Back to Journals » Clinical Ophthalmology » Volume 20
Simple Superior Inverted Flap Technique with Extended Internal Limiting Membrane Peeling for the Treatment of Large Macular Holes
Authors Bajdik B, Kemenes G, Jain V, Noronha KM, Fodor M ![]() , Takács L
, Takács L ![]()
Received 31 March 2026
Accepted for publication 13 May 2026
Published 17 June 2026 Volume 2026:20 612899
DOI https://doi.org/10.2147/OPTH.S612899
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yousef Fouad
Supplementary video of “Inverted flap technique for treatment of large macular holes” [612899].
Views: 42
Beáta Bajdik, Gréta Kemenes, Vipasha Jain, Keith Martin Noronha, Mariann Fodor, Lili Takács
University of Debrecen, Faculty of Medicine, Department of Ophthalmology, Debrecen, Hungary
Correspondence: Lili Takács, University of Debrecen, Faculty of Medicine, Department of Ophthalmology, Nagyerdei krt 98, Debrecen, 4032, Hungary, Email [email protected]
Purpose: To evaluate the anatomical and functional outcomes of a simplified superior inverted internal limiting membrane (ILM) flap technique with extended ILM peeling for the surgical treatment of large idiopathic macular holes (iMH).
Patients and Methods: This retrospective, non-randomized, interventional consecutive case series included 42 eyes of 40 patients with iMH. Patients were grouped according to the CLOSE study classification: Group 1: large holes (n=19, minimum linear diameter [MLD] > 400 to ≤ 550 μm), Group 2: extra-large holes (n=18, MLD > 550 to ≤ 800 μm), and Group 3: XXL holes (n=5, MLD > 800 to ≤ 1000 μm). The mean follow-up time was 20.63 ± 18.32 months. The primary endpoint was MH closure rate. Secondary outcomes included closure type, changes in best-corrected visual acuity (BCVA), ellipsoid zone (EZ) defect, flap position, and surgical complications.
Results: Anatomical type 1 closure was achieved in all 42 eyes (100%). The proportion of favorable U-shaped closure decreased significantly with increasing hole size (χ2 = 9.26, df = 2, p = 0.010), with rates of 84.2%, 81.3%, and 20.0% in Groups 1, 2, and 3, respectively. BCVA and EZ defect improved significantly over time in all groups. Final BCVA gain was 4.4 ± 3.3, 6.2 ± 2.7, and 7.3 ± 4.7 ETDRS lines in Groups 1, 2, and 3, respectively, without significant inter-group differences (p > 0.05). Final BCVA correlated with preoperative BCVA (r = 0.51, p < 0.001) and final EZ defect (r = 0.39, p = 0.013), but not with iMH size or symptom duration (p > 0.05). No major complications were observed.
Conclusion: The described surgical technique, involving the combination of a superior inverted ILM flap with extended ILM peeling and minimal manipulation of the posterior pole is highly effective in achieving anatomical and functional success in large iMHs up to 1000 μm, with a favorable safety profile and consistent structural recovery.
Keywords: large macular hole, pars plana vitrectomy, surgical closure, novel surgical technique
Introduction
Idiopathic macular hole (iMH) is a disruption of all neurosensory retinal layers at the foveal center that develops during anomalous posterior vitreous detachment and leads to significant visual loss.1
Successful surgical treatment with pars plana vitrectomy was first reported in 1991 by Kelly and Wendel,2 and the introduction of internal limiting membrane (ILM) peeling by Eckardt in 1997 improved closure rates to 92%.3 Multiple studies have demonstrated the benefits of ILM peeling in closing iMHs and preventing reopening.4,5 Following further surgical modifications, such as the inverted ILM flap technique,6 closure rates of up to 95–100% have been reported.
However, for large iMHs with a minimum linear diameter (MLD) over 400 µm, surgical success rates decline, and in macular holes (MHs) larger than 500 µm, closure rates may fall to 60–85%.7–9 Moreover, closure morphologies associated with worse visual prognosis are more often observed in large holes, such as type 2, or “flat open” closure.10 Even when complete (type 1) closure of the MH is achieved, suboptimal configurations such as V shaped (approximated hole edges without repair of the outer layers) or W shaped (with irregular foveal contour) closure11 may occur. Various surgical techniques have been proposed to improve outcomes in large MHs, including extended ILM peeling,12 different ILM flap techniques,13–16 autologous retinal transplantation,17 amniotic membrane graft,18 and subretinal fluid-assisted MH edge mobilization.19 Recent meta-analyses suggest that both extended ILM peeling and flap techniques improve closure rates in MHs ≥400 µm MLD. ILM flap techniques are effective and safe in large holes, while other techniques are mostly recommended for very large refractory holes due to their procedural complexity or higher complication rates.20–22
Numerous modifications of the ILM flap method have been described, including temporal and superior flaps with limited ILM peeling and flaps trimmed to cover the hole area, with or without more extensive ILM peeling. The shape and orientation of the flap vary as well, with descriptions including clover leaf, retracting door, and pedicle rotational flaps.14,23,24
In earlier studies, the definition of large MH was variable; however, more recent evidence indicates that closure rates decline primarily in holes exceeding 500–550 µm MLD.7 The CLOSE study refined classification by defining size based subgroups: large >400 ≤550 µm, XL >550 ≤800 µm, XXL >800 ≤1000 µm, and giant >1000 µm.8
In this study, we present the outcomes of a simplified superior inverted ILM flap technique (SIFT). This technique combines a superior inverted flap with extended ILM peeling, both considered advantageous in large iMHs. Flap positioning is achieved using suction, without perfluorocarbon liquid or viscoelastic material, to minimize manipulation of the posterior pole.
Materials and Methods
This retrospective, non-randomized, interventional consecutive case series included patients who underwent the simple superior inverted ILM flap technique (SIFT) for full-thickness iMHs with a minimum linear diameter (MLD) ≥400 μm, performed at our institution between January 2019 and June 2025 by one experienced surgeon (LT). The examination protocol of this retrospective study was approved by the Regional and Institutional Ethical Committee of the University of Debrecen Clinical Centre (permission No.: RKEB-7347-2025) and was conducted in accordance with the Helsinki Declaration. Written informed consent to the intervention and to the use of anonymous clinical data for scientific and educational purposes was obtained from all patients before performing the operation.
Clinical charts of 147 consecutive patients were reviewed, and those with iMHs larger than 400 μm (MLD) and operated on with the SIFT technique were selected. The study involved 42 eyes of 40 patients, grouped according to the CLOSE study classification.8 Eyes with high myopia (above −10.0D), traumatic MHs, MHs associated with retinal detachment, or previously operated iMHs that did not close (refractory MHs) were excluded. Seven eyes with iMHs with MLD between 400–500 µm were excluded, because they were operated with ILM peeling only, without flap creation (all reaching type 1 anatomical closure). All iMH cases above 500 µm MLD were operated on with the SIFT technique. Group 1 included 19 eyes with large (L) holes: MLD >400 to ≤550 μm. Group 2 included 18 eyes with extra-large (XL) holes: MLD >550 to ≤800 μm. Group 3 included 5 eyes with XXL holes: MLD >800 to ≤1000 μm. There were no giant holes (MLD >1000 μm) in this cohort. Patients were followed-up for a mean duration of 20.63 ±18.32 months. The primary endpoint was the MH closure rate assessed across groups. Secondary outcomes included closure type, changes in best corrected visual acuity (BCVA), ellipsoid zone (EZ) defect, flap position, and surgical complications.
Snellen BCVA was recorded in decimal notation and converted to logarithm of the minimum angle of resolution (logMAR) for statistical analysis. For standardized interpretation, logMAR values were further converted into Early Treatment Diabetic Retinopathy Study (ETDRS) letter scores using the formula Letters = 85 − 50 × logMAR. Visual improvement was calculated as the difference between preoperative and final logMAR values and expressed in ETDRS letters and lines using the formulas Letters gained = (Preoperative logMAR − Final logMAR) × 50 and Lines gained = (Preoperative logMAR − Final logMAR) × 10.
Surgical Technique
A modified and simplified superior inverted flap technique with extended ILM peeling (SIFT) was employed (Video S1). All patients underwent standard 23-gauge vitrectomy. During surgery, PVD was induced with triamcinolone acetate assistance. Peripheral vitrectomy and vitreous base shaving with indentation were performed, and any peripheral retinal breaks were treated with endolaser photocoagulation. ILM was stained using Brilliant Blue-G 0.025% and Trypan Blue 0.15% (Membrane blue Dual, DORC). The ILM was removed between the major vascular arcades, at least 2 disc diameters in every direction from the center of the fovea, except for the superior flap in the following way: peeling was initiated at the inferior vascular arcade with a diamond-dusted sweeper (DORC) or Finesse Flex loop (Alcon). The ILM was then removed from the inferior part of the macula up to the vascular arcades, pulling toward the center of the MH from the initiation site. Similarly, peeling was initiated on the superior macula, creating 2–3 flower petal-shaped ILM flaps, of which one flap was left attached at the MH edge and trimmed with the vitrector to cover the hole only, the other 1 or 2 flaps were removed by pulling towards the center, similarly to the inferior part of the macula. Fluid-air exchange (FAX) was performed, during which fluid was suctioned to turn the flap onto the hole without forceps manipulation. No viscoelastic material or perfluorocarbon liquid (PFCL) was used during the procedure. If the flap failed to flip over the hole during FAX, a few drops of BSS were injected into the vitreous cavity, and the process was repeated. When epiretinal proliferation (EP) was present, it was left at the edge of the hole, trimmed, and turned onto the MH with the ILM flap. ERM, if present, was removed before ILM peeling. At the end of surgery, the vitreous cavity was filled with 20% SF6 gas, and patients were instructed to maintain face-down positioning for one week. Phacoemulsification was performed simultaneously with the pars plana vitrectomy if the patient was not pseudophakic. Postoperatively, patients were examined at 1, 3, 6, and 12 months, with follow-ups extending up to 60 months. At each visit, best corrected visual acuity (BCVA) was measured using Snellen charts, fundus examination along with spectral-domain OCT (SD-OCT) were performed using the Heidelberg Spectralis or SOLIX OCT platforms, depending on the site of examination. Data regarding closure type, EZ defect size, and flap position were recorded.
Statistical Analysis
Continuous variables are presented as mean ± standard deviation (SD), and categorical variables as counts and percentages. Normality of distribution was assessed using the Shapiro–Wilk test. Comparisons between groups were performed using one-way analysis of variance (ANOVA) for continuous variables and the chi-square (χ2) test for categorical variables. All statistical tests were two-tailed, and a p-value < 0.05 was considered statistically significant. Correlations were analyzed using Spearman’s rank correlation coefficient (r). Correlation matrices were visualized using triangular heat maps, with positive correlations shown in red, negative correlations in blue, and neutral values in white. Statistical significance was indicated as *p < 0.05, **p < 0.01, and ***p < 0.001. Statistical analyses were performed using IBM SPSS Statistics (version 24.0; IBM Corp., Armonk, NY).
Results
Patient baseline demographic characteristics are summarized in Table 1. There were no differences in age, gender, symptom duration, preoperative BCVA, or mean follow-up time between groups. Anatomical closure (type 1) was achieved in all cases across all groups (100%). However, the proportion of U-shaped closure decreased markedly with increasing hole size, from 89.5% in 400–550 µm to 81.3% in 550–800 µm and 20.0% in >800 µm (χ2=9.26, df=2, p=0.0098). Post-hoc comparisons demonstrated that eyes with holes >800 µm had significantly lower rates of U-shaped closure compared to both smaller groups, while no significant difference was observed between the 400–550 µm and 550–800 µm (Figure 1). In Figure 2a, a typical U-shaped closure pattern of a 625 µm MH is shown, where regeneration of the outer layers under the flap is observed with a small residual EZ defect at 12M postoperatively. Importantly, centripetal migration of the outer retinal layers beneath the flap was observed during follow-up, with progressive improvement in closure configuration. First, ELM continuity was reestablished, then the initial EZ defect decreased (Figures 2b and 3c). Such regeneration was seen in every case with good flap positioning. Only one case showed minimal migration of the outer layers (as described in the next paragraph). No major complications occurred.
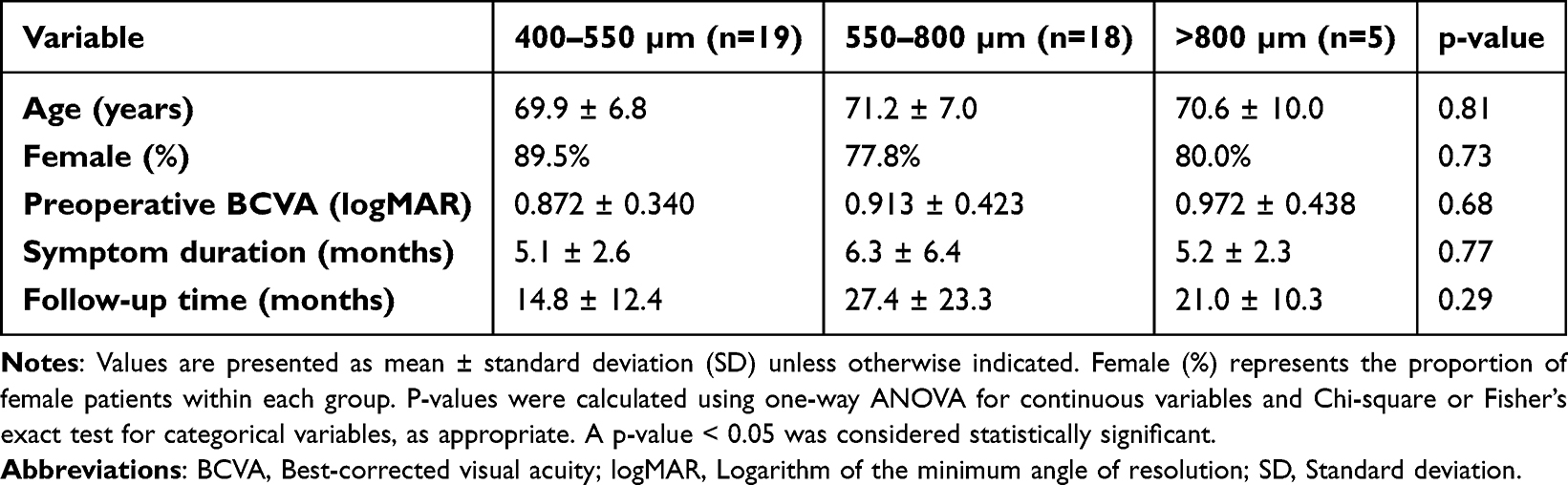 |
Table 1 Baseline Characteristics of Patients Grouped by Macular Hole Size |
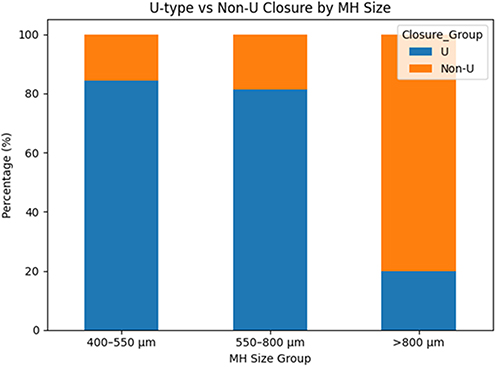 |
Figure 1 Closure morphology was significantly associated with macular hole size (χ2 = 9.26, df = 2, p = 0.0098). The proportion of U-shaped closure decreased markedly with increasing hole size, from 89.5% in 400–550 µm to 81.3% in 550–800 µm and 20.0% in >800 µm. Post-hoc comparisons demonstrated that eyes with holes >800 µm had significantly lower rates of U-shaped closure compared to both smaller groups, while no significant difference was observed between the 400–550 µm and 550–800 µm groups. |
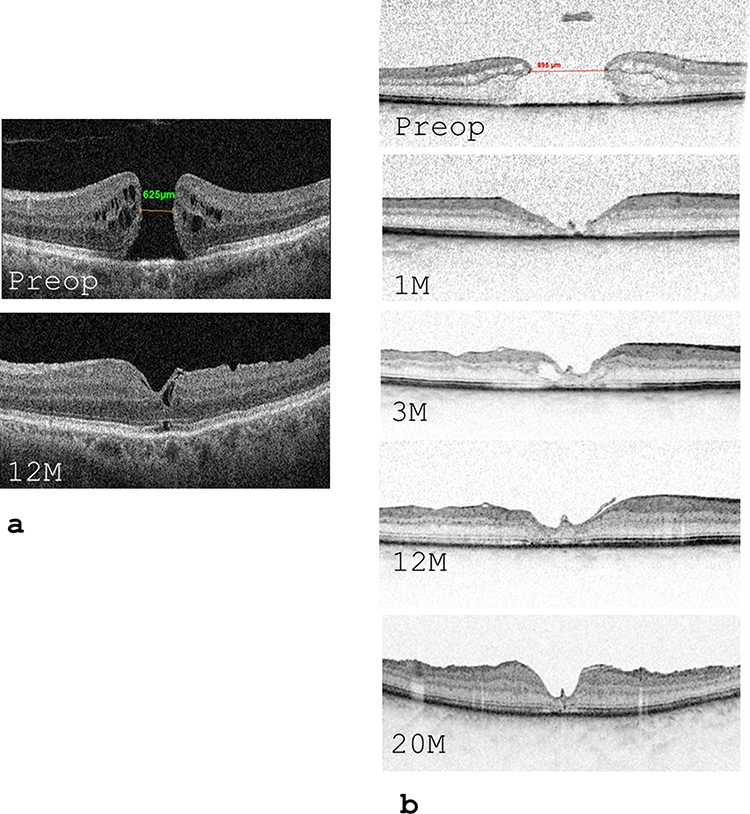 |
Figure 2 MH closure after operation with the simple inverted ILM flap technique (SIFT). (a) Typical closure pattern of a XL hole: in a 625 µm MH, regeneration of the outer layers under the flap is observed, with closed ONL and ELM, but remaining little EZ defect 12M postoperatively. (b) In a patient with XXL 895 µm MH, initial W shaped closure is seen at 1M, subsequently, a slow regeneration of the outer layers is seen under the flap, with partial regeneration of the ONL, ELM and EZ layer by the 20M visit. |
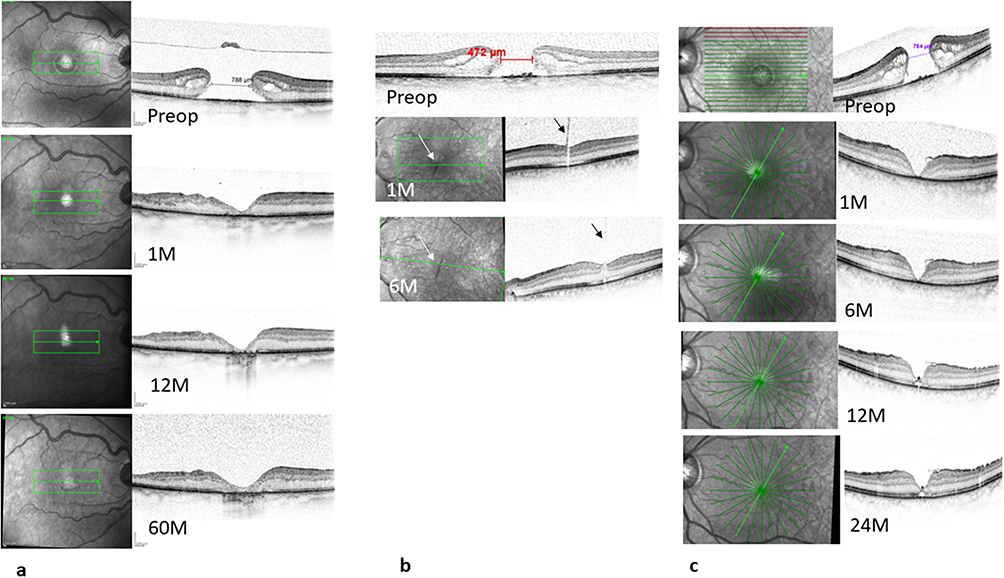 |
Figure 3 Three minor complications were observed. (a) A 72 year old lady had a 788 µm MH and a central RPE defect. During FAX, the ILM flap was lost. In spite of this, the MH was closed with a V type closure. Subsequently, the RPE defect enlarged and glial tissue was observed in the central macula. The ELM, EZ or ONL layers did not regenerate over the very long follow-up time. (b) In a patient who could not keep face-down position, flap displacement occurred (arrows) but the MH closed with a U-shaped pattern and partial EZ recovery was also observed by 6M. (c) A patient with a 784 µm MH could not keep face_down position. The ILM flap was partially displaced and an initial V-shaped closure was observed. Later, the ELM closed under the flap and significant EZ restauration was also observed and a deep U shaped closure was observed at the 14M visit. |
Three minor complications were noted. In one case (MLD 788μm), ILM flap was lost during FAX. After flap loss, massaging of the hole edges was attempted, the case was finalized with 20% SF6 fill and the patient was asked to keep face-down position for one week. This case also demonstrated a round central retinal pigment epithelial (RPE) defect that enlarged during the postoperative follow-up and surgical manipulation possibly contributed to its enlargement. During a very long follow-up period (60M), EZ and ELM defect persisted, possibly due to the concurrent RPE defect, although glial proliferation could be observed in the foveal area, which ensured type 1 anatomical closure (Figure 3a). In two cases, patients were unable to maintain face-down positioning. In one (MLD 472 µm), flap displacement occurred; however, the MH remained closed (Figure 3b). In the other case (MLD 784 μm), a V-shaped closure was detected with the flap covering approximately 2/3 of the hole; however, outer-layer morphology progressively improved beneath the flap, achieving a deep U-shaped configuration by the 24-month visit (Figure 3c).
Best corrected visual acuity significantly improved in all groups at 1, 3, 6 months, and final follow-up (Figure 4a, Table 2 and Table 3). There was no significant difference in the BCVA between groups at any time point (Table 2). The final BCVA gain was 4.4±3.3, 6.2±2.7 and 7.3±4.7 ETDRS lines in Groups 1, 2 and 3, respectively (Table 3). Alongside BCVA improvement, a decrease in the EZ defect was observed across all groups (Figure 4b). Larger holes demonstrated greater initial EZ disruption and a tendency toward larger defects at follow-up; however, no statistically significant differences were observed between groups at any postoperative time point (all p > 0.05, Table 4). Correlation analysis demonstrated strong positive associations between EZ defect measurements across postoperative time points (up to r = 0.94, p < 0.001), indicating high temporal consistency of structural recovery. Similarly, BCVA measurements were strongly correlated over time (up to r = 0.88, p < 0.001). Final BCVA showed a moderate correlation with preoperative BCVA (r = 0.51, p < 0.001) and final EZ defect (r = 0.39, p = 0.013). In contrast, no significant correlations were found between final BCVA and MH size or symptom duration (Figure 5).
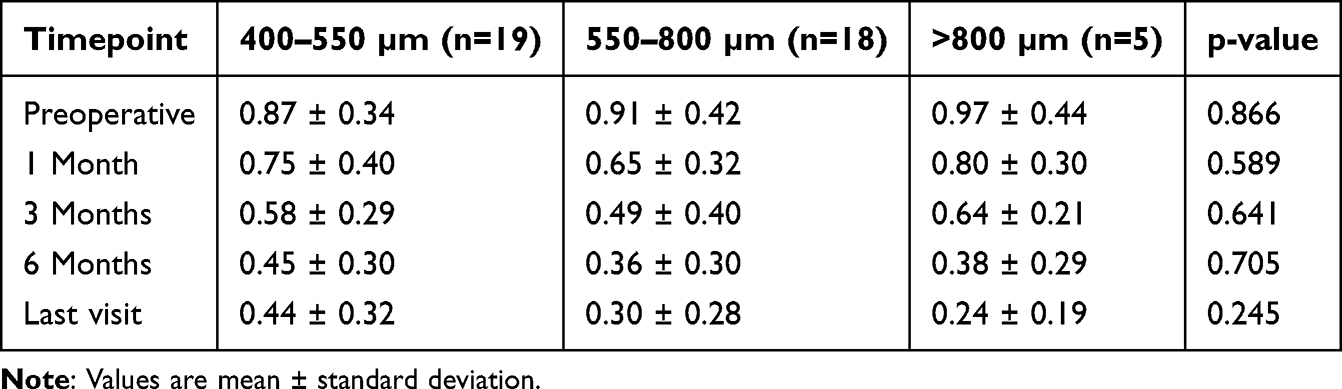 |
Table 2 Changes in BCVA(LogMar) After Surgery According to Macular Hole Size |
 |
Table 3 Visual Acuity Improvement |
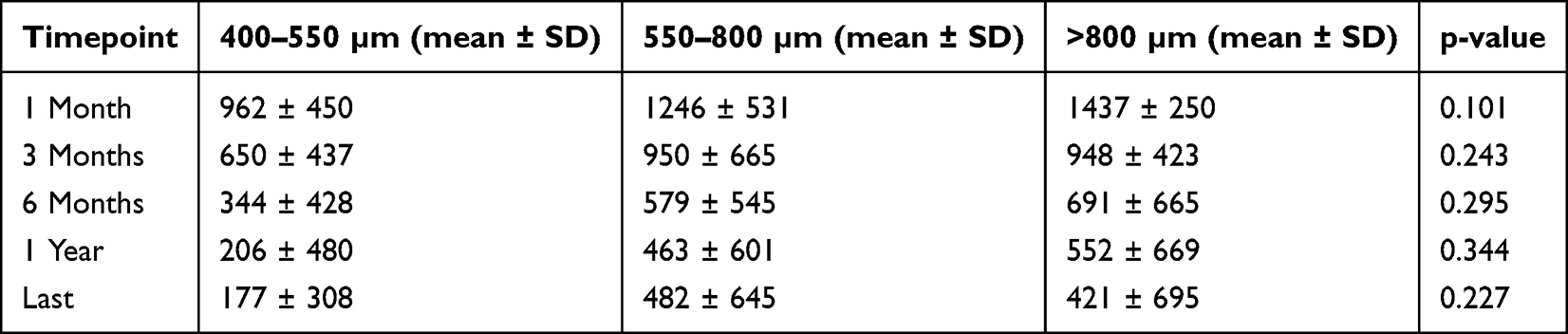 |
Table 4 EZ Defect Size Over Time According to Macular Hole Size |
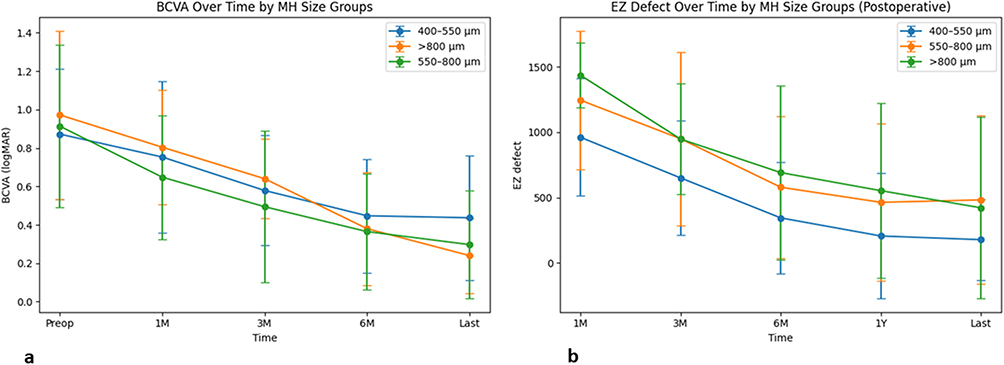 |
Figure 4 (a) Change in best corrected visual acuity (BCVA) over time after surgery. (b) Change in ellipsoid zone (EZ) defect over time after surgery. |
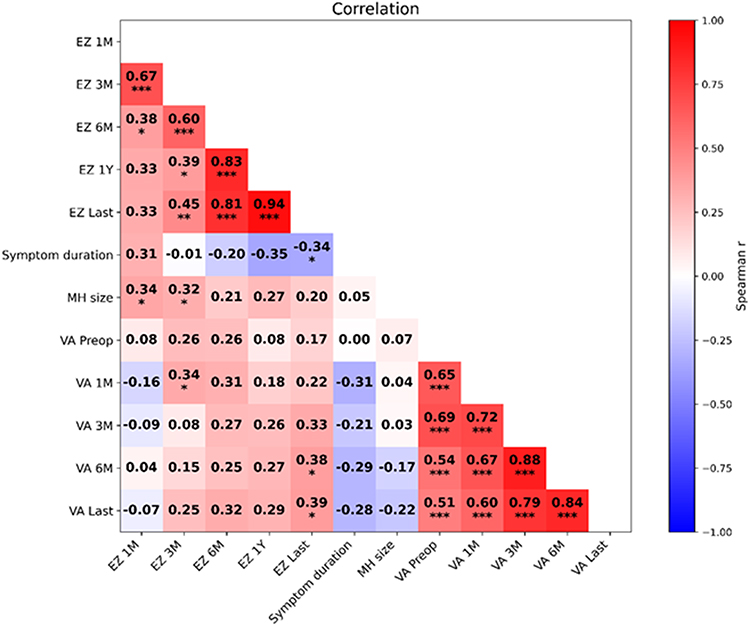 |
Figure 5 Spearman correlation heatmap demonstrating relationships between BCVA at different time points, EZ defect measurements, MH size and symptom duration. Positive correlations are shown in red, negative correlations in blue, and weak or absent correlations in white. Statistical significance is indicated by asterisks (*p < 0.05, **p < 0.01, ***p < 0.001). |
Discussion
In this report, we present the results of a simplified superior inverted ILM flap technique (SIFT) for treating large iMHs. The method is a simplified modification of the superior inverted ILM flap technique,16 combined with enlargement of ILM peeling up to the vascular arcades. Type 1 anatomical closure and significant functional improvement were achieved in all our cases treated with this method. The SIFT technique represents a novel incremental refinement of the superior ILM flap technique that may contribute to increased MH closure in several ways:
1) The extended peeling area improves retinal compliance and encourages centripetal migration of MH edges. Similarly, enlargement of the ILM peel up to the vascular arcades has been shown to be beneficial in extra-large holes and refractory MH cases.12,25 2) Pulling ILM pieces toward the center during peeling may further enhance MH edge mobilization. Recently, in the APOSTEL study, mobilizing MH edges by injecting fluid subretinally effectively promoted closure in refractory MHs.19 Massaging the MH edges toward the center26 was shown to aid closure as well. 3) The single-layer inverted ILM flap acts as a scaffold and promotes centripetal migration of outer layers, as demonstrated by many studies using various flap techniques („flap closure”).27,28 4) Trimming the inverted ILM flap to the size of the MH ensures adequate coverage but prevents potential fibrosis and shrinkage of the ILM flap, which can cause long-term visual disturbances, seen in some previous studies with large ILM flaps.29,30 5) Minimizing manipulation around the hole by flipping the flap over the MH using only suction, without viscoelastic material or PFCL, helps preserve the foveal structure.31,32
While the large-area ILM removal in SIFT offers benefits, it may also harm Müller cell pedicles and lead to dissociated optic nerve fiber layer (DONFL). Initially, DONFL was thought to reduce macular sensitivity.33,34 However, a recent study showed that decreased retinal sensitivity after ERM peeling correlates with outer and inner retinal layer damage caused by ERM, rather than the presence of DONFL.35 Furthermore, a randomized trial found similar DONFL scores whether ILM was peeled only temporally or circumferentially around the MH, with comparable retinal sensitivity in both groups.36 Functional outcomes tend to be poorer if secondary surgery is required due to failed MH closure, making primary closure preferable.31 We believe that the BCVA gains and 100% primary closure rate observed in our patients outweigh any subtle functional issues related to larger ILM peel areas.
Most studies have suggested that final visual recovery depends on MH size.37–39 We could not demonstrate such an association. This may be due to the long (> 1-year) follow-up in most of our cases. During this period, significant visual recovery and EZ repair were observed even in very large (800–1000 μm) holes. In a previous study, continuous visual improvement was seen for at least 3 years after MH surgery,40 and centripetal migration of photoreceptor cells was suggested during MH recovery.28 A recent study confirmed increased spacing and dispersion of photoreceptors (PRs) near the MH edges, indicating that stretching/elongation of the PR layer may play a role during MH repair.41 The ILM flap placed over the MH acts as a scaffold for MH closure,27 and RPE cells can promote photoreceptor migration toward the centre.28 In fact, in one case where we experienced flap loss and the patient had a central RPE defect, central EZ restoration was not observed, and VA recovery remained modest.
An important observation in our study is that long-term postoperative BCVA correlated only with preoperative BCVA. Similar associations were found in other studies as well.9,42 This suggests that the repair processes seen after successful closure—such as ELM closure, inward migration of the outer retinal layers, and decreasing EZ defects—occur even in very large holes, and long-term visual recovery may depend on initial PR damage, as previously suggested by our group.43 Unlike in other studies,9 the duration of symptoms before surgery did not significantly influence final BCVA in our cohort. After MH opening, photoreceptors at the MH edges elevate from the RPE and contact the hypoosmotic vitreous fluid, leading to gradual deterioration of the photoreceptor bacillary layer. The transition from swelling to more pronounced loss was observed after a mean duration of ≈280 days.44 Most of our patients were operated on within this timeframe, before severe PR loss occurred, which likely explains why we could not observe a significant correlation with symptom duration.
We advised our patients to maintain face-down positioning for one week. Studies have shown that with superior flaps, prone positioning may not be necessary.13,16 Other research has suggested that face-down positioning offers advantages in large holes.45 We observed flap displacements in cases when patients could not remain in a prone position. In the first case (421 μm hole), the closure was complete despite displacement; in the second, most of the flap remained in place, and the EZ layer recovered on the long-term under the flap, with significant BCVA improvement. Nonetheless, we recommend that maintaining face-down positioning for several days may be prudent in cases of large holes, even when using superior inverted flaps.
While the results demonstrate a high anatomical closure rate and favorable functional recovery, several limitations must be considered.
First, the retrospective design and lack of a control group preclude direct comparison with standard ILM peeling or alternative flap techniques. Therefore, no conclusions regarding superiority can be drawn. Second, the small number of cases in the XXL group limits the statistical power of subgroup analyses. Third, the use of two different OCT platforms (Spectralis and SOLIX) may introduce variability in EZ defect measurements, although imaging protocols were applied consistently within each device.
Although this study involved consecutive iMH cases, more challenging MHs secondary to trauma or high myopia as well as giant and refractory holes were not included. The 100% closure rate observed in this cohort is encouraging but should be interpreted with caution, and usefulness of this technique in challenging cases must be further examined.
Conclusion
The simple superior inverted ILM flap technique (SIFT) described in this study is a safe and highly effective method for closing large iMHs up to 1000 µm. In this cohort, a 100% type 1 anatomical closure rate was achieved, accompanied by the gradual recovery of the outer retinal layers under the flap and parallel improvement in BCVA over the long term, even in very large holes. No significant surgery-related complications were observed. However, further prospective, controlled studies are required to confirm these findings and to compare outcomes with other established surgical techniques.
Acknowledgement
We acknowledge the financial support from the University of Debrecen Program for Scientific Publication.
Disclosure
Dr Lili Takács reports meeting/travel support from OPC Hungary, Roche Hungary, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Duker JS, Kaiser PK, Binder S, et al. The International Vitreomacular Traction Study Group classification of vitreomacular adhesion, traction, and macular hole. Ophthalmology. 2013;120(12):2611–10. doi:10.1016/j.ophtha.2013.07.042
2. Kelly NE, Wendel RT. Vitreous surgery for idiopathic macular holes. Results of a pilot study. Arch Ophthalmol. 1991;109(5):654–659. doi:10.1001/archopht.1991.01080050068031
3. Eckardt C, Eckardt U, Groos S, et al. [Removal of the internal limiting membrane in macular holes. Clinical and morphological findings]. Ophthalmologe. 1997;94(8):545–551. German. doi:10.1007/s003470050156
4. Mester V, Kuhn F. Internal limiting membrane removal in the management of full-thickness macular holes. Am J Ophthalmol. 2000;129(6):769–777. doi:10.1016/s0002-9394(00)00358-5
5. Rahimy E, McCannel CA. Impact of internal limiting membrane peeling on macular hole reopening: a systematic review and meta-analysis. Retina. 2016;36(4):679–687. doi:10.1097/IAE.0000000000000782
6. Michalewska Z, Michalewski J, Adelman RA, et al. Inverted internal limiting membrane flap technique for large macular holes. Ophthalmology. 2010;117(10):2018–2025. doi:10.1016/j.ophtha.2010.02.011
7. Ch’ng SW, Patton N, Ahmed M, et al. The manchester large macular hole study: is it time to reclassify large macular holes? Am J Ophthalmol. 2018;195:36–42. doi:10.1016/j.ajo.2018.07.027
8. Rezende FA, Ferreira BG, Rampakakis E, et al. Surgical classification for large macular hole: based on different surgical techniques results: the CLOSE study group. Int J Retina Vitreous. 2023;9(1):4. doi:10.1186/s40942-022-00439-4
9. Steel DH, Donachie PHJ, Aylward GW, et al. Factors affecting anatomical and visual outcome after macular hole surgery: findings from a large prospective UK cohort. Eye. 2021;35(1):316–325. doi:10.1038/s41433-020-0844-x
10. Kang SW, Ahn K, Ham DI. Types of macular hole closure and their clinical implications. Br J Ophthalmol. 2003;87(8):1015–1019. doi:10.1136/bjo.87.8.1015
11. Michalewska Z, Michalewski J, Cisiecki S, et al. Correlation between foveal structure and visual outcome following macular hole surgery: a spectral optical coherence tomography study. Graefes Arch Clin Exp Ophthalmol. 2008;246(6):823–830. doi:10.1007/s00417-007-0764-5
12. Al Sabti K, Kumar N, Azad RV. Extended internal limiting membrane peeling in the management of unusually large macular holes. Ophthalmic Surg Lasers Imaging. 2009;40(2):185–187. doi:10.3928/15428877-20090301-03
13. Choi SR, Kang JW, Jeon JH, et al. The efficacy of superior inverted internal limiting membrane flap technique for the treatment of full-thickness macular hole. Retina. 2018;38(1):192–197. doi:10.1097/IAE.0000000000001619
14. Hu Z, Ye X, Lv X, et al. Non-inverted pedicle internal limiting membrane transposition for large macular holes. Eye. 2018;32(9):1512–1518. doi:10.1038/s41433-018-0107-2
15. Michalewska Z, Michalewski J, Dulczewska-Cichecka K, et al. Temporal inverted internal limiting membrane flap technique versus classic inverted internal limiting membrane flap technique: a Comparative Study. Retina. 2015;35(9):1844–1850. doi:10.1097/IAE.0000000000000555
16. Shin MK, Park KH, Park SW, et al. Perfluoro-n-octane-assisted single-layered inverted internal limiting membrane flap technique for macular hole surgery. Retina. 2014;34(9):1905–1910. doi:10.1097/IAE.0000000000000339
17. Grewal DS, Mahmoud TH. Autologous neurosensory retinal free flap for closure of refractory myopic macular holes. JAMA Ophthalmol. 2016;134(2):229–230. doi:10.1001/jamaophthalmol.2015.5237
18. Rizzo S, Caporossi T, Tartaro R, et al. A human amniotic membrane plug to promote retinal breaks repair and recurrent macular hole closure. Retina. 2019;39(Suppl 1):S95–S103. doi:10.1097/IAE.0000000000002320
19. Meyer CH, Szurman P, Haritoglou C, et al. Application of subretinal fluid to close refractory full thickness macular holes: treatment strategies and primary outcome: APOSTEL study. Graefes Arch Clin Exp Ophthalmol. 2020;258(10):2151–2161. doi:10.1007/s00417-020-04735-3
20. Hanai M, Amaral DC, Jacometti R, et al. Large macular hole and autologous retinal transplantation: a systematic review and meta-analysis. Int J Retina Vitreous. 2024;10(1):56. doi:10.1186/s40942-024-00573-1
21. Quiroz-Reyes MA, Quiroz-Gonzalez EA, Quiroz-Gonzalez MA, et al. Effect of internal limiting membrane surgical techniques on the idiopathic and refractory management of macular holes: a systematic review and meta-analysis. Int J Retina Vitreous. 2024;10(1):44. doi:10.1186/s40942-024-00564-2
22. Teh BL, Li Y, Nanji K, et al. Internal limiting membrane peel size and macular hole surgery outcome: a systematic review and individual participant data study of randomized controlled trials. Eye. 2025;39(7):1406–1413. doi:10.1038/s41433-025-03666-9
23. Felfeli T, Yin GS, Shwarzman R, et al. The cloverleaf internal limiting membrane flap technique for repair of challenging macular holes. Retina. 2025;45(11):2169–2174. doi:10.1097/IAE.0000000000004446
24. Finn AP, Mahmoud TH. Internal limiting membrane retracting door for myopic macular holes. Retina. 2019;39(Suppl 1):S92–S94. doi:10.1097/IAE.0000000000001787
25. Che X, He F, Lu L, et al. Evaluation of secondary surgery to enlarge the peeling of the internal limiting membrane following the failed surgery of idiopathic macular holes. Exp Ther Med. 2014;7(3):742–746. doi:10.3892/etm.2014.1477
26. Chakraborty D, Sengupta S, Mukherjee A, et al. Anatomical and functional outcomes one year after vitrectomy and retinal massage for large macular holes. Indian J Ophthalmol. 2021;69(4):895–899. doi:10.4103/ijo.IJO_1680_20
27. Boninska K, Nawrocki J, Michalewska Z. Mechanism of “Flap Closure” after the inverted internal limiting membrane flap technique. Retina. 2018;38(11):2184–2189. doi:10.1097/IAE.0000000000001861
28. Spaide RF. Healing mechanisms after macular hole repair suggests process of foveation. Retina. 2023;43(4):539–546. doi:10.1097/IAE.0000000000003727
29. Hirata A, Takano A, Kawaji T, et al. Macular pucker formation after macular hole surgery with inverted internal limiting membrane flap technique and silicone oil tamponade. Am J Ophthalmol Case Rep. 2020;19:100847. doi:10.1016/j.ajoc.2020.100847
30. Mase Y, Matsubara H, Ueji N, et al. Development of secondary epiretinal membrane after vitrectomy with inverted ILM flap technique to treat a macular hole. Am J Ophthalmol Case Rep. 2025;39:102416. doi:10.1016/j.ajoc.2025.102416
31. Chatziralli IP, Theodossiadis PG, Steel DHW. Internal limiting membrane peeling in macular hole surgery; why, when, and how? Retina. 2018;38(5):870–882. doi:10.1097/IAE.0000000000001959
32. Ghassemi F, Khojasteh H, Khodabande A, et al. Comparison of three different techniques of inverted internal limiting membrane flap in treatment of large idiopathic full-thickness macular hole. Clin Ophthalmol. 2019;13:2599–2606. doi:10.2147/OPTH.S236169
33. Tadayoni R, Svorenova I, Erginay A, et al. Decreased retinal sensitivity after internal limiting membrane peeling for macular hole surgery. Br J Ophthalmol. 2012;96(12):1513–1516. doi:10.1136/bjophthalmol-2012-302035
34. Terasaki H, Miyake Y, Nomura R, et al. Focal macular ERGs in eyes after removal of macular ILM during macular hole surgery. Invest Ophthalmol Vis Sci. 2001;42(1):229–234.
35. Matos AMF, Defina RLS, Costa-Cunha LVF, et al. Correlation between retinal sensitivity assessed by microperimetry and structural abnormalities on optical coherence tomography after successful epiretinal membrane surgery. Int J Retina Vitreous. 2024;10(1):24. doi:10.1186/s40942-024-00542-8
36. Ehrhardt A, Delpuech M, Luc A, et al. Dissociated optic nerve fiber layer appearance after macular hole surgery: a randomized controlled trial comparing the temporal inverted internal limiting membrane flap technique with conventional peeling. Ophthalmol Retina. 2023;7(3):227–235. doi:10.1016/j.oret.2022.09.002
37. Ruiz-Moreno JM, Staicu C, Pinero DP, et al. Optical coherence tomography predictive factors for macular hole surgery outcome. Br J Ophthalmol. 2008;92(5):640–644. doi:10.1136/bjo.2007.136176
38. Ullrich S, Haritoglou C, Gass C, et al. Macular hole size as a prognostic factor in macular hole surgery. Br J Ophthalmol. 2002;86(4):390–393. doi:10.1136/bjo.86.4.390
39. Wakely L, Rahman R, Stephenson J. A comparison of several methods of macular hole measurement using optical coherence tomography, and their value in predicting anatomical and visual outcomes. Br J Ophthalmol. 2012;96(7):1003–1007. doi:10.1136/bjophthalmol-2011-301287
40. Elhusseiny AM, Schwartz SG, Flynn HW Jr, et al. Long-term outcomes after macular hole surgery. Ophthalmol Retina. 2020;4(4):369–376. doi:10.1016/j.oret.2019.09.015
41. Oquendo PL, Wright T, Naidu SC, et al. Comparison of the photoreceptor mosaic before and after macular hole surgery with high-resolution adaptive optics imaging. Am J Ophthalmol. 2025;270:261–272. doi:10.1016/j.ajo.2024.10.018
42. Obata S, Ichiyama Y, Kakinoki M, et al. Prediction of postoperative visual acuity after vitrectomy for macular hole using deep learning-based artificial intelligence. Graefes Arch Clin Exp Ophthalmol. 2022;260(4):1113–1123. doi:10.1007/s00417-021-05427-2
43. Bajdik B, Vajas A, Kemenes G, et al. Prediction of long-term visual outcome of idiopathic full-thickness macular hole surgery using optical coherence tomography parameters that estimate potential preoperative photoreceptor damage. Graefes Arch Clin Exp Ophthalmol. 2024;262(10):3181–3189. doi:10.1007/s00417-024-06500-2
44. Pecaku A, Melo IM, Cao JA, et al. Morphologic stages of full-thickness macular hole on spectral-domain OCT. Ophthalmol Retina. 2025;9(4):305–313. doi:10.1016/j.oret.2024.10.018
45. Raimondi R, Tzoumas N, Toh S, et al. Facedown positioning in macular hole surgery: a systematic review and individual participant data meta-analysis. Ophthalmology. 2025;132(2):194–205. doi:10.1016/j.ophtha.2024.08.012
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.