Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 9
Shear bond strength of different surface treatments in bulk fill, microhybrid, and nanoparticle repair resins
Authors de Jesus Tavarez RR ![]() , Almeida Júnior LJS, Guará TCG, Ribeiro IS, Maia Filho EM
, Almeida Júnior LJS, Guará TCG, Ribeiro IS, Maia Filho EM ![]() , Firoozmand LM
, Firoozmand LM
Received 23 February 2017
Accepted for publication 4 May 2017
Published 3 July 2017 Volume 2017:9 Pages 61—66
DOI https://doi.org/10.2147/CCIDE.S135416
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Rudys Rodolfo de Jesus Tavarez,1 Lauber Jose dos Santos Almeida Júnior,2 Tayanne Christine Gomes Guará,1 Izabella Santos Ribeiro,1 Etevaldo Matos Maia Filho,1 Leily Macedo Firoozmand2
1Department of Restorative Dentistry, Ceuma University (CEUMA), 2Department of Dentistry I, University Federal of Maranhão (UFMA), São Luís, Maranhão, Brazil
Objectives: The purpose of this study was to evaluate the influence of surface treatment and different types of composite resin on the microshear bond strength of repairs.
Materials and methods: Seventy-two specimens (n=72) were prepared using a nanoparticle resin and stored in artificial saliva at 37 ± 1°C for 24 h. After this period, the specimens (n=24) were restored with microhybrid resin P60 (3M ESPE), nanoparticle resin Filtek Z350 (3M ESPE), and Bulk Fill Surefil SDR Flow (Dentsply) composite resins. Previously, the surfaces of the samples were treated, forming the following subgroups (n=12): (A) conditioned with 37% phosphoric acid for 30 s, and (B) abrasioned with a diamond tip for 3 s and conditioned with 37% phosphoric acid. In all groups, before insertion of the composite resin, the adhesive system Adper Single Bond 2 was actively applied and photopolymerized for 20 s.
Results: The microshear test was executed to assess bond strength. Kruskal–Wallis (p<0.05) and Mann–Whitney statistical tests showed significant statistical difference considering that the bulk-fill resin turned out to have a lower bond strength than the conventional nanoparticle and microhybrid composites. With regard to the technique, the roughening with diamond bur followed by the application of phosphoric acid exhibited values higher than the exclusive use of acid.
Conclusion: The microshear bond strength of the composite resin repairs varies in accordance with the type of composite resin utilized, and roughening the surface increased the bond strength of these materials.
Keywords: bulk-fill resins, composite resins, dental restoration repair, microshear strength, surface treatment composite repair
Introduction
In recent years, the concept of minimally invasive odontology suggests the repair of restorations instead of their replacement when clinically indicated.1 Restorations with minor damage—small fractures, signs of absence of marginal infiltration, and secondary caries—may be repaired. Studies reveal that the repair of composite resin restorations is viable in the long term2 and is a safe and effective treatment.1
When repairing aesthetic restorations, the identification of the composite resin is a known clinical problem. Different commercial brands have different compositions, and the type of resin seems to be the main factor influencing the bond strength of the repair.3 However, it is noted that the practice of associating composite resins of different compositions is common during the restoration procedure.4 Beyond the vast variety of resins already existing in the market, in recent years, resin composites called “bulk-fill” (BF) that can be inserted into a cavity with larger increments have come to light. Some BF resin composites have a higher fluidity and penetration in hard access cavities, helping eliminate factors associated with polymerization stress, such as marginal fractures.5 Nevertheless, little is yet known about the behavior of these resins in composite resin restoration repair.
Besides the composition of these restoring materials, the treatment of the restoration surface to be repaired must also be observed. Treatment success is achieved through the adequate union of the remaining restoration and the restoring material,6 taking into consideration that this repair may include mechanical and/or chemical treatment.7,8 Several methods, such as abrasion with diamond burs,7,9 acid conditioning with hydrofluoric acid or phosphoric acid,6,7 abrasion with squirts of aluminum oxide particles with or without silane coupling agents, and adhesive systems in the resin, were proposed to improve bond strength between the remaining substrate and the new resin material.10
Although there are comparative studies on surface treatment in literature, none of the treatments can be recommended as a universally applicable repair technique. Furthermore, the professional does not always dispose of all materials at the clinic, often simplifying the technique with diamond tips and phosphoric acid. Moreover, in order to choose the most adequate repair technique to obtain bond strength between the composite resins, the interaction between these different resinous materials must be known. There are few clinical and laboratory results that indicate significant advantages for the use of BF composite resins and encourage clinical implementation of the material.11
Thus, this study aims to evaluate the bond strength of repairs made with BF resin as well as conventional nanoparticle and microhybrid resins, through two surface treatment techniques, by using the microshear test. The tested hypotheses are as follows: 1) there is no difference in bond strength between the composite resins tested and 2) the different surface treatment techniques do not influence the bond strength of the repair in composite resins.
Materials and methods
Seventy-two specimens were confectioned using the nanoparticle resin Filtek Z350 (3M ESPE, São Paulo, Brazil). Specimens were prepared employing Teflon matrices (diameter 4 mm, thickness 2 mm) where the composite resin Z350 (3M ESPE, São Paulo, Brazil) was inserted and photopolymerized with the aid of the Optilux 501 (Demetron®, 3M, Danbury, CT, USA) for 40 s. The specimens were then positioned in PVC tubes and embedded in acrylic resin (Classic Jet, São Paulo, Brazil), in a way that allowed the correct positioning of the specimens. Posteriorly, they were submerged in artificial saliva and stored in a bacteriological incubator (37±1°C) for 24 h. The composite resin surface was then cleaned with pumice stone and water was applied with a Robinson brush.
Afterwards, the specimens were allocated randomly to three groups (n=24) for the execution of the repair using the following resins: G350 - resin Filtek Z350 (3M ESPE), G60 - resin P60 (3M ESPE), and GBF - bulk-fill Surefil SDR Flow resin (Dentsply) (Table 1).
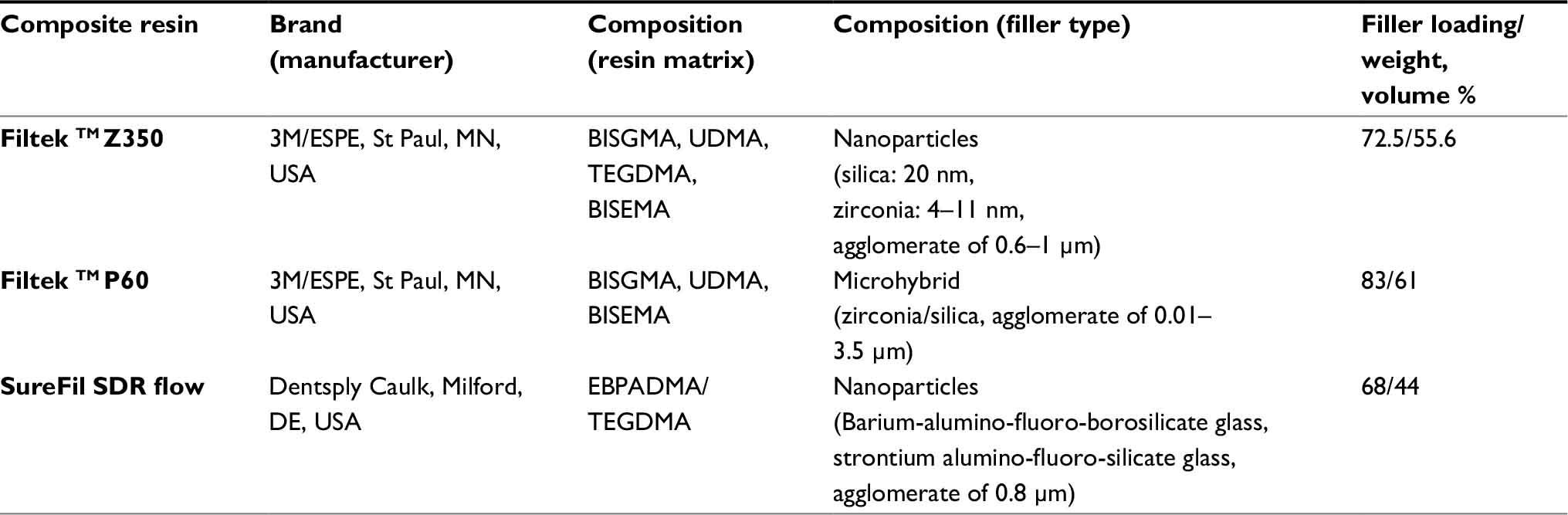 | Table 1 Characteristics of the materials Abbreviations: BISGMA, bisphenol A diglycidyl ether dimethacrylate; BISEMA, bisphenol A polyethylene glycol diether dimethacrylate, UDMA, diurethane dimethacrylate; TEGDMA, triethyleneglycol dimethacrylate; EBPADMA, ethoxylated bisphenol-A dimethacrylate. |
Prior to surface treatment, each group was subdivided into subgroups A and B, with 12 specimens in each. Subgroup A was conditioned with phosphoric acid at 37% (Ultra-etch – ULTRADENT, SP, Brazil) for 30 s and washed with abundant water for the same duration. Subgroup B was submitted to surface abrasion with a diamond-rounded tip (3146 KG Sorensen, Cotia, SP, Brazil) for 3 s and then acid conditioned in a similar manner as subgroup A. In every group, the adhesive system Adper Single Bond 2 (3M, Sumaré, SP, Brazil) was applied in accordance with the manufacturer’s recommendations, and in compliance with the previously established subgroup division. After surface treatment and adhesive system application, the specimens were repaired in conformity with specifications of the groups G350, G60, and GBF.
Three tubes (Tygon® 54-HL Medical Tubing, Saint Gobain, Akron, OH, USA) with an approximate internal diameter of 0.7 mm and measuring 0.4 mm in height were applied to the resin surface of each specimen. The composite resins (color A3) were positioned in the interior of the tubes, filling the internal volume of the tube, and photopolymerized for 40 s. All of the photoactivation procedures were realized with the polymerization lamp for 40 s under a light intensity of 600 mW/cm2.
Posteriorly, they were submerged into distilled water and then stored in an incubator (37±1ºC) for 24 h. Thereafter, the tubes were carefully removed with the aid of a scalpel blade to expose the composite resin cylinders.
The specimens were attached to a bench vice, immobilizing them parallel to the microshear. For the microshear test, a stainless steel wire (0.2 with 0.2 mm diameter; Morelli Ortodontia, São Paulo, SP, Brazil) was inserted around the resin cylinder and aligned to the adhesive union interface, allowing the force vector to be parallel to the specimen surface. The test was carried out in the universal testing machine, at a speed of 0.5 mm/min to the point of fracture. The arithmetic mean of the fracture in the three composite resin cylinders was used as the final value of bond strength in each specimen.
After the microshear tests, the surfaces of the specimens were examined to determine the kind of adhesive imperfections that were evident. The specimens were analyzed through a stereomicroscope under 40× magnification to verify the type of fracture that occurred. The surfaces of specimens were analyzed on the basis of the scores proposed by Diniz et al12: 1) adhesive fracture – interface resin/adhesive, 2) cohesive fracture – composite resin substrate, 3) cohesive fracture – composite resin repair, and 4) mixed fractures – composite resin/adhesive.
Statistical analysis
The data were organized and submitted to statistical tests. The Kolmogorov–Smirnov test showed that adhesive resistances in the distinct groups did not present a normal distribution (p<0.05). Next, the Kruskal–Wallis and Mann–Whitney tests were applied to compare the adhesive resistance values and the type of fracture. The value α equal to 0.05 with Bonferroni correction was used for multiple comparisons resulting in an α for each of the six comparisons of 0.008. The software used were PASW Statistic (v.17; SPSS Inc., Chicago, IL, USA) and GraphPad Prism (v. 5-2007, San Diego, CA, USA; release 17.0.2.2009).
Results
The arithmetic mean, average deviation, and average true range of values of resistance to shearing in the studied groups are presented on Table 2.
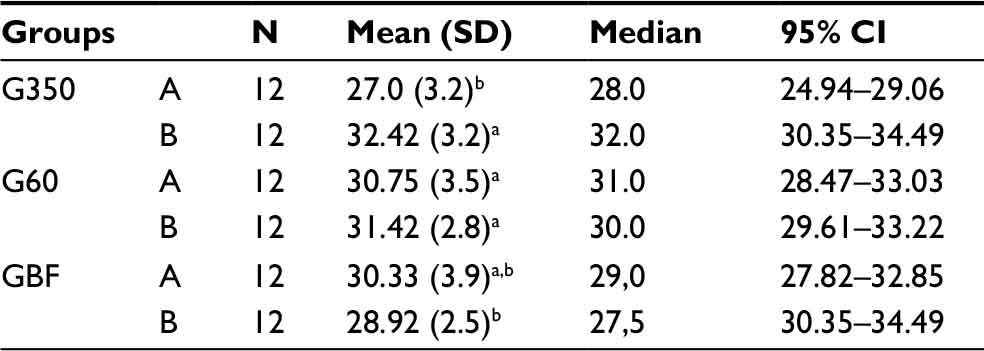 | Table 2 Mean (standard deviation) values of bond strength (MPa) and Mann–Whitney test Notes: Mann–Whitney test; different letters (a and b) after the median value stand for significant differences with treatment (p<0.008). Subgroup A: conditioned with phosphoric acid at 37%. Subgroup B: submitted to surface abrasion with a diamond rounded tip + conditioned with phosphoric acid at 37%. |
The Kruskal-Wallis test (p<0.05) and the Mann-Whitney test evidenced significant statistical difference between the groups (Table 2). Groups G350_B, G60-A, and G60-B manifested the highest bond strength compared to groups GBF-B and G350-A; the remaining groups did not differ from each other.
After the microshear test, analysis of the type of fracture (Table 3), showed that the greatest number of failures found were adhesive.
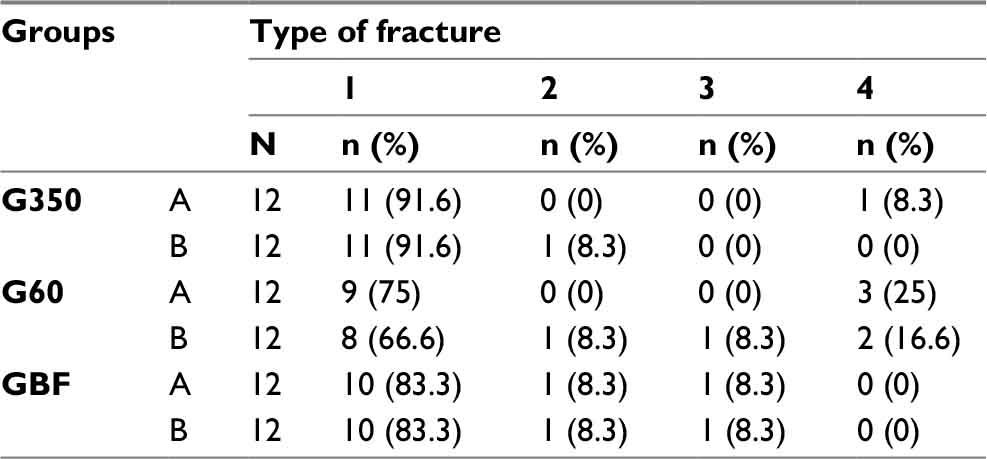 | Table 3 Distribution of absolute and relative frequency (type of fracture for groups) Notes: 1-adhesive fracture – interface resin/adhesive, 2-cohesive fracture – composite resin substrate, 3-cohesive fracture – composite resin repair, 4-mixed fractures – composite resin/adhesive. |
Discussion
It is increasingly evident that there is a need for conservative techniques that make the conservation and maintenance of composite resin restorations viable. The tested hypotheses which suggest that there is no difference between restorative repairs executed with different types of composite resins and that the differences in surface treatment techniques do not influence the bond strength of repairs in composite resin were not accepted.
The microshear test is considered an adequate method for verifying the bond strength of materials.13 Advantages of the microshear bond test include less demanding specimen collection and easier control of the bond test area by means of microbore (Tygon) tubes.14 According to Thanaratikul, Santiwong, and Harnirattisai,15 tests of shear bond strength, especially traction and shear tests, are applied for evaluating restoration materials. Furthermore, the shear test is a better representation of the forces clinically experienced by a restoration.
The results of this study made it possible to verify a lower bond strength for the resins GBF (nanoparticles) and Z350 (nanoparticles) compared to resin P60 (microhybrid) when they were utilized as a repair over a remaining restoration. The BF resin is composed of ethoxylated bisphenol A dimethacrylate (EBPADMA) and triethylene glycol dimethacrylate (TEGDMA) with a 44% volume in its inorganic part. On the other hand, the resin Z350 is composed of bisphenol A diglycidyl ether dimethacrylate (Bis-GMA), urethane dimethacrylate, and Bisphenol A polyethylene glycol diether dimethacrylate (Bis-EMA) with a volume of 55.6%. By contrast, the resin P60 is composed of Bis-GMA, Bis-EMA, and TEGDMA with a volume of 61%. The higher bond strength for resin P60 may be related to the higher quantity of inorganic particle (61%) in it compared to Z350 (55.6%) and GBF (44%). Therefore, it is possible that resins with a higher inorganic particle quantity are more resistant when put through the microshear test, corroborating reports in the literature that indicate a higher resistance to shearing in resins with a higher inorganic particle rate.4
Moreover, particle sizes may influence bond strength. Evaluating the mechanical and structural characteristics of materials,16 flexural strength,17 and color stability18 has been recently tested nanofilled materials, but there is a lack of studies evaluating adhesive resistance after repair. Rodrigues et al8 observed that the microstructure of composite resins influences average bond strength values, wherein a microhybrid resin displays a higher strength compared to a nanoparticle resin, corroborating results found in our study. Spyrou et al3, on the other hand, observed repairs between different resin compositions and particle size and concluded that there are differences between them.
When evaluating the bond strength of restorations using BF, flow, and nanoparticle resins, the BF resin manifested lower values in class V cavities.19 However, another study, which investigated the shear bond strength of hybrid/hybrid resins and hybrid/nanoparticle resins, did not reveal a statistical difference between hybrid and nanoparticle resins when associated.4
The results found in this study for different surface treatments display statistical difference, because the groups in which the specimen surface was abraded with a diamond bur followed by phosphoric acid conditioning – G350 and G60 – displayed better results than the GBF group. When the treatment was carried out only with phosphoric acid, the G60 group displayed better results, followed by the BF and G350 groups, respectively.
Differences in union resistance depend on the surface treatment.20 Surface treatments permit mechanical retention and linkage between substrates with the same kind of material. According to Rodrigues et al,8 repairs occur through three mechanisms: 1) micromechanical union through surface irregularities, 2) chemical linking between two resin matrices, and 3) chemical linking in the filling.
Among the various kinds of surface treatments available, the one with most technical simplicity, availability, and clinical praxis is the use of phosphoric acid and/or diamond tips. Abrasion with diamond tips is an important method for promoting microretention in the substrate. However, variations in diamond granules do not affect repair endurance21; microretention promoted by the bur is probably a frequent cause of bond ing to the substrate or exposed particles.22
The effectiveness of acid conditioning depends on the organic and inorganic composition of the composite resin,7 and this effect is generally associated with the removal of occasional surface impurities.23 Furthermore, another study has shown that the removal of contaminants like saliva and residual material has proved to be more important than mechanical surface abrasions.24 In addition to the chemical composition of the organic part, the inorganic portion must be observed. All of the studied resins have silica in their structure; however, the BF resin does not have zirconia in its matrix. This must be taken into consideration, as zirconia is mechanically more resistant than aluminum oxides.25
The microretentions promoted by abrasion with a diamond bur could justify a higher retention of microhybrid resins, because these microporosities promote higher retention than nanoparticle resins do.8 Although BF resin presents a low viscosity and elevated fluidity with internal adaptation in dentine,26 these characteristics, by themselves, are not sufficient to promote a higher bond strength in repairs done with composite resins. Fluid resins have reduced mechanical and physical features compared to traditional hybrid resins27; this may represent a concern when the repair is in a high-tension area,28 suggesting indications for cracking.29
The validity of the shear bond test was confirmed by the low variability in the results related to imperfection type, whereas, in the present study, more imperfections of the adhesive type were observed, corroborating other studies.4,30
Conclusion
Despite the limitations of this study, BF resin presented inferior results compared to conventional nanoparticle and microhybrid resins in the bond strength of repairs that included surface abrasion with a diamond bur followed by acid conditioning in vitro. The type of surface treatment showed greater influence on the conventional nanoparticulate resin (z350), because the abrasion with diamond tip indicated better results for the restorative repair. When repairs with composite resins are made, the kind of material used must be taken into account, as surface detrition may favor the adhesion of certain materials over others. Future studies are needed in order to confirm the results of the present report.
Acknowledgments
The authors are grateful to the assistance granted by the Assistance Foundation of Research of Maranhão (FAPEMA) and the Institutional Scholarship Program for Scientific Initiation (PIBIC)-CEUMA.
Disclosure
The authors report no conflicts of interest in this work.
References
Fernández E, Martín J, Vildósola P, et al. Can repair increase the longevity of composite resins? Results of a 10-year clinical trial. J Dent. 2015;43(2):279–286. | ||
Blum IR, Schriever A, Heidemann D, Mjör IA, Wilson NH. The repair of direct composite restorations: an international survey of the teaching of operative techniques and materials. Eur J Dent Educ. 2003;7(1):41–48. | ||
Spyrou M, Koliniotou-Koumpia E, Kouros P, Koulaouzidou E, Dionysopoulos P. The reparability of contemporary composite resins. Eur J Dent. 2014;8(3):353–359. | ||
Ribeiro JC, Gomes PN, Moysés MR, Dias SC, Pereira LJ, Ribeiro JG. Shear strength evaluation of composite-composite resin associations. J Dent. 2008;36(5):326–330. | ||
Burgess J, Cakir D. Comparative properties of low-shrinkage composite resins. Compend Contin Educ Dent. 2010;31(2):10–15. | ||
Loomans BA, Cardoso MV, Opdam NJ, et al. Surface roughness of etched composite resin in light of composite repair. J Dent. 2011;39(7):499–505. | ||
Papacchini F, Dall’Oca S, Chieffi N, et al. Composite-to-composite microtensile bond strength in the repair of a microfilled hybrid resin: effect of surface treatment and oxygen inhibition. J Adhes Dent. 2007;9(1):25–31. | ||
Rodrigues SA Jr, Ferracane JL, Della Bona A. Influence of surface treatments on the bond strength of repaired resin composite restorative materials. Dent Mater. 2009;25(4):442–451. | ||
Valente LL, Silva MF, Fonseca AS, Münchow EA, Isolan CP, Moraes RR. Effect of diamond bur grit size on composite repair. J Adhes Dent. 2015;17(3):257–263. | ||
Swift EJ Jr, LeValley BD, Boyer DB. Evaluation of new methods for composite repair. Dent Mater. 1992;8(6):362–365. | ||
El-Safty S, Silikas N, Watts DC. Creep deformation of restorative resin-composites intended for bulk-fill placement. Dent Mater. 2012;28(8):928–935. | ||
Diniz AC, Bandeca MC, Pinheiro LM, et al. Influence of different etching modes on bond strength to enamel using universal adhesive systems. J Contemp Dent Pract. 2016;1;17(10):820–825. | ||
Han IH, Kang DW, Chung CH, Choe HC, Son MK. Effect of various intraoral repair systems on the shear bond strength of composite resin to zirconia. J Adv Prosthodont. 2013;5(3):248–255. | ||
Foong J, Lee K, Nguyen C, et al. Comparison of microshear bond strengths of four self-etching bonding systems to enamel using two test methods. Aust Dent J. 2006;51(3):252–257. | ||
Thanaratikul B, Santiwong B, Harnirattisai C. Self-etch or etch-and-rinse mode did not affect the microshear bond strength of a universal adhesive to primary dentin. Dent Mater J. 2016;35(2):174–179. | ||
Bijelic-Donova J, Garoushi S, Lassila LV, Keulemans F, Vallittu PK. Mechanical and structural characterization of discontinuous fiber-reinforced dental resin composite. J Dent. 2016;52(6):70–78. | ||
Sfondrini MF, Massironi S, Pieraccini G, et al. Flexural strengths of conventional and nanofilled fiber-reinforced composites: a three-point bending test. Dent Traumatol. 2014;30(1):32–35. | ||
Dias HB, Carrera ET, de Souza Rastelli AN. The influence of pH and chemical composition of beverages on color stability of a nanofilled composite resin. Gen Dent. 2016;64(6):e21–e27. | ||
Caixeta RV, Guiraldo RD, Kaneshima EN, et al. Push-out bond strength of restorations with bulk-fill, flow, and conventional resin composites. ScientificWorldJournal. 2015;2015:452976. | ||
Imbery TA, Gray T, DeLatour F, Boxx C, Best AM, Moon PC. Evaluation of flexural, diametral tensile, and shear bond strength of composite repairs. Oper Dent. 2014;39(6):E250–E260. | ||
da Costa TR, Serrano AM, Atman AP, Loguercio AD, Reis A. Durability of composite repair using different surface treatments. J Dent. 2012;40(6):513–521. | ||
Wahsh MM, Ghallab OH. Influence of different surface treatments on microshear bond strength of repair resin composite to two CAD/CAM esthetic restorative materials. TDJ. 2015;12(3):178–184. | ||
Rambhia S, Heshmati R, Dhuru V, Iacopino A. Shear bond strength of orthodontic brackets bonded to provisional crown materials utilizing two different adhesives. Angle Orthod. 2009;79(4):784–789. | ||
Thean HP, Chew CL, Goh KI. Shear bond strength of denture teeth to base: a comparative study. Quintessence Int. 1996;27(6):425–428. | ||
Piconi C, Maccauro G. Zirconia as a ceramic biomaterial. Biomaterials. 1999;20(1):1–25. | ||
Agarwal RS, Hiremath H, Agarwal J, Garg A. Evaluation of cervical marginal and internal adaptation using newer bulk fill composites: an in vitro study. J Conserv Dent. 2015;18(1):56–61. | ||
Clelland NL, Pagnotto MP, Kerby RE, Seghi RR. Relative wear of flowable and highly filled composite. J Prosthet Dent. 2005;93(2):153–157. | ||
Caneppele TM, Zogheib LV, Gomes I, Kuwana AS, Pagani C. Bond strength of a composite resin to an adhesive luting cement. Braz Dent J. 2010;21(4):322–326. | ||
Hickel R, Brüshaver K, Ilie N. Repair of restorations – criteria for decision making and clinical recommendations. Dent Mater. 2013;29(1):28–50. | ||
Maneenut C, Sakoolnamarka R, Tyas MJ. The repair potential of resin composite materials. Dent Mater. 2011;27(2):e20–e27. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.