Back to Journals » Clinical Ophthalmology » Volume 20
Short-Term Intraocular Pressure Changes After 0.1% Fluorometholone in Pediatric Strabismus Surgery
Authors Hozumi K ![]() , Yagasaki T
, Yagasaki T ![]() , Yokoyama Y
, Yokoyama Y ![]()
Received 16 October 2025
Accepted for publication 12 January 2026
Published 14 January 2026 Volume 2026:20 574783
DOI https://doi.org/10.2147/OPTH.S574783
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Kenta Hozumi,1 Teiji Yagasaki,1,2 Yoshimi Yokoyama1
1Department of Ophthalmology, Japan Community HealthCare Organization (JCHO) Chukyo Hospital, Nagoya, Aichi, Japan; 2Yagasaki Eye Clinic, Ichinomiya, Aichi, Japan
Correspondence: Kenta Hozumi, Department of Ophthalmology, Japan Community HealthCare Organization (JCHO) Chukyo Hospital, 1-1-10 Sanjo, Minami-ku, Nagoya, Aichi, 457-8510, Japan, Tel +81 52 691 7151, Fax +81 52 692 5220, Email [email protected]
Purpose: To investigate the effect of 0.1% fluorometholone ophthalmic solution (FM) on intraocular pressure (IOP) in children after strabismus surgery.
Patients and Methods: We included 224 eyes of 224 children aged < 15 years who underwent strabismus surgery at JCHO Chukyo Hospital from January 2014 to December 2023, received FM four times daily in the operated eye for 1 month postoperatively, and underwent IOP measurement using a non-contact tonometer NT-530Ⓡ (NIDEK Co. Ltd. Aichi, Japan). We assessed pre- and postoperative IOPs, postoperative changes in IOP, the number of children with a postoperative increase of > 6 mmHg in the IOP, and the number of children with a postoperative IOP > 20 mmHg.
Results: The participants included 106 boys and 118 girls, with a mean age of 8.6 years. The mean pre- and postoperative IOPs were 14.7 ± 2.4 mmHg and 14.8 ± 3.3 mmHg, respectively, with no significant difference (p = 0.552). At 1 month postoperatively, 8 eyes (3.6%) had an increase of > 6 mmHg, 14 eyes (6.3%) had a postoperative IOP > 20 mmHg, and 3 eyes (1.3%) had both.
Conclusion: Short-term use of FM may not significantly increase IOP and may be considered safe for anti-inflammatory treatment in pediatric patients after strabismus surgery.
Keywords: pediatric ophthalmology, steroid responder, strabismus surgery, postoperative complication, subconjunctival dexamethasone
Introduction
Steroid eye drops are frequently used for anti-inflammatory treatment; however, they may increase intraocular pressure (IOP) as a side effect.1,2 Therefore, cautious use is warranted. Although the impact of steroid eye drops on IOP in adults has been extensively investigated,3,4 there is limited research on this topic in pediatric populations.5
Compared with adults, children have a higher incidence of increased IOP following treatment with steroid eye drops,6 particularly younger children.7,8 Some reports suggest that 0.1% fluorometholone ophthalmic solution (FM) has a lower impact on IOP than other topical steroids.6–8 However, these studies included a limited number of pediatric cases treated with FM (≤20–30 cases) and did not fully elucidate the effect of FM on IOP in children; consequently, robust evidence in pediatric strabismus surgery remains limited.
In our previous study, we concluded that FM is unlikely to cause a significant increase in IOP in children after short-term use (1 month) and is considered safe for use in the anti-inflammatory treatment of pediatric patients.9 However, that report was published only in Japanese. Accordingly, the present study aims to validate these findings in a substantially larger cohort and to present the results to an international audience. Moreover, because some individuals exhibit an exaggerated IOP response to corticosteroids (“steroid responders”),10 this study also aimed to assess the prevalence of steroid responders among pediatric patients.
Materials and Methods
Study Design and Patients
In this retrospective cohort study, we included pediatric patients aged ≤15 years who underwent strabismus surgery at the Japan Community HealthCare Organization (JCHO) Chukyo Hospital Ophthalmology Department from January 1, 2014, to December 31, 2023. A total of 224 cases were included, comprising 108 bilateral, 64 left-eye, and 52 right-eye surgeries, in which both preoperative and 1-month postoperative IOP measurements were obtained using a non-contact tonometer (NT-530Ⓡ; NIDEK Co., Ltd., Aichi, Japan). For patients who underwent simultaneous bilateral surgery, a random algorithm was applied to include either the left or right eye. Specifically, a computer randomly assigned a value of 0 or 1 to each case; with 0 indicating selection of the right-eye IOP, and 1 indicating selection of the left-eye IOP. Consequently, a total of 224 eyes were included in the analysis.
The exclusion criteria were as follows: reoperation, simultaneous surgery involving three or more extraocular muscles per eye; a history of systemic or ocular diseases that may influence intraocular pressure such as glaucoma; use of systemic or topical corticosteroids; and failure to adhere to the prescribed eye drop regimen. Additionally, IOP measurement at 1 month postoperatively was mandatory, and patients without available measurements were excluded.
All surgeries were conducted under general anesthesia through either a limbal or fornix conjunctival incision, with the conjunctiva closed using 8–0 polyglycolic acid sutures. The choice of incision (limbal or fornix) followed a standardized protocol. All procedures were performed by five surgeons; however, because all surgeons were experienced, surgeon-related effects on IOP were considered negligible. After surgery, 0.5 mL of dexamethasone sodium phosphate was administered via subconjunctival injection. Beginning on postoperative day 1, FM and 1.5% levofloxacin eye drops were administered four times a day for ≥1 month. Postoperative visits were scheduled on postoperative day 1, day 7, and at 1 month, with IOP measured at each visit using a non-contact tonometer (NT-530Ⓡ; NIDEK Co., Ltd). Changes in IOP were evaluated by comparing baseline and 1-month postoperative values, including both absolute IOP and the percentage change (1-month postoperative ― preoperative; Δ%IOP). Preoperative IOP was measured 2–5 times per eye on separate examination days, and the mean value was used for analysis. In cases of IOP elevation during the observation period, antiglaucoma eye drops were initiated or steroid eye drops were discontinued at the discretion of the examining physician.
The severity of steroid-induced IOP elevation was classified into three categories—no response, low response, and high response—as described by Armaly10 and Becker11 (Table 1), based on the postoperative IOP values and postoperative changes in IOP. According to Armaly’s criteria, a postoperative–preoperative IOP difference of <6 mmHg indicates no response, 6 to <15 mmHg indicates a low response, and ≥15 mmHg indicates a high response. According to Becker’s criteria, a postoperative IOP of <20 mmHg indicates no response, 20 to <30 mmHg indicates a low response, and ≥30 mmHg indicates a high response.
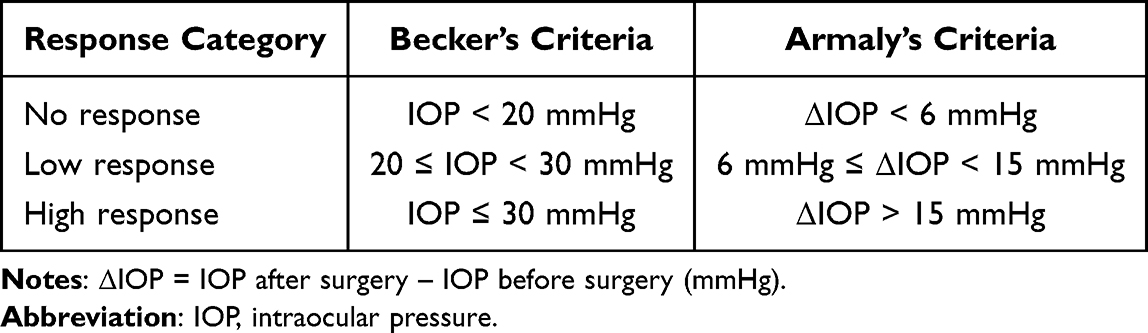 |
Table 1 Criteria for IOP Change in This Study |
Additionally, preoperative, postoperative, and changes in IOP values were compared between two pediatric age groups (<10 years and ≥10 years) to assess whether the impact of steroid eye drops on IOP varied by age.
Postoperative ocular surface symptoms, including redness, stinging, burning, foreign body sensation, and allergy-related symptoms, were assessed and documented at 1 month after surgery.
The primary endpoint was the mean absolute change and percentage change in IOP at 1 month. Secondary endpoints included the proportion of eyes meeting the Armaly and Becker criteria, age-group comparisons, and postoperative ocular surface symptoms at 1 month after surgery.
This retrospective study was approved by the Ethics Committee of JCHO Chukyo Hospital (approval number: 2019033) on February 3, 2020. All procedures were performed in accordance with the tenets of the Declaration of Helsinki.
Statistical Analysis
Preoperative and 1-month postoperative IOP values in the same pediatric patients were compared using a paired t-test. Age-group comparisons of baseline IOP, 1-month postoperative IOP, and IOP change were performed using Welch’s t-test to account for potential differences in sample size or variance between groups. All statistical analyses were performed using GraphPad Prism (GraphPad Software, San Diego, USA) and Microsoft Excel for Windows version 16 (Microsoft Corp., Redmond, WA, USA). Statistical significance was set at P < 0.05.
Results
The study population comprised 106 boys and 118 girls, with a mean age of 8.6 ± 2.6 years (range: 4–14 years). The mean IOP before surgery and at 1 month postoperatively was 14.7 ± 2.4 mmHg and 14.8 ± 3.3 mmHg, respectively, with no significant difference (p = 0.552). The mean IOP elevation at 1 month postoperatively was 0.2 ± 2.9 mmHg. At 1 month postoperatively, 8 (3.5%) eyes had a postoperative IOP increase of >6 mmHg (range: 6.3–10.0 mmHg), 14 eyes (6.3%) had a postoperative IOP >20 mmHg (range: 20–29 mmHg), and 3 eyes (1.3%) met both criteria (Table 2). According to the classifications proposed by Armaly10 and Becker,11 all eyes were categorized as having no response or a low response, and no high responders were identified.
 |
Table 2 Intraocular Pressure Response at 1 month Postoperatively |
The mean Δ%IOP was +2.1 ± 20.7%, with a median of 0%. Δ%IOP was <0% in 115 cases (51.3%), 0% to +10% in 43 cases (19.2%), +10% to +20% in 32 cases (14.3%), and >+20% in 33 cases (15.2%) (Figure 1).
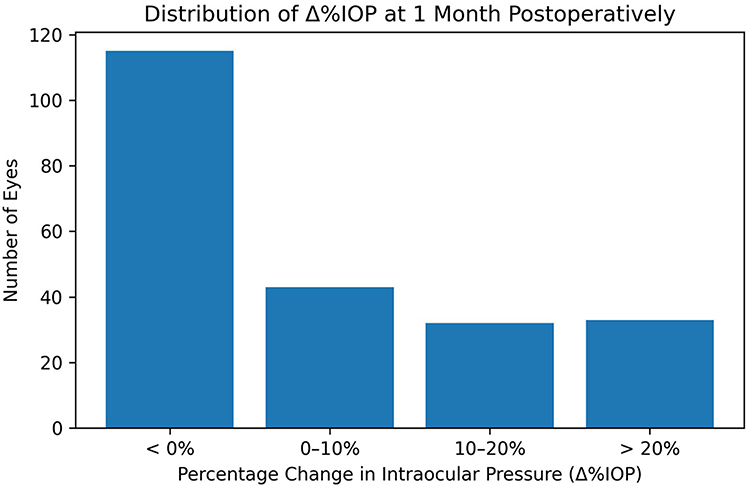 |
Figure 1 Percentage change in intraocular pressure (Δ%IOP) at 1 month postoperatively relative to baseline. Notes: Δ%IOP = [(postoperative IOP – preoperative IOP) / preoperative IOP] x 100%. |
When stratified by age group, children aged ≥10 years had a significantly higher mean postoperative IOP than children aged <10 years (p = 0.006). In contrast, no significant differences were observed in mean preoperative IOP (p = 0.074) or in the change in IOP following eye drop administration (p = 0.116) (Table 3).
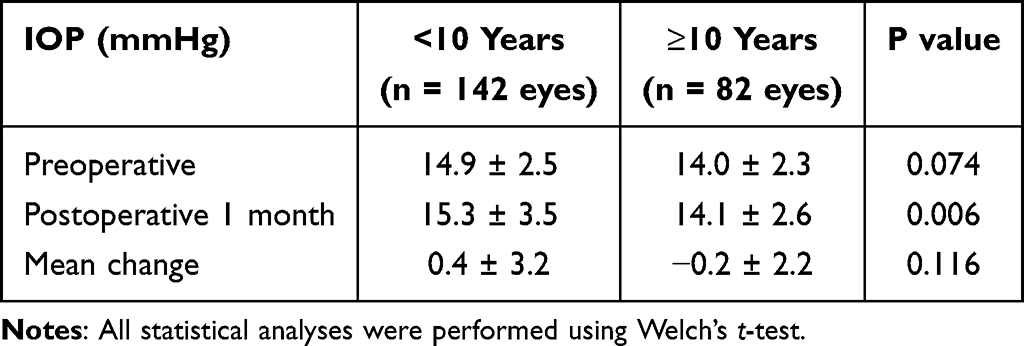 |
Table 3 Comparison of Pre- and Postoperative Mean IOP Between Age Groups |
No patients reported postoperative ocular surface symptoms, including redness, stinging, burning, foreign body sensation, or allergy-related symptoms, at 1 month after surgery.
Regarding the immediate postoperative course, one eye showed a high IOP of 27 mmHg at 1 week postoperatively. In this case, FM was continued, with the additional prescription of carteolol hydrochloride eye drops. Another eye showed a high IOP of 30 mmHg at 1 week postoperatively, which was attributed to severe conjunctival edema displacing the eyeball outward. In both cases, FM was continued, and the IOP normalized at 1 month postoperatively, with no subsequent recurrence of IOP elevation. No cases required the addition of other anti-inflammatory agents because of insufficient anti-inflammatory efficacy of FM.
Discussion
This study evaluated the magnitude and frequency of IOP elevation following short-term use of FM in a large cohort of pediatric patients who underwent strabismus surgery. The findings demonstrated no significant increase in IOP at 1 month postoperatively compared with preoperative values. According to both the Armaly and Becker criteria, all eyes at 1 month postoperatively were classified as no response or low responders, indicating a low likelihood of clinically meaningful steroid-induced IOP elevation with short-term FM use.
Ohji et al reported that all nine patients aged <10 years who were treated with 0.1% dexamethasone after strabismus surgery experienced an Armaly standard hypo- or hyper-responsive IOP increase at 2 weeks.8 However, no IOP elevation was reported in 11 patients aged ≥10 years who were treated with 0.1% dexamethasone and 13 patients aged <10 years who were treated with FM.8
Hanaineh et al12 reported that among 20 pediatric patients aged ≤12 years who underwent strabismus surgery, the FM-induced IOP increase was significantly lower than that in the 0.1% dexamethasone group; two eyes (10.0%) met Armaly’s criteria and one eye (5.0%) met Becker’s criteria. Moreover, Yung et al7 reported an FM-induced IOP increase that met Becker’s criteria in 4 out of 30 (7.5%) patients, indicating that FM was significantly safer than 0.5% etabonate ophthalmic solution. In the present study, 8 eyes (3.6%) and 14 eyes (6.3%) showed IOP elevation meeting Armaly’s and Becker’s criteria, respectively, following treatment with FM, which is consistent with previous reports.
Dror et al conducted a meta-analysis of seven articles from five regions reporting on the use of soft steroids (FM or 0.5% etabonate) or standard steroids (prednisolone acetate 1% or dexamethasone 0.1%). Specifically, they included 593 patients and compared the postoperative anti-inflammatory effects and IOP values between the soft and standard steroid groups.5,13–19 IOP values were lower in the soft steroid group than in the standard steroid group on postoperative days 1, 7, and 28. An increase of ≥10 mmHg in IOP from the preoperative value was observed in one case in the standard group, but not in the soft group. This was attributed to endophthalmic surgery, in which the drug tends to migrate into the anterior chamber. Since we included patients who underwent external ocular surgery, the risk of IOP elevation following treatment with soft steroid eye drops can be considered relatively low.
FM has a lower intraocular transfer rate than other steroid preparations.20,21 The mechanism underlying steroid-induced IOP elevation may involve steroid-dependent deposition of extracellular matrix in the aqueous humor, resulting in increased aqueous humor resistance in the fibrovascular zone and elevated IOP.22 Based on this hypothesis, FM, which has a lower intraocular transfer rate than other steroids, is less likely to increase IOP compared with other steroid eye drops.
Hyperemia, edema, and pain resulting from inflammatory reactions are common after strabismus surgery.23–26 However, because the surgical site primarily involves the extraocular muscles and surrounding connective tissues, including the conjunctiva and Tenon’s capsule, FM is considered to provide sufficient anti-inflammatory efficacy despite its relatively low intraocular penetration. In the present study, no case demonstrated insufficient anti-inflammatory effects with FM, and no additional anti-inflammatory agents were required. Escardó-Paton et al assessed the duration of conjunctival hyperemia following strabismus surgery in adults.26 In that study, conjunctival hyperemia persisted for approximately 9 weeks after administration of 0.1% betamethasone, with eye drops used for only 2 postoperative weeks and no additional treatment. Regarding postoperative pain, children have been reported to experience significantly shorter pain duration and lower pain severity than adults following strabismus surgery.27 Taken together, these findings support the effectiveness of FM administered for approximately 1 month after pediatric strabismus surgery.
In addition, no significant difference in IOP elevation following FM treatment was observed between children aged ≥10 years and those aged <10 years. Previous studies have suggested that steroid eye drops are more likely to increase IOP in patients aged <10 years.5,6 However, other studies have indicated that FM carries a lower risk of IOP elevation than other steroid eye drops, regardless of patient age.28 Taken together, these findings suggest that FM-induced IOP elevation does not differ significantly by age.
Although the primary study endpoint was IOP at 1 month postoperatively, one eye showed an IOP of 27 mmHg at 1 week postoperatively, representing a 10-mmHg increase from the preoperative value. In this study, all patients received a subconjunctival injection of 0.5 mL dexamethasone sodium phosphate at the conclusion of surgery. The reported half-life of dexamethasone in blood is 1.5–3.0 days,29 suggesting that the subconjunctival injection may have contributed to early postoperative IOP elevation. In this case, IOP normalized with concomitant use of IOP-lowering agents while FM was continued, and no recurrence occurred after discontinuing IOP-lowering agents. Another eye was followed for >1 postoperative month but was excluded from the analysis because IOP was slightly elevated at 1 week postoperatively (24 mmHg in the right eye and 21 mmHg in the left eyes) leading to discontinuation of FM. In a separate case, IOP reached 30 mmHg immediately after surgery and remained elevated during the first postoperative week. The patient experienced severe conjunctival edema starting the day after surgery, which may have externally increased the IOP. The patient continued FM treatment, and IOP normalized as the conjunctival edema resolved, with no subsequent elevations despite ongoing FM administration.
This study has several limitations. First, IOP measurements were not performed on a fixed schedule, and the influence of diurnal variation cannot be ruled out. Diurnal variations of IOP in children remain unclear; however, it is estimated to be approximately 5 mmHg in adults, and Becker’s criteria may overestimate the number of eyes with high IOP.
Second, the results are limited to the use of FM in pediatric strabismus surgery and may not be generalizable to other conditions. Anterior chamber migration of ophthalmic solutions is regulated by the barrier function of the corneal epithelium and parenchyma.30,31 Therefore, in cases of impaired barrier function, such as corneal epithelial or parenchymal damage, the risk of IOP elevation may be increased due to enhanced anterior chamber penetration. In our study, no patients exhibited corneal epithelial damage up to 1 month postoperatively, suggesting that corneal barrier dysfunction did not influence IOP elevation. However, when FM is used to treat vernal keratoconjunctivitis with shield ulcers, the risk of IOP elevation may be higher. In such cases, more intensive IOP monitoring is warranted, and switching to alternative anti-inflammatory agents, such as tacrolimus ophthalmic suspension, may be necessary if IOP increases.
Third, the potential effect of subconjunctival dexamethasone injection on postoperative IOP should be considered. All patients in this study received a subconjunctival dexamethasone injection at the end of surgery. Dexamethasone is associated with a higher risk of IOP elevation than FM12 and may contribute to early postoperative IOP elevation. In this study, IOP elevation possibly related to dexamethasone injection was observed in only one eye at 1 week postoperatively. Given the reported half-life of dexamethasone (1.5–3.0 days), FM in combination with a single subconjunctival dexamethasone injection did not appear to cause clinically significant IOP elevation at 1 month, the primary endpoint of this study.
Fourth, the use of a non-contact tonometer in children may introduce additional measurement variability compared with Goldmann applanation tonometry. However, the routine use of Goldmann applanation tonometry in pediatric patients is often impractical. Therefore, in a retrospective study reflecting real-world clinical practice, evaluation using IOP obtained with a non-contact tonometer is considered acceptable.
Fifth, assessment of normality and homogeneity of the IOP data was not performed. As this was a retrospective study using measured values, prior adjustment for statistical assumptions may have been difficult.
Finally, this study had a relatively short observation period of 1 month. Steroids have been shown to induce volume-dependent IOP increases.32,33 Therefore, the possibility of a delayed IOP elevation with long-term FM use cannot be excluded. In our study, only a few cases exhibited IOP elevation within the short observation period. These findings highlight the need for regular IOP monitoring during FM use, regardless of treatment duration.
Conclusion
In this cohort, 0.1% FM administered for approximately 1 month after strabismus surgery, in combination with a single subconjunctival dexamethasone injection, was not associated with clinically significant IOP elevation at 1 month in most children. Nonetheless, regular IOP monitoring remains advisable during steroid therapy.
Abbreviations
IOP, Intraocular pressure; FM, 0.1% fluorometholone ophthalmic solution.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This clinical study was approved by the Ethics Committee of JCHO Chukyo Hospital (approval number: 2019033) on February 3, 2020. Informed consent was obtained from the parents or guardians of all participants. All procedures were conducted in accordance with the tenets of the Declaration of Helsinki.
Acknowledgments
We would like to thank Editage (www.editage.com) for English language editing.
Funding
The authors declare that they have received no funding for the conduct of this study.
Disclosure
The authors report no conflicts of interests in this work.
References
1. Price MO, Price DA, Price FW. Long-term risk of steroid-induced ocular hypertension/glaucoma with topical prednisolone acetate 1% after descemet stripping endothelial keratoplasty. Cornea. 2024;43(3):323–7. doi:10.1097/ICO.0000000000003312
2. Price MO, Price FW, Kruse FE, Bachmann BO, Tourtas T. Randomized comparison of topical prednisolone acetate 1% versus fluorometholone 0.1% in the first year after descemet membrane endothelial keratoplasty. Cornea. 2014;33(9):880–886. doi:10.1097/ICO.0000000000000206
3. Kitazawa Y. Increased intraocular pressure induced by corticosteroids. Am J Ophthalmol. 1976;82(3):492–495. doi:10.1016/0002-9394(76)90500-6
4. Bartlett JD, Woolley TW, Adams CM. Identification of high intraocular pressure responders to topical ophthalmic corticosteroids. J Ocul Pharmacol. 1993;9(1):35–45. doi:10.1089/jop.1993.9.35
5. Vittitow JL, Williams JI. Loteprednol etabonate gel 0.5% vs prednisolone acetate suspension 1% for the treatment of inflammation after cataract surgery in children. J Cataract Refract Surg. 2020;46(8):1092–1101. doi:10.1097/j.jcrs.0000000000000218
6. Kwok AK, Lam DS, Ng JS, Fan DS, Chew SJ, Tso MO. Ocular-hypertensive response to topical steroids in children. Ophthalmology. 1997;104(12):2112–2116. doi:10.1016/S0161-6420(97)30052-9
7. Yoo YJ, Yang HK, Hwang JM. Efficacy and safety of loteprednol 0.5% and fluorometholone 0.1% after strabismus surgery in children. J Ocul Pharmacol Ther. 2018;34(6):468–476. doi:10.1089/jop.2017.0145
8. Ohji M, Kinoshita S, Ohmi E, Kuwayama Y. Marked intraocular pressure response to instillation of corticosteroids in children. Am J Ophthalmol. 1991;112(4):450–454. doi:10.1016/S0002-9394(14)76256-7
9. Hozumi K, et al. Examination of the short-term impact of fluorometholone 0.1% on Japanese children. J Jpn Ophthalmol Soc. 2023;127:543–548. (in Japanese).
10. Armaly MF. Statistical attributes of the steroid hypertensive response in the clinically normal eye I. The demonstration of three levels of response. Invest Ophthalmol. 1965;4(2):187–197.
11. Becker B. Intraocular pressure response to topical corticosteroids. Invest Ophthalmol. 1965;4(2):198–205.
12. Al Hanaineh AT, Hassanein DH, Abdelbaky SH, El Zawahry OM. Steroid-induced ocular hypertension in the pediatric age group. Eur J Ophthalmol. 2018;28(4):372–377. doi:10.1177/1120672118757434
13. Noyman DBE, Chan CC, Mimouni M, Safir M. The efficacy and safety of standard versus soft topical steroids after cataract surgery: a systematic review and meta-analysis. Ophthalmology. 2024;131(5):595–610. doi:10.1016/j.ophtha.2023.11.022
14. Chen PQ, Han XM, Zhu YN, Xu J. Comparison of the anti-inflammatory effects of fluorometholone 0.1% combined with levofloxacin 0.5% and tobramycin/dexamethasone eye drops after cataract surgery. Int J Ophthalmol. 2016;9(11):1619–1623. doi:10.18240/ijo.2016.11.13
15. Wang QW, Yao K, Xu W, et al. Bromfenac sodium 0.1%, fluorometholone 0.1% and dexamethasone 0.1% for control of ocular inflammation and prevention of cystoid macular edema after phacoemulsification. Ophthalmologica. 2013;229(4):187–194. doi:10.1159/000346847
16. Trinavarat A, Atchaneeyasakul LO, Surachatkumtonekul T, Kosrirukvongs P. Comparison of topical prednisolone acetate, ketorolac tromethamine and fluorometholone acetate in reducing inflammation after phacoemulsification. J Med Assoc Thai. 2003;86(2):143–150.
17. van Endt JJ, Veraart HG, Kramer R, Janssen AG, Sunder Raj P. A comparison of two ophthalmic steroid-antibiotic combinations after cataract surgery. Eur J Ophthalmol. 1997;7(2):144–148. doi:10.1177/112067219700700204
18. Kaur R, Matreja PS, Khan B, Bhatnagar RN. Compare the safety and efficacy of loteprednol etabonate 0.5% and prednisolone acetate 1% in the post operative inflammation following cataract extraction with intraocular lens (IOL) implant. Ann Appl Bio-sci. 2015;2.
19. Lane SS, Holland EJ. Loteprednol etabonate 0.5% versus prednisolone acetate 1.0% for the treatment of inflammation after cataract surgery. J Cataract Refract Surg. 2013;39(2):168–173. doi:10.1016/j.jcrs.2012.10.039
20. Kupferman A, Leibowitz HM. Penetration of fluorometholone into the cornea and aqueous humor. Arch Ophthalmol. 1975;93(6):425–427. doi:10.1001/archopht.1975.01010020439008
21. Yamauchi H, Kito H, Uda K. Studies on intraocular penetration and metabolism of fluoromethalone in rabbits: a comparison between dexamethasone and prednisolone acetate. Jpn J Ophthalmol. 1975;19(4):339–347.
22. Kubota T, Okabe H, Hisatomi T, Yamakiri K, Sakamoto T, Tawara A. Ultrastructure of the trabecular meshwork in secondary glaucoma eyes after intravitreal triamcinolone acetonide. J Glaucoma. 2006;15(2):117–119. doi:10.1097/00061198-200604000-00007
23. Bradbury JA, Taylor RH. Severe complications of strabismus surgery. J AAPOS. 2013;17(1):59–63. doi:10.1016/j.jaapos.2012.10.016
24. Wan MJ, Hunter DG. Complications of strabismus surgery: incidence and risk factors. Semin Ophthalmol. 2014;29(5–6):421–428. doi:10.3109/08820538.2014.959190
25. Olitsky SE, Coats DK. Complications of strabismus surgery. Middle East Afr J Ophthalmol. 2015;22(3):271–278. doi:10.4103/0974-9233.159692
26. Escardó-Paton JA, Harrad RA. Duration of conjunctival redness following adult strabismus surgery. J AAPOS. 2009;13(6):583–586. doi:10.1016/j.jaapos.2009.09.013
27. Camille B, et al. Evaluation of postoperative pain and painkiller consumption after strabismus surgery, differences between adults and children. Assoc Res Vis Ophthalmol Annu Meet. 2014.
28. Sen P, Jain S, Mohan A, Shah C, Sen A, Jain E. Pattern of steroid misuse in vernal keratoconjunctivitis resulting in steroid induced glaucoma and visual disability in Indian rural population: an important public health problem in pediatric age group. Indian J Ophthalmol. 2019;67(10):1650–1655. doi:10.4103/ijo.IJO_2143_18
29. Schimmer BP, Parker KL. Adrenocorticotropic hormone; adrenocortical steroids and their synthetic analogs; inhibitors of the synthesis and actions of adrenocortical hormones. In: Gilman AG, editor. Pharmacological Basis of Therapeutics,
30. Schoenwald RD, Huang HS. Corneal penetration behavior of beta-blocking agents I: physiochemical factors. J Pharm Sci. 1983;72(11):1266–1272. doi:10.1002/jps.2600721108
31. Chien DS, Sasaki H, Bundgaard H, Buur A, Lee VH. Role of enzymatic lability in the corneal and conjunctival penetration of timolol ester prodrugs in the pigmented rabbit. Pharm Res. 1991;8(6):728–733. doi:10.1023/A:1015845916293
32. Ng JS, Fan DS, Young AL, et al. Ocular hypertensive response to topical dexamethasone in children: a dose-dependent phenomenon. Ophthalmology. 2000;107(11):2097–2100. doi:10.1016/S0161-6420(00)00357-2
33. Fan DS, Ng JS, Lam DS. A prospective study on ocular hypertensive and antiinflammatory response to different dosages of fluorometholone in children. Ophthalmology. 2001;108(11):1973–1977. doi:10.1016/S0161-6420(01)00781-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.