Back to Journals » Research and Reports in Urology » Volume 17
Short-Term Functional Outcomes After Robot-Assisted Sacrocolpopexy versus Transvaginal Mesh Surgery for Pelvic Organ Prolapse: A Retrospective Comparative Study
Authors Hanawa K ![]() , Miyashita Y, Usami Y, Doba K, Kimura R, Mitsui T
, Miyashita Y, Usami Y, Doba K, Kimura R, Mitsui T
Received 19 July 2025
Accepted for publication 17 November 2025
Published 22 November 2025 Volume 2025:17 Pages 461—468
DOI https://doi.org/10.2147/RRU.S554947
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Guglielmo Mantica
Kazushi Hanawa,1,2 Yukie Miyashita,3 Yoshito Usami,1 Keisuke Doba,1 Ryosuke Kimura,1 Takahiko Mitsui2
1Department of Urology, Shizuoka Saiseikai General Hospital, Shizuoka, Japan; 2Department of Urology, Interdisciplinary Graduate School of Medicine, University of Yamanashi, Chuo, Yamanashi, Japan; 3Department of Urogynecology, Shizuoka Saiseikai General Hospital, Shizuoka, Japan
Correspondence: Kazushi Hanawa, Department of Urology, Shizuoka Saiseikai General Hospital, 1-1-1 Oshika, Suruga-ku, Shizuoka, 422-8021, Japan, Tel +81542856171, Fax +81542855179, Email [email protected]
Purpose: This study aimed to compare lower urinary tract symptoms (LUTS) in women with pelvic organ prolapse (POP) undergoing robot-assisted sacrocolpopexy (RSC) or transvaginal mesh surgery (TVM).
Methods: A retrospective analysis was conducted on patients who underwent RSC or TVM at our institution between August 2017 and December 2024. Patient demographics, surgical records, and questionnaire responses were collected. LUTS were evaluated using the Overactive Bladder Symptom Score (OABSS), International Prostate Symptom Score (IPSS), and Quality of Life (QOL) score. Preoperative and 1-month postoperative questionnaire responses were compared within each group using the Mann–Whitney U-test. Intergroup comparisons were performed after adjusting for baseline differences through propensity score matching, and their significance was analyzed using the Wilcoxon rank-sum test.
Results: A total of 51 patients underwent RSC and 21 underwent TVM. No significant differences were observed in age, body mass index, or Pelvic Organ Prolapse Quantification stage between the groups. The RSC group had a longer operative time (273 vs 127 minutes, p < 0.01) and less blood loss (10.0 vs 150 mL, p < 0.01). Both groups showed significant improvements in IPSS and QOL scores, whereas the OABSS did not change significantly. The RSC group had a significantly lower postoperative QOL score compared with the TVM group, but no significant differences were found after propensity score matching. No significant differences were observed between the groups in either the absolute changes or relative reductions of LUTS questionnaire scores. The incidence of de novo stress urinary incontinence was similar between the groups.
Conclusion: Both RSC and TVM effectively improved LUTS in women with POP. After adjusting for baseline differences, no significant differences in postoperative voiding symptoms were observed between the two procedures. These findings support flexible surgical decision-making based on patient characteristics, perioperative risks, surgeon experience, and shared decision-making.
Keywords: robot-assisted sacrocolpopexy, transvaginal mesh surgery, pelvic organ prolapse, overactive bladder symptom score, quality of life score, de novo stress urinary incontinence
Introduction
Pelvic organ prolapse (POP) is a prevalent condition in women, characterized by the descent of pelvic organs, including the bladder, uterus, or rectum, into the vaginal canal. When evaluated according to symptomatic definitions, the prevalence of POP is reported to be approximately 3%–6%, but this may reach up to 50% when assessed by vaginal examination.1 The established risk factors for POP include vaginal delivery, multiparity, elevated body mass index (BMI), and menopause, all of which contribute to the weakening of pelvic support structures.2–4 POP can cause significant morbidity, adversely affecting urinary, bowel, and sexual function, as well as overall quality of life.
Women with mild-to-moderate symptoms are generally prescribed conservative management strategies, including pelvic floor muscle training and pessary use.4 However, women with severe or refractory prolapse often require surgical intervention to restore anatomical support and improve symptoms.5 Surgical approaches may involve native tissue repair or mesh augmentation. The widely performed mesh-based procedures include transvaginal mesh surgery (TVM) and abdominal approaches, such as laparoscopic sacrocolpopexy and robot-assisted sacrocolpopexy (RSC).
Over the years, TVM has faced increased scrutiny because of concerns regarding mesh-related complications, such as mesh erosion, infection, and chronic pain.6 In fact, TVM has been withdrawn from the market in several countries, including the United States, leading to the emergence of laparoscopic sacrocolpopexy and RSC as the preferred mesh-augmented surgical options. RSC, in particular, offers advantages such as enhanced visualization, greater surgical precision, and reduced blood loss, albeit at the expense of longer operative times and higher costs.
Beyond anatomical outcomes, clinicians are increasingly focusing on the functional impact of prolapse surgery, particularly its impact on lower urinary tract symptoms (LUTS). Many women with POP experience LUTS preoperatively, including urinary frequency, urgency, incomplete emptying, stress urinary incontinence (SUI), and urinary retention.7 Surgical correction often improves obstructive voiding symptoms by restoring anatomical support; however, it can also precipitate new or worsening symptoms, notably de novo SUI due to changes in bladder outlet dynamics.8
While anatomical success rates of RSC and TVM have been compared extensively, few studies have focused on subjective, patient-reported functional outcomes. Furthermore, validated voiding-related questionnaires, such as the Overactive Bladder Symptom Score (OABSS), International Prostate Symptom Score (IPSS), and Quality of Life (QOL) score, have been underutilized in comparative studies.
Despite the global decline in TVM usage, TVM is still performed in some countries, but long-term data on its functional outcomes remain limited. A comparative analysis of the effects of RSC and TVM on urinary function is crucial, particularly in the context of informed surgical decision-making for POP. This study provides clinically meaningful data to inform surgical decision-making and enhance preoperative counseling regarding expectations for postoperative urinary function.
Materials and Methods
This retrospective study included patients who underwent POP surgery at Shizuoka Saiseikai General Hospital between August 2017 and December 2024. The RSC group comprised 51 cases, whereas the TVM group comprised 21 cases. The choice of surgical procedure was based on patient preference and shared decision-making. Patients were informed of both RSC and TVM, and the final decision was made based on individual comorbidities and surgical risks. All procedures were performed by a single surgeon with expertise in urogynecology. TVM was performed using the Elevate-type transvaginal mesh, and the posterior arms of the mesh were anchored to the sacrospinous ligaments using the Capio® suturing device (Boston Scientific). RSC was performed using a double mesh technique with both anterior and posterior mesh placement in all cases except one, which involved only anterior mesh placement. The surgeon collected and stored demographic data (age, BMI, stage), operative data, and questionnaire responses in the electronic medical records. The severity of POP was assessed using the POP Quantification (POP-Q) stage classification. To assess the improvement in urinary function following surgery, preoperative and postoperative questionnaires on LUTS were analyzed within each group. Lower urinary tract function was evaluated using the OABSS, QOL score, and supplementary IPSS. We collected questionnaires during the preoperative outpatient visit and during the first postoperative visit, which was conducted 1 month after surgery. Relative reduction was defined as (preoperative score – postoperative score)/preoperative score × 100. The presence of de novo SUI was confirmed based on patient interviews and questionnaire responses at the first postoperative visit. Regarding preoperative and postoperative OAB medication use, no recorded changes were identified during the study period based on available medical records, but it is possible that unrecorded variations may have influenced the OABSS results. The primary outcome of this study was the change in LUTS from baseline to 1 month after surgery, as assessed by the OABSS, IPSS, and QOL score. Secondary outcomes included operative time, blood loss, postvoid residual volume (PVR), and the incidence of de novo SUI.
The statistical significance of comparisons was determined using the Mann–Whitney U-test, with a p-value < 0.05 indicative of a significant difference. Propensity score matching was performed on the basis of age, BMI, and POP-Q stage to minimize baseline differences between the groups. After matching, questionnaire responses were compared between the RSC and TVM groups using the Wilcoxon rank-sum test. This retrospective study was approved by the Ethics Committee of Shizuoka Saiseikai General Hospital and all patients provided informed consent for their data to be used in a manner that does not reveal personal information. In accordance with the committee’s guidelines, informed consent was obtained using an opt-out method, whereby information regarding the study was made available to patients and the opportunity to decline participation was provided. The study was conducted in accordance with the principles of the Declaration of Helsinki and relevant national regulations.
Results
Patient demographics are presented in Table 1. In the RSC and TVM groups, the median patient age was 71 vs 73 years (p = 0.32) and the median BMI was 23.82 vs 25.50 kg/m2 (p = 0.10), respectively. Of the 51 patients in the RSC group, 41 were classified as stage III and 10 as stage IV, according to the POP-Q staging system. Of the 21 patients in the TVM group, 1 was classified as stage II, 11 as stage III, and 9 as stage IV. The POP-Q stage distribution did not differ significantly between the groups (p = 0.10). Cystocele was the most common type of POP in both groups.
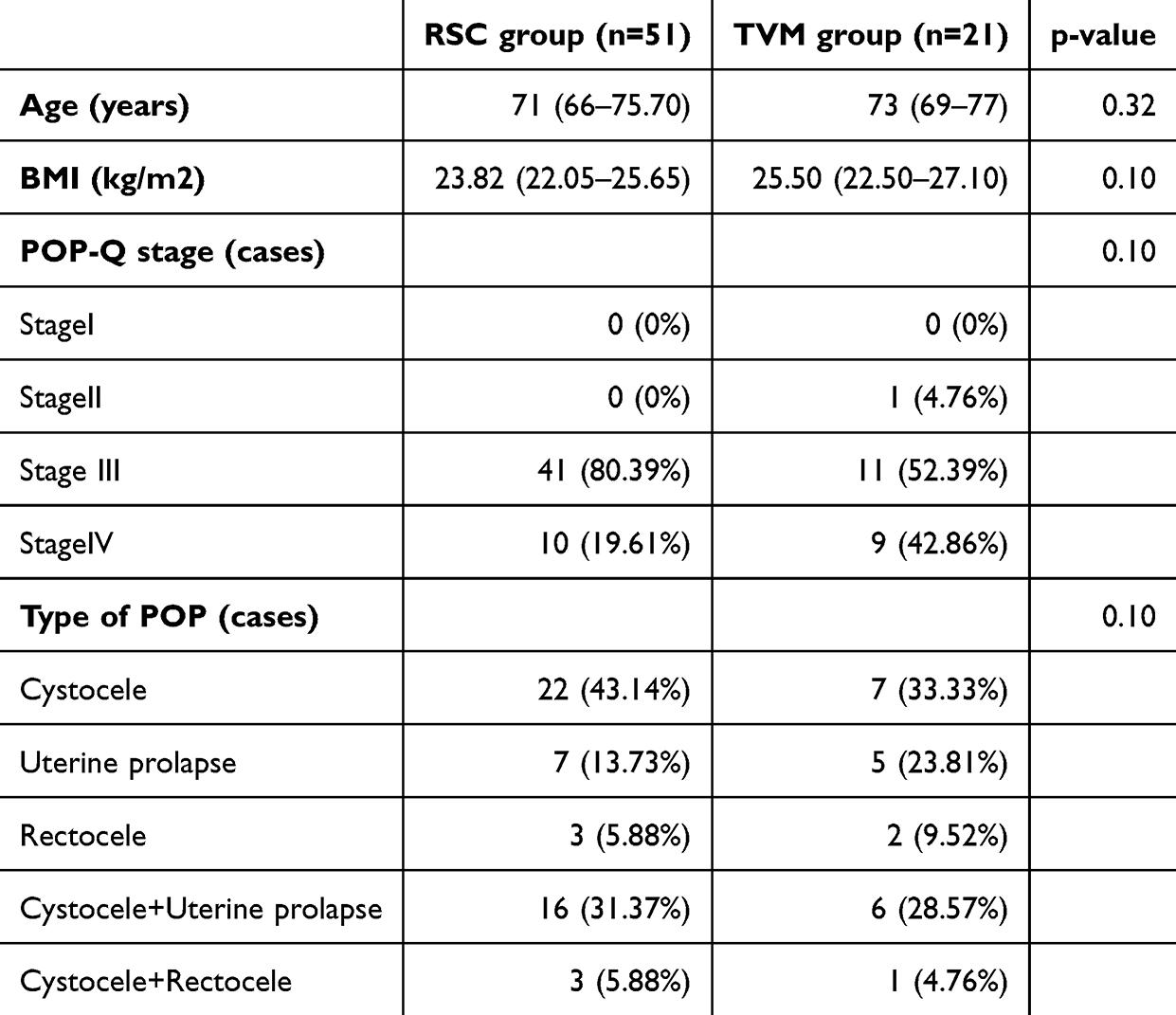 |
Table 1 Patient Demographics in the RSC and TVM Groups |
The surgical outcomes are summarized in Table 2. The median operative time was significantly longer in the RSC group compared with the TVM group (273 vs 127 minutes, respectively; p < 0.01). Estimated blood loss was significantly lower in the RSC group (10 mL vs 150 mL, p < 0.01). No cases of postoperative recurrence were observed in the RSC group, whereas one such case was reported in the TVM group (p = 0.54). The incidence rate of de novo SUI within 1 month postsurgery was 17.65% in the RSC group and 14.29% in the TVM group, exhibiting no significant difference (p = 0.74).
 |
Table 2 Surgical Outcomes in the RSC and TVM Groups |
The LUTS questionnaire results and PVR data are shown in Table 3. Preoperatively, the RSC group differed significantly from the TVM group in the OABSS (5 vs 9), QOL score (5 vs 6), and IPSS (11 vs 21; p < 0.01 for all). Postoperatively, the two groups differed significantly only in the QOL score (p = 0.04).
 |
Table 3 Preoperative and Postoperative LUTS Questionnaire Results and PVR in the RSC and TVM Groups |
The comparison of LUTS questionnaire results and PVR are shown in Table 4. In the RSC group, a trend toward improvement in OABSS was observed between the preoperative and postoperative periods, although it was not statistically significant (5 vs 3, p = 0.05). In contrast, both IPSS (11 vs 4, p < 0.01) and QOL scores (5 vs 2, p < 0.01) showed significant improvement. Similarly, in the TVM group, the OABSS did not improve significantly between the preoperative and postoperative periods (9 vs 4, p = 0.05), but IPSS (21 vs 4, p < 0.01) and QOL scores (6 vs 3, p < 0.01) did. Given that the difference in OABSS significance was on the borderline, each OABSS item was analyzed separately to assess the possibility that specific symptom domains might have been differentially affected. No significant differences were observed in questions 1, 2, and 4. However, for question 3 (urgency), significant differences were found between preoperative and postoperative scores in both the RSC group (1.0 [0.3–3] vs 0 [0–2.0], p = 0.01) and the TVM group (3.5 [1.0–4.0] vs 0 [0–2.0], p < 0.01).
 |
Table 4 Comparison of Preoperative and Postoperative LUTS Questionnaire Results and PVR in the RSC and TVM Groups |
No significant difference in preoperative PVR was observed between the two groups (p = 0.11), but the RSC group showed significantly lower postoperative PVR compared with the TVM group (p = 0.04; Table 3). PVR improved significantly in both the RSC and TVM groups after surgery (40.0 to 0.00 mL and 50.0 to 0.00 mL, respectively; p < 0.01; Table 4).
The absolute changes and relative reductions in LUTS questionnaire results between the RSC and TVM groups are presented in Table 5. There are no significant differences in absolute changes between the two groups: ΔOABSS (−1 vs −2, p = 0.09), ΔQOL score (−2 vs −3, p = 0.08), and ΔIPSS (−8 vs −14, p = 0.15). Similarly, there were no statistically significant differences in the relative reduction rates of OABSS (23.00% VS 56.35%, P = 0.17), QOL score (50.00 VS 50.00, P = 0.27), and IPSS (63.96% VS 60.00%, P = 0.95) between the two groups.
 |
Table 5 Comparison of the Absolute Changes and Relative Reductions in LUTS Questionnaire Scores Between the RSC and TVM Groups |
Given the aforementioned baseline differences, we performed propensity score matching. Post-matching analysis revealed no significant differences in postoperative questionnaire outcomes: OABSS (3 vs 4, p = 0.16), QOL score (1 vs 3, p = 0.08), and IPSS (4 vs 4, p = 0.49; Table 6). Similarly, no significant difference was observed in postoperative PVR between the two groups after matching (p = 0.09).
 |
Table 6 Comparison of Postoperative LUTS Questionnaire Results and PVR After Propensity Score Matching |
Discussion
RSC and TVM are two established surgical options for the POP repair, and both have yielded high success rates and improvements in urinary function.9,10 However, both procedures are associated with postoperative voiding dysfunctions, particularly de novo SUI. Previous studies comparing the incidence of de novo SUI between RSC and TVM have reported inconsistent findings. One study discovered a lower incidence of de novo SUI within 3 months postoperatively in the RSC group compared with the TVM group (5.4% vs 23.1%, p < 0.05),9 whereas another study reported a higher incidence in the RSC group (33.3% vs 3.3%, p = 0.007), with a non-significant trend toward higher rates based on urodynamic studies (46.7% vs 26.7%, p = 0.16).10 In our study, the incidence of de novo SUI was consistent with previous findings, but no significant difference was observed between the groups (17.6% vs 14.3%, p = 0.74). However, our evaluation was limited to 1 month postoperatively. Longer-term assessment is necessary to capture the full spectrum of postoperative urinary outcomes.
Postoperative voiding function and de novo SUI are considered to be strongly influenced by anatomical changes following surgery. Chia-Hua Chang et al reported that vesicovaginal space dissection can lead to periurethral denervation, resulting in a significant decrease in maximum urethral closure pressure postoperatively in both groups.10 Additionally, correction of urethral kinking and excessive anterior vaginal wall tension following mesh fixation have also been proposed as mechanisms contributing to de novo SUI.11
Urethral kinking is known to contribute to bladder outlet obstruction, and the severity of obstructive symptoms is positively correlated with POP severity.12 Correction of kinking can thus improve voiding function, supported by reduced PVR and improved uroflowmetry parameters after surgery.10
In this study, subjective urinary symptoms were evaluated using validated questionnaires. Both RSC and TVM led to significant improvements in IPSS, QOL scores and question 3 of OABSS indicating better voiding function and enhanced patient satisfaction. However, no significant improvement was observed in the OABSS postoperatively in either group. This finding suggests that overactive bladder symptoms may not be solely attributable to mechanical obstruction secondary to POP but may instead reflect underlying bladder wall remodeling, sensory nerve alterations, or chronic detrusor overactivity, all of which are less likely to resolve immediately following anatomical correction. Previous studies have similarly demonstrated that although prolapse repair can lead to improvements in storage symptoms, complete resolution of overactive bladder symptoms is not consistently achieved, indicating a multifactorial pathophysiology.13–15 Nevertheless, we must acknowledge that the present study did not incorporate objective assessments, such as urodynamic studies; therefore, the proposed mechanisms for persistent overactive bladder symptoms remain hypothetical and should be interpreted with appropriate caution. These findings underscore the necessity of comprehensive preoperative counseling to adequately inform patients of the possibility of urgency-related symptoms persisting despite successful anatomical correction. Furthermore, individualized postoperative follow-up should be considered on the basis of PVR evaluation. In cases where urgency-related symptoms persist, adjunctive pharmacological therapies, such as antimuscarinics or β3-adrenergic agonists, may be an appropriate option to improve long-term functional outcomes.
Importantly in this study, although the RSC group initially had a lower postoperative QOL score and postoperative PVR compared with the TVM group, this difference disappeared after adjustment for baseline characteristics using propensity score matching. Additionally, no significant differences were observed between the two groups in the changes or change rates of LUTS questionnaire scores. These results suggest that both procedures are similarly effective in improving LUTS among women with POP. These findings are consistent with previous comparative studies demonstrating similar outcomes between mesh-based vaginal and minimally invasive sacrocolpopexy procedures in both Japanese and international cohorts.16–18 Therefore, any assumptions regarding the superiority of one technique over the other should be discarded, and the surgical approach for a given case should be selected on the basis of factors such as anatomical considerations, comorbidities, perioperative risks, surgeon expertise, and patient preferences. Although further large-scale studies are needed to validate these findings, our results provide useful insights for clinical decision-making in the surgical management of POP.
Previous studies comparing RSC and TVM have focused mainly on anatomical and perioperative outcomes, but few have systematically evaluated subjective functional outcomes using validated urinary symptom questionnaires. Our findings add to the growing body of evidence highlighting the need to incorporate patient-reported functional outcomes into the assessment of POP surgery. Although TVM has already been banned or withdrawn in the United States and many other countries, TVM is still performed in Japan, and our data provide useful insights into its short-term functional outcomes.
This study has several limitations. First, the retrospective, single-center design of this study may introduce selection bias and limit the generalizability of the findings. Second, the sample size was relatively small, particularly in the TVM group, potentially resulting in insufficient statistical power. Third, postoperative evaluation was limited to 1 month, and because the data collection was retrospective, follow-up data beyond 3–6 months were scarce. Therefore, the long-term course of LUTS and de novo SUI could not be thoroughly assessed. Fourth, urinary function was evaluated solely on the basis of subjective questionnaires without incorporating objective assessments, such as urodynamic studies. Fifth, potential confounding factors, such as pelvic floor dysfunction and perioperative management strategies, were not fully accounted for. Nevertheless, a notable strength of this study is that all surgeries were performed by a single surgeon specializing in urogynecology, ensuring procedural consistency. Future studies should be prospective and multicenter, involving larger cohorts with longer follow-up periods and incorporating objective evaluations to validate and expand upon these findings. Such studies will help confirm our present results and pave the way for establishing evidence-based strategies for individualized postoperative care.
Conclusion
Both RSC and TVM were associated with improvement in LUTS in women with POP. After adjusting for baseline differences, the two groups did not differ significantly in postoperative LUTS questionnaires and PVR. These findings suggest that both approaches may offer comparable functional outcomes, and that surgical decisions should be taken by considering patient characteristics, perioperative risks, and surgeon experience. It is also important to note that surgical experience can affect the outcomes of advanced prolapse surgery.
Acknowledgments
We thank the staff of Shizuoka Saiseikai General Hospital for their support and the patients who participated in this study. We thank enago (www.enago.jp) for English language editing.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Barber MD, Maher C. Epidemiology and outcome assessment of pelvic organ prolapse. Int Urogynecol J. 2013;24(11):1783–1790. doi:10.1007/s00192-013-2169-9
2. Schulten SFM, Claas-Quax MJ, Weemhoff M, et al. Risk factors for primary pelvic organ prolapse and prolapse recurrence: an updated systematic review and meta-analysis. Am J Obstet Gynecol. 2022;227(2):192–208. doi:10.1016/j.ajog.2022.04.046
3. Vergeldt TFM, Weemhoff M, IntHout J, et al. Risk factors for pelvic organ prolapse and its recurrence: a systematic review. Int Urogynecol J. 2015;26(11):1559–1573. doi:10.1007/s00192-015-2695-8
4. Raju R, Linder BJ. Evaluation and management of pelvic organ prolapse. Mayo Clin Proc. 2021;96(12):3122–3129. doi:10.1016/j.mayocp.2021.09.005
5. Robinson MO, Linder BJ. Evaluation and treatment of pelvic organ prolapse. Minerva Med. 2023;114(4):516–528. doi:10.23736/S0026-4806.22.08396-3
6. Barski D, Deng DY. Management of mesh complications after SUI and POP repair: review and analysis of the current literature. Biomed Res Int. 2015;2015:831285. doi:10.1155/2015/831285
7. Guidance Nice. Urinary incontinence and pelvic organ prolapse in women: management: © NICE (2019) Urinary incontinence and pelvic organ prolapse in women: management. BJU Int. 2019;123(5):777–803. doi:10.1111/bju.14763
8. Tran H, Chung DE. Incidence and management of de novo lower urinary tract symptoms after pelvic organ prolapse repair. Curr Urol Rep. 2017;18(11):87. doi:10.1007/s11934-017-0732-5
9. Kusuda M, Kagami K, Takahashi I, Nozaki T, Sakamoto I. Comparison of transvaginal mesh surgery and robot-assisted sacrocolpopexy for pelvic organ prolapse. BMC Surg. 2022;22(1):268. doi:10.1186/s12893-022-01702-z
10. Chang CH, Su TH, Lau HH. The changes in bladder function and symptoms after robot-assisted sacrocolpopexy and transvaginal mesh surgery for pelvic organ prolapse. Taiwan J Obstet Gynecol. 2024;63(1):68–72. doi:10.1016/j.tjog.2023.05.016
11. Nomura Y, Okada Y, Hiramatsu A, Matsubara E, Kato K, Yoshimura Y. A new method of adjusting mesh tension using cystoscopy during laparoscopic sacrocolpopexy. Int Urogynecol J. 2021;32(11):3089–3093. doi:10.1007/s00192-021-04791-1
12. Kowalski JT, Wiseman JB, Smith AR, et al. Natural history of lower urinary tract symptoms in treatment-seeking women with pelvic organ prolapse; the symptoms of lower urinary tract dysfunction research network (LURN). Am J Obstet Gynecol. 2022;227(6):875.e1–875.e12. doi:10.1016/j.ajog.2022.07.038
13. Abrams M, Sears S, Wherley S, Rhodes S, Mangel J, Sheyn D. Resolution of overactive bladder symptoms after anterior and apical prolapse repair. Urogynecology. 2025;31(2):147–153. doi:10.1097/SPV.0000000000001502
14. Karjalainen PK, Tolppanen AM, Mattsson NK, Wihersaari OA, Jalkanen JT, Nieminen K. Pelvic organ prolapse surgery and overactive bladder symptoms—a population-based cohort (FINPOP). Inter Urogynecol J. 2022;33(1):95–105. doi:10.1007/s00192-021-04920-w
15. Kwon J, Kim DY, Cho KJ, et al. Pathophysiology of overactive bladder and pharmacologic treatments including β3-adrenoceptor agonists -basic research perspectives. Int Neurourol J. 2024;28(Suppl 1):12–33. doi:10.5213/inj.2448002.001
16. Obinata D, Sugihara T, Yasunaga H, et al. Tension-free vaginal mesh surgery versus laparoscopic sacrocolpopexy for pelvic organ prolapse: analysis of perioperative outcomes using a Japanese national inpatient database. Int J Urol. 2018;25(7):655–659. doi:10.1111/iju.13587
17. Menefee SA, Richter HE, Myers D, et al. Apical suspension repair for vaginal vault prolapse: a randomized clinical trial. JAMA Surg. 2024;159(8):845–855. doi:10.1001/jamasurg.2024.1206
18. Poutakidis G, Falconer C, Falconer C, et al. Pelvic organ prolapse repair using robotic assisted sacral hysterocolpopexy vs vaginal surgery with the Uphold™ system: 1-year clinical outcomes. Int Urogynecol J. 2025;36(3):585–597. doi:10.1007/s00192-024-06017-6
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.