Back to Journals » Research and Reports in Urology » Volume 6
Simultaneous laparoscopic management of ureteropelvic junction obstruction and renal lithiasis: the combined experience of two academic centers and review of the literature
Authors Stravodimos K, Giannakopoulos S, Tyritzis S, Alevizopoulos A, Papadoukakis S, Touloupidis S, Constantinides C
Received 19 December 2013
Accepted for publication 7 February 2014
Published 20 May 2014 Volume 2014:6 Pages 43—50
DOI https://doi.org/10.2147/RRU.S59444
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Konstantinos G Stravodimos,1 Stilianos Giannakopoulos,2 Stavros I Tyritzis,1 Aristeides Alevizopoulos,1 Stefanos Papadoukakis,1 Stavros Touloupidis,2 Constantinos A Constantinides1
1Department of Urology, Athens University Medical School, Laiko Hospital, Athens, 2Department of Urology, Democritus University of Thrace, Alexandroupolis, Greece
Introduction: Approximately one out of five patients with ureteropelvic junction obstruction (UPJO) present lithiasis in the same setting. We present our outcomes of simultaneous laparoscopic management of UPJO and pelvic or calyceal lithiasis and review the current literature.
Methods: Thirteen patients, with a mean age of 42.8±13.3 years were diagnosed with UPJO and pelvic or calyceal lithiasis. All patients were subjected to laparoscopic dismembered Hynes–Anderson pyeloplasty along with removal of single or multiple stones, using a combination of laparoscopic graspers, irrigation, and flexible nephroscopy with nitinol baskets.
Results: The mean operative time was 218.8±66 minutes. In two cases, transposition of the ureter due to crossing vessels was performed. The mean diameter of the largest stone was 0.87±0.25 cm and the mean number of stones retrieved was 8.2 (1–32). Eleven out of 13 patients (84.6%) were rendered stone-free. Complications included prolonged urine output from the drain in one case (Clavien grade I) and urinoma formation requiring drainage in another case (Clavien grade IIIa). The mean postoperative follow-up was 30.2 (7–51) months. No patient has experienced stone or UPJO recurrence.
Conclusion: Laparoscopy for the management of UPJO along with renal stone removal seems a very appealing treatment, with all the advantages of minimally invasive surgery. Concomitant renal stones do not affect the outcome of laparoscopic pyeloplasty, at least in the midterm. According to our results and the latest literature data, we advocate laparoscopic management as the treatment of choice for these cases.
Keywords: laparoscopic pyeloplasty, lithiasis, ureteropelvic junction obstruction
Introduction
Ureteropelvic junction obstruction (UPJO) and lithiasis of the renal pelvis or the renal calyces can coexist.1 This coexistence might trouble the surgeon urologist, since the selection of the appropriate management can be challenging. Several factors might affect the final decision, which can be related to either the UPJO or the lithiasis itself. However, the main therapeutic objective is a non-obstructed, stone-free upper urinary tract.
Until recently, the preferred minimally invasive option was percutaneous endopyelotomy in the setting of UPJO and concurrent lithiasis.2 Nonetheless, skepticism of the rather lower success rates of endopyelotomy,3 along with its restricted indications, have stimulated and extended the use of other minimally invasive techniques, especially the laparoscopic approach, which can be combined with other flexible endoscopic instruments.
We present the experience of two academic institutions in the management of UPJO and renal lithiasis, performing laparoscopic dismembered pyeloplasty combined with selective use of laparoscopic instruments and/or flexible nephroscopy for stone retrieval. We report the series with the longest follow-up among the currently existing studies in the literature on this topic. Additionally, the relevant literature is reviewed.
Materials and methods
We retrospectively reviewed the files of 13 patients, with a mean age of 42.8±13.3 years, who were diagnosed with UPJO and pelvic or calyceal lithiasis. The study was approved by the Institutional Scientific and Ethical Committee of both participating institutions. All patients were symptomatic prior to diagnosis, either with flank pain or obstructive pyelonephritis. No patient required ureteral stent placement preoperatively. Diagnosis was set by intravenous urography (IVU), computed tomography (CT) or magnetic resonance imaging (MRI) urography, and diethylene triamine pentaacetic acid (DTPA) scan. Obstruction was defined as half-time more than 20 minutes after diuretic on renal scan, and as delayed nephrogram and/or excretion with hydronephrosis on radiological examinations. None of our patients had a history of previous intervention for UPJO. All of them were first-time stone formers with no history of stones or stone-related surgery. All patients were subjected to transperitoneal laparoscopic Hynes–Anderson dismembered pyeloplasty (DHA) with removal of stones. The following intraoperative data were recorded: number and size of stones, methods for stone retrieval, presence of crossing vessels, blood loss, and operative time. The latter was calculated from first skin incision to last skin suture. All patients had a plain X-ray film (kidney, ureter, bladder [KUB]) and renal ultrasound before discharge to check for residual stones. Follow-up consisted of IVU or CT or MRI at 3 months, DTPA at 6 months, and renal ultrasound annually. In order to have a meaningful comparison, the radiological examination at 3 months was the same as the preoperative examination by which the diagnosis had been set. Success was defined as resolution of pre-existing symptoms and improvement of pelvicalyceal dilatation on radiological examinations.
Operative technique
Under general anesthesia and with the patient in a 90° flank position, pneumoperitoneum was established with the Hasson technique. A standard 3-port transperitoneal approach was used. An additional 5 mm port was used if needed. Dissection along the line of Toldt using the harmonic scalpel was performed in order to mobilize the colon and expose the ureter. After dissection of the renal pelvis, an initial pyelotomy was made, in order to remove all stones. This was accomplished by using a combination of the following: laparoscopic graspers, irrigation for flushing out fragments, and flexible nephroscopy combined with nitinol baskets (Figure 1). By extending the initial pyelotomy, redundant pelvic tissue was removed, the ureteropelvic junction was circumferentially transected, and the ureter was spatulated towards the lower pole of the kidney over 1–2 cm. In case of a crossing vessel, prior to the initiation of the anastomosis, the ureter was transposed to the opposite (anterior) side. A classic dismembered Hynes–Anderson pyeloplasty was performed using 4-0 absorbable interrupted (in eight cases) or running (in five cases) sutures for both anterior and posterior anastomosis. Intracorporeal knot tying was performed in a free-hand fashion. When the posterior part of the anastomosis was concluded, a guidewire was inserted through a trocar in the ureter reaching the bladder and antegrade stenting (using a double J stent) was performed. A 16F drain was finally placed through one of the port sites.
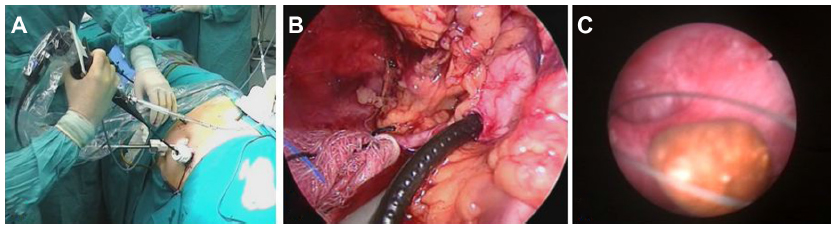 | Figure 1 (A) Intraoperative use of the flexible nephroscope through a 10 mm port; (B) nephroscope inside the renal pelvis through pyelotomy; (C) nephroscopic view of a calyceal stone and a nitinol basket. |
Results
The procedure was completed uneventfully in all cases. Individual patient characteristics and selected type of intervention are shown in Table 1. In two cases, transposition of the ureter was performed due to crossing vessels. In another two patients (cases 8 and 13), ureteral transposition was not performed because the aberrant vessels did not seem to interfere with the uteropelvic junction (UPJ) (Table 1). The mean operative time was 218.8±66 minutes. The mean diameter of the largest stone was 0.87±0.25 cm and the mean number of stones retrieved was 8.2 (1–32). Eleven out of 13 patients (84.6%) were rendered stone-free. One patient (case 6) had very small residual fragments of the lower calyx (<5 mm), which are under observation, since he is asymptomatic. Another patient (case 9) had five residual stones 3–5 mm in diameter. After stent removal, he spontaneously passed three stones. He still has two stones in the lower pole and he is asymptomatic as well. The urinary catheter was removed either on postoperative day (POD) 6–7 or 2–3 according to surgeon preference (KGS and SG, respectively). Postoperative complications were recorded in two cases (Table 2). In case 11, we observed prolonged urine output from the drain. This caused a minimal deviation from the expected postoperative course (Clavien grade I) since both bladder catheter and drain were removed later than usual. The patient was discharged on POD 7. Case 12 had urinoma formation; the patient was managed with percutaneous drain for the urinoma and percutaneous nephrostomy tube to enhance drainage of the urinary tract. Both tubes were placed under local anesthesia (Clavien grade IIIa). Nevertheless, the outcome was excellent for both patients.
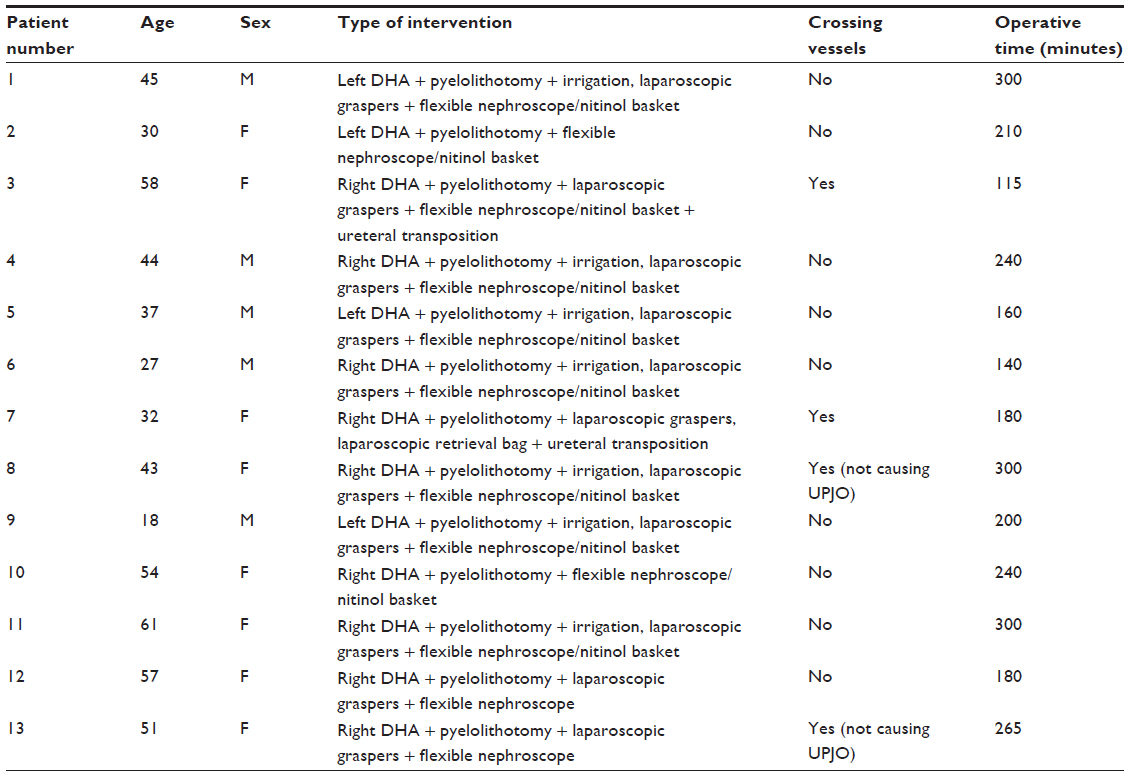 | Table 1 Demographics and intraoperative data |
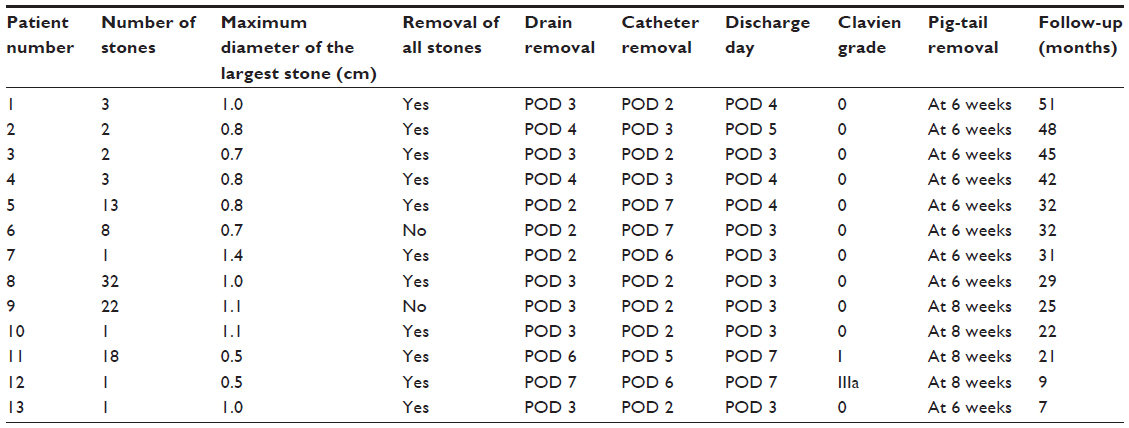 | Table 2 Postoperative data |
The mean postoperative follow-up was 30.2 (7–51) months. Currently, all patients except two are stone-free and have had no recurrence of UPJO (Figure 2). The postoperative data are summarized in Table 2.
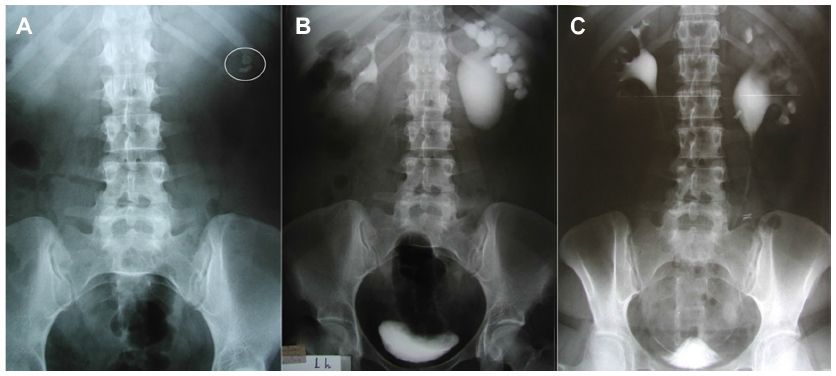 | Figure 2 (A) Preoperative KUB demonstrating two stones in the left kidney (circle); (B) preoperative IVU; (C) postoperative IVU (case 2). |
Discussion
Since Wickham attempted to remove a stone from the retroperitoneum using an endoscope,4 laparoscopy, as a minimally invasive technique, has been increasingly used in an effort to improve success rates and decrease complications and patient discomfort. The European Association of Urology (EAU) Guidelines on urolithiasis of 2013 summarized the indications for laparoscopy, which include stones in caliceal diverticula, stones in anomalous and/or ectopic kidneys, and stones associated with UPJO when other minimally invasive procedures are not indicated or have failed.5 In a systematic review, Skolarikos et al determined that the highest level of evidence supporting the role of laparoscopy in the management of lithiasis was IIa for laparoscopic ureterolithotomy.6 However, Lusuardi and Janetschek suggested that laparoscopy can be offered as first-choice treatment when anatomic abnormalities are involved, such as UPJO.7 In fact, several series support laparoscopy by reporting excellent stone-free rates and functional results in the setting of concomitant UPJO and lithiasis, ranging between 75%–100% (Table 3).8–19 Their techniques are more or less similar to each other, combining pure laparoscopy and flexible endoscopy. It should be also stated that even though laparoscopic pyelolithotomy is rarely indicated nowadays, with a level of evidence III/B,6 in the majority of the above series, a pyelotomy was enough to extract the stones and perform the pyeloplasty without further maneuvers in the pelvis.
 | Table 3 Contemporary series of combined treatment |
Until recently, the minimally invasive treatment of choice was percutaneous endopyelotomy in the setting of UPJO and concurrent lithiasis.1,2 Several series have estimated that the success rate of this approach fluctuates from 65%–90% in a maximum follow-up of 55 months.20–22 On the other hand, it is advocated that endopyelotomy is contraindicated in cases of severe hydronephrosis (grade III–IV), crossing vessels, long strictures >2 cm, renal failure, significant bleeding disorder, and extended periureteral inflammation.22 Taking the above into consideration along with the obvious fact that laparoscopy is advantageous in terms of better functional results in the combined pathology than the retrograde or antegrade approaches, it might be safe to consider laparoscopy as a first-choice treatment for the management of UPJO and lithiasis.22–24 Laparoscopy can even be performed as a salvage operation in cases of failed endopyelotomies.20
It is noticeable that the number of cases treated laparoscopically for both UPJO and lithiasis at the same time range between 3 and 21 (Table 3). Our series also consisted of 13 cases. The small numbers of patients in all these published series is clearly related to the rarity of this clinical combination. This is of course a major drawback for the above assumptions. Still, the majority of the reported cases were performed by very experienced surgeons with similar excellent results indicating the efficacy of this combined treatment. Another limitation of the existing studies in the literature is the short follow-up (Table 3). Probably one of the most important advantages of our study is the length of the follow-up, which is the longest among the currently existing studies in the literature reporting simultaneous laparoscopic treatment of UPJO and lithiasis. Given that most UPJO recurrences take place within the first postoperative year, it was previously advocated that in patients undergoing reconstruction of the ureteropelvic junction, follow-up is not strictly required after the first year. However, more recent studies with much longer follow-up have changed this notion. Dimarco et al25 found that long-term success rates after both endopyelotomy and pyeloplasty are worse than previously reported. Although most failures in both techniques occurred within 2 years, failures continued to appear after 5 and 10 years, and patients should be followed up accordingly. Similar results were reported by Yanke et al,26 who recommend that patients should receive long-term follow-up. Therefore, a follow-up period of less than 24 months does not seem adequate for safe conclusions. Unfortunately, among the 12 studies in the literature on the topic, only the study by Mufarrij et al17 has follow-up lengths longer than 24 months (28.5 months). This multi-institutional study reports on 13 patients with UPJO and renal stones. It should be noted, however, that the procedure was a robotic and not a traditional laparoscopic dismembered pyeloplasty. Their success rate was 100% (Table 3). Similarly, our study with a mean follow-up of 30.2 months and a success rate of 100%, indicates that traditional laparoscopic pyeloplasty for UPJO correction is also a highly effective procedure even in the setting of concomitant renal lithiasis. In other words, concomitant renal stones do not seem to affect the outcome of laparoscopic pyeloplasty, at least in the midterm. However, in order to avoid missing late recurrences, we followed our patients after the first year with annual renal ultrasound examination. This extended follow-up reached a total of 5 years. The outcome is still considered successful if the patient remains asymptomatic and the renal ultrasound demonstrates improvement in pelvicalyceal dilatation compared to in those performed before surgery. Thereafter, the patient is advised to return only if symptoms recur.
The stone-free rate in the present study was 84.6%. This is within the 75%–100% stone-free rate reported in the literature (Table 3). The stone-free rate is primarily influenced by the number of stones and secondarily by size and location. Obviously, it is much easier to render a patient stone-free when a single stone is present in the renal pelvis compared to another patient with multiple calyceal stones. The use of the flexible nephroscope is among the most important measures to ensure complete clearance and it has been used in the majority of the reported series. However, a few studies have reported excellent results with the utilization of rigid instruments only.18,19 It should be mentioned that our series has the second highest mean stone number which implies a high level of difficulty to achieve a stone-free status (Table 3). Still, longer follow-up would be necessary to access the future of renal lithiasis in the presence of an un-obstructed upper urinary tract. A metabolic factor may be present when UPJO together with lithiasis are encountered. Unfortunately, in our series, we were not able to obtain data on stone analysis in any of our patients, due to the fact that the analysis is not performed in any of the two participating institutions. Therefore, patients are referred to specialized centers for stone analysis and metabolic work-up.
We should also acknowledge the fact that two surgeons performed the operations. Their only difference though, was the time of the removal of the bladder catheter, which was due to surgeon preference and it did not alter the outcome. When the catheter was removed at POD 2–3, the drain was removed 1 day later in order to ascertain that there would be no urine leakage due to vesicoureteric reflux. The alternative strategy which has been used in three cases included removal of the drain on POD 2 followed by catheter removal a few days later. All of the surgical steps were common for both. Although two different strategies were employed, we admit that the duration of bladder catheterization and hospital stay were longer than those reported in other series.11,14,16 This was mainly due to the fact that the vast majority of our patients were referred to our specialized laparoscopic centers from distant areas of the country, including the islands of the Aegean archipelago. Therefore, we had to ensure that there was absolutely no urine leakage before sending these patients home, far away from specialized urological centers.
Robot-assisted laparoscopic pyeloplasty and pyelolithotomy is emerging as the future of laparoscopy, but its role for calyceal or staghorn stones is still under investigation. In their review, Badalato et al identified just four series of robot-assisted laparoscopic pyelolithotomy with or without pyeloplasty, in a sum of 39 patients.27 They concluded that the results of robot-assisted laparoscopic pyelolithotomy are promising but that more prospective randomized trials are warranted, as well as longer follow-up to verify its superiority. The advantages of the robotic system are well-known.28 Nevertheless, Link and associates concluded that robot-assisted laparoscopic pyeloplasty was 2.7 times more costly than the laparoscopic approach, with higher costs stemming from longer operative time, higher consumable costs, and depreciation of robotic equipment.29
In conclusion, laparoscopy for the management of UPJO along with renal stone removal seems a very appealing treatment, with all the advantages of minimally invasive surgery. Concomitant renal stones do not affect the outcome of laparoscopic pyeloplasty, at least in the midterm. Even though there is no prospective, randomized trial to support its value as a first-line treatment, it should be a first option for the management of correctly selected cases by experienced laparoscopic surgeons.
Disclosure
The authors report no conflicts of interest in this work.
References
Berkman DS, Landman J, Gupta M. Treatment outcomes after endopyelotomy performed with or without simultaneous nephrolithotomy: 10-year experience. J Endourol. 2009;23(9):1409–1413. | |
Bernardo NO, Smith AD. Percutaneous endopyelotomy. Urology. 2000;56(2):322–327. | |
Nadu A, Mottrie A, Geavlete P. Ureteropelvic Junction Obstruction: Which Surgical Approach? Eur Urol Suppl. 2009;8:778–781. | |
Wickham JEA, Miller RA. Percutaneous renal access. In: Percutaneous Renal Surgery. Edinburgh, Scotland: Churchill Livingstone; 1983:33–39. | |
Türk C, Knoll T, Petrik A, et al. Guidelines on Urolithiasis. 2013 edition. Arnhem, The Netherlands: European Association of Urology. Available from: http://www.uroweb.org/gls/pdf/21_Urolithiasis_LRV4.pdf. Accessed March 25, 2014. | |
Skolarikos A, Papatsoris AG, Albanis S, Assimos D. Laparoscopic urinary stone surgery: an updated evidence-based review. Urol Res. 2010;38(5):337–344. | |
Lusuardi L, Janetschek G. Indications and outcomes of laparoscopic uretero-renal stone surgery. Curr Opin Urol. 2011;21(2):161–165. | |
Micali S, Moore RG, Averch TD, Adams JB, Kavoussi LR. The role of laparoscopy in the treatment of renal and ureteral calculi. J Urol. 1997;157(2):463–466. | |
Agarwal A, Varshney A, Bansal BS. Concomitant percutaneous nephrolithotomy and transperitoneal laparoscopic pyeloplasty for ureteropelvic junction obstruction complicated by stones. J Endourol. 2008;22(10):2251–2255. | |
Ramakumar S, Lancini V, Chan DY, Parsons JK, Kavoussi LR, Jarrett TW. Laparoscopic pyeloplasty with concomitant pyelolithotomy. J Urol. 2002;167(3):1378–1380. | |
Ball AJ, Leveillee RJ, Patel VR, Wong C. Laparoscopic pyeloplasty and flexible nephroscopy: simultaneous treatment of ureteropelvic junction obstruction and nephrolithiasis. JSLS. 2004;8(3):223–228. | |
Nambirajan T, Jeschke S, Albqami N, Abukora F, Leeb K, Janetschek G. Role of laparoscopy in management of renal stones: single-center experience and review of literature. J Endourol. 2005;19(3):353–359. | |
Inagaki T, Rha KH, Ong AM, Kavoussi LR, Jarrett TW. Laparoscopic pyeloplasty: current status. BJU Int. 2005;95 Suppl 2:102–105. | |
Atug F, Castle EP, Burgess SV, Thomas R. Concomitant management of renal calculi and pelvi-ureteric junction obstruction with robotic laparoscopic surgery. BJU Int. 2005;96(9):1365–1368. | |
Srivastava A, Singh P, Gupta M, et al. Laparoscopic pyeloplasty with concomitant pyelolithotomy – is it an effective mode of treatment? Urol Int. 2008;80(3):306–309. | |
Stein RJ, Turna B, Nguyen MM, et al. Laparoscopic pyeloplasty with concomitant pyelolithotomy: technique and outcomes. J Endourol. 2008;22(6):1251–1255. | |
Mufarrij PW, Woods M, Shah OD, et al. Robotic dismembered pyeloplasty: a 6-year, multi-institutional experience. J Urol. 2008;180(4):1391–1396. | |
Chen Z, Zhou P, Yang ZQ, et al. Transperitoneal mini-laparoscopic pyeloplasty and concomitant ureteroscopy-assisted pyelolithotomy for ureteropelvic junction obstruction complicated by renal caliceal stones. PLoS One. 2013;8(1):e55026. | |
Zheng J, Yan J, Zhou Z, et al. Concomitant treatment of ureteropelvic junction obstruction and renal calculi with robotic laparoscopic surgery and rigid nephroscopy. Urology. 2014;83(1):237–242. | |
Knudsen BE, Cook AJ, Watterson JD, et al. Percutaneous antegrade endopyelotomy: long-term results from one institution. Urology. 2004;63(2):230–234. | |
Kletscher BA, Segura JW, LeRoy AJ, Patterson DE. Percutaneous antegrade endopyelotomy: review of 50 consecutive cases. J Urol. 1995;153(3 Pt 1):701–703. | |
Eden CG. Minimally invasive treatment of ureteropelvic junction obstruction: a critical analysis of results. Eur Urol. 2007;52(4):983–989. | |
Elabd SA, Elbahnasy AM, Farahat YA, et al. Minimally-invasive correction of ureteropelvic junction obstruction: do retrograde endo-incision techniques still have a role in the era of laparoscopic pyeloplasty? Ther Adv Urol. 2009;1(5):227–234. | |
Szydełko T, Kopeć R, Kasprzak J, et al. Antegrade endopyelotomy versus laparoscopic pyeloplasty for primary ureteropelvic junction obstruction. J Laparoendosc Adv Surg Tech A. 2009;19(1):45–51. | |
Dimarco DS, Gettman MT, McGee SM, et al. Long-term success of antegrade endopyelotomy compared with pyeloplasty at a single institution. J Endourol. 2006;20(10):707–712. | |
Yanke BV, Lallas CD, Pagnani C, McGinnis DE, Bagley DH. The minimally invasive treatment of ureteropelvic junction obstruction: a review of our experience during the last decade. J Urol. 2008;180(4):1397–1402. | |
Badalato GM, Hemal AK, Menon M, Badani KK. Current role of robot-assisted pyelolithotomy for the management of large renal calculi: a contemporary analysis. J Endourol. 2009;23(10):1719–1722. | |
Uberoi J, Disick GI, Munver R. Minimally invasive surgical management of pelvic-ureteric junction obstruction: update on the current status of robotic-assisted pyeloplasty. BJU Int. 2009;104(11):1722–1729. | |
Link RE, Bhayani SB, Kavoussi LR. A prospective comparison of robotic and laparoscopic pyeloplasty. Ann Surg. 2006;243(4):486–491. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.