Back to Journals » International Journal of Women's Health » Volume 18
Silent but Destructive: Ureteral Deep Infiltrating Endometriosis Progressing to Renal Injury – A Case Report
Authors Asmara EC ![]() , Rachmawati A, Nisa AS
, Rachmawati A, Nisa AS ![]() , Syam HH
, Syam HH ![]()
Received 2 March 2026
Accepted for publication 6 June 2026
Published 18 June 2026 Volume 2026:18 605680
DOI https://doi.org/10.2147/IJWH.S605680
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Erick Caesarrani Asmara, Anita Rachmawati, Aisyah Shofiatun Nisa, Hanom Husni Syam
Department of Obstetrics and Gynecology, Hasan Sadikin General Hospital-Padjadjaran University, Bandung, Indonesia
Correspondence: Erick Caesarrani Asmara, Department of Obstetrics and Gynecology, Hasan Sadikin General Hospital-Padjadjaran University, Pasteur 38, Bandung, Indonesia, Tel +62 821 1533 5095, Email [email protected]
Background: Ureteral endometriosis is a rare form of deep infiltrating endometriosis that may lead to silent ureteral obstruction and progressive renal injury. Early diagnosis remains challenging because symptoms are often nonspecific.
Case Report: A 41-year-old nulliparous woman presented with lower abdominal pain radiating to the rectum and thigh. Pelvic examination revealed an immobile posterior cervical mass. Transvaginal ultrasound demonstrated a deep infiltrating endometriosis nodule associated with hydroureter and grade IV hydronephrosis, which was confirmed by magnetic resonance imaging. Surgical management was recommended; however, the patient declined surgery and opted for conservative treatment. She received monthly leuprolide acetate injections for three months. Follow-up evaluation showed reduction in lesion size and improvement in pain symptoms.
Conclusion: Ureteral endometriosis should be considered in reproductive-age women with unexplained hydroureteronephrosis. Hormonal therapy may provide temporary symptom control in patients refusing surgery, although careful follow-up is required because of the risk of ongoing renal damage.
Keywords: ureteral endometriosis, deep infiltrating endometriosis, hydronephrosis, hormonal therapy
Introduction
Endometriosis affects approximately 5–10% of women of reproductive age worldwide, with pooled prevalence estimates ranging from 1.0% in population-based studies to 5.0% in self-reported cohorts and an overall incidence of 1.4 to 3.5 cases per 1000 person-years.1,2 Although peritoneal and ovarian lesions constitute the majority of cases, the ureter is involved in fewer than 1% of all endometriosis patients, with urinary tract endometriosis accounting for less than 10% of surgical diagnoses and ureteral involvement comprising only a quarter of these urinary lesions.3 Such figures underline the rarity of ureteral endometriosis and its potential for delayed diagnosis due to non-specific presentations and the lack of population-based surveillance data.1,2
Ureteral endometriosis is commonly categorized into intrinsic and extrinsic types according to the depth of ureteral involvement. Intrinsic disease involves infiltration of the ureteral wall, whereas extrinsic disease is characterized by periureteral fibrosis and external compression without direct mucosal invasion. Although this distinction has become less emphasized in recent literature because overlapping pathological features are frequently observed, it remains clinically important because the extent of ureteral infiltration may influence the choice of surgical management and postoperative outcomes.4,5 Severe intrinsic involvement or advanced obstruction may require ureteral resection and reconstruction, while selected extrinsic lesions may be managed more conservatively.4,5
Ureteral endometriosis, characterized by fibrotic lesions causing extrinsic ureteral compression or intrinsic infiltration, may lead to silent renal obstruction and irreversible renal damage if not promptly identified.3 Clinical manifestations often include flank pain, hematuria, or incidental hydronephrosis on imaging, but up to 50% of patients present without urologic symptoms.3 Although multiple reviews on urinary tract endometriosis have been published, most available evidence regarding diagnosis and treatment continues to originate from retrospective studies, small case series, and case reports due to the rarity of the disease.5 Consequently, no universally accepted diagnostic algorithm currently exists, and early recognition still depends largely on clinical suspicion combined with imaging and histopathological confirmation.
When patients decline surgical intervention, conservative hormonal therapy offers a non-invasive alternative aimed at suppressing ectopic endometrial tissue and alleviating ureteral compression. Gonadotropin-releasing hormone agonists, progestins, and combined oral contraceptives have demonstrated efficacy in reducing lesion size and improving hydronephrosis in selected patients, although treatment response may be incomplete in cases with extensive fibrosis.6 Therefore, close imaging and renal function follow-up are essential during conservative management to prevent progressive renal impairment.
However, in this case, ureteral endometriosis was not diagnosed at an early stage, resulting in a severe complication characterized by a decline in renal function to approximately 10% of its remaining capacity. This condition reflects the serious consequences of undetected chronic ureteral obstruction, which ultimately leads to progressive renal damage and the potential for permanent loss of kidney function.
Case Illustration
A 41-year-old Asian nulliparous woman was referred from a regional hospital with a diagnosis of an ovarian cyst. The patient had been experiencing abdominal pain for one year before admission, which had progressively worsened over the past four months. The pain was predominantly associated with menstruation. It was described as a dull, persistent ache radiating posteriorly to the rectum and extending distally to both thighs. Over the last few months, the pain had significantly intensified and markedly interfered with her daily activities and quality of life (VAS 10). To relieve the pain, the patient had been taking Dexketoprofen.
She reported regular menstrual cycles every 25–28 days, lasting 5–7 days, with menstrual bleeding requiring 2–3 sanitary pads per day. She denied any abdominal mass, abnormal uterine bleeding, vaginal discharge, urinary or bowel complaints, weight loss, or decreased appetite. Cervical cancer screening history, including Pap smear and HPV testing, was unavailable because the patient had not undergone prior screening before referral. Mammography was also not performed, as the referring hospital did not have mammography facilities and there were no clinical findings suggestive of breast pathology. There was no family history of malignancy. The patient had a previous history of laparotomy for appendectomy. Physical examination revealed no obvious abnormalities. However, digital rectal examination identified a firm, immobile mass located at the right posterior aspect of the cervix. The mass measured approximately 5×4 × 4 cm, with a solid consistency and irregular surface.
Transvaginal ultrasonography demonstrated findings consistent with deep infiltrating endometriosis (DIE), particularly a suspected DIE nodule located at the lower right posterior aspect of the uterus. The nodule measured 2.65 cm in its longest diameter and 1.56 cm in its shortest diameter, with echogenic characteristics typical of endometriotic tissue (Figure 1A). Importantly, the ultrasound examination also revealed right hydronephrosis (Figure 1B), extrinsic ureteral compression secondary to deep infiltrating endometriosis. These findings indicated advanced disease with possible infiltration into adjacent pelvic structures.
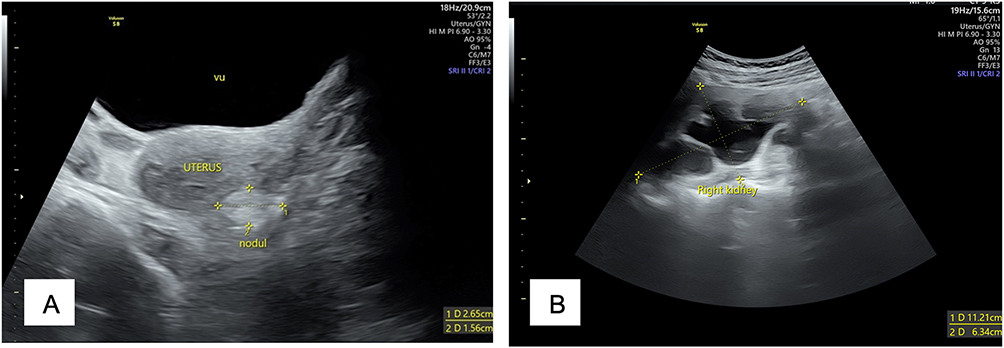 |
Figure 1 Ultrasonography examination. (A) Transvaginal ultrasonography demonstrating VU (vesica urinaria, urinary bladder) and a deep infiltrating endometriosis (DIE) nodule located at the lower right posterior aspect of the uterus. The lesion measured 2.65×1.56 cm and exhibited echogenic characteristics consistent with endometriotic tissue; (B) Ultrasonographic image showing right-sided hydronephrosis characterized by dilation of the renal pelvis and calyces, suggestive of ureteral obstruction secondary to deep infiltrating endometriosis. |
Further evaluation with magnetic resonance imaging (MRI) provided more detailed assessment of disease extent and confirmed significant urological complications. The MRI revealed right hydroureter and grade IV hydronephrosis of the right kidney, representing severe dilation of the renal collecting system (Figure 2). These findings demonstrated serious urinary tract involvement by the endometriotic process, with a high risk of permanent renal damage if left untreated. The imaging characteristics were consistent with deep infiltrating endometriosis involving the posterior pelvic compartment with secondary genitourinary involvement.
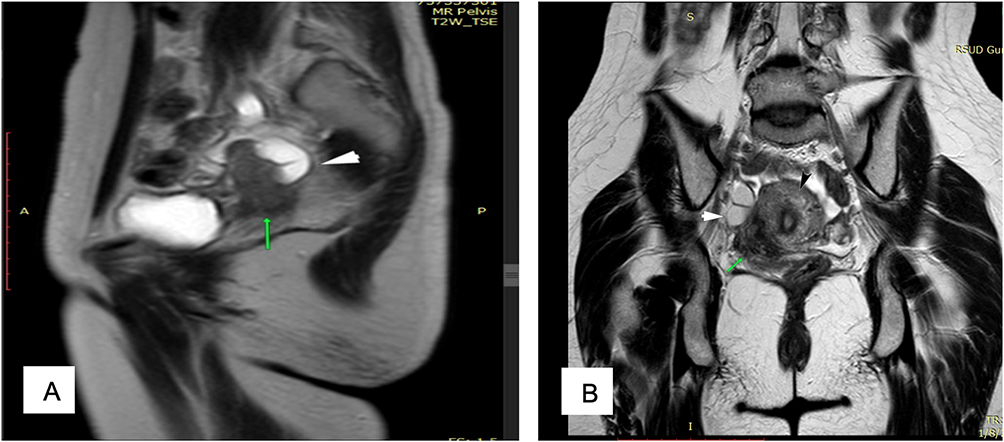 |
Figure 2 Magnetic resonance imaging (MRI) of the pelvis revealing right hydroureter and grade IV hydronephrosis, indicating severe dilation of the renal collecting system due to ureteral involvement by deep infiltrating endometriosis in the posterior pelvic compartment. A = anterior orientation marker; P = posterior orientation marker. (A) Green arrow: cervical mass extending to the right adnexa; White arrow: distal right hydroureter. (B) Black arrow: uterine fundus. Green arrow: deep infiltrating endometriosis nodule located adjacent to the right cervix. |
To evaluate renal function, a nuclear renogram was performed. The examination demonstrated markedly reduced tracer uptake and delayed excretion in the right kidney, consistent with severe obstructive uropathy and significantly impaired right renal function (Figure 3). These findings suggested substantial functional compromise secondary to longstanding ureteral obstruction. The residual renal function of the affected kidney was extremely limited, indicating advanced and likely irreversible renal damage caused by longstanding ureteral obstruction.
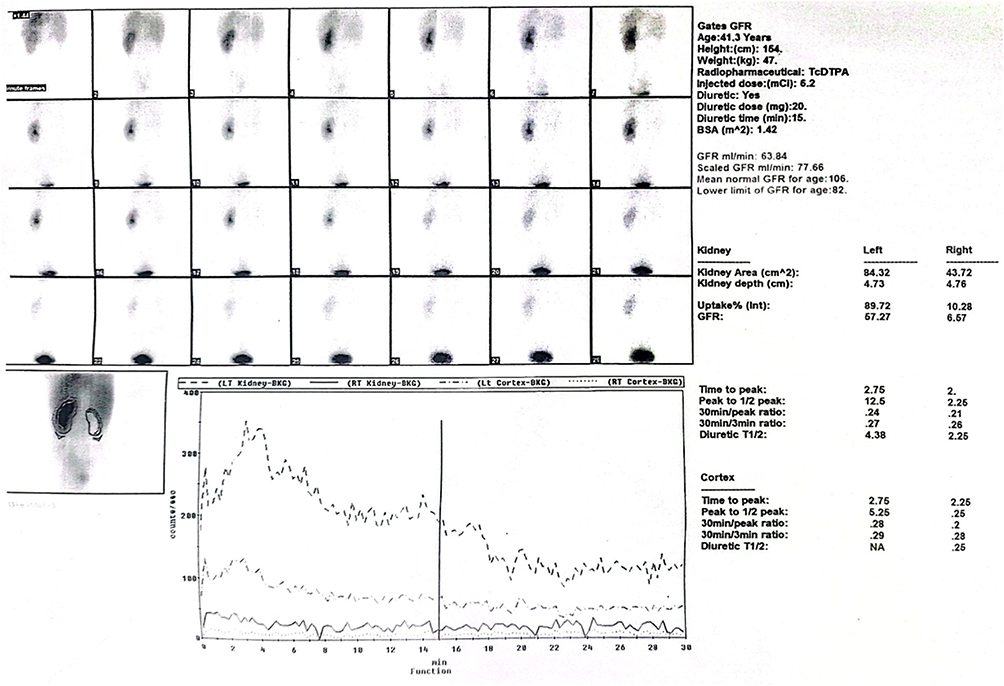 |
Figure 3 Nuclear renogram demonstrating severely impaired function of the right kidney with reduced tracer uptake and delayed excretion, consistent with obstructive uropathy secondary to ureteral involvement by deep infiltrating endometriosis. The numbered boxes (1–28) represent sequential dynamic scintigraphic images acquired over time during the renogram study, illustrating tracer uptake, transit, and excretion by both kidneys. The accompanying time–activity curves demonstrate markedly reduced tracer uptake and delayed washout in the right kidney compared with the left kidney. |
Based on the clinical presentation and imaging findings, a multidisciplinary management approach involving gynecology and urology was recommended. The proposed surgical intervention included complete resection of the endometriotic nodule combined with nephrectomy of the affected kidney, given the severity of hydronephrosis and the markedly diminished residual renal function demonstrated on nuclear renography. Ureteral reconstructive procedures such as ureteral reimplantation were considered unlikely to provide meaningful functional recovery because the kidney was considered functionally nonviable. However, after thorough counseling regarding the risks, benefits, and alternative treatment options, the patient declined surgical intervention and opted for conservative management, despite understanding the potential long-term consequences of untreated severe endometriosis with urological involvement.
The patient was subsequently treated with monthly leuprolide acetate injections for three consecutive months. Follow-up transrectal ultrasonography demonstrated partial reduction in the size of the deep infiltrating endometriosis nodule compared to baseline evaluation (Figure 4). Despite this interval decrease in lesion size and improvement in pain symptoms, right hydronephrosis persisted, indicating ongoing structural obstruction and the need for close surveillance of renal function. Long-term follow-up with periodic imaging and renal function monitoring was planned. The patient was also counseled that definitive surgical management, including nephrectomy and excision of the endometriotic lesion, would be reconsidered if lesion progression, worsening hydronephrosis, or further renal deterioration occurred during follow-up.
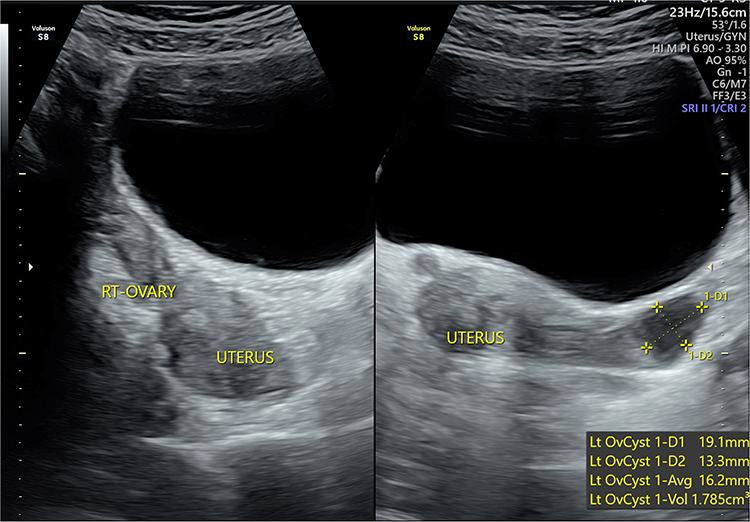 |
Figure 4 Follow-up transrectal ultrasonography after three months of hormonal therapy with leuprolide acetate, showing partial reduction in the size of the deep infiltrating endometriosis nodule compared to baseline evaluation. Persistent right hydronephrosis remains evident despite interval lesion shrinkage. |
Discussion
The present case describes a 41-year-old nulliparous woman with deep infiltrating endometriosis (DIE) involving the ureter, manifesting as a 2.65×1.56 cm nodule with associated hydroureter and grade IV hydronephrosis. This presentation aligns with prior reports of ureteral endometriosis where silent progression led to significant renal compromise before diagnosis.3 In a similar case, medical therapy with the GnRH agonist goserelin achieved complete resolution of ureteral dilation and hydronephrosis within three months, followed by maintenance with dienogest and levonorgestrel intrauterine system, preserving renal function and fertility potential.6 Unlike those reports where hydronephrosis fully reversed, our patient experienced only partial nodule reduction (to 1.91×1.33 cm) and pain improvement (VAS 9 to 5) after three monthly leuprolide acetate injections, likely reflecting the intrinsic fibrotic component of DIE adjacent to the ureter that may limit rapid lesion regression.7
This case highlights that ureteral endometriosis is a potentially serious condition which can lead to severe complications, particularly hydronephrosis, which may result in irreversible renal damage if not diagnosed and treated in a timely manner.3,7,8 Obstructive uropathy caused by ureteral involvement often progresses silently, and in many cases, renal impairment is detected only after significant functional loss has already occurred.9 Therefore, early diagnosis of ureteral endometriosis is crucial to prevent progressive and permanent renal damage.
The clinical manifestations of ureteral endometriosis are highly variable. Patients may present with cyclical flank pain associated with menstruation, chronic pelvic pain, dysuria, or nonspecific abdominal discomfort, while others may remain entirely asymptomatic despite advanced obstruction.3 As summarized in Table 1, previously reported cases of ureteral endometriosis demonstrate considerable variability in clinical presentation, treatment approach, duration of management, and patient outcomes. This variability underscores the importance of maintaining a high index of suspicion, particularly in women with known deep infiltrating endometriosis (DIE). In this context, renal ultrasonography should be considered as part of routine evaluation in selected patients with DIE, as it represents a simple, non-invasive, and accessible modality for early detection of silent hydronephrosis.7
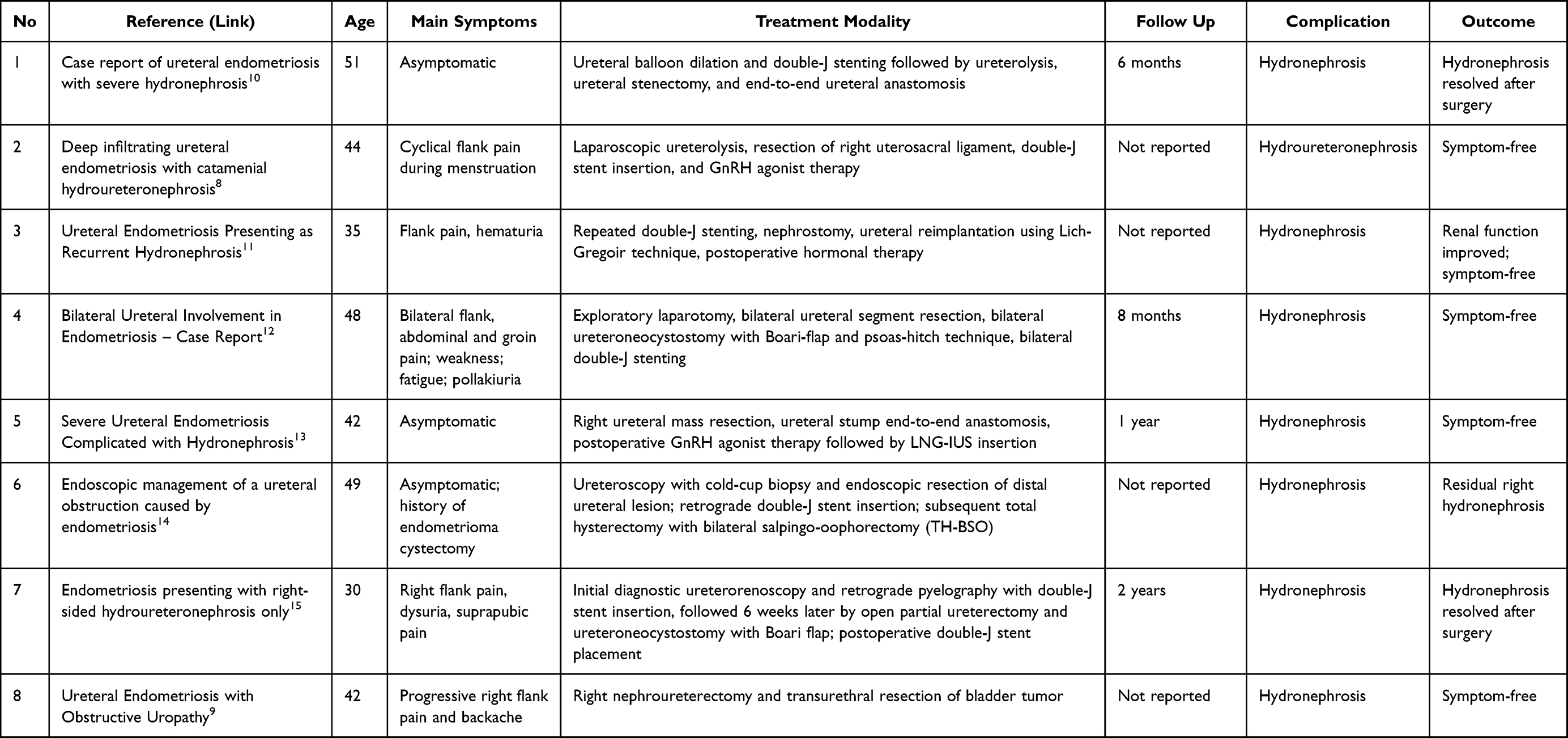 |
Table 1 Summary of Published Case Reports on Ureteral Endometriosis |
Refusal of surgical intervention in our patient echoes the choice of conservative management described in several case series. One report detailed intrinsic ureteral endometriosis managed with progestin therapy and ureteral stenting, resulting in symptomatic relief and stabilization of renal function over 24 months without surgery. The decision to postpone immediate surgery underscores the significance of patient autonomy and highlights the necessity of comprehensive, multidisciplinary counseling. Such counseling should carefully weigh the risk of progressive renal deterioration against the patient’s reproductive goals, as well as the potential adverse effects associated with long-term hormonal therapy. Patients should also be counseled regarding warning symptoms that warrant urgent reassessment, including worsening flank pain, fever, dysuria, gross hematuria, decreased urine output, or recurrent severe pelvic pain, as these may indicate progressive obstruction, urinary tract infection, or further renal compromise. The partial anatomical improvement suggests that leuprolide acetate, while effective in suppressing endometrial activity, may require longer duration or adjunctive treatments—such as add-back progestins or intrauterine systems—to achieve outcomes comparable to GnRH agonist protocols reported elsewhere.6
Comparative analysis of hormonal regimens for ureteral endometriosis reveals variable efficacy based on agent, duration, and lesion characteristics. While goserelin achieved complete anatomical resolution in moderate hydronephrosis, progestin monotherapy with dienogest has demonstrated durable symptom control and quality-of-life improvements in bowel and urinary DIE, despite residual imaging findings.3,6,16 Leuprolide acetate shares the mechanism of hypoestrogenism but may induce more profound hypoestrogenic symptoms, potentially limiting long-term adherence.7 In our patient, moderate lesion shrinkage and pain relief indicate that leuprolide acetate is a viable initial conservative strategy; however, literature suggests that combining GnRH agonist therapy with progestin add-back or switching to dienogest could enhance lesion regression and sustain symptom remission while mitigating hypoestrogenic sequelae.16
The pathophysiology of ureteral DIE involves both intrinsic invasion of ureteral muscularis and extrinsic compression from adjacent parametrial lesions.7 Surgical ureterolysis with or without segmental resection remains the definitive treatment to restore ureteral patency, as demonstrated in cases where medical therapy alone failed to reverse obstruction or preserve renal function over long-term follow-up.15 Our patient’s ongoing monitoring is crucial given her grade IV hydronephrosis and only partial response to leuprolide acetate. The literature supports that early surgical intervention, particularly when hydronephrosis is advanced, may prevent irreversible renal damage despite patient preference for conservative management. Thus, close imaging surveillance and shared decision-making are imperative to balance the benefits and limitations of hormonal therapy against the potential need for elective surgery should lesion progression or renal impairment recur.7,17 During follow-up, periodic imaging evaluation and renal function assessment remain essential to detect disease progression at an early stage and to reassess the indication for definitive surgical management if conservative therapy fails.
Conclusion
Ureteral endometriosis is a potentially serious condition that may lead to hydronephrosis and irreversible renal damage if not diagnosed early. Because clinical manifestations can be variable or even asymptomatic, early detection through appropriate imaging, including renal ultrasonography, is essential. Conservative hormonal therapy with GnRH agonists may reduce nodule size and relieve symptoms in patients who decline surgery; however, persistent hydronephrosis indicates ongoing risk to renal function. Therefore, while hormonal therapy can serve as a temporary strategy, definitive surgical management remains crucial to prevent permanent ureteral obstruction and preserve long-term renal function.
Institutional Approval
Institutional approval was not required for the publication of this single-patient case report, in accordance with institutional policies and the ethical standards of the Declaration of Helsinki.
Informed Consent Patient Statement
The authors confirm that written informed consent was obtained from the patient. The patient was informed about the details of the case and provided approval for the publication of the case report, including any accompanying images. All identifying information has been appropriately anonymized to ensure patient confidentiality.
Acknowledgment
This publication charge is funded by Unpad through the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology and managed under the EQUITY Program (Contract No. 4303/B3/DT.03.08/2025 and 3927/UN6. RKT/HK.07.00/2025).
Disclosure
The authors declare that they have no competing interests for this work.
References
1. Sarria-Santamera A, Orazumbekova B, Terzic M, Issanov A, Chaowen C, Asúnsolo-del-Barco A, editors. Systematic review and meta-analysis of incidence and prevalence of endometriosis. In: Healthcare. MDPI; 2020.
2. von Theobald P, Cottenet J, Iacobelli S, Quantin C. Epidemiology of endometriosis in France: a large, nation‐wide study based on hospital discharge data. Biomed Res Int. 2016;2016(1):3260952. doi:10.1155/2016/3260952
3. Palla -V-V, Karaolanis G, Katafigiotis I, Anastasiou I. Ureteral endometriosis: a systematic literature review. Indian J Urol. 2017;33(4):276–8. doi:10.4103/iju.IJU_84_17
4. Durant Des Aulnois C, Razakamanantsoa L, Crestani A, et al. Urinary tract endometriosis: revisiting the definition of ureterolysis. Int J Gynecol Obstet. 2026;172(1):279–294. doi:10.1002/ijgo.70290
5. Barra F, Scala C, Biscaldi E, et al. Ureteral endometriosis: a systematic review of epidemiology, pathogenesis, diagnosis, treatment, risk of malignant transformation and fertility. Human Reprod Update. 2018;24(6):710–730. doi:10.1093/humupd/dmy027
6. Nguyen T, Nguyen M, Hoang T. Reversal of endometriosis-induced unilateral ureteral obstruction and hydronephrosis with medical therapy. Cureus. 2024;16(11):e73983–e. doi:10.7759/cureus.73983
7. Kızılay F, Şimşir A, Nazlı O. Management of ureteral endometriosis and review of the literature. Turk J Urol. 2018;45(Suppl 1):S166. doi:10.5152/tud.2018.21605
8. Lee HJ, Lee YS. Deep infiltrating ureteral endometriosis with catamenial hydroureteronephrosis: a case report. J Med Case Rep. 2017;11(1):346. doi:10.1186/s13256-017-1518-6
9. Hsieh M-F, Wu IW, Tsai C-J, Huang -S-S, Chang L-C, Wu M-S. Ureteral endometriosis with obstructive uropathy. Internal Med. 2010;49(6):573–576. doi:10.2169/internalmedicine.49.2797
10. Li J, Bai J, Wang H, Chen B. A case report of ureteral endometriosis with severe hydronephrosis. Urol Case Rep. 2024;56:102815. doi:10.1016/j.eucr.2024.102815
11. Al Ayoubi O, Aldakak MA, Tannous G, Mhimid A, Awad MA, Alia L. Ureteral Endometriosis Presenting as Recurrent Hydronephrosis: a Case Report. Res Rep Urol. 2025;17:421–426. doi:10.2147/RRU.S554886
12. Köse M. Bilateral Ureteral Involvement in Endometriosis-Case Report. Int J Current Med Biol Sci. 2023;3(3):142–146.
13. Bai Y, Li Y, Li Q, Zhao W. Severe ureteral endometriosis complicated with hydronephrosis: a case report. Am J Case Rep. 2022;23:e937172–1. doi:10.12659/AJCR.937172
14. Juan HC, Yeh HC, Hsiao HL, Yang SF, Wu WJ. Endoscopic management of a ureteral obstruction caused by endometriosis: a case report. Kaohsiung J Med Sci. 2009;25(4):217–221. doi:10.1016/S1607-551X(09)70064-6
15. Karadag MA, Aydin T, Idem Karadag O, et al. Endometriosis presenting with right side hydroureteronephrosis only: a case report. J Med Case Rep. 2014;8(1):420. doi:10.1186/1752-1947-8-420
16. Alenezi S, Zaheer M, Khudair S. Intrinsic unilateral ureteral endometriosis: a rare case report. Int J Surg Case Rep. 2023;104:107966. doi:10.1016/j.ijscr.2023.107966
17. Lu Y, Wang Y. Ureteral endometriosis post-hysterectomy for adenomyosis: a case report and literature review. BMC Urol. 2025;25(1):164. doi:10.1186/s12894-025-01866-9
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.