Back to Journals » Local and Regional Anesthesia » Volume 14
Short Communication: Lumbar Plexus Block versus Suprainguinal Fascia Iliaca Block to Provide Analgesia Following Hip and Femur Surgery in Pediatric-Aged Patients – An Analysis of a Case Series
Authors DeLong L ![]() , Krishna S, Roth C
, Krishna S, Roth C ![]() , Veneziano G
, Veneziano G ![]() , Arce Villalobos M, Klingele K
, Arce Villalobos M, Klingele K ![]() , Tobias JD
, Tobias JD ![]()
Received 20 August 2021
Accepted for publication 22 September 2021
Published 19 October 2021 Volume 2021:14 Pages 139—144
DOI https://doi.org/10.2147/LRA.S334561
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Stefan Wirz
Lauren DeLong,1 Senthil Krishna,2,3 Catherine Roth,2 Giorgio Veneziano,2,3 Mauricio Arce Villalobos,2,3 Kevin Klingele,4 Joseph D Tobias2,3
1Heritage College of Osteopathic Medicine - Athens Campus (Athens, Ohio) and Ohio University, Athens, OH, USA; 2Department of Anesthesiology & Pain Medicine, Nationwide Children’s Hospital, Columbus, OH, USA; 3Department of Anesthesiology & Pain Medicine, The Ohio State University College of Medicine, Columbus, OH, USA; 4Department of Orthopedic Surgery, Nationwide Children’s Hospital and The Ohio State University College of Medicine, Columbus, OH, USA
Correspondence: Joseph D Tobias
Department of Anesthesiology & Pain Medicine, Nationwide Children’s Hospital, Columbus, OH, USA
Email [email protected]
Introduction: For surgical procedures involving the hip and femur, various regional anesthetic techniques may be used to provide analgesia. Although there has been an increase in the use of lumbar plexus block (LPB), the technique may be time consuming and associated with complications. Suprainguinal fascia iliaca compartment block (FICB) is a potentially easier and safer alternative. The current study prospectively compares LPB with suprainguinal FICB.
Methods: This prospective, double-blinded, randomized, study included patients undergoing elective orthopedic procedures of the hip and/or femur. All study patients received general anesthesia with randomization to either an LPB or suprainguinal FICB using 0.5% ropivacaine with epinephrine and dexamethasone. Postoperative pain control was achieved with intravenous hydromorphone delivered by patient-controlled analgesia with scheduled acetaminophen and ketorolac. Outcome data included time to perform the block, perioperative opioid consumption, postoperative pain scores (VAS) and hospital length of stay.
Results: The study cohort included 15 patients between the ages of 7 and 16 years (LPB N = 7, FICB N = 8). The median block time was 6 minutes (IQR: 4.11) for the LPB group and 3 minutes (IQR: 3.6) for the FICB group (p = 0.107). Median postoperative pain scores were 4 (IQR: 0.6) for the LPB group and 2 (IQR: 0.5) for the FICB group (p = 0.032). There were no differences in the intraoperative or postoperative opioid and NSAID use between the two groups.
Discussion: The suprainguinal FICB provides analgesia that is at least as effective as a LPB following hip and femur surgery. Time to perform the block was shorter with the FICB due to the supine patient position and limited needle trajectory. Although we noted no adverse effects, the superficial needle trajectory of the FICB offers a less invasive approach and the potential for decreased risks of adverse effects.
Keywords: orthopedic surgery, postoperative analgesia, lumbar plexus block, suprainguinal fascia iliaca block
Introduction
Regional anesthetic techniques have been shown to provide effective postoperative analgesia, reduce opioid consumption, decrease the time to discharge, and minimize the exposure to general anesthetic agents in children undergoing orthopedic procedures.1–4 With advances in pediatric regional techniques, neuraxial blocks are being replaced with peripheral nerve blockade such as lumbar plexus block (LPB) to achieve a selective unilateral blockade for procedures involving the hip and thigh.5–8 However, placement of a LPB requires lateral or prone positioning and a deep needle trajectory to contact the lumbar plexus in the paravertebral space, which may be associated with complications such as needle advancement into the peritoneum, retroperitoneal hematoma, and renal injury. Occasional local anesthetic spread into the epidural space may also negate some of the benefits of selective peripheral nerve blockade.9–12
The suprainguinal fascia iliaca compartment block (FICB) is a more recently described technique to anesthetize the femoral, lateral femoral cutaneous, and obturator nerves in a superficial fascial plane for postoperative analgesia in adult patients after hip arthroplasty.13–15 To our knowledge, there are no studies comparing LPB to suprainguinal FICB for pain management after orthopedic procedures involving the hip and femur in the pediatric population. The current study prospectively compared the time required for placement of the block, perioperative opioid consumption, postoperative pain scores, and hospital length of stay to determine the effectiveness of these blocks in providing analgesia following hip and femur surgery in the children.
Methods
The study was approved by the Institutional Review Board of Nationwide Children’s Hospital (Columbus, Ohio) and conducted in accordance with the Declaration of Helsinki. Patients aged 2–18 years, ASA physical status I–III, scheduled for orthopedic procedures involving the hip, femur, and upper thigh were recruited. Informed written consent was obtained from a parent or guardian. Additionally, assent was obtained from patients ≥9 years of age were obtained. The study was registered at ClinicalTrials.gov (NCT03746951). Exclusion criteria included opioid use within the 3 months prior to surgery, history of opioid abuse or dependence, pre-existing motor or sensory deficits, and patient or parent refusal. Using data from similar comparative studies and for the proposed t-test to have 80% power to confirm a statistically significant difference at 95% confidence level, at least 29 patients were needed to be enrolled in each group. A sample size of 70 patients was determined prior to the start of the study to account for any dropouts or missing data.
After consent was obtained, the patients were randomized into two groups (LPB or suprainguinal FICB) using a 10-block simple randomization service. Other than the type of the regional block, anesthetic and perioperative care was standardized in all patients. Patients who required anxiolysis received premedication with either oral midazolam (0.3–0.5 mg/kg, maximum 20 mg) 30 minutes before the surgery or intravenous midazolam (0.05 mg/kg, maximum 2 mg) prior to transport to the operating room. All patients were monitored using standard American Society of Anesthesiologists’ monitors. Anesthetic induction was achieved with 70% nitrous oxide in oxygen and sevoflurane or intravenous propofol (2–3 mg/kg). Once the patient lost consciousness, fentanyl (2 ug/kg) was administered intravenously and the trachea was intubated. If needed, endotracheal intubation was facilitated by the administration of intravenous succinylcholine (1–2 mg/kg).
After securing the airway, the primary anesthesia team stepped out of the operating room and the study team headed by an attending anesthesiologist performed either the LPB or suprainguinal FICB with 3 mg/kg (0.6 mL/kg) of 0.5% ropivacaine with 1:200,000 epinephrine and dexamethasone 0.2 mg/mL (maximum volume of 30 mL). At the completion of the regional nerve block, two dressings were placed over the actual needle insertion site and the imaginary needle insertion site where the other block (LPB or FICB) would have been performed. The time required to complete the block was measured from the start of the regional block time-out until the patient was repositioned for the surgical procedure. The care was resumed by the primary anesthesia team following surgical positioning.
Anesthesia was maintained with 1–2 MAC of sevoflurane in 50% oxygen and air. Intravenous rocuronium 0.6–1 mg/kg was administered to maintain neuromuscular blockade after completion of the block. Additional bolus doses of intravenous fentanyl (1 ug/kg) were administered intraoperatively for analgesia as needed to maintain the heart rate and blood pressure within 20% of baseline. In addition, intravenous dexamethasone (0.1–0.15 mg/kg up to 8 mg) and ondansetron (0.1–0.15 mg/kg up to 4 mg) were administered prophylactically for the management of postoperative nausea and vomiting. At the conclusion of the surgical procedure, residual neuromuscular blockade was reversed with intravenous sugammadex (2 mg/kg) boluses as needed prior to tracheal extubation.
Postoperative analgesia was achieved with intravenous hydromorphone 0.02 mg/kg demand only delivered by patient-controlled or nurse-controlled analgesia with a lockout interval of 12 minutes. Patients also received intravenous acetaminophen 15 mg/kg every 6 hours and intravenous ketorolac 0.5 mg/kg every 6 hours during the 48-hour study period. The first dose of these two agents was administered in the operating room at the completion of the surgical procedure. Postoperatively, once patient was tolerating oral feeds, intravenous analgesics were replaced with oral oxycodone/hydrocodone as needed (0.1 mg/kg to a maximum of 5 mg every 4 hours) in addition to around-the-clock oral acetaminophen (10 mg/kg) and oral ibuprofen (10 mg/kg).
The primary objective was to measure the total block procedure time (in minutes and seconds) while the secondary objectives were to determine the opioid consumption in the first 48 postoperative hours, median pain scores during the first 48 postoperative hours using a visual analogue score (VAS), and the hospital length of stay. Additionally, patient demographics as well as surgical parameters were collected. Continuous outcomes were compared between the two groups using 2-sample t-test or rank-sum tests according to the normality of the distribution and confirmed with the Shapiro–Wilk test. Categorical outcomes were characterized using Chi-square or Fisher’s exact tests according to cell size.
Results
Patients were enrolled from April 2019 through February 2021. The study cohort included 15 patients, 9 male and 6 female, ranging in age from 7 to 16 years undergoing elective hip and femur surgery. Seven patients were randomized to receive a LPB and 8 received a suprainguinal FICB. The groups were similar with regard to age, gender, weight, ASA physical status, and body mass index (Table 1). Intraoperative data listed in Table 2 include the dose of ropivacaine, the time to perform the block, credentials of the person performing the block, surgery time, post-anesthesia care unit (PACU) length of stay (LOS), hospital LOS, and postoperative pain scores. The time required to perform the LPB block was longer compared to the suprainguinal FICB group (median 6 minutes versus 3 minutes); however, the difference in block time was not statistically significant (p = 0.107). There were no statistically significant differences in the surgery time and PACU length of stay between the groups. The median hospital length of stay for the LPB group was 2.19 days compared to 1.25 days for the suprainguinal FICB group (p = 0.001). Pain scores in the PACU were similar between the two groups (p = 0.47). Pain scores were lower postoperatively in the suprainguinal group compared to the LPB group (median pain score of 2 versus 4, p = 0.032). The opioid and NSAID use intraoperatively, in the PACU, and postoperatively are outlined in Table 3. There were no statistically significant differences in the medications given during surgery, in the PACU, and postoperatively.
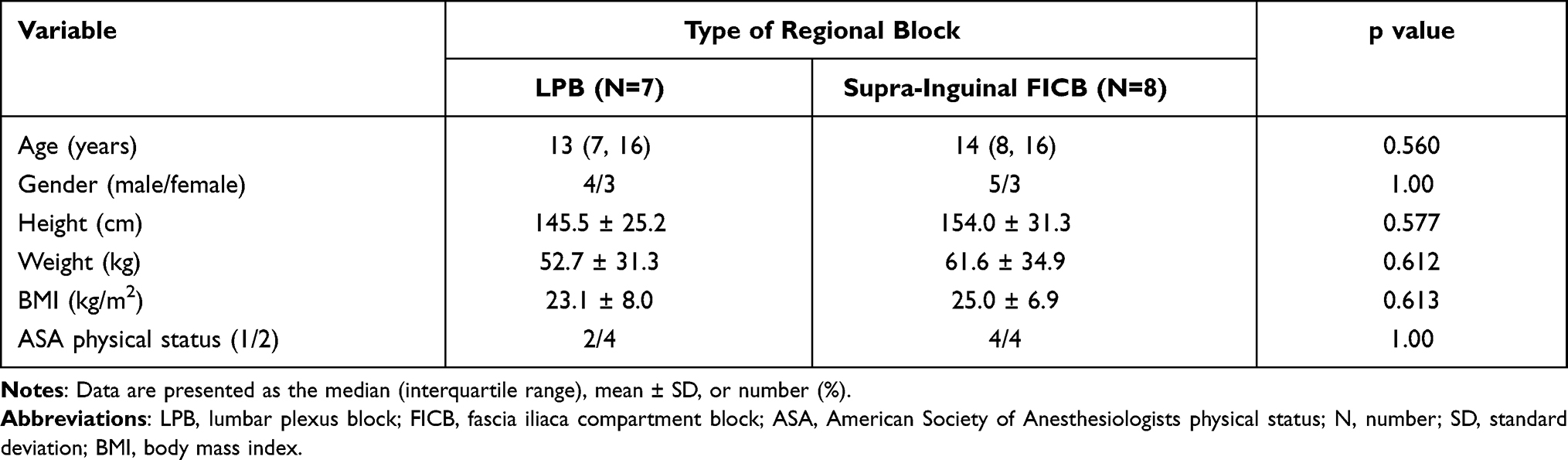 |
Table 1 Demographic Data of the Study Cohorts |
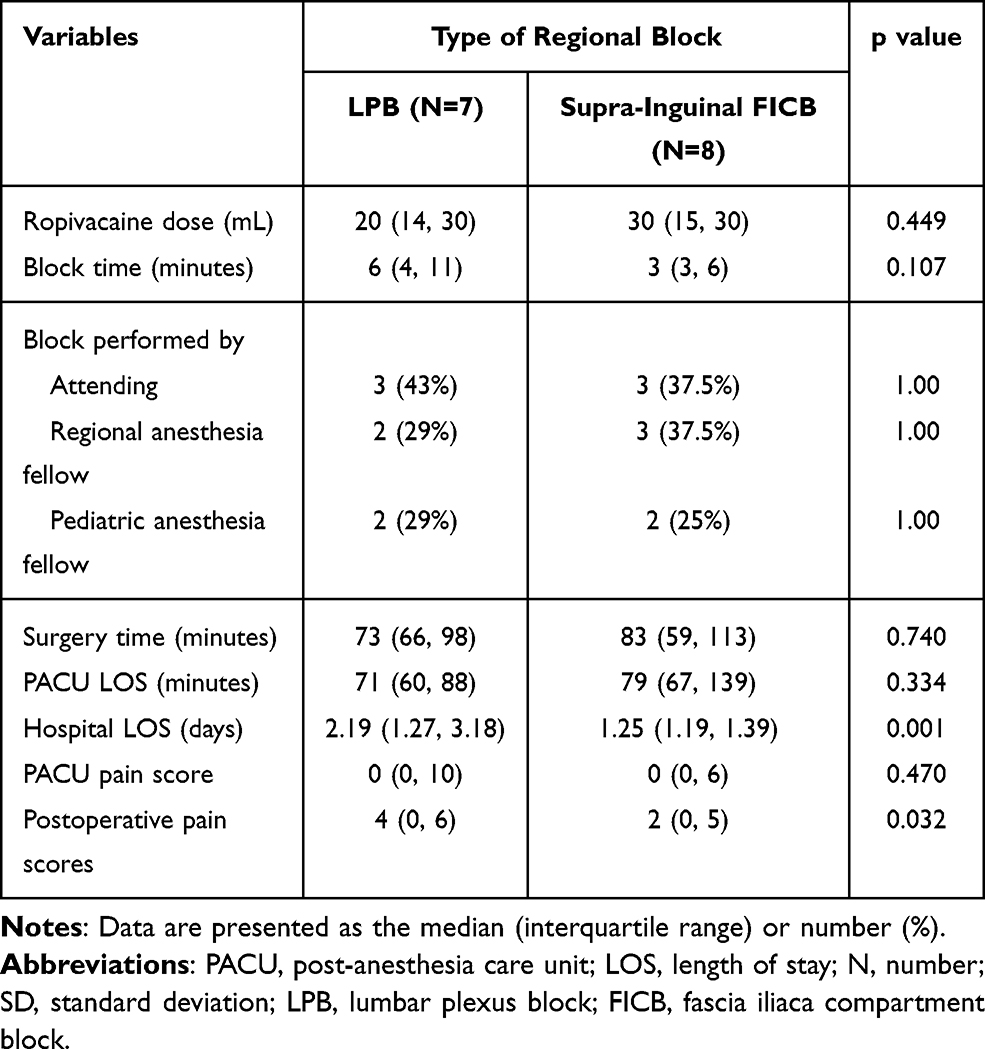 |
Table 2 Outcomes According to Type of Regional Block |
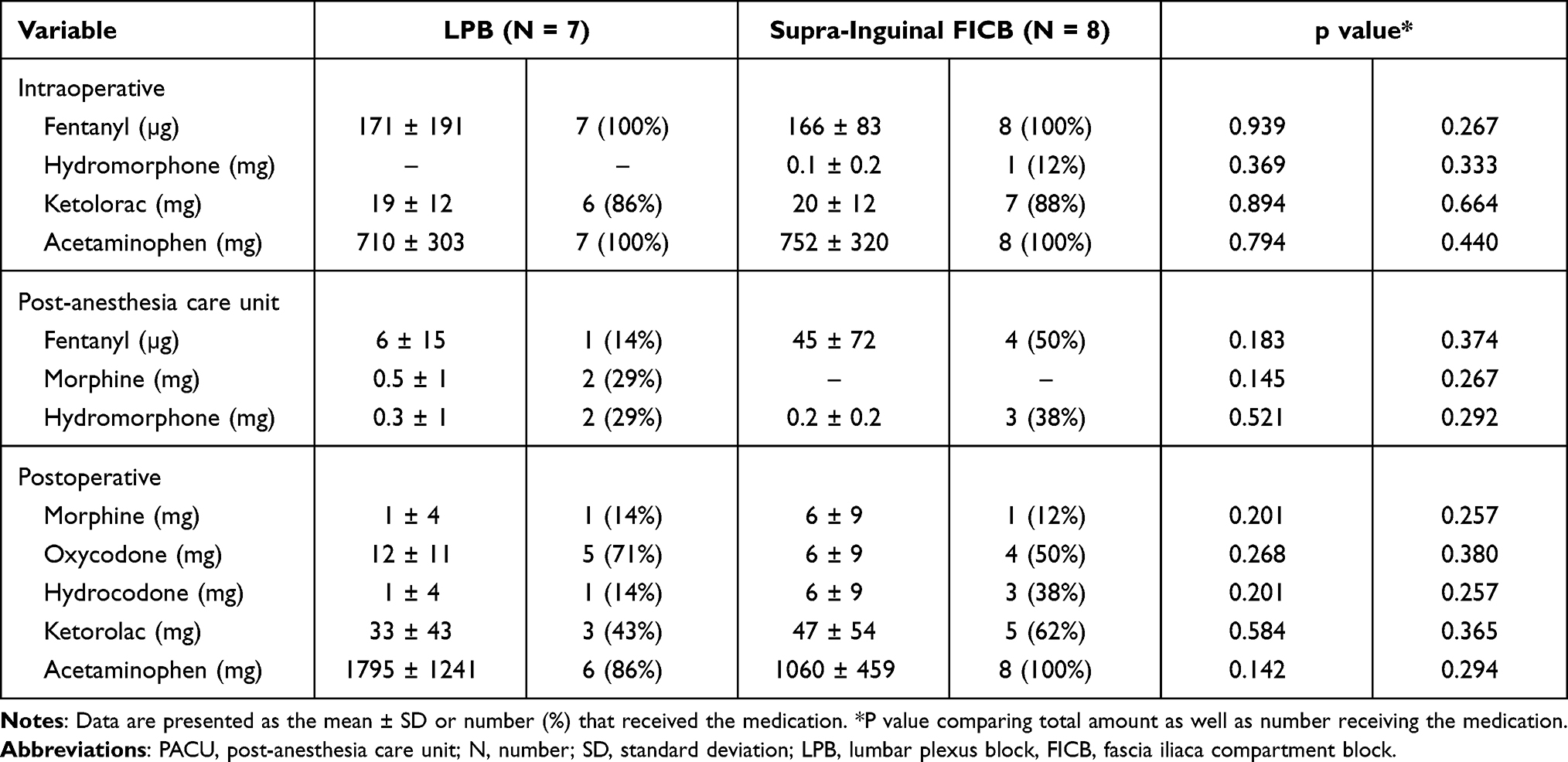 |
Table 3 Medications During Surgery, in the PACU, and During the Initial 48 Postoperative Hours |
Discussion
Orthopedic procedures involving the hip, femur, and upper thigh in pediatric patients are associated with moderate-to-severe postoperative pain.14,16 As in adults, regional anesthetic techniques are frequently used to supplement general anesthesia and provide postoperative analgesia following major pediatric orthopedic surgery involving the hip, femur, and upper thigh.3,17 These regional anesthetic techniques have gained favor in the pediatric population as they have been shown to decrease intraoperative volatile anesthetic requirements, decrease opioid consumption postoperatively, and reduce the time to discharge.1–3 Minimizing opioid consumption also improves the postoperative course and decreases opioid-related adverse effects including nausea and vomiting, confusion, constipation, respiratory depression, and sedation.3,17–19
Selective regional blockade such as LPB has gained popularity for unilateral procedures of the hip and femur.3,9 Although LPB provides reliable analgesia, the procedure requires lateral positioning and can be technically challenging, requiring use of a nerve stimulator with identification of the lumbar plexus in the paravertebral space.3,9,10 Given the deeper trajectory of the needle, potential complications may include bowel puncture, retroperitoneal hematoma, and renal injury.9,10,17 Additionally, spread of the local anesthetic agent into the epidural space may result in bilateral lower extremity blockade.8,13,19,20 Ultrasound-guided suprainguinal FICB has been shown to provide effective postoperative analgesia for total hip arthroplasty.15,21 The superficial approach makes the procedure relatively easier, the block can be placed with the patient positioned supine, and with use of ultrasound-guidance the potential for adverse effects is limited.21 While the analgesic effects of the LPB and the suprainguinal FICB have been compared in adult patients, the current study is the first to compare these two techniques in the pediatric-aged patient.13,22
In the current study, we noted that the suprainguinal FICB provided analgesia that was at least as effective as the LBP in terms of both pain scores and postoperative analgesic needs. Although pain scores in the PACU were equivalent between the two groups, the postoperative pain scores were lower in patients who received a suprainguinal FICB. There was no need to move the position from the supine position. Although it did not reach statistical significance given the limited size of our study cohort, decreased time was required to perform the suprainguinal FICB. As time to perform the block included return to the supine position for these surgical procedures, shorter block times for the LBP would have been noted had the surgery been performed in the lateral position.
There were several limitations in our study, the primary one being the small sample size. Study recruitment and sample size were impacted by the COVID-19 pandemic limiting elective surgical procedures and enrollment of patients in our study. Once the impact of the COVID-19 pandemic had waned, our surgical colleagues were impressed with the efficacy of the suprainguinal FICB and the efficacy of block placement. Given ethical concerns as we believe that the adverse effect profile of the ultrasound-guided, superficial suprainguinal FICB is limited, we chose to close enrollment and proceed with the suprainguinal block as our standard practice. The other limitation was the occasional study protocol deviations in terms of the use of the opioids and NSAIDs in study cohort which may have impacted postoperative pain scores and analgesic requirements.
In conclusion, the suprainguinal FICB proved to be at least as effective as a LPB in providing analgesia following hip, femur, and upper thigh surgery in children and adolescents. In addition, we noted the suprainguinal block to be more efficient and easier thereby decreasing block time. As a superficial technique, ultrasound-guidance is feasible which may limit adverse effects when compared to the deeper needle trajectory required for a LPB. Due to the small sample size and variability in the analgesic use in the current study population, further investigation is necessary to further support our conclusions.
Data Sharing Statement
Requests for individual deidentified participant data will be reviewed on an individual basis and information provided as appropriate. All data will be maintained for at least 3 years from the date of publication. Inquiries may be sent to the corresponding author via e-mail ([email protected]).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wong J, Marshall S, Chung F, Sinclair D, Song D, Tong D. Spainal anesthesia improves the early recovery profile of patients undergoing ambulatory knee arthroscopy. Can J Anaesth. 2001;48(4):369–374. doi:10.1007/BF03014965
2. Rappaport B, Mellon RD, Simone A, Woodcock J. Defining safe use of anesthesia in children. N Engl J Med. 2011;364:1387–1390.
3. Ross AK, Eck JB, Tobias JD. Pediatric regional anesthesia: beyond the caudal. Anesth Analg. 2000;91:16–26.
4. Schloss B, Bhalla T, Klingele K, Phillips D, Prestwich B, Tobias JD. A retrospective review of femoral nerve block for postoperative analgesia after knee surgery in the pediatric population. J Pediatr Orthop. 2014;34:459–461.
5. Schloss B, Martin D, Tripi J, Klingele K, Tobias JD. Caudal epidural blockade for major orthopedic hip surgery in adolescents. Saudi J Anaesth. 2015;9:128–131.
6. Dadure C, Raux O, Gaudard P, et al. Continuous psoas compartment blocks after major orthopedic surgery in children: a prospective computed tomographic scan and clinical studies. Anesth Analg. 2004;98:623–628.
7. Manion SC, Tobias JD. Lumbar plexus blockade in children. Amer J Pain Manage. 2005;15:120–126.
8. Villalobos MA, Veneziano G, Miller R, et al. Evaluation of postoperative analgesia in pediatric patients after hip surgery: lumbar plexus block versus caudal epidural analgesia. Loco Reg Anesth. 2019;12:997–1001.
9. Awad IT, Duggan EM. Posterior lumbar plexus block: anatomy, approaches, and techniques. Reg Anesth Pain Med. 2005;30:143–149.
10. Kirchmair L, Entner J, Wissel J, Moriggl B, Kapral S, Mitterschiffthaler G. A study of the paravertebral anatomy for ultrasound-guided posterior lumbar plexus block. Anesth Analg. 2001;93:477–481.
11. Joshi G, Gandhi K, Shah N, Gadsen J, Corman SL. Peripheral nerve blocks in the management of postoperative pain: challenges and opportunities. J Clin Anesth. 2016;35:524–529.
12. Dalens B, Tanguy A, Vanneuville G. Lumbar plexus block in children: a comparison of two procedures in 50 patients. Anesth Analg. 1988;67:750–758.
13. Badiola I, Liu J, Huang S, Kelly
14. Eastburn E, Hernandez M, Boretsky K. Technical success of the ultrasound-guided supra-inguinal fascia iliaca compartment block in older children and adolescents for hip arthroscopy. Pediatr Anesth. 2017;27:1120–1124.
15. Desmet M, Vermeylen K, Van Herreweghe I, et al. A longitudinal supra-inguinal fascia iliaca compartment block reduces morphine consumption after total hip arthroplasty. Reg Anesth Pain Med. 2017;42:327–333.
16. Shamim R, Prasad G, Bais PS, et al. Ultrasound-guided suprainguinal fascia iliaca compartment block in patients undergoing hip and femur surgeries: a retrospective analysis. Anesth Essays Res. 2020;14:525–530.
17. Murray JM, Derbyshire S, Shields MO. Lower limb blocks. Anaesthesia. 2010;65:57–66.
18. Koehler RM, Okoroafor UC, Cannada LK. A systematic review of opioid use after extremity trauma in orthopedic surgery. Injury. 2018;49:1003–1007. doi:10.1016/j.injury.2018.04.003
19. Gadsden JC, Lindemuth DM, Hadzic A, Xu D, Somasundarum L, Flisinski K. Lumbar plexus block using high-pressure injection leads to contralateral and epidural spread. Anesthesiology. 2008;109:683–688.
20. Ivani G, Mossetti V. Pediatric regional anesthesia. Minerva Anesthesiol. 2009;75:577–583.
21. Hebbard P, Ivanusic J, Sha S. Ultrasound-guided supra-inguinal fascia iliaca block: a cadaveric evaluation of a novel approach. Anaesthesia. 2011;66:300–305.
22. Bravo D, Layera S, Aliste J, et al. Lumbar plexus block versus suprainguinal fascia iliaca block for total hip arthroplasty: a single-blinded, randomized trial. J Clin Anesth. 2020;66:1–6.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.