C5 ventral rami (Figure 3D).
- Finally, the ultrasound transducer is moved in reverse caudally and identify the ST, MT, and C8VR: an integrated sonographic view is created, displaying two key areas (Figure 3C):

The upper part shows the MT and ST located between the anterior and middle scalene muscles.
The lower part shows the C8VR, typically hypoechoic, above the First rib-T1TP complex near the subclavian artery and pleura.
This approach provides coverage of the ST, MT, and IT through a single-entry point, with T1 and IT blocked by LA diffusion from C8VR. It also allows for superficial cervical plexus blockade when the injury involves the shoulder or clavicle using the same skin entry point.
Our ultrasound imaging technique is performed under aseptic conditions: The C8VR is targeted first, followed by the MT and ST. Using a single skin entry point, the S-SeTB involves three sequential injections: 8–10 mL below the C8 VR, 8–10 mL between and around the MT and ST, and 4–5 mL above the ST. The total volume of local anesthetic (LA) ranges from 20 to 25 mL.
In practice, the block is initiated by gently displacing the C8VR superficially from the first rib–T1TP complex. This is achieved by placing the needle tip between the first rib and the C8VR and injecting 8–10 mL of local anesthetic (Figure 4 and video). Next, we redirect the needle and proceed with an injection between and around the MT and ST, and finally above the ST, allowing diffusion towards the suprascapular nerve. (video).
 |
Figure 4 Single-entry selective trunk block (S-SeTB) combined with superficial cervical plexus (SCP) block. The illustration shows the needle trajectories (dashed lines) for performing the S-SeTB alongside the SCP block using a single skin entry point. Dashed line 1: Needle path targeting the C8VR blockade. Dashed line 2: Needle path between the ST and MT. Dashed line 3: Needle path for the SCP block. Abbreviations: SCM, sternocleidomastoid muscle; ST, superior trunk; MT, middle trunk; C8VR, C8 ventral ramus; SCP, superficial cervical plexus. |
After completing the block, an upward scan confirms the spread of LA within the interscalene groove. Scanning downward into the supraclavicular fossa consistently shows LA diffusion surrounding the brachial plexus, as well as the “corner pocket” region (Figure 5). By keeping the needle tip away from the pleural dome and selectively targeting the ST, MT, C8VR, this approach theoretically reduces the risks of pneumothorax and nerve injury.
 |
Figure 5 Sonographic views before and after local anesthetic injection. Injection was performed at the scalene groove between the superior trunk and middle trunk, and between the first rib-T1 transverse process complex. Note the spread of local anesthetic in the supraclavicular fossa, particularly at the “corner pocket” region and the scalene groove. Abbreviations: sca, subclavian artery; MSM, medium scalene muscle; ASM, anterior scalene muscle; LA, local anesthetic. |
Superficial Cervical Plexus Block
For upper limb surgeries that involve the shoulder or clavicle, the S-SeTB is supplemented with a SCP block using the same entry point. An additional injection is administered into the potential space between the investing cervical fascia and the prevertebral fascia, at the posterior border of the sternocleidomastoid and anterior border of the trapezius. This technique ensures adequate anesthesia for debridement or incisions extending to the shoulder, clavicular region, or neck (Figure 4 and Video).
Intercostobrachial Nerve Block
The ICBN block can be performed using two ultrasound-guided approaches, each providing reliable sensory blockade depending on procedural needs: a proximal approach, where the injection is made between the pectoralis minor and the second rib, and a distal approach, targeting the area above the conjoint tendon of the latissimus dorsi.20–22
When using the latissimus dorsi infiltration approach, the injection should be performed after the S-SeTB and SCP blocks to optimize anesthetic onset. As the injured upper limb is positioned with the shoulder abducted and the elbow flexed during the procedure, this maneuver may cause discomfort.
In our clinical practice, we prefer the proximal approach for ICBN blockade. This approach minimizes arm mobilization, reducing pain and discomfort in weapon-wounded patients with severe upper extremity injuries. The latissimus dorsi infiltration method is simple and effective, offering a viable alternative in challenging cases.
Technical Tips for Optimizing Regional Blocks
Block the C8VR First
Positioning the injection between the first rib and the C8VR serves to displace the targeted neural structures superficially—including the C8VR, MT, and ST—thereby enhancing both contrast and sonographic visualization. This maneuver not only improves anatomical delineation but also facilitates more effective local anesthetic diffusion, ensuring adequate coverage of the IT and T1. In certain cases, the contour of the C8VR may be difficult to define clearly. When this occurs, initiating the injection between the ST and MT can improve visibility of the C8VR by enhancing its separation from surrounding structures.
Optimize Ultrasound Imaging
Tilting the ultrasound transducer cranially enhances the visualization of the ST, MT, and C8VR, leading to a more precise injection.
Safety Considerations
Diaphragmatic Impairment
Similar to other supraclavicular approaches for brachial plexus blockade, the S-SeTB carries a risk of diaphragmatic impairment, necessitating caution in patients with respiratory compromise.23 Among supraclavicular approaches, the interscalene block poses the highest risk of affecting diaphragmatic function24 (Figure 6).
 |
Figure 6 Diaphragmatic assessment before (A) and 30 min after (B) single entry-selective trunk block. Note the reduction in diaphragm excursion after the S-SeTB. |
Transverse Cervical Artery
During the S-SeTB, careful consideration of transverse cervical artery (TCA) anatomical variation is crucial to avoid vascular puncture or intravascular injection. In 60–70% of cases, the TCA originates from the thyrocervical trunk, coursing anterior to the brachial plexus trunks, posing minimal risk. However, in 30% of cases, it arises from the subclavian artery, potentially passing anterior or between the trunks, increasing the risk of vascular injury, hematoma, or intravascular injection (Figure 7). Doppler ultrasound should be employed to identify vascular structures, with needle trajectory and ultrasound plane adjustments to minimize complications25,26 (Figure 7).
 |
Figure 7 Course of the transverse cervical artery and its relationship to the brachial plexus at the truncal level. The transverse cervical artery is positioned between the middle trunk and the C8 ventral ramus, as demonstrated in the Doppler image (B). Abbreviations: ST, superior trunk; MT, middle trunk; C8VR, C8 ventral ramus; TCA, transverse cervical artery; msm, middle scalene muscle; asm, anterior scalene muscle. |
Dorsal Scapular Nerve and Long Thoracic Nerve
The dorsal scapular nerve (DSN), primarily from C5 (with possible C6 contributions), travels near the ST, pierces the middle scalene, and passes beneath the levator scapulae (Figure 8A). The long thoracic nerve (LTN), arising from C5–C7, runs along or within the middle scalene, often close to the DSN (Figure 8B).27,28 Our study on the S-SeTB highlights the frequent presence of these nerves along the needle path, underscoring the importance of their identification to prevent injury (Figure 8C). The DSN is generally more visible on ultrasound than the LTN.27,28 Similarly, previous studies have emphasized the risk of DSN and LTN injury during ultrasound-guided interscalene blocks, particularly with the conventional in-plane lateral-to-medial needle trajectory through the middle scalene.27,28
 |
Figure 8 Sonograms of dorsal scapular nerve, long thoracic nerve, and Needle pathway during S-SeTB. (A) Sonogram depicting the dorsal scapular nerve emerging from the C5 nerve root. (B) Sonogram illustrating the superior (ST) and middle (MT) trunks of the brachial plexus, along with the C8 ventral ramus (C8VR). The dorsal scapular nerve (DSN) and long thoracic nerve (LTN) are identified within the middle scalene muscle (highlighted by a large white arrow), with the ultrasound probe positioned midway between the interscalene groove and the supraclavicular fossa. (C) Simulated needle trajectory (dashed arrow) during the S-SeTB, targeting the C8 ventral ramus as well as the middle and superior trunks. The yellow dashed circle highlights the proximity of the needle pathway to the DSN and LTN, emphasizing the potential risk of nerve injury. Abbreviations: msm, middle scalene muscle; asm, anterior scalene muscle. |
Clinical Evaluation
Initial Clinical Experience (Supplementary Video)
Our initial experience with the S-SeTB encompasses over 600 procedures across diverse upper extremity surgeries performed within field hospital projects managed by the International Committee of the Red Cross. Surgical indications included complex wound management, fracture fixation, reconstructive procedures, and emergency vascular repairs.
In all cases, S-SeTB was effectively utilized as either a standalone anesthesia technique or in combination with ICBN and SCP blocks. Importantly, no conversions to general anesthesia were required, underscoring the high reliability of this regional anesthesia approach.
Ongoing Research
Currently, a multicentric prospective study titled “Effectiveness of Single-Entry Selective Trunk Block for Complete Upper Extremity Anesthesia in Weapon-Wounded Patients” is underway, designed to rigorously evaluate the effectiveness, safety, and broader applicability of S-SeTB across various clinical settings. The study was reviewed and approved by the Ethics Review Board of the International Committee of the Red Cross on 21st November 2024 in Geneva, Switzerland (Study Reference Number: 2413_NOV).
Discussions
Our study confirms the feasibility of regional anesthesia as the sole anesthetic technique for complex upper extremity surgeries. This approach provides comprehensive anesthesia coverage, including the shoulder and clavicle, making it a viable alternative to general anesthesia in resource-limited settings.
By utilizing a single skin entry point, our technique combines a S-SeTB and a SCP Block, offering broad anesthesia coverage from the anteromedial neck and clavicle down to the fingers. Additionally, an ICBN block is performed separately to extend anesthesia to the medial upper arm.21,22 To our knowledge, this is the first documented report demonstrating comprehensive upper extremity anesthesia—including the shoulder and clavicle—using a streamlined, single-entry approach.
Our S-SeTB technique is routinely used as the primary anesthetic strategy for weapon-wounded patients with upper extremity gunshot injuries, including those involving the shoulder and clavicle. Notably, no cases required conversion to general anesthesia or additional rescue blocks. Our high success rate aligns with previous studies on selective trunk blocks.10,13,23,29
Unlike the hybrid brachial plexus block techniques and conventional SeTB, which require two needle entries and ultrasound transducer repositioning, our technique provides comprehensive upper limb anesthesia with a single entry and no transducer repositioning. In contrast, Karmakar et al describe a technique requiring two skin entry points and two ultrasound transducer repositioning, while Hong et al utilize a single skin entry point but still require two transducer repositioning—both increasing procedural complexity (table 1).10,29 Our approach also differs from the intertruncal brachial plexus block proposed by Siddiqui et al and the two-step SeTB technique by Karmakar’s team (Table 1). These alternative approaches may carry a risk of dorsal scapular artery puncture—a branch of the subclavian artery—particularly when targeting the inferior trunk at the supraclavicular fossa.10,11 Anatomical variations may position this artery between the IT and MT or between the MT and ST, further increasing the risk of vascular injury30,31 (Figure 9A and B).
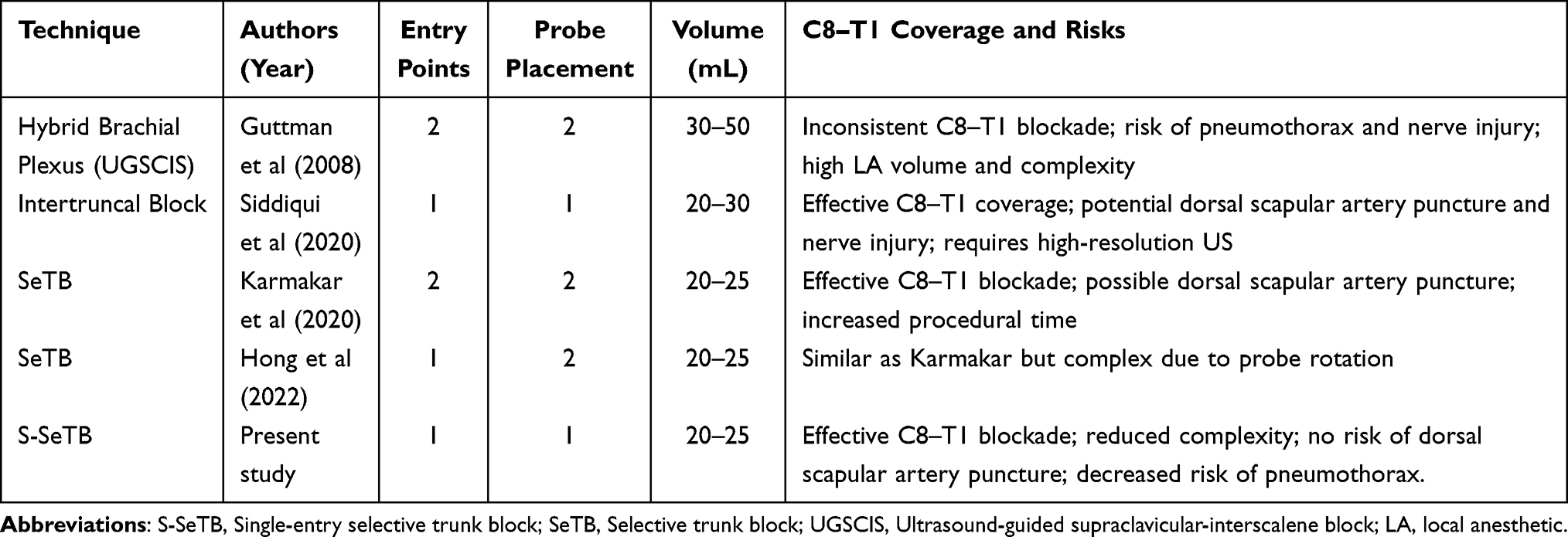 |
Table 1 Comparison of Regional Anesthesia Techniques for Complete Upper Extremity Block |
 |
Figure 9 Variations in the course of the dorsal scapular artery relative to the brachial plexus trunks at supraclavicular fossa. (A) The dorsal scapular artery passing between the middle trunk and the inferior trunk. (B) The dorsal scapular artery passing between the middle trunk and the superior trunk. Abbreviations: ST, superior trunk; MT, middle trunk; IT, inferior trunk; SS, suprascapular nerve; STp, posterior division of ST; STa, anterior division of ST; C8vr, C8 ventral ramus; sa, subclavian artery; dsa, dorsal scapular artery. |
In adult patient, we administer 20–25 mL of a 1:1 mixture of levobupivacaine 0.5% and lidocaine 1% with adrenaline (1:200,000) to optimize LA volume while minimizing the risk of systemic toxicity—an important consideration in low-resource settings. Similar dosages have been reported by Karmakar and Sivakumar.10,13,23 Our observations of LA diffusion are consistent with findings by Songthamwat et al, who documented comparable spread patterns in cadaveric studies32 (Figures 5).
This technique offers a resource-efficient alternative to conventional SeTB, general anesthesia, and hybrid brachial plexus block techniques such as the combination of interscalene block with supraclavicular, infraclavicular, or axillary blocks. By relying on a single-entry point, it achieves extensive anesthesia coverage while maintaining minimal procedural complexity. The method also allows for stable ultrasound transducer positioning, reducing the need for frequent adjustments during the procedure. Additionally, it requires a lower volume of local anesthetic (20–25 mL) compared to the hybrid brachial plexus block techniques, which enhances patient safety and minimizes the risk of local anesthetic systemic toxicity.12,33 Importantly, the risk of pneumothorax is reduced, as the needle trajectory remains distant from the pleural dome (Table 1).
Limitations
This study is primarily based on observational clinical experience in field hospitals treating weapon-wounded patients, without a control group or randomized comparison. Key metrics such as onset time, duration of anesthesia, and block resolution were not systematically recorded, limiting detailed analysis of block dynamics. Ongoing prospective studies are expected to address these limitations and provide more comprehensive data.
Conclusion
The S-SeTB, when combined with SCP and ICBN blocks, appears to offer a promising, resource-efficient alternative to general anesthesia, conventional SeTB, and hybrid brachial plexus block techniques. This single-entry approach provides comprehensive anesthetic coverage of the clavicle, shoulder, and upper extremity, while significantly reducing local anesthetic volumes—an essential consideration in trauma care and low-resource settings.
Further prospective studies with larger and more diverse patient populations are needed to confirm its general applicability, refine the understanding of block dynamics, and rigorously assess its long-term safety and efficacy across various clinical scenarios.
Overall, S-SeTB presents a practical and impactful innovation in regional anesthesia, particularly valuable for trauma management in austere or conflict-affected environments, where simplicity, safety, and efficiency are critical.
Acknowledgments
We sincerely thank Dr. Xavier Raingeval, President of ADRALE (Association pour le Développement et la Recherche en Anesthésie Locorégionale Échoguidée), for his invaluable contribution in introducing the Single-entry selective trunk block (S-SeTB) for surgery in low-resource settings. His dedication has been instrumental in advancing regional anesthesia techniques, particularly in war surgery within the International Committee of the Red Cross (ICRC), improving anesthesia accessibility and patient care in austere environments.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Meara JG, Leather AJ, Hagander L, et al. Global surgery 2030: evidence and solutions for achieving health, welfare, and economic development. Lancet. 2015;386(9993):569–624.
2. Loeser JD, Treede RD. The Kyoto protocol of IASP basic pain terminology. Pain®. 2008;137(3):473–477. doi:10.1016/j.pain.2008.04.025
3. Dubowitz G, Detlefs S, Kelly McQueen KA. Global anesthesia workforce crisis: a preliminary survey revealing shortages contributing to undesirable outcomes and unsafe practices. World J Surg. 2010;34:438–444. doi:10.1007/s00268-009-0229-6
4. Peprah P, Agyemang-Duah W, Appiah-Brempong E, Akwasi AG, Morgan AK. With tramadol, I ride like a Jaguar”: a qualitative study of motivations for non-medical purpose tramadol use among commercial vehicle operators in Kumasi, Ghana. Subst Abuse Treat Prev Policy. 2020;15:1–5. doi:10.1186/s13011-020-00292-4
5. Boun SS, Omonaiye O, Yaya S. Prevalence and health consequences of nonmedical use of tramadol in Africa: a systematic scoping review. PLOS Global Public Health. 4 1 e0002784 doi: 10.1371/journal.pgph.0002784.
6. Ivasiy R, de Leon SJ G, Meteliuk A, et al. Responding to health policy recommendations on managing opioid use disorder during Russia’s invasion of Ukraine: divergent responses from the frontline to the west. Front Public Health. 2023;10:1044677. doi:10.3389/fpubh.2022.1044677
7. Hughey S, Cole J, Drew B, Brust A, Stedjelarsen E. Regional anesthesia in resource-limited and disaster environments: a daring discourse. Reg Anesth Pain Med. 2024;rapm–2024–105680. doi:10.1136/rapm-2024-105680
8. Jensen G, Bar-On E, Wiedler JT, et al. Improving management of limb injuries in disasters and conflicts. Prehospital Disaster Med. 2019;34(3):330–334. doi:10.1017/S1049023X19004242
9. Hsu PC, Chang KV, Mezian K, et al. Sonographic pearls for imaging the brachial plexus and its pathologies. Diagnostics. 2020;10(5):324. doi:10.3390/diagnostics10050324
10. Karmakar MK, Areeruk P, Mok LY, Sivakumar RK. Ultrasound-guided selective trunk block to produce surgical anesthesia of the whole upper extremity: a case report. A&A Pract. 2020;14(9):e01274. doi:10.1213/XAA.0000000000001274
11. Siddiqui U, Perlas A, Chin K, et al. Intertruncal approach to the supraclavicular brachial plexus, current controversies and technical update: a daring discourse. Reg Anesth Pain Med. 2020;45(5):377–380. doi:10.1136/rapm-2019-101260
12. Guttman OT, Soffer RJ, Rosenblatt MA. The ultrasound‐guided supraclavicular‐interscalene (UGSCIS) block: a case report. Pain Pract. 2008;8(1):62–64. doi:10.1111/j.1533-2500.2007.00156.x
13. Sivakumar RK, Areeruk P, Karmakar MK. Selective trunk block (SeTB): a simple alternative to hybrid brachial plexus block techniques for proximal humeral fracture surgery during the COVID-19 pandemic. Reg Anesth Pain Med. 46 4 376–378 doi: 10.1136/rapm-2020-101733.
14. Ryan DJ, Iofin N, Furgiuele D, Johnson J, Egol K. Regional anesthesia for clavicle fracture surgery is safe and effective. J Shoulder Elbow Surg. 2021;30(7):e356–60. doi:10.1016/j.jse.2020.10.009
15. Abdelghany MS, Ahmed SA, Afandy ME. Superficial cervical plexus block alone or combined with interscalene brachial plexus block in surgery for clavicle fractures: a randomized clinical trial. Minerva Anestesiologica. 2021;87(5):523–532. doi:10.23736/S0375-9393.21.14865-5
16. Samerchua A, Leurcharusmee P, Panjasawatwong K, Pansuan K, Mahakkanukrauh P. Cadaveric study identifying clinical sonoanatomy for proximal and distal approaches of ultrasound-guided intercostobrachial nerve block. Reg Anesth Pain Med. 2020;45(11):853–859. doi:10.1136/rapm-2020-101783
17. Akboru IM, Solmaz I, Secer HI, Yusuf IZ, Daneyemez M. The surgical anatomy of the brachial plexus. Turk Neurosurg. 2010;20(2):142–150. doi:10.5137/1019-5149.JTN.2368-09.2
18. Orebaugh SL, Williams BA. Brachial plexus anatomy: normal and variant. Sci World J. 2009;9(1):300–312. doi:10.1100/tsw.2009.39
19. Feigl GC, Litz RJ, Marhofer P. Anatomy of the brachial plexus and its implications for daily clinical practice: regional anesthesia is applied anatomy. Reg Anesth Pain Med. 2020;45(8):620–627. doi:10.1136/rapm-2020-101435
20. Altinpulluk EY, Galluccio F, Salazar C, et al. New approach for blocking intercostobrachial and medial brachial cutaneous nerve in the axillary area: response to Varela. Reg Anesth Pain Med. 2020;45:841–842.
21. Magazzeni P, Jochum D, Iohom G, Mekler G, Albuisson E, Bouaziz H. Ultrasound-guided selective versus conventional block of the medial brachial cutaneous and the intercostobrachial nerves: a randomized clinical trial. Reg Anesth Pain Med. 2018;43(8):832–837.
22. Samerchua A, Supphapipat K, Leurcharusmee P, Thammasupapong P, Lapisatepun P, Lorsomradee S. Randomized comparison between ultrasound-guided proximal and distal approaches of intercostobrachial nerve block as an adjunct to supraclavicular brachial plexus block for upper arm arteriovenous access procedures. Reg Anesth Pain Med. 2024. doi:10.1136/rapm-2024-105973
23. Sivakumar RK, Samy W, Pakpirom J, Songthamwat B, Karmakar MK. Ultrasound-guided selective trunk block: evaluation of ipsilateral sensorimotor block dynamics, hemidiaphragmatic function and efficacy for upper extremity surgery. A single-centre cohort study. Eur J Anaesthesiol. 2022;39(10):801–809. doi:10.1097/EJA.0000000000001736
24. Wang J, Hou X, Wang X, et al. Comparison of pulmonary function during interscalene block vs. supraclavicular block: a single-center, double-blind, randomized trial. BMC Anesthesiol. 2023;23(1):12. doi:10.1186/s12871-022-01967-0
25. Hurley M, Tomasik Z, Heller S, Isbrandt R, Stevens T, Olivieri M. Variations in the transverse cervical artery (543.6). FASEB J. 2014;28:543–546. doi:10.1096/fasebj.28.1_supplement.543.6
26. Murata H, Sakai A, Hadzic A, Sumikawa K. The presence of transverse cervical and dorsal scapular arteries at three ultrasound probe positions commonly used in supraclavicular brachial plexus blockade. Anesthesia Analg. 2012;115(2):470–473. doi:10.1213/ANE.0b013e3182568557
27. Hanson NA, Auyong DB. Systematic ultrasound identification of the dorsal scapular and long thoracic nerves during interscalene block. Reg Anesth Pain Med. 2013;38(1):54–57. doi:10.1097/AAP.0b013e31826f0a63
28. Saporito A. Dorsal scapular nerve injury: a complication of ultrasound-guided interscalene block. Br J Anaesth. 2013;111(5):840–841. doi:10.1093/bja/aet358
29. Hong B, Jo Y, Oh C. Kill two birds with one stone: selective trunk block (SeTB) with single skin penetration. Korean J Anesthesiol. 2022;76(2):165. doi:10.4097/kja.22480
30. Reiner A, Kasser R. Relative frequency of a subclavian vs. a transverse cervical origin for the dorsal scapular artery in humans. Anatomical Record. 1996;244(2):265–268. doi:10.1002/(SICI)1097-0185(199602)244:2<265::AID-AR14>3.0.CO;2-N
31. Lai KC, Ho HC. Origin variations and brachial plexus relationship of the dorsal scapular artery. Sci Rep. 2023;13(1):7803. doi:10.1038/s41598-023-35054-2
32. Songthamwat B, Luangjarmekorn P, Kampitak W, Sivakumar RK, Karmakar MK. Ultrasound-guided selective trunk block (SeTB): a cadaver anatomic study to evaluate the spread of dye after a simulated injection. Reg Anesth Pain Med. 2022;47(7):414–419. doi:10.1136/rapm-2022-103630
33. Tognù A, Enrico B, Pacini I, Bosco M. Proximal humeral fracture surgery in the COVID-19 pandemic: advocacy for regional anesthesia. Reg Anesth Pain Med. 2021;46(4):375–376. doi:10.1136/rapm-2020-101626
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.