Back to Journals » Open Access Emergency Medicine » Volume 18
Shock Index versus Systolic Blood Pressure for Mortality Prediction in Traumatic Hemorrhage: A Comparative Prognostic Evaluation in a Middle-Income Country
Authors Wogu AF ![]() , Xiao M, Barnhart DA, Centi S, Lategan H, Oosthuizen G
, Xiao M, Barnhart DA, Centi S, Lategan H, Oosthuizen G ![]() , Wylie C
, Wylie C ![]() , de Vries S, Verster J
, de Vries S, Verster J ![]() , Stassen W, Sammel MD, Schauer SG, Dixon JM, Mould-Millman NK
, Stassen W, Sammel MD, Schauer SG, Dixon JM, Mould-Millman NK ![]()
Received 18 April 2026
Accepted for publication 27 June 2026
Published 10 July 2026 Volume 2026:18 618018
DOI https://doi.org/10.2147/OAEM.S618018
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Charles V Pollack
Adane F Wogu,1 Mengli Xiao,1 Dale A Barnhart,2 Sophia Centi,2 Hendrick Lategan,3 George Oosthuizen,3 Craig Wylie,4 Shaheem de Vries,5 Janette Verster,6 Willem Stassen,7 Mary D Sammel,1 Steven G Schauer,8 Julia M Dixon,2 Nee-Kofi Mould-Millman2
1Department of Biostatistics and Informatics, Colorado School of Public Health, Anschutz Medical Campus, Aurora, CO, USA; 2Department of Emergency Medicine, School of Medicine, University of Colorado Anschutz Medical Campus, Aurora, CO, USA; 3Division of Surgery, Department of Surgical Sciences, Stellenbosch University, Stellenbosch, Cape Town, South Africa; 4Emergency Medical Services, Western Cape Government Health, Bellville, Cape Town, South Africa; 5Collaborative for Emergency Care in Africa, Cape Town, South Africa; 6Division of Forensic Medicine, Department of Pathology, Faculty of Medicine and Health Science, Stellenbosch University and Tygerberg Forensic Pathology Service, Stellenbosch, Cape Town, South Africa; 7Division of Emergency Medicine, Department of Family, Community and Emergency Care, University of Cape Town, Cape Town, South Africa; 8US Army Institute of Surgical Research, JBSA Ft. Sam Houston, San Antonio, TX, USA
Correspondence: Adane F Wogu, Colorado School of Public Health, Department of Biostatistics and Informatics, 13001 E. 17th Place, Mail Stop B119, Aurora, CO, 80045, USA, Email [email protected]
Purpose: This study aims to evaluate and compare the prognostic performance of shock index (SI) and systolic blood pressure (SBP) for predicting mortality among trauma patients at risk of hemorrhage in South Africa, a high-trauma burden setting with resource constraints.
Patients and Methods: This is a secondary analysis of data from the EpiC study, a prospective, multicenter observational investigation of trauma patients in the Western Cape, South Africa. Adult patients with blunt or penetrating injuries and no significant head injury were included. The predictor variables–SI and SBP at facility arrival–and the outcome (30-day mortality) were analyzed through a sequential analytical framework. Segmented logistic regressions identified inflection points; ROC analyses with Youden’s J statistic determined optimal thresholds. Model comparisons employed DeLong’s test, calibration plots, Brier scores, and decision curve analysis. Subgroup analyses were conducted by injury mechanism and severity.
Results: Among 3609 patients, 6.1% died within 30 days. SI demonstrated an inflection point at 0.69 and SBP at 82 mmHg. ROC analysis yielded similar AUCs of 0.62 (SI) and 0.60 (SBP) (p=0.418). However, SI showed superior calibration (Brier score: 0.054 vs 0.058), a higher positive likelihood ratio (2.70 vs 2.01; p< 0.001), and greater net benefit across a broader range of predicted-risk thresholds on decision curve analysis. The optimal SI cutoff of ≥ 1.21 yielded 85.1% specificity and 40.3% sensitivity.
Conclusion: Both SI and SBP demonstrated only modest discrimination for 30-day mortality, reflecting the inherent limitations of single vital-sign predictors in complex trauma populations. Within these constraints, SI showed marginally better calibration and rule-in performance than SBP; however, neither predictor alone is sufficient for definitive mortality risk prediction. An SI threshold of ≥ 1.21 may serve as a practical screening tool to flag high-risk patients warranting closer monitoring or escalated care, particularly in resource-limited settings where laboratory and imaging resources are constrained.
Keywords: shock index, systolic blood pressure, traumatic hemorrhage, low- and middle-income countries
Introduction
Injuries claim over 4.4 million lives annually, with traumatic brain injury and uncontrolled bleeding being the leading causes of death worldwide in both civilian and military settings.1,2 Trauma-related mortality and morbidity are disproportionately higher in low- and middle-income countries (LMIC) due to delayed transport, inadequate surgical care, and treatment gaps, amongst other reasons.3–6 Traumatic hemorrhage remains the most common and most preventable cause of early post-injury death, peaking within three hours—a pattern unchanged for decades despite advances in trauma care.7–12 Systolic blood pressure (SBP) is widely used for triage in trauma, yet its reliability is limited because compensatory mechanisms can maintain normal SBP despite substantial hemorrhage.13 The Shock Index (SI)—the ratio of heart rate (HR) to SBP—was introduced by Allgöwer and Burri14 in 1967 as a simple clinical tool to identify early circulatory compromise when SBP alone remains deceptively normal. SI leverages the inverse relationship between increasing tachycardia and falling arterial pressure during progressive blood loss.
A recent international systematic review—including studies from the US, Europe, Asia, and Australia but none from Africa—found that SI had limited value as a standalone predictor of MT and was inaccurate for predicting mortality in adult trauma patients.15 Across the broader literature, findings on SI and SBP predictive performance are highly inconsistent, shaped by heterogeneity in study populations (injury severity, mechanism, age, comorbidities), timing of measurement (prehospital vs emergency department), choice of cutoffs, and resource availability.16–20 Wu et al in their most recent study reported that dynamic changes in shock index, termed delta SI, improved prediction of massive transfusion compared with single SBP or SI values.18
In LMICs—where prehospital delays, limited blood-product availability, and constrained diagnostic capacity are common—there is great potential value of simple physiology-based triage tools; however, empirical research rigorously evaluating the predictive performance of SI and SBP in these settings remains critically sparse, leaving a substantial evidence gap. Few studies have evaluated SI or SBP in LMIC settings, and only a few have been conducted in sub-Saharan Africa, reporting generally limited predictive accuracy for SI and its derivatives.17,20–22 Importantly, prior studies have seldom provided head-to-head comparisons of SI and SBP within the same LMIC trauma populations, nor have they systematically examined nonlinear risk–outcome relationships or clinically actionable thresholds tailored to resource-constrained settings.
To address these gaps, we conducted a comparative evaluation of SI and SBP for mortality prediction in an LMIC trauma cohort, with emphasis on (i) directly contrasting their predictive performance, (ii) characterizing potential nonlinear associations and inflection points, and (iii) identifying pragmatic decision thresholds relevant to low-resource clinical environments. Findings from this study hold potential to improve trauma care in resource-constrained trauma settings.
Materials and Methods
Study Design and Patient Population
This study is a secondary analysis of data from the Epidemiology and Outcomes of Prolonged Trauma Care (EpiC) study, a prospective, multicenter observational investigation conducted in the Western Cape Province of South Africa.23 The EpiC study was designed to advance the understanding of trauma epidemiology and outcomes, particularly in resource-limited settings where trauma burden is high and there are barriers to intensive and definitive trauma care. The study encompasses 12 Western Cape Government public health agencies, including six hospitals (spanning primary, secondary, and tertiary levels), four EMS ambulance bases, and two forensic pathology laboratories. This infrastructure enables the creation of South Africa’s first multi-institutional trauma database, prospectively linking prehospital, in-hospital, and mortuary data from the point of injury through to final disposition.
Eligible trauma patients were identified through systematic review of EMS, hospital, and mortuary records. Medical records were carefully screened to confirm eligibility and subsequently entered into REDCap, with cases followed until discharge or death. Detailed data abstraction was performed, and records were probabilistically linked across sources. Rigorous data cleaning and verification ensured analytic accuracy.23 For this secondary analysis, we included adult patients (aged ≥18 years) at risk for hemorrhage, defined as experiencing a blunt, penetrating, or mixed force type and at least one of: Sequential Organ Failure Assessment (SOFA) cardiovascular score ≥3, initial lactate ≥4.0, base deficit ≥6, pH ≤7.2, circulatory diagnoses (shock, hemorrhagic hypovolemia, cardiac tamponade, cardiac arrest), or hemorrhage as primary/secondary mechanism of death. We further excluded those with moderate or greater head injuries (Abbreviated Injury Scale [AIS] head ≥2) to isolate hemorrhage-related shock physiology without confounding from traumatic brain injury.24
The Western Cape setting—marked by large trauma caseloads, high incidence of penetrating injury, prolonged prehospital times, and limited access to intensive care and definitive therapies—mirrors challenges faced by many LMICs, making this cohort valuable for understanding trauma care in high-burden environments.25,26 The study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.27 Ethics approval, with a waiver of informed consent, was obtained from the Stellenbosch University Health Research Ethics Committee (Project ID 14866; Ref. N20/03/036), with oversight ceded by the University of Colorado (Protocol 20–2176) and concurrence from the Defense Health Agency Office of Human Research Oversight (OHRO Log E01863.1x).
Statistical Analysis
Primary predictor variables were SI and SBP, obtained from the first set of vital signs recorded on facility arrival using routinely calibrated automated monitors and standardized data-entry procedures across all sites. Facility arrival was selected as prior work with this study cohort found about one-half of all patients arrive directly at the emergency center and thus were missing prehospital vital signs.28 The primary outcome was all-cause mortality within 30 days of injury, analyzed as a binary variable to capture acute trauma-related mortality. The literature shows no consensus on mortality time points for evaluating SI or SBP, often reporting in-hospital or overall mortality without a fixed horizon. Fixed short-term outcomes (eg, 24- or 48-hour mortality) are less common and variably defined. In this context, our choice of 30-day mortality aligns with prevailing practice and provides a standardized, clinically meaningful endpoint.6,8,15–17,20,26 Study size was determined by the available eligible population. Complete case analysis was performed, as missing data were minimal (<0.3%) and unlikely to introduce bias.
Prior to analysis, SI values and SBP measures were screened for outliers using complementary statistical methods, including z-scores and Tukey’s interquartile range; outliers were retained in the primary analysis to reflect real-world physiologic variation, with their presence documented. We assessed and compared the prognostic performance of SI and SBP for mortality prediction among trauma patients at risk of hemorrhagic shock through a sequential analytical framework. This framework was selected because standard discrimination metrics, such as the area under the curve (AUC), alone cannot fully capture the clinical utility of a prognostic tool. Segmented regression was used to identify clinically meaningful inflection points and characterize nonlinear risk relationships that would be missed by conventional approaches. Calibration assessment directly validated that predicted mortality probabilities align with observed outcomes. Decision curve analysis (DCA) quantified net benefit across realistic decision thresholds, demonstrating superior value compared to discrimination-only approaches. Together, these components provide a comprehensive evaluation that discrimination metrics alone cannot achieve.29–31
First, we fitted univariate segmented logistic regression models for each predictor (SI and SBP) to characterize potential nonlinear relationships with mortality, allowing the slope to vary across different ranges of the data, reflecting a shift in the underlying risk gradient. This approach fits a piecewise regression model that estimates the breakpoint (inflection point) where the predictor–outcome slope changes. The breakpoint was identified iteratively using Muggeo’s (2003) algorithm, with starting values guided by restricted cubic spline plots, and convergence assessed by stability across iterations.32 Using 2000 bootstrap replicates, we iteratively estimated the inflection points where slopes changed and derived corresponding 95% confidence intervals (CIs).32 This resampling approach also provided bias-corrected performance estimates by quantifying and subtracting optimism, ie, the difference between bootstrap and original sample performance, yielding more conservative and reliable measures of model discrimination. Second, we evaluated the discriminatory performance of the two models using receiver operating characteristic (ROC) curve analysis and reported the AUC with 95% CIs. For each model and across all cutoffs, we calculated sensitivity, specificity, and positive likelihood ratios (LR+). Optimal thresholds were determined using Youden’s J statistic, and we report the corresponding sensitivity, specificity, and LR+ at those thresholds, emphasizing high specificity to better identify patients truly at high risk of early death while minimizing false positives and unnecessary escalation of care and resource use.33–35 This approach was complemented by decision curve analysis to evaluate whether the identified cutoffs offer meaningful net clinical benefit beyond default strategies of treating all or no patients as high risk. Finally, we compared the performance of the two models—SI and SBP—by assessing discrimination using AUCs with DeLong’s test, predictive accuracy using calibration plots and Brier scores. We also compared LR+ based on the optimal cut point identified for each model.
Subgroup Analyses
We conducted several subgroup analyses to evaluate whether the predictive performance of SI and SBP varied across clinically relevant patient populations. Subgroups were defined by mechanism of injury (blunt vs penetrating trauma) to reflect differences in physiology and injury patterns between trauma types, and by New Injury Severity Score (NISS) categories representing minor-to-moderate (NISS <16), moderate (NISS 16–25), and severe (NISS >25) injuries. To assess clinical generalizability, the optimal thresholds identified in the primary analysis were applied uniformly across all subgroups, rather than deriving subgroup-specific cutoffs. This approach evaluates whether thresholds derived from the overall cohort maintain consistent discriminative performance across subgroups, addressing a key question for research and clinical implementation—whether a single threshold remains valid across varying injury mechanisms and severity levels.
All analyses were performed using R (version 4.5.0) with the segmented, pROC, and rmda packages for segmented regression, ROC analysis, calibration assessment, and decision curve analysis.36–38
Results
Of 14,888 patients screened across all EpiC Study sites between June 2022 and December 2024, exclusions included burns, hangings/chokings, or drownings (n = 381), other injury force types than penetrating or blunt (n = 73) and pediatric patients (n = 6), leaving 14,428 eligible trauma patients. Among these, 5054 were classified as at risk for hemorrhage; exclusions at this stage included patients not at risk for hemorrhage (n =10,675), and concomitant head injury (AIS Head ≥ 2; n = 132). After removing patients with invalid timestamps and missing SI or SBP (n = 12), the final analytic cohort comprised 3609 patients (Figure S1).
Included patients had a median age of 31.2 years (interquartile range [IQR], 25.6–38.4), and 85.9% were male. Penetrating injuries accounted for 74.6% of the patients, with stabbing or cutting being the predominant mechanism (55.6%). At presentation, patients had a median shock index of 0.9 (IQR: 0.7–1.1) and a median SBP of 100 mmHg (IQR, 88–123). Hypotension (SBP ≤90 mmHg) was present in 29.5% of patients. Using the prespecified z-score threshold of |z| >3, potential outliers were identified in 57 observations (1.6%) for SI and 23 observations (0.6%) for SBP; both variables demonstrated stable distributions with minimal extreme values. The median NISS was 10 (IQR, 3–19), with 34.3% classified as moderate or severe injuries (NISS ≥16). The median time from injury to discharge or death was 3.5 days (IQR, 1.2–7.2). Overall, 221 patients (6.1%) died within 30 days of injury (Table 1).
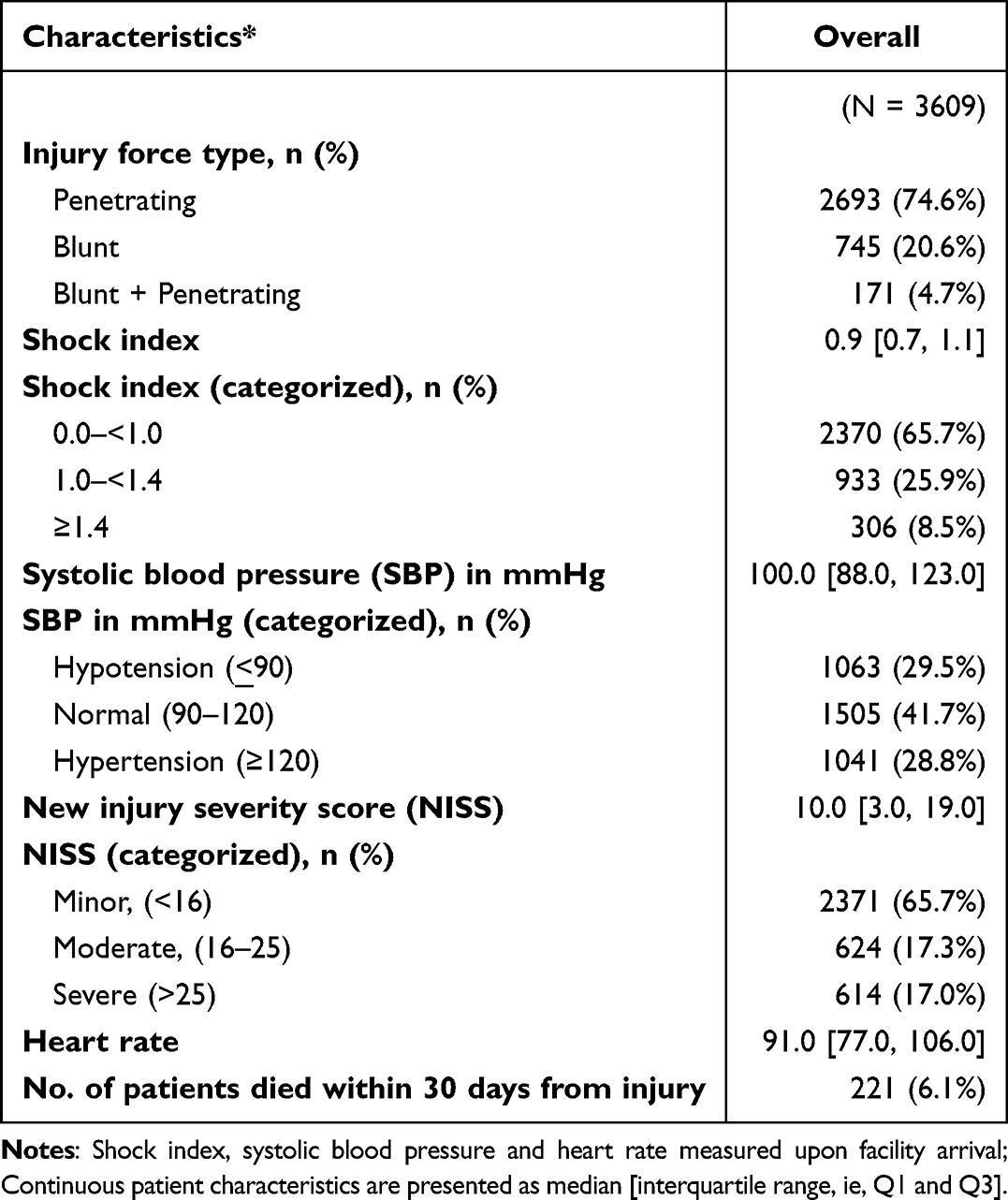 |
Table 1 Patient Physiologic and Injury Characteristics |
Nonlinear Associations and Optimal Cutoff Points for Mortality
Segmented logistic regression analysis identified distinct inflection points in the relationships between SI and SBP with mortality. The estimated inflection point for SI was 0.69 (95% CI, 0.63–0.73), above which the risk of death increased sharply. For SBP, the estimated inflection point was 82 mmHg (95% CI, 63–95 mmHg), with mortality probability rising steeply below this value (Table 2). Segmented logistic regression plots depicting the nonlinear associations of SI and SBP with mortality, along with estimated inflection points and bootstrapped 95% CIs, are presented in Figure S2.
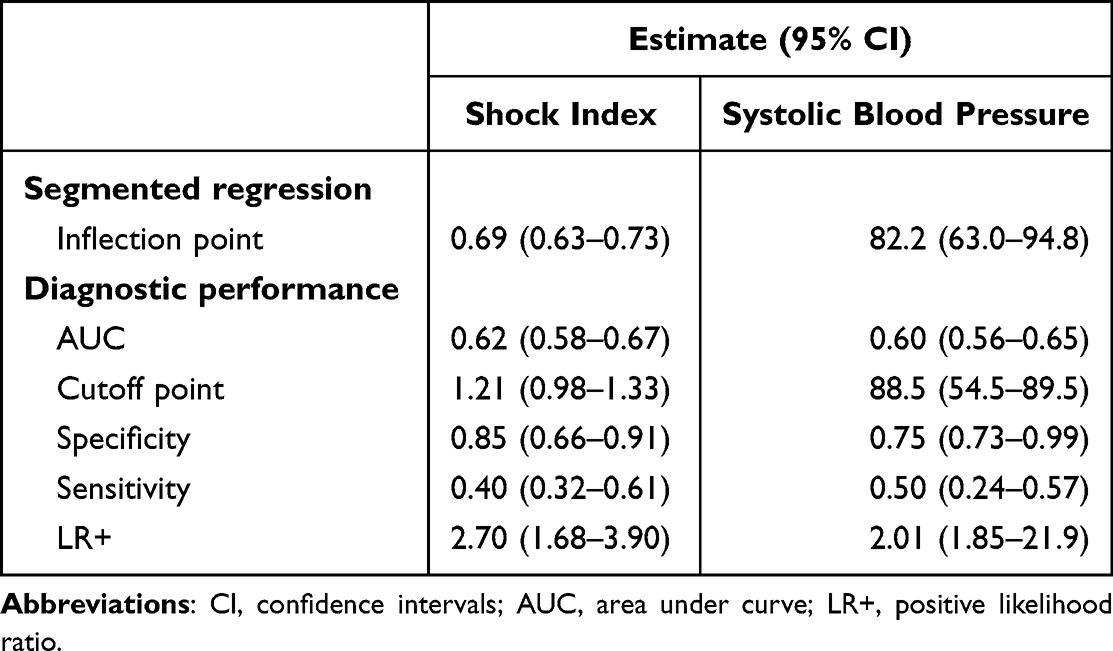 |
Table 2 Diagnostic Performance of Shock Index and Systolic Blood Pressure for 30-Day Mortality |
ROC curve analysis demonstrated modest discriminatory performance for both SI (AUC, 0.62; 95% CI, 0.58–0.67) and SBP (AUC, 0.60; 95% CI, 0.56–0.65) in predicting mortality (Table 2). ROC curves and corresponding AUC estimates for SI and SBP are presented in Figure S3. Using Youden’s J statistic, the optimal cutoff for SI was 1.21 (95% CI, 0.98–1.33), yielding a specificity of 85.1% (95% CI, 65.6–90.9%), sensitivity of 40.3% (95% CI, 31.7–60.6%), and LR+ of 2.70 (95% CI, 1.68–3.90). For SBP, the optimal cutoff was 89 mmHg (95% CI, 55–90 mmHg), with specificity of 75.0% (95% CI, 73.3–98.8%), sensitivity of 50.2% (95% CI, 24.4–56.6%), and LR+ of 2.01 (95% CI, 1.85–21.9). Both indices achieved high specificity but modest sensitivity, consistent with clinical priorities that favor minimizing false-positive classifications in emergency risk stratification. The high specificity supports the utility of these thresholds for identifying elevated risk, whereas the modest sensitivity indicates that reliance on these parameters alone would fail to capture a substantial proportion of high-risk patients.
Integrated Comparison of Overall Predictive Performance
Direct comparison showed similar discrimination between SI (AUC, 0.62) and SBP (AUC, 0.60), with no statistically significant difference using DeLong’s test (p=0.418), suggesting that neither parameter substantially outperforms the other in identifying patients at risk of mortality. However, SI demonstrated superior calibration (Figure S4), with predicted probabilities more closely aligned with observed mortality and a lower Brier score (0.054 from SI-based model vs 0.058 from SBP-based model), indicating modestly improved overall accuracy—a distinction that may be important when precise risk estimates are required for quantitative risk characterization. Furthermore, the absolute difference in LR+ was 0.69 (95% CI, 0.30–1.10; p<0.001), indicating superior rule-in performance of SI compared with SBP, which may facilitate more reliable identification of higher-risk individuals in prognostic applications. Finally, DCA showed that both SI and SBP yielded higher net benefit than reference strategies in which all or no patients were classified as high risk, across varying levels of predicted mortality risk, with particularly strong performance at lower probabilities, supporting their potential role in risk-based stratification. While SBP showed a modest advantage at very low predicted-risk levels ranging from 0.15 to 0.25, SI demonstrated consistently higher and more sustained net benefit across a broader range of predicted-risk values (up to 0.85), indicating greater robustness of SI for mortality risk stratification across heterogeneous patient profiles and injury severity distributions (Figure S5).
Subgroup Analyses
The subgroup analyses revealed variations in predictive performance across different patient populations (Tables 3 and 4). Among patients with blunt injury, the mortality rate was 6.85%, with SI demonstrating an inflection point at 0.67 and an AUC of 0.58, while SBP showed an inflection point at 85 mmHg with an AUC of 0.56, where predictive performance analyses for SI and SBP were conducted at fixed thresholds of 1.21 and 89 mmHg, respectively (Table 3). For penetrating injury patients, the mortality rate was 5.94%, with SI having an inflection point of 0.70 and AUC of 0.63 compared to SBP’s inflection point of 62.8 mmHg and AUC of 0.60. When stratified by injury severity (Table 4), patients with NISS <16 had the lowest mortality at 1.18%, while those with NISS >25 experienced the highest mortality at 23.78%. The SI inflection points varied considerably across severity groups, ranging from 0.51 in the most severely injured to 0.89 in patients with NISS <16, while SBP inflection points ranged from 63 to 94 mmHg across these same groups.
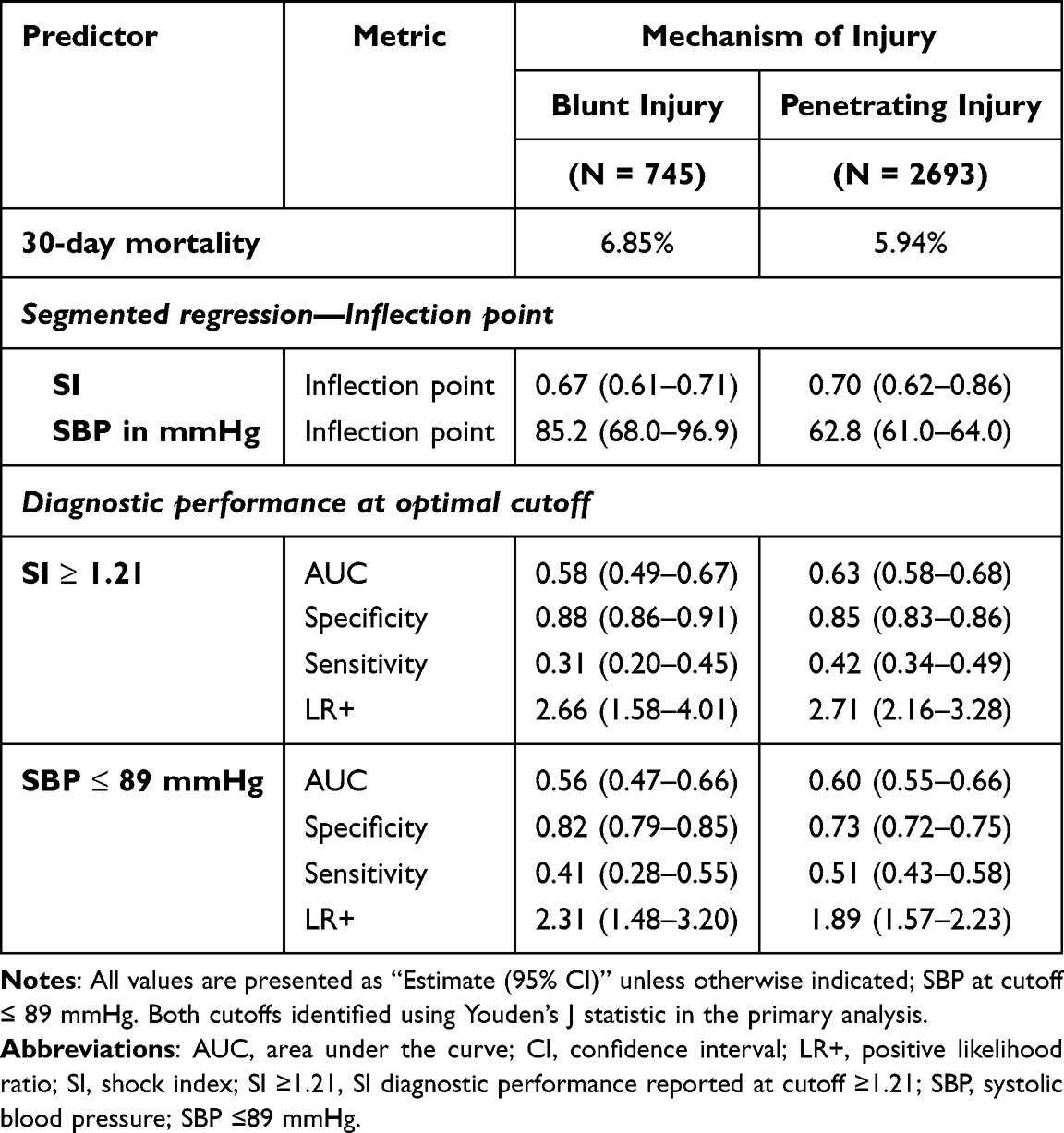 |
Table 3 Subgroup Analyses (by Mechanism of Injury) of Shock Index and Systolic Blood Pressure Performance for Mortality Prediction |
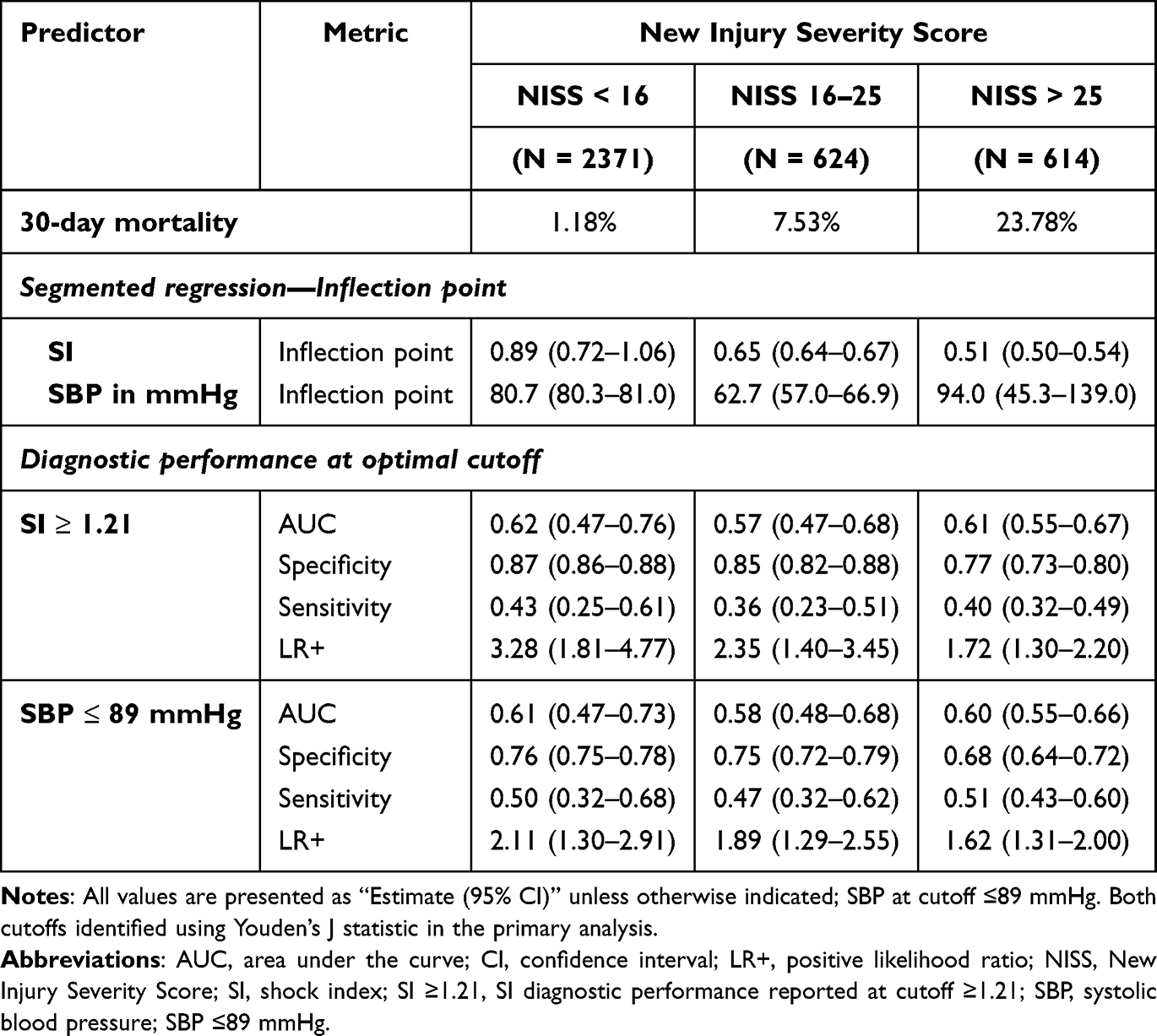 |
Table 4 Subgroup Analyses (by New Injury Severity Score) of Shock Index and Systolic Blood Pressure Performance for Mortality Prediction |
Comparing the predictive performance of SI and SBP in the subgroup analyses yielded results similar to those observed in the main analysis. DeLong’s test showed no statistically significant differences in AUC between the two predictors in any subgroup. However, SI demonstrated superior calibration performance in patients with NISS <16 and NISS >25, while calibration was similar between the two measures in other subgroups. Brier scores consistently favored SI across all subgroups, although the differences between the Brier scores of SI and SBP were generally minimal. Decision curve analysis suggested that SI provided wider net benefit ranges in most subgroups, particularly in penetrating injury and lower severity injury patients. Positive likelihood ratio comparisons revealed a statistically significant advantage for SI only in the penetrating injury subgroup (p<0.001) and in patients with NISS <16 (p=0.032), while no significant differences were observed in the remaining subgroups.
Discussion
Traditional vital signs such as SBP and heart rate are routinely used as physiologic indicators of significant hemorrhage, yet their ability to detect early or occult shock has been repeatedly challenged.13,19,39,40 This ongoing uncertainty has prompted growing interest in integrative indicators that more accurately reflect the underlying hemodynamic status. The shock index, which combines heart rate and SBP into a single parameter, has been proposed as one such marker. Its simplicity and potential for improved diagnostic accuracy make it an appealing target for research aimed at advancing early risk stratification in trauma patients.
Our study demonstrated that SI performed slightly better than SBP in predicting mortality among trauma patients at risk for hemorrhage, reinforcing its potential role in mortality risk stratification. However, these differences should be interpreted cautiously: the AUCs for both predictors were modest and statistically indistinguishable (0.62 vs 0.60; p=0.418), suggesting that neither measure alone provides strong prognostic accuracy. In segmented logistic regression models, SI exhibited superior calibration and improved accuracy predictions over SBP. Although the AUCs for SI and SBP were similar in ROC analysis, SI showed a higher LR+, indicating stronger discrimination for death. Specifically, a SI ≥1.21 was associated with a 2.7-fold increase in the likelihood of mortality compared to those with SI <1.21. Decision curve analysis further revealed that SI provided higher net benefit across a range of threshold probabilities compared to SBP. These findings are consistent with prior research demonstrating superior prognostic accuracy of SI over traditional vital signs, particularly in identifying patients at risk of hemodynamic instability despite apparently normal SBP values.19,39,41 Nevertheless, the small and statistically non-significant difference in discrimination between SI and SBP suggests that any apparent advantage of SI is limited in practical terms and reinforces that neither measure alone—particularly within a univariable framework—offers sufficient prognostic accuracy; rather, both are best considered complementary screening tools to support, rather than replace, comprehensive clinical assessment.
Determining appropriate thresholds for SI and SBP is an important methodological consideration when these measures are used for risk stratification. In our analysis, the inflection point identified through segmented regression for SI (0.69) differed from the cutoff obtained using Youden’s J statistic (1.21). This difference reflects the distinct conceptual aims of the two methods: segmented regression detects the point at which the association between SI and mortality begins to change, indicating a shift in the underlying risk gradient, whereas Youden’s J identifies the threshold that maximizes combined sensitivity and specificity for outcome classification. Thus, the former emphasizes structural change in the exposure–outcome relationship, while the latter prioritizes predictive discrimination. For SBP, the two approaches produced more similar estimates (82 and 89 mmHg), close to the conventional 90-mmHg benchmark. These observations highlight that threshold selection is method-dependent and should follow the analytic purpose rather than a universal criterion.
Although both measures showed modest discrimination, the shock index demonstrated better calibration, a higher positive likelihood ratio (2.70 vs 2.01), and superior net benefit across multiple risk thresholds. A shock index ≥1.21 could be useful to alert clinicians to patients requiring immediate resuscitative attention, early activation of massive transfusion protocols, and prioritization for higher-level trauma care. Importantly, our study contributes novel evidence from a LMIC context, where trauma remains a leading cause of preventable death and where immediate access to advanced diagnostic tools and therapeutics may be limited. The superior performance of SI compared with SBP likely reflects its ability to capture early circulatory compensation by integrating both heart rate and blood pressure. In LMIC settings, where high burdens of anemia, malnutrition, chronic infection, and limited preventive care reduce physiological reserve, patients—especially younger trauma victims or pregnant individuals commonly seen in emergency care—often maintain normal SBP despite substantial hypovolemia, hemorrhage, or blood loss, rendering hypotension a late and insensitive shock indicator.42–45 Shock index rises earlier through disproportionate tachycardia, better accounting for these compensatory mechanisms and improving risk stratification where advanced diagnostics are unavailable.45
Several limitations merit acknowledgment. First, our study population was relatively young, with 75% of patients aged between approximately 25 and 38 years. Prior investigations, such as by Bhandarkar et al, have reported that age-adjusted SI improves predictive accuracy compared with the conventional SI, largely reflecting the influence of age-related physiologic differences in cardiovascular response to trauma.46 Because of our predominantly young adult cohort, we were unable to explore this relationship. Second, the analysis was univariable and did not adjust for other relevant covariates, such as Injury Severity Score, comorbidities, or mechanism of injury, which likely contributed to the modest discriminatory performance of both predictors. The influence of unmeasured physiologic and clinical factors therefore cannot be fully ruled out. Finally, selection and survival biases cannot be excluded: our dataset captured only patients who survived to hospital presentation, thereby excluding both those who died before seeking care and those who died in the prehospital phase — arguably the most critically ill patients with the most extreme physiological derangements. This restriction of the severity spectrum may have affected the true prognostic performance of both predictors, potentially limiting the generalizability of our findings to the broader hemorrhagic trauma population. Collectively, these limitations suggest that residual confounding, selection bias, and the specific LMIC clinical context should be considered when interpreting these findings and their generalizability.
Conclusion
In trauma patients at risk of hemorrhage, SI shows marginally greater prognostic performance than SBP across multiple performance metrics, though the difference in discrimination was small and statistically nonsignificant. Its superior calibration and net benefit across risk thresholds highlight its potential value in advancing research on trauma care and outcomes. Overall, our findings add to growing evidence that SI provides clinically useful, rapid, and inexpensive risk stratification in trauma settings; its potential utility at higher thresholds may be particularly relevant for advancing research and informing care in resource-limited environments. Given the incremental nature of SI’s advantage, future research should prioritize multivariable prediction models that integrate physiologic, anatomical, and contextual variables, alongside external validation across diverse LMIC trauma populations, to establish more robust prognostic frameworks. Future studies incorporating age-adjusted indices and pre-hospital data are also warranted to refine its prognostic utility across diverse trauma populations.
Abbreviations
LMIC, Low- and middle-income countries; SBP, Systolic blood pressure; SI, Shock index; HR, heart rate; MT, massive transfusion; EpiC, Epidemiology and Outcomes of Prolonged Trauma Care study; EMS, emergency medical services; OHRO, Office of Human Research Oversight; AIS, Abbreviated Injury Scale; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology; CI, Confidence intervals; ROC, Receiver operating characteristic; AUC, Area under the curve; LR+, Positive likelihood ratios; DCA, Decision curve analysis; NISS, New Injury Severity Score; IQR, interquartile range.
Data Sharing Statement
Data is provided within the manuscript or additional information files. Public access to the dataset is closed due to contractual limitations. The datasets included and/or analysed during the current study are available from the corresponding author upon reasonable request and upon satisfying contractual and regulatory requirements.
Ethics Approval
This study was performed in line with the principles of the 1964 Declaration of Helsinki. Ethics approval was originally provided with a waiver of informed consent from the Stellenbosch University Health Research Ethics Committee, Cape Town, South Africa, the primary IRB (Project ID 14866; Ref. No. N20/03/036) on 25 AUG 2020. The University of Colorado ceded oversight to Stellenbosch (Protocol 20-2176). The Defense Health Agency’s Office of Human Research Oversight, Virginia, United States provided second-level review and concurrence (OHRO Log Number E01863.1x).
Consent
Due to the high patient acuity and challenging emergency care environments, an exemption from obtaining informed consent was granted by the primary ethics board.
Acknowledgments
No artificial intelligence assisted technologies were used in the production of the submitted work. The findings, views, and conclusions presented are those of the authors and do not represent the official policy or position of the United States Defense Health Agency or the Western Cape Department of Health and Wellness.
We would like to thank and acknowledge the EpiC study research staff who helped collect data for this process: Dr. Mandy Abels; Dr. Raeesah Bray; Mr. Anthony Carr; Dr. Melany Codling; Ms. Zuleiga Davids; Ms. Magzane Ghall, Dr. Chloe Ile; Ms. Daisy Inglis; Ms. Alana Jooste; Mr. Vusumzi Kose; Dr. Kelsey Mc Intyre; Mr. Fabio Moriera; Dr. Jani Marais; Dr. Lindi Martin; Sr. Minnie Minnaar; Ms. Tanisha Morris; Dr. Tevarus Naicker; Dr. Azia Parker; Dr. Tahrir Rasool; Ms. Regan Smith; Dr. Alexa van der Walt; Ms. Catherine Wandie.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
United States Defense Health Agency award numbers/grant log numbers: W81XWH-20-2-0042 and HT9425-23-1-1025.
Disclosure
SGS, SdV, HL, WS, CW, JD, and NKMM have all received grant funds from the United States Defense Health Agency. SGS has received grant funding from SeaStar Medical and reports meeting/travel support from Special Operations Medicine Association, outside the submitted work. MDS participated on a data safety/advisory board for National Institute of Aging (NIA) and National Institute of Health Disparities (NIHD), outside the submitted work. None of the military authors have received salary support. The authors report no other conflicts of interest in this work.
References
1. World Health Organization. Injuries and Violence. [Internet]. World Health Organization; 2024. Available from: https://www.who.int/news-room/fact-sheets/detail/injuries-and-violence.
2. Eastridge BJ, Mabry RL, Seguin P, et al. Death on the battlefield (2001-2011): implications for the future of combat casualty care. J Trauma Acute Care Surg. 2012;73(6 Suppl 5):S431–11. doi:10.1097/TA.0b013e3182755dcc
3. Merchant AAH, Haider AH. International variation in injury burden and comparative outcomes: how injury looks like in different parts of the world. Surgery. 2024;176(3):972–975. doi:10.1016/j.surg.2024.05.018
4. Kulkarni AJ, Batra A, Eisner ZJ, et al. Prehospital hemorrhage management in low- and middle-income countries: a scoping review. World J Surg. 2024;48(3):547–559. doi:10.1002/wjs.12054
5. Shanthakumar D, Payne A, Leitch T, Alfa-Wali M. Trauma care in low- and middle-income countries. Surg J. 2021;7(4):e281–e285. doi:10.1055/s-0041-1732351
6. Tyson AF, Varela C, Cairns BA, Charles AG. Hospital mortality following trauma: an analysis of a hospital-based injury surveillance registry in sub-Saharan Africa. J Surg Educ. 2015;72(4):e66–72. doi:10.1016/j.jsurg.2014.09.010
7. Bernhardt IM, Moore EE, Sauaia A, et al. Timing of trauma deaths due to uncontrolled bleeding have not changed in three decades: a multicenter study of patients in hemorrhagic shock. Am J Surg. 2025;250:116510. doi:10.1016/j.amjsurg.2025.116510
8. Eastridge BJ, Holcomb JB, Shackelford S. Outcomes of traumatic hemorrhagic shock and the epidemiology of preventable death from injury. Transfusion. 2019;59(S2):1423–1428. doi:10.1111/trf.15161
9. Wohlgemut JM, Pisirir E, Stoner RS, et al. Identification of major hemorrhage in trauma patients in the prehospital setting: diagnostic accuracy and impact on outcome. Trauma Surg Acute Care Open. 2024;9(1):e001214. doi:10.1136/tsaco-2023-001214
10. Christie SA, Zheng D, Dissak-Delon F, et al. How trauma patients die in low resource settings: identifying early targets for trauma quality improvement. J Trauma Acute Care Surg. 2023;94(2):288–294. doi:10.1097/TA.0000000000003768
11. Yeboah D, Mock C, Karikari P, Agyei-Baffour P, Donkor P, Ebel B. Minimizing preventable trauma deaths in a limited-resource setting: a test-case of a multidisciplinary panel review approach at the Komfo Anokye Teaching Hospital in Ghana. World J Surg. 2014;38(7):1707–1712. doi:10.1007/s00268-014-2452-z
12. Sobrino J, Shafi S. Timing and causes of death after injuries. Proc. 2013;26(2):120–123. doi:10.1080/08998280.2013.11928934
13. Mutschler M, Nienaber U, Munzberg M, et al. The Shock Index revisited - a fast guide to transfusion requirement? A retrospective analysis on 21,853 patients derived from the TraumaRegister DGU. Crit Care. 2013;17(4):R172. doi:10.1186/cc12851
14. Allgower M, Burri C. “Shock index”. Dtsch Med Wochenschr. 1967;92(43):1947–1950. “Schockindex”. doi:10.1055/s-0028-1106070
15. Carsetti A, Antolini R, Casarotta E, et al. Shock index as predictor of massive transfusion and mortality in patients with trauma: a systematic review and meta-analysis. Crit Care. 2023;27(1):85. doi:10.1186/s13054-023-04386-w
16. Pandit V, Rhee P, Hashmi A, et al. Shock index predicts mortality in geriatric trauma patients: an analysis of the National Trauma Data Bank. J Trauma Acute Care Surg. 2014;76(4):1111–1115. doi:10.1097/TA.0000000000000160
17. Singh A, Ali S, Agarwal A, Srivastava RN. Correlation of shock index and modified shock index with the outcome of adult trauma patients: a prospective study of 9860 patients. N Am J Med Sci. 2014;6(9):450–452. doi:10.4103/1947-2714.141632
18. Wu SC, Rau CS, Kuo SCH, Hsu SY, Hsieh HY, Hsieh CH. Shock index increase from the field to the emergency room is associated with higher odds of massive transfusion in trauma patients with stable blood pressure: a cross-sectional analysis. PLoS One. 2019;14(4):e0216153. doi:10.1371/journal.pone.0216153
19. Kheirbek T, Martin TJ, Cao J, Hall BM, Lueckel S, Adams CA. Prehospital shock index outperforms hypotension alone in predicting significant injury in trauma patients. Trauma Surg Acute Care Open. 2021;6(1):e000712. doi:10.1136/tsaco-2021-000712
20. Aleka P, Van Koningsbruggen C, Hendrikse C. The value of shock index, modified shock index and age shock index to predict mortality and hospitalisation in a district level emergency centre. Afr J Emerg Med. 2023;13(4):287–292. doi:10.1016/j.afjem.2023.09.007
21. Crawford R, Kruger D, Moeng M. Shock index as a prognosticator for emergent surgical intervention and mortality in trauma patients in Johannesburg: a retrospective cohort study. Ann Med Surg Lond. 2021;69:102710. doi:10.1016/j.amsu.2021.102710
22. Barnes R, Clarke D, Farina Z, et al. Vital sign based shock scores are poor at triaging South African trauma patients. Am J Surg. 2018;216(2):235–239. doi:10.1016/j.amjsurg.2017.07.025
23. Suresh K, Dixon JM, Patel C, et al. The epidemiology and outcomes of prolonged trauma care (EpiC) study: methodology of a prospective multicenter observational study in the Western Cape of South Africa. Scand J Trauma Resusc Emerg Med. 2022;30(1):55. doi:10.1186/s13049-022-01041-1
24. Wogu AF, Dixon JM, Xiao M, et al. Tranexamic acid is associated with post-injury mortality in a resource-limited trauma system: findings from the epidemiology and outcomes of prolonged trauma care cohort study. Transfusion. 2025;65 Suppl 1(Suppl 1):S276–S287. doi:10.1111/trf.18171
25. Quake SYL, Khoda F, Arjomandi Rad A, et al. The current status and challenges of prehospital trauma care in low- and middle-income countries: a systematic review. Prehosp Emerg Care. 2024;28(1):76–86. doi:10.1080/10903127.2023.2165744
26. Odland ML, Abdul-Latif AM, Ignatowicz A, et al. Equitable access to quality trauma systems in low-income and middle-income countries: assessing gaps and developing priorities in Ghana, Rwanda and South Africa. BMJ Glob Health. 2022;7(4). doi:10.1136/bmjgh-2021-008256
27. Vandenbroucke JP, von Elm E, Altman DG, et al. Strengthening the reporting of observational studies in epidemiology (STROBE): explanation and elaboration. Int J Surg. 2014;12(12):1500–1524. doi:10.1016/j.ijsu.2014.07.014
28. Mould-Millman NK, Dixon JM, Lategan HJ, et al. Feasibility of conducting a military-relevant multicenter cohort study to assess outcomes of early trauma resuscitative interventions in a prolonged care civilian setting. J Trauma Acute Care Surg. 2023;95(2S Suppl 1):S88–S98. doi:10.1097/TA.0000000000004066
29. Huang Y, Li W, Macheret F, Gabriel RA, Ohno-Machado L. A tutorial on calibration measurements and calibration models for clinical prediction models. J Am Med Inform Assoc. 2020;27(4):621–633. doi:10.1093/jamia/ocz228
30. Rufibach K. Use of Brier score to assess binary predictions. J Clin Epidemiol. 2010;63(8):938–9; authorreply939. doi:10.1016/j.jclinepi.2009.11.009
31. Vickers AJ, van Calster B, Steyerberg EW. A simple, step-by-step guide to interpreting decision curve analysis. Diagn Progn Res. 2019;3:18. doi:10.1186/s41512-019-0064-7
32. Muggeo VM. Estimating regression models with unknown break-points. Stat Med. 2003;22(19):3055–3071. doi:10.1002/sim.1545
33. Parsons R, Blythe R, Cramb SM, McPhail SM. Integrating economic considerations into cutpoint selection may help align clinical decision support toward value-based healthcare. J Am Med Inform Assoc. 2023;30(6):1103–1113. doi:10.1093/jamia/ocad042
34. Veldhuis LI, Hollmann MW, Kooij FO, Ridderikhof ML. A pre-hospital risk score predicts critical illness in non-trauma patients transported by ambulance to a Dutch tertiary referral hospital. Scand J Trauma Resusc Emerg Med. 2021;29(1):32. doi:10.1186/s13049-021-00843-z
35. Costa A, Carron PN, Zingg T, Roberts I, Ageron FX, Swiss Trauma R. Early identification of bleeding in trauma patients: external validation of traumatic bleeding scores in the Swiss Trauma Registry. Crit Care. 2022;26(1):296. doi:10.1186/s13054-022-04178-8
36. Fasola S, Muggeo VMR, Küchenhoff H. A heuristic, iterative algorithm for change-point detection in abrupt change models. Comput Stat. 2018;33(2):997–1015. doi:10.1007/s00180-017-0740-4
37. Robin X, Turck N, Hainard A, et al. pROC: an open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinf. 2011;12:77. doi:10.1186/1471-2105-12-77
38. Rmda: Risk Model Decision Analysis. CRAN (Comprehensive R Archive Network); 2018. Version 1.6.
39. Haider AA, Azim A, Rhee P, et al. Substituting systolic blood pressure with shock index in the National Trauma Triage Protocol. J Trauma Acute Care Surg. 2016;81(6):1136–1141. doi:10.1097/TA.0000000000001205
40. Bruijns SR, Guly HR, Bouamra O, Lecky F, Lee WA. The value of traditional vital signs, shock index, and age-based markers in predicting trauma mortality. J Trauma Acute Care Surg. 2013;74(6):1432–1437. doi:10.1097/TA.0b013e31829246c7
41. Cannon CM, Braxton CC, Kling-Smith M, Mahnken JD, Carlton E, Moncure M. Utility of the shock index in predicting mortality in traumatically injured patients. J Trauma. 2009;67(6):1426–1430. doi:10.1097/TA.0b013e3181bbf728
42. Lin TM, Memon AM, Reeson EA, et al. Shock index identifies compensated shock in the ‘Normotensive’ trauma patient. Injury. 2025;56(9):112419. doi:10.1016/j.injury.2025.112419
43. Kassavin DS, Kuo YH, Ahmed N. Initial systolic blood pressure and ongoing internal bleeding following torso trauma. J Emerg Trauma Shock. 2011;4(1):37–41. doi:10.4103/0974-2700.76833
44. Guly HR, Bouamra O, Spiers M, et al. Vital signs and estimated blood loss in patients with major trauma: testing the validity of the ATLS classification of hypovolaemic shock. Resuscitation. 2011;82(5):556–559. doi:10.1016/j.resuscitation.2011.01.013
45. Birkhahn RH, Gaeta TJ, Terry D, Bove JJ, Tloczkowski J. Shock index in diagnosing early acute hypovolemia. Am J Emerg Med. 2005;23(3):323–326. doi:10.1016/j.ajem.2005.02.029
46. Bhandarkar P, Munivenkatappa A, Roy N, Kumar V, Moscote-Salazar LR, Agrawal A. Pattern and distribution of shock index and age shock index score among trauma patients in towards improved trauma care outcomes (TITCO) dataset. Bull Emerg Trauma. 2018;6(4):313–317. doi:10.29252/beat-060407
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.