Back to Journals » Clinical Ophthalmology » Volume 20
Short-Term Preliminary Results of Outcomes with and without Tenonectomy During Open Conjunctival XEN45 Gel Stent Implantation
Authors Applebaum SS ![]() , Hundito A, Ajjawi I, Teng CC, Sarrafpour S, Liu J
, Hundito A, Ajjawi I, Teng CC, Sarrafpour S, Liu J ![]()
Received 16 July 2025
Accepted for publication 25 September 2025
Published 24 June 2026 Volume 2026:20 554193
DOI https://doi.org/10.2147/OPTH.S554193
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Serina S Applebaum,1 Addiskidan Hundito,1 Ismail Ajjawi,1 Christopher C Teng,2 Soshian Sarrafpour,3 Ji Liu3
1Yale School of Medicine, New Haven, CT, USA; 2Department of Ophthalmology and Visual Sciences, University of Massachusetts Medical School, Worcester, MA, USA; 3Department of Ophthalmology and Visual Science, Yale School of Medicine, New Haven, CT, USA
Correspondence: Ji Liu, Department of Ophthalmology and Visual Science, Yale School of Medicine, 40 Temple Street, Suite 3B, New Haven, CT, 06510, USA, Tel +1 877 925 3637, Email [email protected]
Purpose: To compare outcomes of eyes with and without tenonectomy during ab externo open conjunctival (AEO) implantation of a gelatin stent (XEN45 Gel Stent [XGS]) with mitomycin C.
Methods: We conducted a retrospective comparative cohort study of adults aged ≥ 40 with open-angle glaucoma and preoperative intraocular pressure (IOP) > 17mmHg who underwent XGS AEO with or without tenonectomy at a single academic center (April 2021-September 2023). We matched eyes undergoing tenonectomy 1:3 to controls using nearest-neighbor algorithm. The primary outcome was success at 1 year (6 ≤ IOP ≤ 21mmHg, with ≥ 20% reduction from baseline, with or without IOP-lowering medication). Secondary outcomes included IOP, medication burden, visual acuity, and postoperative complications and interventions.
Results: We included 40 eyes (38 patients): 10 with tenonectomy and 30 without. At 1 year, 70%, 60%, and 40% of tenonectomy eyes and 55%, 52%, and 36% of non-tenonectomy eyes achieved success at IOP thresholds of 21, 18, and 15 mmHg, respectively (all p> 0.05). There were no significant differences between groups in IOP, medication burden, or visual acuity. At 1 year, mean IOP was 14.83 ± 2.08 on 1.13 ± 0.38 IOP-lowering medications in the tenonectomy group and 16.88 ± 1.53 on 1.36 ± 0.31 medications in the non-tenonectomy group. Tenonectomy eyes tended toward more early complications (30% vs 23%, p=0.69), but fewer postoperative interventions (30% vs 57%, p=0.28) and reoperations (20% vs 30%, p=0.70).
Conclusion: Both techniques provided effective IOP control and reduced medication burden. In this short-term preliminary study, tenonectomy may be more effective than the traditional technique. Given the small sample size and retrospective design, findings should be interpreted cautiously. More data are needed to guide optimal surgical technique.
Keywords: open-angle glaucoma, glaucoma surgery, XEN gel stent, tenonectomy, surgical outcomes
Introduction
Postoperative fibrosis and scarring can compromise the success of filtration procedures in the treatment of glaucoma. Tenon’s capsule has been identified as a key source of fibroblasts and a main site of failure for glaucoma surgery. Fibrotic encapsulation of the filtering bleb after glaucoma surgery, known as Tenon’s cyst, can impair bleb function and limit long-term intraocular pressure (IOP) control.1 Tenonectomy, the surgical removal of Tenon’s capsule, has been proposed as a strategy to reduce fibroblast proliferation and mitigate postoperative scarring and surgical failure.2,3 This approach may particularly benefit patients who are at high risk for fibrosis, such as younger individuals, those with thicker Tenon’s capsule, and those with prior conjunctival or glaucoma surgeries in whom Tenon’s scarring may have contributed to surgical failure.1,3,4
Evidence from prior studies suggests a potential role for tenonectomy in improving surgical outcomes. In a study by Abu et al of Indian patients undergoing trabeculectomy, the addition of tenonectomy resulted in significantly greater IOP reduction compared to trabeculectomy alone5 Pediatric eyes, which exhibit rapid and robust healing, are prone to fibrosis and often involve a thicker Tenon’s capsule.4,6,7 A randomized controlled trial of pediatric trabeculectomy found that eyes undergoing tenonectomy had consistently lower postoperative IOP and required fewer medications.6 These findings support the exploration of tenonectomy in filtration-based procedures beyond trabeculectomy.
The role of tenonectomy is poorly understood in modern microinvasive glaucoma surgery (MIGS) or MIGS-plus, like the XEN45 Gel Stent (Allergan PLC, Irvine, CA, USA). The XEN45 Gel Stent (XGS) lowers IOP by creating a subconjunctival filtration bleb, and its long-term function depends on bleb morphology and resistance to scarring.8–10 Notably, the ab externo approach to implantation, which involves direct conjunctival and Tenon’s dissection, is associated with more diffuse, posteriorly directed blebs which tend to be less prone to postoperative fibrosis and scarring than ab interno implantation, which results in flatter, thinner, and more avascular blebs.11,12 Tenon’s capsule can contribute to fibrotic bleb encapsulation and to distal occlusion of the stent. Thus, removing Tenon’s tissue during ab externo placement could, in theory, improve bleb architecture and long-term patency. In contrast, by increasing tissue manipulation, tenonectomy may predispose patients to higher rates of early bleeding-related complications. Surgeons therefore face a clinical dilemma of balancing potentially higher early complication risks of tenonectomy against theoretical long-term benefits in fibrosis-prone patients. Existing studies have shown conflicting results regarding the utility of tenonectomy, with some demonstrating improved outcomes,5,13 and others showing no significant benefit.14,15 In this study, we aim to evaluate the effectiveness and safety of tenonectomy performed during ab externo open conjunctiva (AEO) XGS implantation using a matched cohort design.
Material and Methods
Study Cohort
This study was approved by the Yale Institutional Review Board (#2000032431) and adheres to the tenets of the declaration of Helsinki. The Yale Institutional Review Board waived the requirement of patient consent to review medical records due to the retrospective nature of the review. All data was anonymized and maintained confidentially. We conducted a retrospective review of the medical records of patients aged ≥40 who underwent XGS AEO implantation with mitomycin-C (MMC) at our institution from April 2021 to September 2023. We excluded eyes with preoperative IOP ≤17 mmHg, closed-angle glaucoma, proliferative diabetic retinopathy, exudative age-related macular degeneration, or a history of prior XEN surgery. The initial considered cohort consisted of 83 eyes (10 with tenonectomy and 73 without). We matched eyes that underwent XGS AEO with tenonectomy to controls without tenonectomy using a nearest neighbor algorithm in a 1:3 ratio based on age, sex, race, preoperative IOP, and glaucoma severity using the R package MatchIt. The final matched cohort included 40 eyes from 38 patients, including 10 eyes with tenonectomy and 30 without.
Data Collection and Definitions
We recorded demographic and preoperative data from manual review of the electronic medical record, including age, sex, race and ethnicity, smoking status, hypertension, diabetes, and use of antiplatelet or anticoagulant medications. We recorded ocular characteristics including glaucoma type and severity, lens status (phakic or pseudophakic), prior glaucoma surgeries or laser procedures, and baseline preoperative IOP, number of IOP-lowering medications, and best-corrected visual acuity (BCVA). Glaucoma severity was determined by ICD-10 code and visual field criteria. We converted Snellen visual acuity measurements to logarithm of minimum angle of resolution (LogMAR) values for analysis.
We defined the primary outcome as surgical success over a one-year follow-up period. Surgical success required IOP ≥6 mmHg under three different upper limit thresholds (≤21 mmHg, ≤18 mmHg, ≤15 mmHg) and IOP reduction ≥20% from baseline. We defined qualified success as maintaining this IOP range with the use of IOP-lowering medications, and complete success without IOP-lowering medications. We considered eyes that failed to meet these criteria at two consecutive time points to be a surgical failure. We censored patients who were lost to follow-up and had not failed the success criteria after their last follow-up office visit.
We assessed secondary outcomes including change in IOP, medication use, and visual acuity over time, as well as the occurrence of postoperative complications, interventions, and reoperations. We categorized complications as early (within 3 months) or late (after 3 months). We collected postoperative data at postoperative day 1 (day 1–3), week 1 (day 4–14), month 1 (day 15–60), month 3 (day 61–122), month 6 (day123-122), and month 12 (day 273–456) and calculated the average IOP value when multiple visits fell within the eligible follow-up window, per the World Glaucoma Association’s Guidelines on Design and Reporting of Glaucoma Surgical Trials.16
Surgical Technique
All procedures were performed or supervised by one of three fellowship-trained glaucoma surgeons using an ab externo open conjunctiva approach. A traction suture was placed through the superior limbus. Subconjunctival 2% lidocaine with 1:100,000 epinephrine was injected into the superior subconjunctival space to achieve anesthesia and hemostasis. A superior peritomy was created and the subconjunctival area was dissected posteriorly. Mitomycin-C, 0.2mg/mL via injection or sponge, was applied to the subconjunctival space based on manufacture’s recommendation, followed by copious irrigation. The XEN injector needle was entered to the sclera 2mm superior to the limbus, and advanced towards the limbus through a scleral tunnel and deployed into the anterior chamber (AC). The position of the stent was adjusted with forceps, with 1mm in the AC and 3mm in the subconjunctival space. In eyes with prior glaucoma surgery, the stent was preferentially placed at least one clock hour away from prior surgical sites to minimize scarring risk and improve filtration. Here, a tenonectomy of approximately 3mm by 4mm was created at the surgeon’s discretion. The conjunctiva was then reapproximated to the limbus using interrupted 10–0 nylon or vicryl limbal anchoring sutures. The subconjunctival portion of the stent was confirmed as straight, perpendicular to the limbus, and not tangled with Tenon’s capsule after conjunctival closure.
Postoperatively, all topical IOP-lowering agents were discontinued on the day of surgery. A topical antibiotic and topical 1% prednisolone acetate or difluprednate 4 times per day were initiated for the first week, and subsequently tapered at surgeon’s discretion. Medical management was titrated over time determined by clinical assessment of the postoperative eye.
Statistical Analysis
We compared baseline differences in demographic and preoperative characteristics between groups using Wilcoxon rank sum tests for continuous variables and Fisher’s exact tests for categorical variables. We performed Kaplan-Meier survival analysis with Log rank tests, adjusting for bilateral cases in the same patient, to evaluate the primary outcome of surgical success over a one-year follow-up period. We analyzed secondary outcomes using linear mixed-effects models to assess changes in IOP, medication use, and visual acuity over time, with the random subject effect accounting for correlation among multiple observations on the same patient. We compared rates of postoperative complications, interventions, and reoperations between groups using Fisher’s exact test. We used RStudio (Version 2024.04.2) for all statistical analyses, and set the significance level at p<0.05.
Results
Baseline Characteristics
A total of 40 eyes of 38 patients were included in the study, with 10 eyes undergoing XGS AEO with tenonectomy and 30 eyes without tenonectomy. Baseline characteristics were similar between the two groups. The majority of patients were male in both the tenonectomy and non-tenonectomy groups (73% and 80%, respectively). The median age was 72 years (interquartile range [IQR], 65–79). Most eyes (78%) had severe glaucoma, and most eyes (80%) had primary open-angle glaucoma. Other glaucoma types included 5 cases of pseudoexfoliative glaucoma, 1 case of pigmentary glaucoma, 1 case of traumatic glaucoma, and 1 case of low-tension glaucoma. The median preoperative IOP was 22.0 (IQR, 20.0–25.0) mmHg in the tenonectomy group and 22.0 (IQR, 19.0–24.8) mmHg in the non-tenonectomy group. A higher proportion of eyes in the tenonectomy group had prior glaucoma surgery (50% vs. 30%; p=0.28). Mean recorded follow-up duration was 9.7 months, with 7 individuals, all in the non-tenonectomy group, lost to follow-up after the 6-month postoperative visit. There were no significant differences in demographic variables, including age, sex, and race, glaucoma severity, lens status, diabetes status, or prior glaucoma surgeries between groups (Table 1).
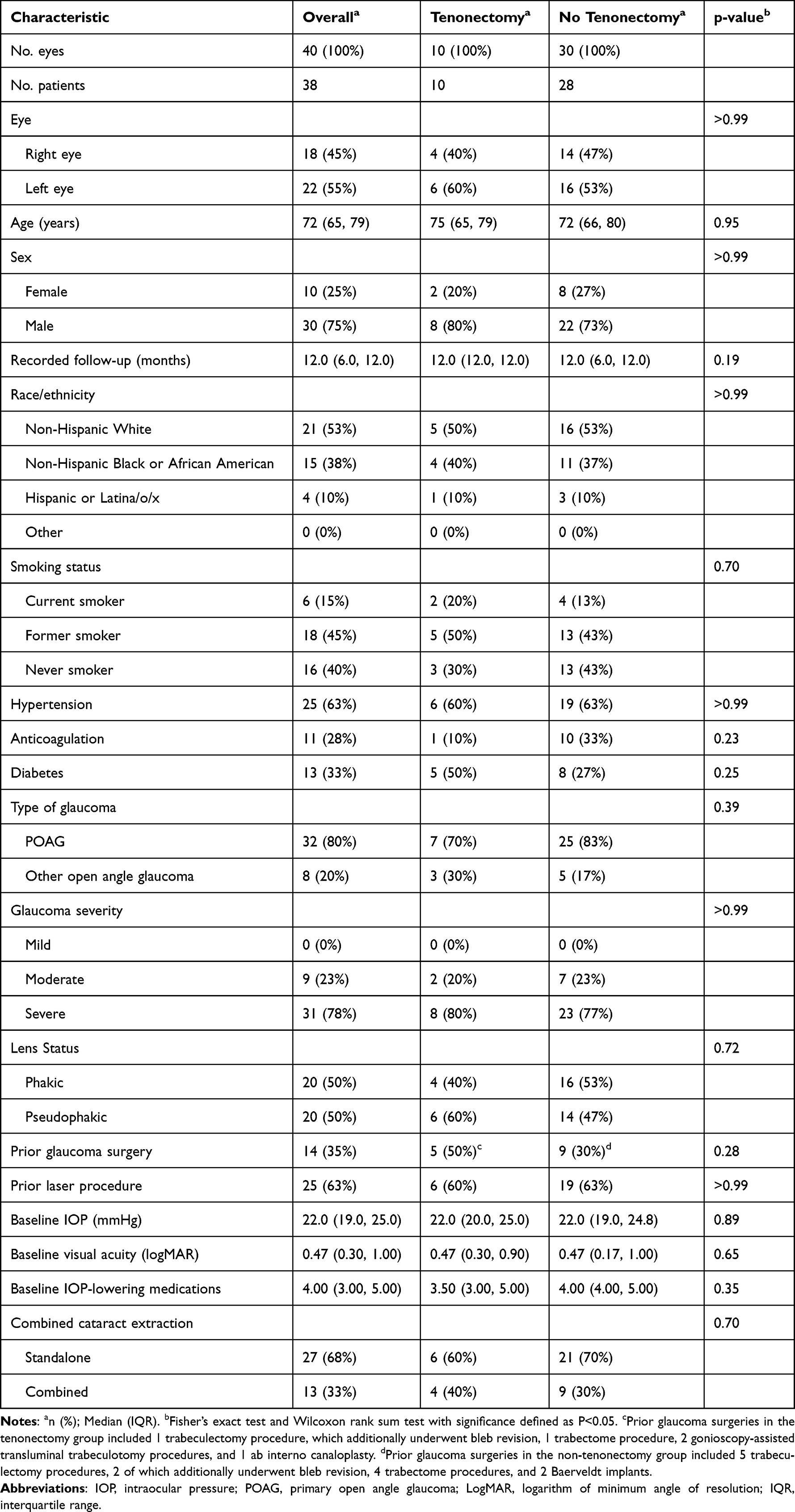 |
Table 1 Demographics and Baseline Characteristics of 40 Eyes That Underwent Ab Externo Open Conjunctival XEN45 Gel Stent Implantation |
Primary and Secondary Outcomes
At postoperative month 12, we assessed success rates using IOP upper thresholds of ≤21 mmHg, ≤18 mmHg, and ≤15 mmHg. At ≤21 mmHg, the cumulative probability of survival was 70% in the tenonectomy group and 55% in the non-tenonectomy group under qualified success criteria (p=0.43), and 40% and 37%, respectively, under complete success criteria (p=0.65). At ≤18 mmHg, the cumulative probability of survival was 60% and 52%, respectively, under qualified success criteria (p=0.58) and 40% and 38% under complete success criteria (p=0.72). At ≤15 mmHg, survival probability was 40% and 36%, respectively, for qualified success (p=0.91), and 30% and 27% for complete success (p=0.98). While the tenonectomy group had higher success rates across all thresholds, the differences were not statistically significant (Figure 1).
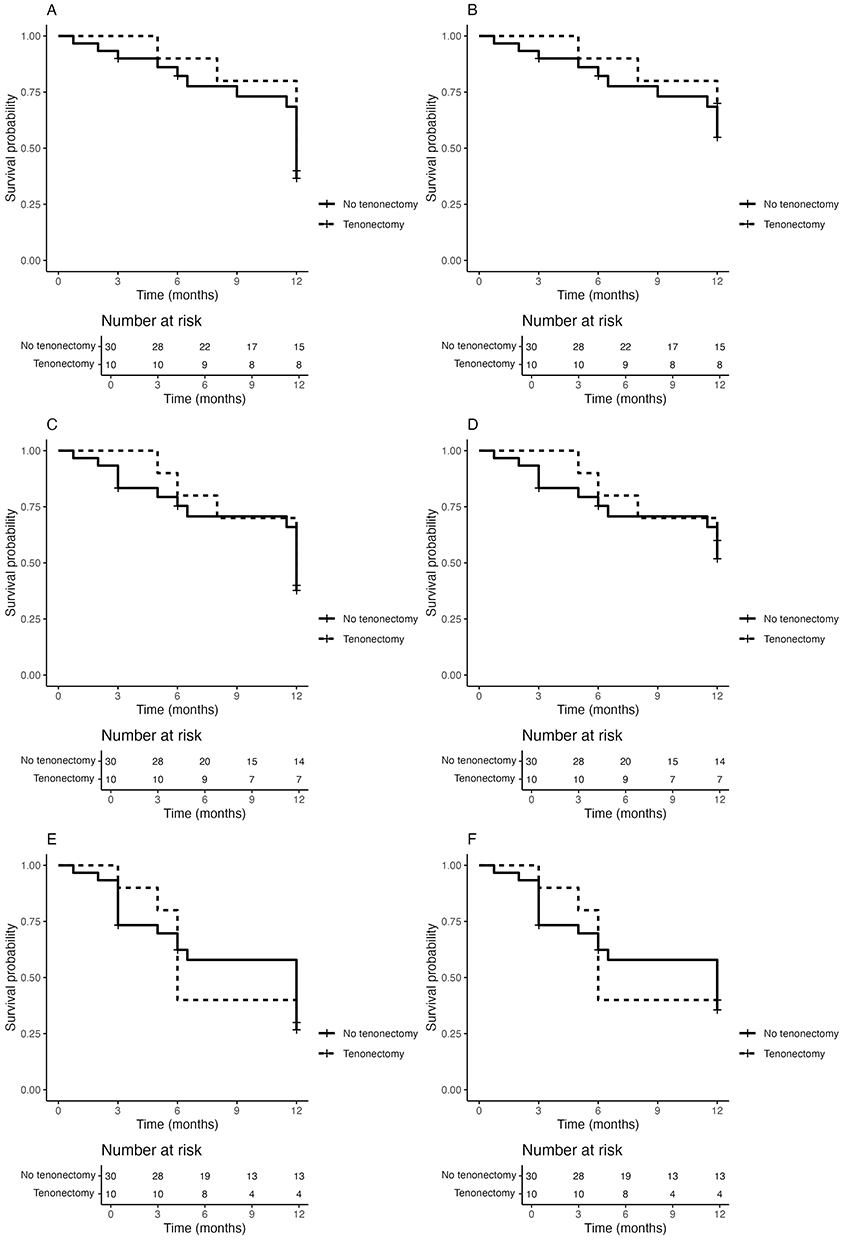 |
Figure 1 Kaplan-Meier plots of the probability of complete and qualified success under the definition of (A) complete success with 6 mmHg ≤ IOP ≤ 21 mmHg, (B) qualified success with 6 mmHg ≤ IOP ≤ 21 mmHg, (C) complete success with 6 mmHg ≤ IOP ≤ 18 mmHg, (D) qualified success with 6 mmHg ≤ IOP ≤ 18 mmHg, (E) complete success with 6 mmHg ≤ IOP ≤ 15 mmHg, (F) qualified success with 6 mmHg ≤ IOP ≤ 15 mmHg. IOP = intraocular pressure. |
In terms of secondary outcomes, both groups demonstrated significant reductions in IOP from baseline at all postoperative time points. At postoperative month 6, mean IOP was reduced to 16.96 ± 2.08 mmHg in the tenonectomy group and 18.07 ± 1.19 mmHg in the non-tenonectomy group (p=0.64). At postoperative month 12, mean IOP was 14.83 ± 2.08 mmHg in the tenonectomy group and 16.88 ± 1.53 mmHg in the non-tenonectomy group (p=0.43). IOP-lowering medication burden also decreased significantly in both groups to 1.13 ± 0.38 agents in the tenonectomy group and 1.36 ± 0.31 agents in the non-tenonectomy group at postoperative month 12 (p=0.64). Best-corrected visual acuity remained stable over the follow-up period, with no significant differences between groups at any time point (Figure 2).
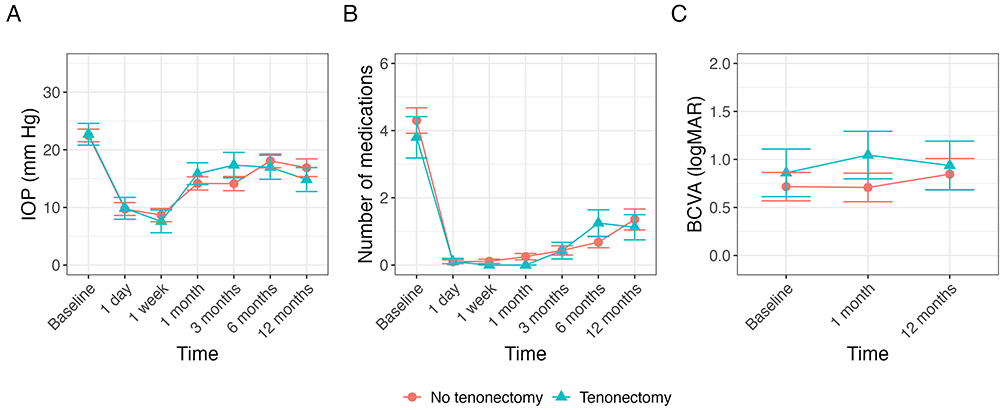 |
Figure 2 Plots depicting (A) linear mixed effects model of IOP, (B) linear mixed model of the number of active compounds of IOP-lowering medications, (C) linear mixed effects model of BCVA for patients with open conjunctival ab externo XEN45 Gel Stent implantation that underwent tenonectomy (blue triangle) or did not (Orange circle). Data are presented as estimated marginal means ± standard error. |
Complications
Early complications, defined as events occurring within three months postoperatively, occurred in 30% of eyes in the tenonectomy group compared to 23% in the non-tenonectomy group (p=0.69). Choroidal effusion with or without accompanying shallow anterior chamber occurred in 20% of eyes with tenonectomy and 10% of eyes without. Hyphema (20% vs. 3.3%) and vitreous hemorrhage (10% vs. 0%) were more frequent in the tenonectomy group. Late complications were rare, with one case of endophthalmitis (3.3%) reported in the non-tenonectomy group (Table 2).
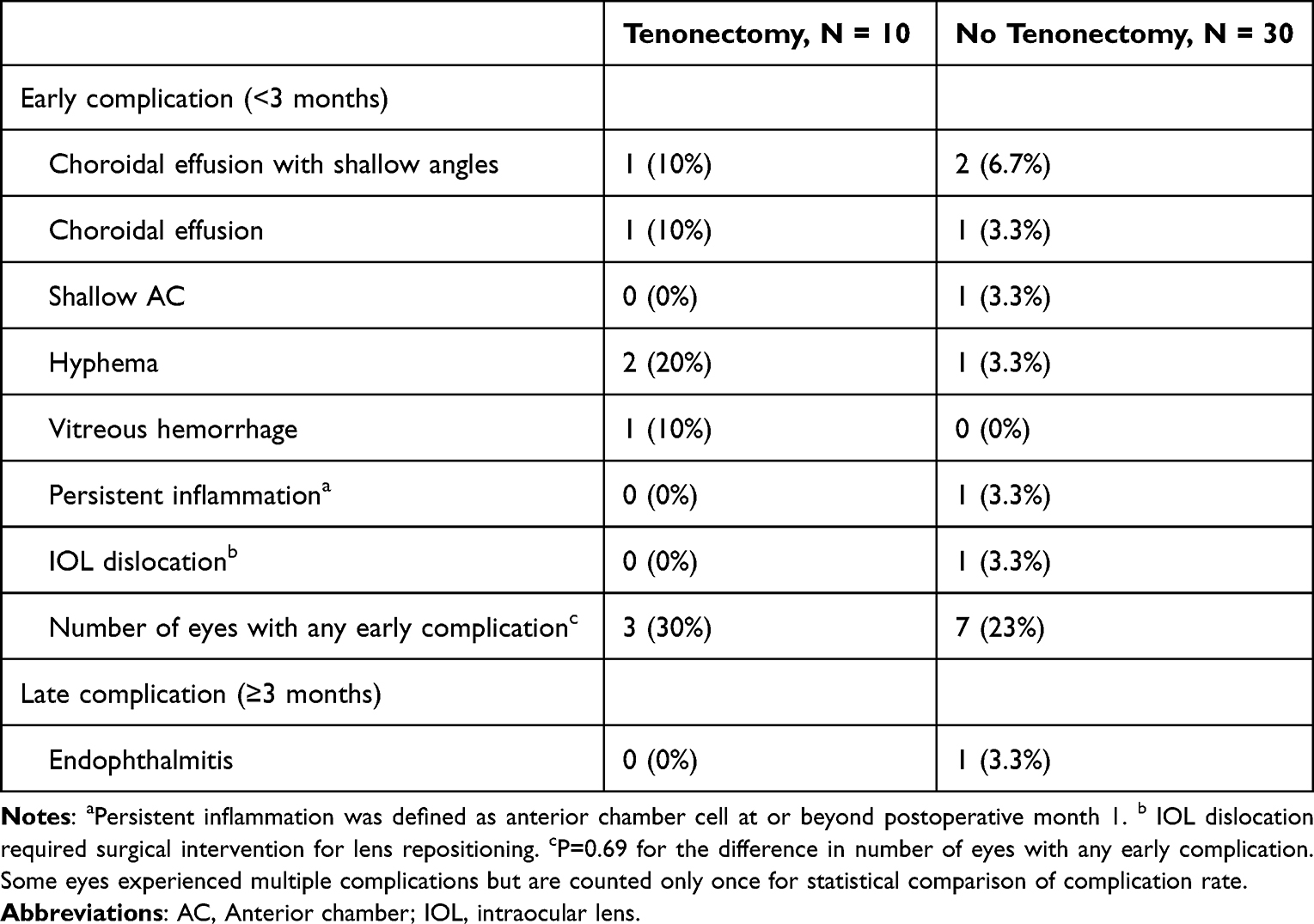 |
Table 2 Complications Following Ab Externo Open Conjunctival XEN45 Gel Stent Implantation with or Without Tenonectomy |
Interventions and Reoperations
The proportion of eyes requiring any postoperative intervention was higher in the non-tenonectomy group (53%) compared to the tenonectomy group (30%), though this difference was not statistically significant (p=0.28). The rate of needling was similar (30% in the tenonectomy group vs. 27% in the non-tenonectomy group). Other interventions, including anterior chamber reformation (10%), paracentesis (6.7%), and selective laser trabeculoplasty (3.3%), were used only in the non-tenonectomy group. Reoperation rates were non-significantly lower in the tenonectomy group (20%) compared to the non-tenonectomy group (30%; p=0.70). Of the two reoperations in the tenonectomy group, one underwent trabeculectomy and one underwent gonioscopy-assisted transluminal trabeculotomy (Table 3).
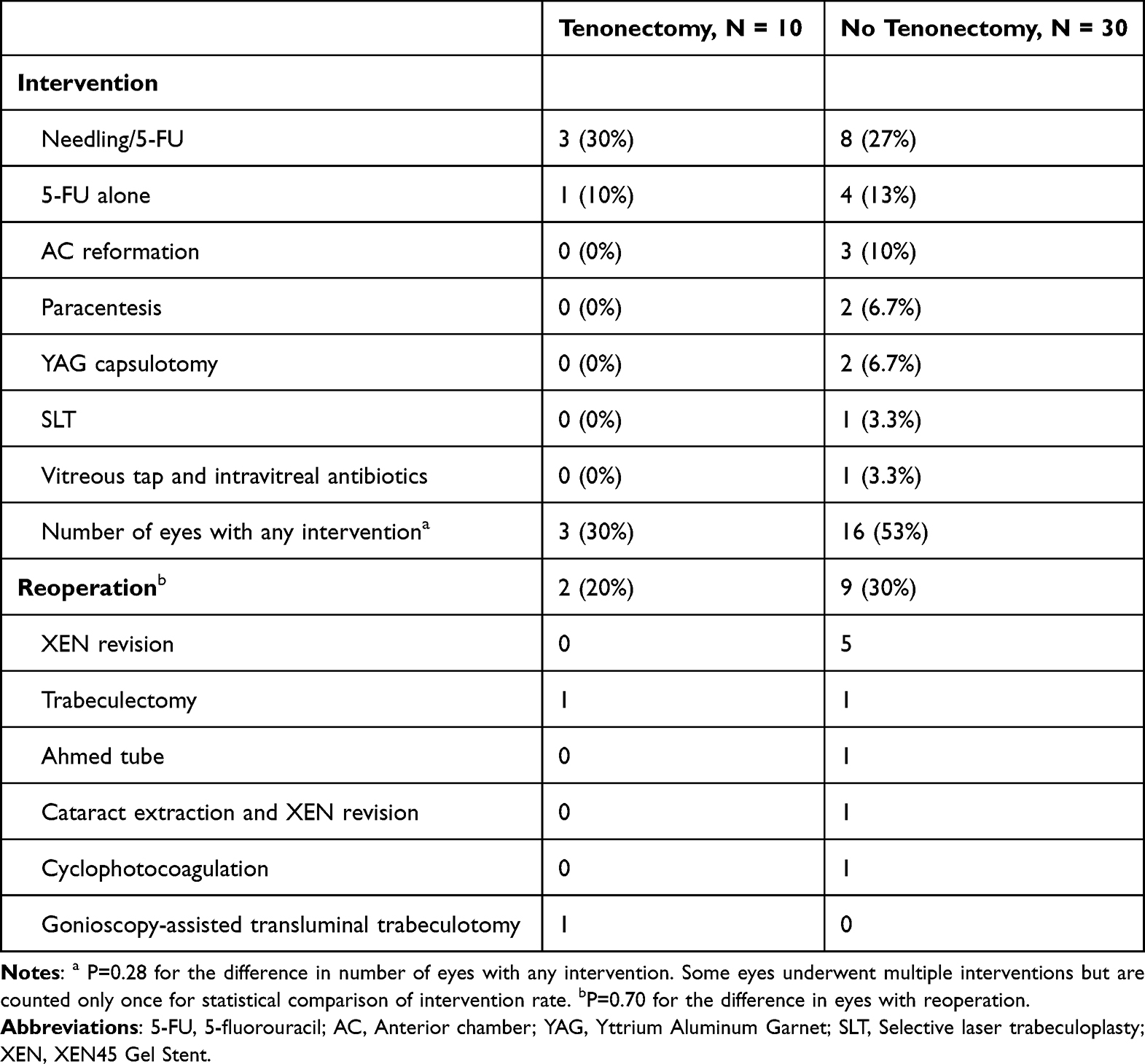 |
Table 3 Postoperative Interventions and Reoperations Following Ab Externo Open Conjunctival XEN45 Gel Stent Implantation with or Without Tenonectomy |
Discussion
Our study retrospectively compares eyes undergoing XGS AEO which received tenonectomy to those that did not. Tenonectomy has been studied in the past in various glaucoma surgeries, but there have been conflicting results regarding its benefits. While the XGS AEO has gained popularity in recent years, few studies have evaluated the addition of tenonectomy to this procedure. In this single-center cohort, both techniques significantly lowered IOP and reduced medication burden. Although between group differences were not statistically significant, the tenonectomy group trended towards higher success rates and fewer interventions and reoperations, but slightly more complications.
At one year, eyes undergoing tenonectomy consistently demonstrated higher survival probabilities, although these differences were not statistically significant (70% vs. 55% at ≤21 mmHg; 60% vs. 52% at ≤18 mmHg; 40% vs. 36% at ≤15 mmHg under qualified success criteria). Lack of statistical significance likely reflects limited power due to our small sample size rather than true equivalence in this setting. This may support the theoretical advantage of reduced postoperative scarring and therefore lower failure risk after tenonectomy. A retrospective study by El Helwe et al, which used a 2–3mm perilimbal tenonectomy as part of their standard XGS AEO technique, reported qualified and complete success rates of 62% and 29%, respectively, for maintaining IOP ≤18mmHg at 1 year, which was significantly higher than the success in the ab externo closed conjunctiva (AEC) comparison group17 The success rates in our study were similar. Of note, El Helwe et al compared an AEO technique with tenonectomy to AEC, which differ on multiple fronts including conjunctival dissection which may decrease outflow resistance and improve bleb morphology, whereas our study isolated use of tenonectomy in the AEO technique17,18 An additional plausible explanation for the lack of significant difference in our groups is that the narrow lumen of the XGS device may be the limiting factor for aqueous outflow, which could supersede any effect of tenonectomy in long-term IOP reduction. Even so, we suggest that tenonectomy may still be considered especially in cases of significant Tenon’s thickening or where scarring risk is elevated, without compromising the overall success of XGS AEO implantation.
The success rates in our XGS AEO cohort are similar to those reported in other studies evaluating the XEN stent, which range from 48.6% to 83%, compared to 55–70% in our study.8,9,17,19–22 One previous retrospective analysis of 44 eyes undergoing XGS AEO with tenonectomy reported a somewhat lower success rate of 43%.23 This discrepancy may be due to differences in the patient population for that study, which did not exclude patients with previous XEN surgery nor advanced comorbid eye disease that could have impacted the success rates. In contrast, a small retrospective case series of six eyes with refractory glaucoma treated with XGS AEO and tenonectomy reported a 100% success rate, with no complications or changes in visual acuity after a one-year follow-up.13 Unlike these prior studies, which only evaluated eyes undergoing XGS AEO with tenonectomy without a comparison group, we conducted a direct comparison to similar eyes without tenonectomy. While evidence supporting the use of tenonectomy in adult patients with glaucoma is limited, these findings suggest that tenonectomy may indeed be a suitable option for those at elevated risk of fibrosis. Future investigation with larger, prospective randomized trials is warranted to validate its role and refine patient selection criteria.
Most complications in our study were minor, and most cases had no severe adverse events. Eyes in the tenectomy group trended towards a slightly higher rate of early postoperative complications (30% vs. 23%). This may be attributable to the more invasive nature of the procedure. The higher incidence of bleeding-related complications such as hyphema (20%) and vitreous hemorrhage (10%) may result from the disruption of normal vascularized tissue barriers and exposure blood vessels following removing Tenon’s capsule, increasing the risk of intraoperative and postoperative bleeding. Additionally, as Tenon’s capsule contributes to normal wound healing, tenonectomy may interfere with tissue healing making and increase susceptibility to hemorrhage.2–4 Only one individual in the tenonectomy group was on anticoagulant therapy; this eye did not experience any early complications. Even so, because of this potential risk, additional caution may be taken when considering tenonectomy among patients using anticoagulants to reduce the risk of hemorrhagic events. Of note, despite the more extensive dissection involved in tenonectomy, no cases of XGS implant exposure occurred in either group. One theoretical concern with tenonectomy is that reduced tissue coverage may increase the risk of implant exposure. The absence of such cases in our study could reflect limited sample size, but it may also be that the small, gelatinous, flexible nature of the XGS make it resistant to erosion and exposure, even in the setting of reduced overlying tissue. This observation may further support the safety profile of the tenonectomy during AEO XGS implantation.
Eyes undergoing tenonectomy required non-significantly fewer postoperative interventions than those without tenonectomy. Tenonectomy may promote a more stable early postoperative bleb environment, reducing the need for additional management. However, tenonectomy did not reduce the rate of postoperative bleb needling in our study (30% vs. 27%). Needling revision is typically required to address fibrotic tissue or insufficient flow in the bleb, and it has been hypothesized that tenonectomy may reduce to reduce the need for such interventions by removing Tenon’s capsule, a major contributor to fibrosis.3,24,25 Reported rates of needling after XEN stent implantation range from 28.4% to 42% compared to 30% in our tenonectomy group.26–29 In contrast to our results, a previous study examining outcomes of patients who underwent XGS AEO with tenonectomy reported a needling rate of 18% and concluded that tenonectomy reduces the rate of postoperative needling.23 El Helwe et al observed a needling rate of only 2% in their AEO group with tenonectomy, compared to 27% in the AEC group17 While some studies align with the hypothesis that removing Tenon’s capsule can improve bleb morphology and function, its effect on reducing needling rates remains unclear. Surgical technique, patient-specific healing responses, and other perioperative factors may also significantly influence the need for postoperative needling.
This study has several limitations. We report early and intermediate postoperative events through a 12-month follow-up period, but this is relatively short for assessing very long-term fibrosis-related bleb failure. The retrospective design introduces potential biases, as it does not allow for control over variations in surgical techniques or clinical decision-making among surgeons. However, all procedures were performed or supervised by experienced glaucoma specialists, ensuring a consistent expert standard of care. Importantly, due to our non-randomized design, eyes selected for tenonectomy may have been those already at higher risk for failure. To address this, we employed a matching algorithm to balance baseline characteristics, though there may remain unaccounted-for confounding factors which are not recorded in the electronic health record and influenced both the decision to perform tenonectomy and the final outcomes. The small sample size, particularly in the tenonectomy group, limited the statistical power, such that clinically meaningful differences may not reach statistical significance. Lastly, the inclusion of secondary glaucoma types, such as traumatic glaucoma, may have a higher risk of surgical failure due to their complex pathology. Future work may focus on primary open-angle glaucoma, where XEN implantation is most commonly indicated. Future prospective studies with larger sample sizes and extended follow-up are important to validate our short-term preliminary results and better characterize the role of tenonectomy in glaucoma surgery.
Conclusion
In this preliminary study, XGS AEO with tenonectomy was associated with a trend toward higher survival probability and fewer reoperations and interventions compared to XGS AEO without tenonectomy, at the cost of slightly more hemorrhagic complications. These clinical patterns suggest that tenonectomy may be a reasonable option for patients at elevated risk for fibrosis. However, these findings should be interpreted as hypothesis-generating rather than definitive, and larger randomized studies are warranted to confirm this hypothesis.
Abbreviations
AEO, ab externo open conjunctiva; IOP, intraocular pressure; MIGS, microinvasive glaucoma surgery; XGS, XEN45 Gel Stent; MMC, mitomycin-C; BCVA, best-corrected visual acuity; LogMAR, logarithm of minimum angle of resolution; AC, anterior chamber; IQR, interquartile range; AEC, ab externo closed conjunctiva.
Acknowledgments
The authors would like to acknowledge Lucinda Sisk, consultant at the Yale Library StatLab, for statistical consultation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sherwood MB, Spaeth GL, Simmons ST, et al. Cysts of Tenon’s capsule following filtration surgery. Medical management. Arch Ophthalmol. 1987;105(11):1517–11. doi:10.1001/archopht.1987.01060110063032
2. Xi X, McMillan DH, Lehmann GM, et al. Ocular fibroblast diversity: implications for inflammation and ocular wound healing. Invest Ophthalmol Vis Sci. 2011;52(7):4859–4865. doi:10.1167/iovs.10-7066
3. Maumenee AE. External filtering operations for glaucoma: the mechanism of function and failure. Trans Am Ophthalmol Soc. 1960;58:319–328.
4. Skuta GL, Parrish RK. Wound healing in glaucoma filtering surgery. Surv Ophthalmol. 1987;32(3):149–170. doi:10.1016/0039-6257(87)90091-9
5. Raihan A, Sekhar CG, Naduvilath TJ, Dandona L. The role of tenonectomy in trabeculectomy. Indian J Ophthalmol. 1999;47(2).
6. Awadein A, El Sayed YM. Excision of tenon capsule in pediatric trabeculectomy: a Controlled Study. J Glaucoma. 2016;25(1):39–44. doi:10.1097/ijg.0000000000000220
7. Walton DS. Pediatric Glaucoma: angle Surgery and Glaucoma Drainage Devices. In: Giaconi JA, Law SK, Coleman AL, Caprioli J, editors. Pearls of Glaucoma Management. Berlin Heidelberg: Springer; 2010:403–408.
8. Sabogal E, Ingram Z, Odishelidze N, et al. Comparing outcomes of trabeculectomy with mitomycin c to 45 μm gelatin stent placed ab externo with open conjunctiva. Ophthalmol Glaucoma. 2024;7(3):232–241. doi:10.1016/j.ogla.2023.11.005
9. Ucar F, Cetinkaya S. Xen implantation in patients with primary open-angle glaucoma: comparison of two different techniques. Int Ophthalmol. 2020;40(10):2487–2494. doi:10.1007/s10792-020-01427-z
10. Tan NE, Tracer N, Terraciano A, Parikh HA, Panarelli JF, Radcliffe NM. Comparison of safety and efficacy between ab interno and ab externo approaches to XEN gel stent placement. Clin Ophthalmol. 2021;15:299–305. doi:10.2147/opth.S292007
11. Hasan SM, Theilig T, Tarhan M, Papadimitriou M, Unterlauft JD, Meller D. Novel bleb classification following ab interno implantation of gel-stent using anterior segment optical coherence tomography. J Glaucoma. 2023;32(2):117–126. doi:10.1097/ijg.0000000000002096
12. Dangda S, Radell JE, Mavrommatis MA, et al. Open conjunctival approach for sub-tenon’s xen gel stent placement and bleb morphology by anterior segment optical coherence tomography. J Glaucoma. 2021;30(11):988–995. doi:10.1097/ijg.0000000000001929
13. Cheng AMS, Gupta SK, Vedula GG, et al. Ab-Externo XEN Gel stent implantation effectively treated refractory glaucoma with prior failed shunt tube. BMC Ophthalmol. 2024;24(1):384. doi:10.1186/s12886-024-03648-7
14. Miller KN, Blasini M, Shields MB, Ho CH. A comparison of total and partial tenonectomy with trabeculectomy. Am J Ophthalmol. 1991;111(3):323–326. doi:10.1016/s0002-9394(14)72317-7
15. Susanna R. Partial Tenon’s capsule resection with adjunctive mitomycin C in Ahmed glaucoma valve implant surgery. Br J Ophthalmol. 2003;87(8):994–998. doi:10.1136/bjo.87.8.994
16. WGA guidelines on design and reporting of glaucoma surgical trials. Kugler Publications. 2009.
17. El Helwe H, Ingram Z, Falah H, Trzcinski J, Solá-Del Valle DA. Comparing outcomes of 45 μm gelatin stent placed ab externo with open conjunctiva to ab externo with closed conjunctiva. Ophthalmol Glaucoma. 2024;7(1):66–74. doi:10.1016/j.ogla.2023.07.009
18. Lee RMH, Bouremel Y, Eames I, Brocchini S, Khaw PT. The implications of an ab interno versus ab externo surgical approach on outflow resistance of a subconjunctival drainage device for intraocular pressure control. Transl Vis Sci Technol. 2019;8(3):58. doi:10.1167/tvst.8.3.58
19. Thatcher MD, Coupal DJ, Cheng Y, Podbielski DW. Short-Term efficacy and safety of open conjunctiva ab externo XEN45 gel stent implantation in glaucoma patients. J Glaucoma. 2022;31(9):757–762. doi:10.1097/ijg.0000000000002064
20. To LK, Dhoot RK, Chuang AZ, et al. Defining the role of ab externo Xen gel stent in glaucomatous eyes with prior failed surgical intervention. Graefes Arch Clin Exp Ophthalmol. 2023;261(3):779–789. doi:10.1007/s00417-022-05857-6
21. Ruda RC, Yuan L, Lai GM, Raiciulescu S, Kim WI. Clinical outcomes of ab interno placement versus ab externo placement of XEN45 gel stents. Ophthalmol Glaucoma. 2023;6(1):4–10. doi:10.1016/j.ogla.2022.07.002
22. Do A, McGlumphy E, Shukla A, et al. Comparison of clinical outcomes with open versus closed conjunctiva implantation of the XEN45 gel stent. Ophthalmol Glaucoma. 2021;4(4):343–349. doi:10.1016/j.ogla.2020.12.003
23. N A Johnson, A Li, L W Herndon. Postoperative outcomes of open conjunctival Ab-externo XEN implantation with tenonectomy. J Clin Ophthalmol. 2021;5(7):504–509.
24. Lin S, Byles D, Smith M. Long-term outcome of mitomycin C-augmented needle revision of trabeculectomy blebs for late trabeculectomy failure. Eye. 2018;32(12):1893–1899. doi:10.1038/s41433-018-0199-8
25. Midha N, Gillmann K, Chaudhary A, Mermoud A, Mansouri K. Efficacy of needling revision after XEN gel stent implantation: a prospective study. J Glaucoma. 2020;29(1):11–14. doi:10.1097/ijg.0000000000001394
26. Theilig T, Rehak M, Busch C, Bormann C, Schargus M, Unterlauft JD. Comparing the efficacy of trabeculectomy and XEN gel microstent implantation for the treatment of primary open-angle glaucoma: a retrospective monocentric comparative cohort study. Sci Rep. 2020;10(1):19337. doi:10.1038/s41598-020-76551-y
27. Yang X, Zhao Y, Zhong Y, Duan X. The efficacy of XEN gel stent implantation in glaucoma: a systematic review and meta-analysis. BMC Ophthalmol. 2022;22(1):305. doi:10.1186/s12886-022-02502-y
28. Arnould L, Balsat E, Hashimoto Y, et al. Two-year outcomes of Xen 45 gel stent implantation in patients with open-angle glaucoma: real-world data from the Fight Glaucoma Blindness registry. Br J Ophthalmol. 2024;108(12):1672–1678. doi:10.1136/bjo-2023-325077
29. Buffault J, Baudouin C, Labbé A. XEN(®) Gel Stent for management of chronic open angle glaucoma: a review of the literature. J Fr Ophtalmol. 2019;42(2):e37–e46. doi:10.1016/j.jfo.2018.12.002
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Multicenter 12-Month Retrospective Evaluation of Canaloplasty and Trabeculotomy in Patients with Open-Angle Glaucoma: The ROMEO 2 Study
Murphy III JT, Terveen DC, Aminlari AE, Dhamdhere K, Dickerson Jr JE
Clinical Ophthalmology 2022, 16:3043-3052
Published Date: 14 September 2022