Back to Journals » Journal of Multidisciplinary Healthcare » Volume 10
Simulated interprofessional learning activities for rural health care services: perceptions of health care students
Authors Taylor S ![]() , Fatima Y
, Fatima Y ![]() , Lakshman N, Roberts H
, Lakshman N, Roberts H
Received 3 May 2017
Accepted for publication 25 May 2017
Published 19 June 2017 Volume 2017:10 Pages 235—241
DOI https://doi.org/10.2147/JMDH.S140989
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Selina Taylor,1 Yaqoot Fatima,1,2 Navaratnam Lakshman,1 Helen Roberts1
1Mount Isa Centre for Rural and Remote Health, James Cook University, Mount Isa, 2School of Public Health, University of Queensland, Brisbane, QLD, Australia
Background: The literature on interprofessional learning (IPL) has limited empirical evidence on the impact of simulated IPL sessions in promoting collaborative health care services in rural settings. This study aims to explore health care students’ perception of the relevance of simulated IPL for rural health care services.
Methods: Three focus group interviews were held with pre-registration medical, pharmacy, and allied health students (n=22). Students worked together to manage complex simulation scenarios in small interprofessional teams. Focus group sessions were held at the end of simulation activities to explore students’ views on the relevance of simulated IPL activities. Thematic analysis was undertaken on the qualitative data obtained from the focus groups.
Results: Participants embraced both the interprofessional and the simulation components enthusiastically and perceived these to be useful for their future as rural health care practitioners. Four major themes emerged from the qualitative analysis: appreciation of the role of other health disciplines, collaborative approach to patient care, competency and skills for future health care practice, and relevance for future rural and remote health care practice. Students acknowledged the simulated IPL sessions for improving their understanding of multidisciplinary practice in rural practice and facilitating the appreciation for collaborative practice and expertise.
Conclusion: Based on the findings of this study, simulated IPL activities seem to be a potential intervention for developing collaborative practice among pre-registration health profession students. However, further evidence is required to assess if positive responses to simulated IPL activities are sustained in practice and translate into improving patient outcome.
Keywords: interprofessional, simulation, multidisciplinary, rural health care, collaboration
Introduction
Maldistribution of the workforce, an aging population, and high incidence of chronic diseases have put a strain on Australian rural health care services.1 Many strategies have been proposed to develop efficient health care service models that recognize the inherent challenges of rural health care and accommodate the changing roles of rural health professionals.2,3 The consensus is that health care can no longer be delivered solely by independent practitioners, rather requires a collaborative, team-based approach to ensure patient safety and quality of service delivery.4 Therefore, the emphasis is placed on developing interprofessional competencies within health professions.5
The 2011 report of interprofessional Education Collaborative (IPEC) underscored an expectation of delivering interprofessional education (IPE) in health professions as part of the learning process.6 Interprofessional learning (IPL) activities provide an opportunity to appreciate the differing roles and differing approaches to clinical or social problems, drawing from different disciplines and tailoring care to meet the needs of individuals receiving it.7 That, in turn, leads to future health professionals entering the workforce competent in the essential skills of teamwork and team-based care.8
The development of collaborative skills requires educational efforts engaging students of different disciplines in interactive learning with each other.9 Although during their pre-registration journey, students receive some opportunities to experience multidisciplinary health care service delivery. The existing curriculum and education models, for the most part, are offered in separate, discipline-specific “silos,”10 which, unfortunately, are not enough to develop the competency required to work together in an interprofessional environment within the resource-limited rural settings.11
The implementation of IPL on rural placements provides an ideal context in which future health care students can experience the opportunities and challenges of rural health care services.12 The traditional IPL activities offer limited opportunities for interaction with students of other disciplines and restrict students’ ability to gain the confidence necessary for effective interprofessional collaboration. Simulation activities such as standardized patient role-playing and computer-based simulations offer hands-on experience of managing challenges that participants are likely to encounter in practice,13 thereby enabling interprofessional learners to develop, practice, and refine interprofessional competencies such as communication, collaboration, and delegation.14,15
Although a few studies have highlighted the importance of simulated IPL activities,16 there is limited knowledge on whether these sessions are useful for gaining confidence to practice collaborative care in resource-limited health care settings such as rural and remote health care services.17 Considering the scarcity of evidence on this topic, the broad aim of this project is to explore the experiences and perceptions of health care students’ on simulated IPL activities in a rural and remote context, especially in the context of preparation for practice. The findings of this study are expected to provide evidence for the benefits of simulated IPL activities as effective educational strategies in the context of rural health services and assess the influence of simulated IPL on multidisciplinary learning and skills development.
Methods
Study setting
The Mount Isa Centre for Rural and Remote Health (MICRRH) is a University Department of Rural Health (UDRH) center that hosts a wide range of health professional students, e.g., medicine, occupational therapy, nursing, physiotherapy, pharmacy, speech pathology, nutrition, and dietetics students on rural placement. During their placement, students are provided training and educational opportunities including simulated IPL sessions.
Participant recruitment and data collection
For participant recruitment for this study, we focused on a purposive sample of health care students on remote placement at MICCRH. At the beginning of this project, we envisaged that our study participants will come from a diverse range of health care disciplines. However, considering that the participation was voluntary, we could recruit only those students who were interested in attending focus group sessions after attending the simulated IPL activity. Some students did not want to participate in the study, but they were encouraged to attend the simulated IPL sessions.
At the beginning of each simulation session, participants were informed about the study and asked to give their signed consent to participate in the project. After each session, a focus group discussion was conducted to explore their view on simulated IPL sessions, particularly considering the context of rural and remote health care services. Each focus group was audio recorded with the permission of participants. Each focus group lasted ~30 minutes. As part of the quality improvement activity, participants were also asked to provide their feedback on the IPL session itself.
Each session was consistent in that both students and faculty were interprofessional for each session. For every simulation scenario in each session, students from different disciplines gathered together to represent their relevant field, thus forming a multidisciplinary group. Simulation sessions included the use of high-fidelity simulation mannequins and standardized patients. Sessions involved scenarios of various rural health concerns including chronic disease management, primary care, and emergency medicine. The IPL case scenarios follow a patient through the different stages of diagnosis treatment and long-term rehabilitation. An interprofessional team of students determined and responded to management for the given scenario. The scenarios were related to how the health care system functions in rural and remote locations. The scenarios integrated skills in patient observation, clinical reasoning, problem-solving, leadership, collaboration, communication, delegation, medical practice, and referrals. Each scenario ran for ~30 minutes.
An experienced surgeon (NL) and a clinical pharmacist (ST) facilitated these sessions and provided their input both before and during these interprofessional simulation sessions. Students assumed responsibilities based on their respective professional training. The facilitators also provided clinical pearls and encouragement as needed. Participants were able to see how a particular scenario could be addressed from different perspectives in a respectful and collaborative manner.
Data analysis
Interview transcripts were thematically analyzed. Participants’ narratives were read and reread while listening to the audio recordings to familiarize the researcher with the interview content and confirm the accuracy of transcriptions. Common content between transcripts was coded and grouped into themes, which were then designated titles and further reviewed to ensure coherence.
Principles of credibility and confirmability were followed to ensure the rigor of the analysis.18 Credibility was established by three researchers (NL, ST, YF) examining the data independently and eliciting themes. One of the co-investigators (NL) spends considerable time in facilitating simulation sessions with students from multiple disciplines and, therefore, is well equipped in understanding participants’ perspectives and offsetting researchers’ bias. Direct quotes within the “Results” section of this study are provided to demonstrate confirmability. Reflexivity was employed to ensure that participants’ narratives were not influenced by the researchers’ assumptions and were accurately represented in the research findings. While the involvement of three researchers in the process of translation and data analysis achieved analysis triangulation, comparing the focus group findings with the students’ evaluation of the usefulness of simulation session offered data triangulation.
Ethical considerations
James Cook University Human Research Ethics Committee granted ethical approval (H6629). Students signed a written consent form to participate in the focus group, which stated that they were free to leave the study at any time. As a means of assuring confidentiality, all interview transcripts were de-identified, with any potentially identifying words removed.
Results
Participants’ profile
The study sample included a total of 22 full-time pre-registration (fourth- and fifth-year) students of health care programs. Students representing different professions, i.e., medicine (13), speech pathology (6), and pharmacy (3) who were on rural clinical placements, participated in the study. Of the 22 participants, 16 were females and six were males. All were domestic students, except one medicine student who was international. Three focus group sessions were conducted to gather participants’ perceptions on simulated IPE activities in the context of rural and remote health care services (Table 1). Analysis of focus group data suggested that students considered simulated IPL as a meaningful activity that helped them to learn from and with each other and provided the opportunity to understand the contribution of different disciplines (Table 2). Four themes emerged from the data as outlined later.
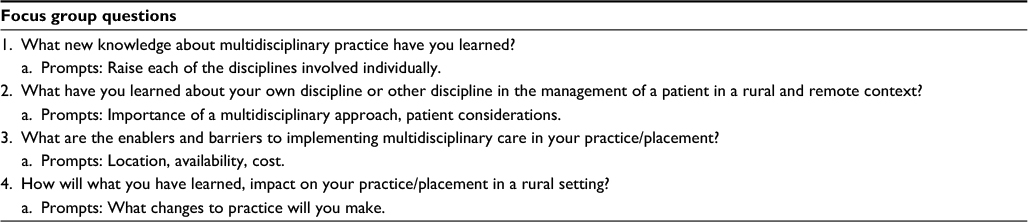 | Table 1 Focus group questions and prompts to explore health care students’ perceptions on simulated interprofessional learning activity in rural and remote context |
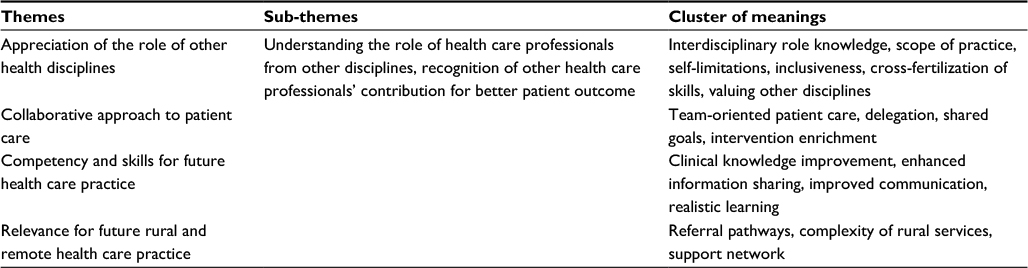 | Table 2 Themes and sub-themes demonstrating health care students’ perceptions of the relevance of simulated interprofessional learning for rural and remote health care practice |
Appreciation of the role of other health disciplines
All simulated IPL sessions were well received by the students. Participants valued simulation sessions as they allowed them to gain further knowledge of the roles and responsibilities of other professions. Their comments included:
Thinking about the pathology around it we do go through and do subjects about that but we don’t get a lot of practice with interprofessional/med students, so it is really good going through a case we can relate to but with Med students (no shared classes) getting their perspective is really interesting.
I thought that when the patient was diagnosed with diabetes that the different pathways you had like dietician and nutritionist involved I thought was really well covered because often in pharmacy we don’t see that way which is our own fault because obviously we just see medication and keep the patient alive and we don’t think how this is impacting on the patient – are they depressed, etc. so yes it was handy.
Participants also pointed out how IPL sessions were a valuable opportunity to gain further knowledge of the boundaries of different disciplines. Not only did students gain a better understanding of other professions, but they were also surprised to realize the limits of their professions.
Yeah multi-disciplinary thing is fantastic, and if had occurred more often it would be a lot easier in the workplace to call up a doctor, and we know what they could do, and they know what we can do.
Just knowing a bit more about respiratory conditions and where our role is and where the medical role is.
Before to be honest, I did not know what speechies did so it will be good to know when to use them, when to refer and what they can contribute as well.
Interprofessional training allowed the students to compare the contribution of their practice with that of other professions when considering various professional approaches to treatment. Students acknowledged simulated IPL sessions for giving them an opportunity to observe other disciplines’ patient interventions. The following excerpt, drawn from the data, offers typical reactions:
I think it was really good to know what the different interprofessional roles were and I will definitely use that in a clinical sort of scenario but also watching the 5th year med kids going about asking history taking questions there are certain questions I would not have considered. Also watching how to do a Paediatric exam and what are the major signs and symptoms to be looking out for, I will definitely be using that in future.
I enjoyed the session today and appreciate learning a bit more about the scope of the speech pathologists and what exactly they are able to do and the different assessment tools and the interventional tools they use at different stages.
Collaborative approach to patient care
Students highlighted that simulated sessions offered a platform where health care professionals from different disciplines discussed the problem together to have a better perspective for targeting the patient’s needs. Thus, simulated IPL sessions reinforced the role of teamwork and collaboration as vital components of maximizing positive outcomes for patients.
Really being able to recognize where everyone plays a part so in practices the GP it is important to be able to know when to refer and who to refer to and just have a very good understanding of what is best for the patient.
It had a way of connecting everyone and what you would do and their role in it, so it was not only the baby sick but the developmental side as well, what the speechies do and all the different tests. How would they refer back to the GP if you needed to.
Students also gained a better awareness of shared goals by helping and reaching out to other professionals, which in turn leads to developing respect and confidence among team members. The following responses are examples of the link between IPL and collaborative clinical problem management:
Yes, it was good to learn what other disciplines did and contributed and exactly how we can work together.
You should explore that it should not just be me and you are not alone. Knowing that other people are out there to help support you.
I think the recognition that you are not the only team at the hospital so getting all the Allied Health involved and reaching out.
Competency and skills for future health care practice
Students acknowledged that IPL positively influenced the way in which they would practice interprofessionally in their future careers. Knowing more about the roles and responsibilities of other professionals felt more confident in interacting with practitioners from other professions. The following comments by students demonstrated the ways in which students’ attitudes to teamwork had changed as a result of their participation in a simulated IPL session.
I think working on how to explain things to other health professionals. We just assume their level of knowledge is the same level as ours more so than with a parent so working with you guys is good for my own practice and figuring that out.
Furthermore, students realized that their intervention might be enriched by gaining a greater understanding of the clients’ situations through an interprofessional approach. IPL enabled them to improve their practice and, subsequently, the well-being of the client.
Watching the med students being able to reflect on their practice … you are not really thinking about it and then getting the feedback was really good.
Quite important to have colleagues in other fields so that if you doubt your decision and make a prescription, but you don’t necessarily make the right one for the patient and get a reaction whatever it is.
Students also acknowledge the authenticity of scenarios in not only highlighting the essential nature of teamwork and collaboration but also preparing them for future practice.
Quite interactive which provided a level of complexity to the scenario which if you are if you haven’t done the scenario before added a bit of stress.
Relevance for future rural and remote health care practice
The small size of the professional health care community in rural and remote settings requires regular interactions between rural practitioners. Many times health care providers work beyond their traditional professional boundaries to achieve the best outcome for the patient. These efforts need a greater understanding of other professionals in the community and interprofessional networking. The following comment is indicative of students’ understanding of the importance of strong inter-professional networking in rural settings:
Definitely get to know Allied Health and what services are available and who to refer people to, who does referrals and that sort of thing so in situations you know exactly where to send people.
Often you don’t have the services available, and you need to work more with the pharmacist and learn exactly what they can do and that’s really important because you often don’t have anyone else to talk to or services you can send them to, so good to know you can rely on the pharmacist just to pick things up and what they can contribute and they do have the knowledge to say hey I don’t think this is right or they are having these issues and you give suggestions.
Rural health professionals often work in a geographically isolated location resulting in little support from their discipline, which can be challenging for new graduates.19 Therefore, interventions that help students to recognize the available support in resource-limited settings and how to access and utilize such support might help in managing similar challenges in the future. The participants in this study were vocal about the necessity of a multidisciplinary approach for successful rural practice.
I found on my rural placement that you are in fact don’t have a much support around you and to have a multi-disciplinary team in the area to help you out and follow a patient [sic].
Just knowing what services are available and that you can use technology like tele-conferences and telephones to access them. In a rural area, you don’t have to have a physical person there.
Discussion
The findings of this study demonstrate that simulated interprofessional training could be a potential intervention to facilitate collaborative practice in the rural health care context. Our results highlight that simulated IPL sessions enhance participants’ acquisition of knowledge and recognition of the value of interprofessional care. Students’ perceived that to improve clinical outcomes in a resource-limited rural setting, the health workforce needs to embrace a collaborative clinical culture.
IPL helps students from different disciplines to share knowledge and information about patients or medical issues and promotes the culture of delivering collaborative, holistic care. Understandably, effective teamwork requires collaboration among practitioners, respectful communication, acknowledging each other’s contribution, and knowledge about the role of team members. Simulation-based strategies, e.g., role play and simulation with a computer programmable mannequin with a touch of reality, facilitate students’ learning while achieving the competence required for effective interprofessional practice.20 Simulated IPL sessions expose students to potential future clinical scenarios that improve confidence when facing the real problems in practice, increase their awareness of health professionals’ roles, and facilitate their transition to the workplace.21 Thus, simulated IPL provides a platform for the early development of skills and competence for multidisciplinary approaches and breaks down potential barriers that might be encountered in practice.
Although it is important for all health professionals to appreciate the value of team-based practice in improving patient outcomes, the concept of interprofessional practice is even more relevant for rural practitioners. There is plenty of anecdotal evidence suggesting that rural health care is more interprofessional than in urban centers.22 Simulated IPL session scenarios unique to the rural context are used to highlight the benefits of interprofessional collaboration in managing a variety of medical situations in rural settings. Such collaborative models of care reflect actual rural health care practice and provide students with a better knowledge of holistic rural health service delivery, which help students develop skills in gathering information about services and resources available in a rural community.23
Another significant challenge for rural health care services is poor retention of health care professionals. Some studies suggest that professional isolation and interpersonal conflict contribute to the pressures to leave.24 Therefore, improving skills for effective interprofessional practice at the undergraduate level may potentially influence longer term rural retention.
Although this study is one of the few studies that explored students’ perceptions of the role of simulated IPL activities for rural health care services, it does, however, suffer from some limitations. This study was a single-center study conducted without a control group. Therefore, assessing the comparative effectiveness of simulated IPL session is not straightforward. Additionally, the results are limited to students’ perspective and experiences and do not demonstrate whether positive feedback was sustained in practice. However, previous literature suggests that students who have experienced IPL during their prequalification education are more confident and better professional communicators than students who study under a discipline-specific curriculum.25 While the majority of evidence is based on medicine and nursing students, our study has participants from the pharmacy and Allied Health as well, which is one of the strengths of our study. The fact that we were able to recruit participants from both regional and metropolitan universities also gives credibility to our findings.
Conclusion
This study adds to evidence that health care students perceive a positive impact of simulated IPL activities on their future practice. Based on the results of this study, it seems that simulated IPL activities can be a potential method for facilitating interprofessional collaborative practice. Future research should explore if embedding simulated IPL activities within mainstream curricula will influence professional behavior and whether such changes can be sustained in practice.
Acknowledgment
We acknowledge students who generously gave their time to participate in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
Humphreys JS, Wakerman J, Wells R. What do we mean by sustainable rural health services? Implications for rural health research. Aust J Rural Health. 2006;14(1):33–35. | ||
Strasser R. Rural health around the world: challenges and solutions. Fam Pract. 2003;20(4):457–463. | ||
Battersby MW. Health reform through coordinated care: SA HealthPlus. BMJ. 2005;330(7492):662–665. | ||
McNair R, Stone N, Sims J, Curtis C. Australian evidence for interprofessional education contributing to effective teamwork preparation and interest in rural practice. J Interprof Care. 2005;19(6):579–594. | ||
Joseph S, Diack L, Garton F, Haxton J. Interprofessional education in practice. Clin Teach. 2012;9(1):27–31. | ||
Interprofessional Education Collaborative Expert Panel. Core Competencies for Interprofessional Collaborative Practice: Report of an Expert Panel. Washington, DC: Interprofessional Education Collaborative; 2011. | ||
Freeth D, Reeves S. Learning to work together: using the presage, process, product (3P) model to highlight decisions and possibilities. J Interprof Care. 2004;18(1):43–56. | ||
Walker PH, Baldwin D, Fitzpatrick JJ, et al. Building community: developing skills for interprofessional health professions education and relationship-centered care. J Gerontol Nurs. 1998;24(3):45–49. | ||
Leggat SG. Effective healthcare teams require effective team members: defining teamwork competencies. BMC Health Serv Res. 2007;7:17. | ||
Robertson J, Bandali K. Bridging the gap: enhancing interprofessional education using simulation. J Interprof Care. 2008;22(5):499–508. | ||
Poulton BC, West MA. Effective multidisciplinary teamwork in primary health care. J Adv Nurs. 1993;18(6):918–925. | ||
Whelan JJ, Spencer JF, Rooney KA. ‘RIPPER’ Project: advancing rural inter-professional health education at the University of Tasmania. Rural Remote Health. 2008;8(3):1017. | ||
R2obins L, Brock DM, Gallagher T, et al. Piloting team simulations to assess interprofessional skills. J Interprof Care. 2008;22(3):325–328. | ||
Mulholland P, Barnett T, Spencer J. Interprofessional learning and rural paramedic care. Rural Remote Health. 2014;14(3):2821. | ||
Bottenberg MM, DeWitt JE, Wall GC, et al. Assessment of interprofessional perceptions and attitudes of health professional students in a simulation laboratory setting. Curr Pharm Teach Learn. 2013;5:167–174. | ||
Bandali K, Parker K, Mummery M, Preece M. Skills integration in a simulated and interprofessional environment: an innovative undergraduate applied health curriculum. J Interprof Care. 2008;22(2):179–189. | ||
Palaganas JC, Brunette V, Winslow B. Prelicensure simulation-enhanced interprofessional education: a critical review of the research literature. Simul Healthc. 2016;11(6):404–418. | ||
Lincoln YS, Guba EG. Naturalistic Inquiry. Newbury Park, CA: SAGE; 1985. | ||
Paliadelis PS, Parmenter G, Parker V, Giles M, Higgins I. The challenges confronting clinicians in rural acute care settings: a participatory research project. Rural Remote Health. 2012;12:2017. | ||
Baker C, Pulling C, McGraw R, Dagnone JD, Hopkins-Rosseel D, Medves J. Simulation in interprofessional education for patient-centred collaborative care. J Adv Nurs. 2008;64(4):372–379. | ||
Bandali KS, Craig R, Ziv A. Innovations in applied health: evaluating a simulation-enhanced, interprofessional curriculum. Med Teach. 2012;34(3):e176–e184. | ||
McNair R, Brown R, Stone N, Sims J. Rural interprofessional education: promoting teamwork in primary health care education and practice. Aust J Rural Health. 2001;9(suppl 1):S19–S26. | ||
Reime MH, Johnsgaard T, Kvam FI, et al. Learning by viewing versus learning by doing: a comparative study of observer and participant experiences during an interprofessional simulation training. J Interprof Care. 2017;31(1):51–58. | ||
Hays RB, Veitch PC, Cheers B, Crossland L. Why doctors leave rural practice. Aust J Rural Health. 1997;5(4):198–203. | ||
Pollard K, Rickaby C, Miers M. Evaluating student learning in an interprofessional curriculum: the relevance of pre-qualifying inter-professional education for future professional practice. Health Sciences and Practice, The Higher Education Academy; 2008. Available from: http://eprints.uwe.ac.uk/7240. Accessed June 15, 2017. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.