Back to Journals » Patient Preference and Adherence » Volume 16
Shared Decision-Making: A Cross-Sectional Study Assessing Patients Awareness and Preferences in Saudi Arabia
Authors Aljaffary A ![]() , Alsheddi F
, Alsheddi F ![]() , Alzahrani R
, Alzahrani R ![]() , Alamoudi S, Aljuwair M, Alrawiai S
, Alamoudi S, Aljuwair M, Alrawiai S ![]() , Aljabri D
, Aljabri D ![]() , Althumairi A
, Althumairi A ![]() , Hariri B
, Hariri B ![]() , Alumran A
, Alumran A ![]()
Received 10 November 2021
Accepted for publication 28 January 2022
Published 13 April 2022 Volume 2022:16 Pages 1005—1015
DOI https://doi.org/10.2147/PPA.S332638
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
Afnan Aljaffary, Fatimah Alsheddi, Raghad Alzahrani, Somayyah Alamoudi, Mona Aljuwair, Sumaiah Alrawiai, Duaa Aljabri, Arwa Althumairi, Bayan Hariri, Arwa Alumran
Department of Health Information Management & Technology, College of Public Health, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia
Correspondence: Afnan Aljaffary, Email [email protected]
Background and Aim: Shared decision-making (SDM) has become broadly accepted during the consultation, especially when there are many options of treatment. This study aims to assess patients’ levels of awareness and preferences of SDM in Saudi Arabia.
Methods: This is a cross-sectional study targeting patients in Saudi Arabia. Two validated questionnaires were used, the first validated questionnaire focuses on measuring knowledge, attitude and experiences of shared-decision making. The second questionnaire is the the Autonomy‐Preference‐Index focusing on patients’ preferences for being involved in SDM. Relevant items to the study aim were chosen and translated into Arabic. Psychometric testing was conducted for Arabic and English versions and tested for content and face validity. The questionnaire administered online via social media channels, between February 2021 and May 2021. A total of 411 respondents completed the questionnaire.
Results: The findings showed a positive association between awareness and preferences of SDM among patients in Saudi Arabia. In the awareness of the SDM domain, females reported higher scores than male participants (t = − 4.504, P < 0.001). Saudis reported higher scores in their awareness of SDM than non-Saudis (t = 2.569, P = 0.011). Participants without health insurance reported higher scores in their awareness of SDM than those insured (t = − 2.130, P = 0.034). Participants with degree have higher knowledge levels than participants with no degree (f = 10.034, P < 0.001). Females reported higher scores in their preferences of SDM than the male (t = − 2.099, P = 0.036). Participants who visited private health-care settings in their last clinical encounter reported higher preferences of SDM than participants who received care in other settings (f = 2.653, P = 0.048).
Conclusion: The study concludes that the more aware a patient is, the more likely they prefer SDM practice. This finding can support health-care policymakers in developing SDM policies that enhance patient-centered care.
Keywords: awareness, preferences, patients, shared decision-making, Saudi Arabia, treatment plan
Introduction
Shared Decision-Making (SDM) has become broadly the acceptable and preferable approach during consultations, especially when there are many available options of treatment.1 SDM is a process where clinicians and patients discuss together the different options supported by the best available evidence for each treatment, clinical plans, and tests balancing the expected outcomes and risks with patient values and preferences.2–4 Unsurprisingly, SDM is the recommended and preferable approach in a lot of health-care policies around the world. There are policy-related practices that have been developed in 13 countries that are intended to enhance SDM across the health-care field.2 The importance of SDM is that it affects patient satisfaction, quality of delivering healthcare, achieves informed preferences, and ensures that patients are supported to consider various options.3,5–7 Also, patients have the right to be involved in SDM and discuss with their physician about their condition and treatments.3 SDM initiatives alone are insufficient to provide more information to patients. To participate in SDM, patients must have both knowledge and power to be able to choose the best available evidence and decisions for treatment. However, achieving the optimum results from a treatment plan is becoming increasingly dependent on an individual’s knowledge, motivation, and skills, as well as their confidence in using them to manage their health care.8,9 More importantly, many studies have shown that patients who are involved in decision-making processes are more likely to adhere to their treatment plans and be more satisfied, which in turn results in better quality and safety outcomes (eg, patients who were not involved in the treatment plan with their doctor may not meet their medical needs nor their treatment goals).6,7,10–12
Awareness of Shared Decision-Making
Training physicians in the practice of SDM is essential because SDM is a different process from the traditional informed consent approach of simply presenting to patients the potential benefits and risks of an intervention or treatment.13 Studies show that when patients are not involved in decision-making processes, it may be due to the physician’s inability to actively involve patients in treatment plans.14 For example, a study conducted in Spain stated that the implementation of SDM is limited and not utilized.15 They concluded that this is mostly a result of the physicians’ having no training in SDM and therefore, not using it in practice. Thus, strategies to increase training in SDM and to implement it into clinical practice are important.15
On a related note, many patients do not expect to be involved in decision-making because they are not aware that their values and preferences, when well informed, may help determine the most appropriate choice of treatment for them.16 A study by Adisso et al investigated the feasibility, impact, and acceptability of an intervention to raise public awareness of SDM in public libraries.17 The intervention was a 1.5-hour interactive workshop divided into 10 sessions to be presented in public libraries. The study concluded that the intervention was an effective and feasible way to increase the awareness of the public about SDM and could be a new approach to implement SDM by preparing potential patients to ask to be involved in discussions about their care during consultations.17 In conclusion, measuring awareness about SDM is important to know what the next step is in order to achieve SDM. Moreover, because of the sophistication of the communication skills involved in SDM, physicians need appropriate training to ensure they can adequately facilitate the process. Additionally, given the complexity of SDM, its implementation in healthcare will need multifaceted strategies, beginning with increased awareness among professionals, organizations, and patients.18 The more the patients are aware of the value of their involvement in decision-making, the more likely they will be interested to do so.
Preferences in Utilizing Shared Decision-Making
Patients’ preferences regarding their involvement in the clinical decision-making process might vary considerably.19 AlHaqwi et al examined the SDM preferences of patients in Saudi Arabia and discussed three different styles of decision-making;20 the paternalistic approach, ie, an approach in which a physician or other health-care professional makes decisions about a patient without the patient’s express consent,6 the informed consumerism, ie, the rights of the patient to select among available options;21,22 and finally, SDM, which was the most preferred style based on the study conducted in Saudi Arabia.20 Moreover, the study showed that the preference of SDM was significantly higher among those with higher educational levels.20 The results show that patients in Saudi Arabia, in general, had a positive attitude toward the SDM process. This study recommended further investigation of the underlying factors that influence patient SDM preferences to achieve optimal treatment outcomes.20
Various studies investigated patients’ involvement in decision-making and identified barriers and facilitators for SDM in advanced Parkinson’s (Nijhuis et al 2018) and Type 2 Diabetes Mellitus (Bailey et al 2018) from the patient’s perspective.21,23 They found that patients want to be involved and feel involved when choosing an advanced treatment, but often do not know all the available treatment options.21,23 The implementation of true patient involvement, which means patients’ participation and engagement in expressing opinions and making decisions about various treatment options, requires personalized information provision on all treatment options and improvement in how this information is presented and communicated.13,24
In addition, a recent study conducted in Saudi Arabia measured patients’ perceptions of SDM practices during clinical encounters and recommended interventions to enhance the culture of SDM to ensure better adherence to treatment plans and, consequently, better health outcomes.1 The study also highlighted the importance of investigating patients’ expectations and preferences with regard to their involvement in SDM processes and its impact on patients’ health-related decisions.1
Regardless of patients’ preferences, it was found that there was a considerable mismatch between the preferences of the patients in decision-making and what they felt took place in the context of their health consultation. Thus, it is critical to validate patients’ preference types with the actual style of consultation related to healthcare decision-making.25 Finally, patient preferences for being involved in the treatment decision-making may vary from one patient to another, as well as from one treatment condition to another. Moreover, the physicians’ attitudes and how they provide the patient with information while acknowledging the importance of patients’ participation and their inputs could influence patients’ preferences and make them more actively engaged in the treatment decision-making process. The challenge on the physicians lies in allowing the patients to participate in decision-making to the extent they desire.26
Study Implications
The gap in the literature review is that resources are scarce in combining the awareness and preferences of SDM among patients in Saudi Arabia. Therefore, this study assessed the level of awareness and preferences that affect the SDM in a patient’s treatment plan. The study has three research questions which are: “What are the factors affecting patients’ awareness of SDM?”, “What are the patients’ preferences in applying SDM during the clinical encounter?”, and “Is there an association between patients’ awareness and preference of SDM?”. This research on the individual level implies that patients will be more confident and more interested in being involved in decision-making. Moreover, the patients will likely be more satisfied with the SDM. This will lead to an increase in the overall awareness of the SDM of the community and support health-care policymakers to develop SDM policies that enhance patient-centered care.
Materials and Methods
Study Design
This is a quantitative cross-sectional study.
Participants
Patients in Saudi Arabia aged 18 and older were eligible to participate in the study. The convenience sampling technique was used to recruit study participants by circulating an online questionnaire to the public through social media applications. The questionnaire focused on the participants’ most recent doctor visits in the previous six months.
Variables
The dependent variables are awareness and preferences of SDM. While the independent variables are age, educational level, region, gender, living area, nationality, insurance status, marital status, type of the last consultation, type of hospital that is generally used, and the existence of chronic diseases.
Data Sources/Measurement
The data were collected via two validated and existing questionnaires that have been developed through a set of literature searches.40,41 The first questionnaire used has been taken from Mathijssen et al., (2020), which was originally developed to measure knowledge, attitudes and experiences of shared decision making during patient’s visit to the doctor.40 The second part of the study’s survey was derived from Autonomy‐Preference‐Index (API) questionnaire that examined patients’ preferences for involvement in clinical decision-making.41 In this study, the items that were relevant to the study aims and objectives were chosen from these questionnaires and tested using psychometric testing: face validity, linguistic validity, and content validity (see Appendix B).
The questionnaire used in this study consists of 38 items; 12 of them were for demographic data, 13 for the awareness domain, and 13 for the preference domain. The responses for both the awareness and preference domains are on a 5-point Likert scale. The questionnaire also includes one scaled question about the knowledge of SDM.
Three validity tests were conducted, which are content, linguistic, and face validity. Firstly, content validity was conducted by selecting a panel of experts. Researchers have suggested including “content experts,” ie, those who have several publications or work experience in the field and have experience in designing healthcare-related questionnaires.27,28 Using a purposive sampling technique, experts were recruited from the Public Health Department at Imam Abdulrahman Bin Faisal University (IAU). An invitation email was sent to seven experts to engage in a content validity evaluation of the scale. 5 out of 7 experts, with a 50% response rate, responded to the invitation. All participants were female, with long experience in the field (10 years or above). The content validity of the questionnaire was then assessed using content validity index (CVI) techniques.29
Secondly, backward-forward translation was conducted to assess the instrument’s linguistic validity. Finally, face validity was done by recruiting 21 participants from the public. In face validity, the clarity of the wording, ability to answer questions, and the layout and style of the face validity form for both the Arabic and English versions were appraised by the responses, with the result being an out of 4.
Scale Validity Test Findings
The content validity assessment indicated that all items had a reasonable I-CVI score of 0.20 to 1. Most of the questions received a high score as a result of the I-CVI, except for two questions that were removed due to their low score. Following the advice of the expert panel, a few modifications to the questionnaire have been made, including some paraphrasing and deleting of items. The questionnaire items are shown in Appendix A, which shows items before and after the expert panel’s recommendations for changes.
In face validity, the participant’s ratings of the items ranged from 3 to 4. Based on the face validity results, some of the questionnaire items were changed to enhance their clarity. Appendix B shows the final version of the questionnaire items after face validity.
Study Size
The rule of thumb provided by Comrey and Lee was used in this study, where 100 participants = fair, 200 participants = good, 500 participants = very good, and >1000 participants = excellent. The total number of completed surveys in this study was 411 participants.30
Statistical Methods
All numerical data were entered and analyzed using the Statistical Package for Social Sciences (SPSS) version 27. Descriptive analysis was conducted by assessing the measures of frequencies and percentages for categorical variables and the central tendency, ie, mean, for continuous data to assess the univariate analysis. The skewness and kurtosis criteria were used to test the normality of awareness and preferences of SDM variables. The three domains were normally distributed; therefore, parametric tests such as analysis of variance (ANOVA) and t-tests were used to conduct bivariate analyses. Therefore, to reach the final result, a correlation analysis was conducted to find the extent of the association between the dependent variables and independent variables.
The SDM scale has three domains: knowledge about SDM (1 refers to no knowledge and 10 refers to high knowledge), awareness of SDM (1 refers to low awareness and 5 refers to high awareness of SDM), and preferences of SDM (1 refers to low preference and 5 refers to the high preference of SDM). Each domain is calculated by computing the sum of the answers to the questions in that domain, keeping in while reverse scoring the items that required that. For each domain, a higher score indicates better value, ie, a higher score in the knowledge domain indicates better knowledge regarding SDM, a higher score in the awareness domain indicates better awareness regarding SDM, and a higher score in the preference domain indicates a higher preference of SDM.
Results
Main Result
There was a total of 411 participants who completed the questionnaire. According to the normality test of awareness and preferences of SDM variables, the skewness and kurtosis criteria were used. According to these criteria, the three domains are normally distributed. The mean score of the knowledge domain is 4.73 (SD = 3.20), the mean of the awareness domain is 48.8 (SD = 7.46), and the mean of the preferences domain is 46.81 (SD = 5.08). According to the skewness and kurtosis criteria, the three domains are normally distributed.31
Univariate Variables
Most of the participants were between 18 and 24 years old (n = 133, 32.4%). Females made up 74% of the respondents (n = 305). Most of the participants in the study have a bachelor’s degree and above (n = 238, 57.9%). Almost half of the participants are married (n = 230, 56%). 26% of the participants indicated that they always or sometimes have language barriers with their doctor (n = 107, 26%) (Table 1).
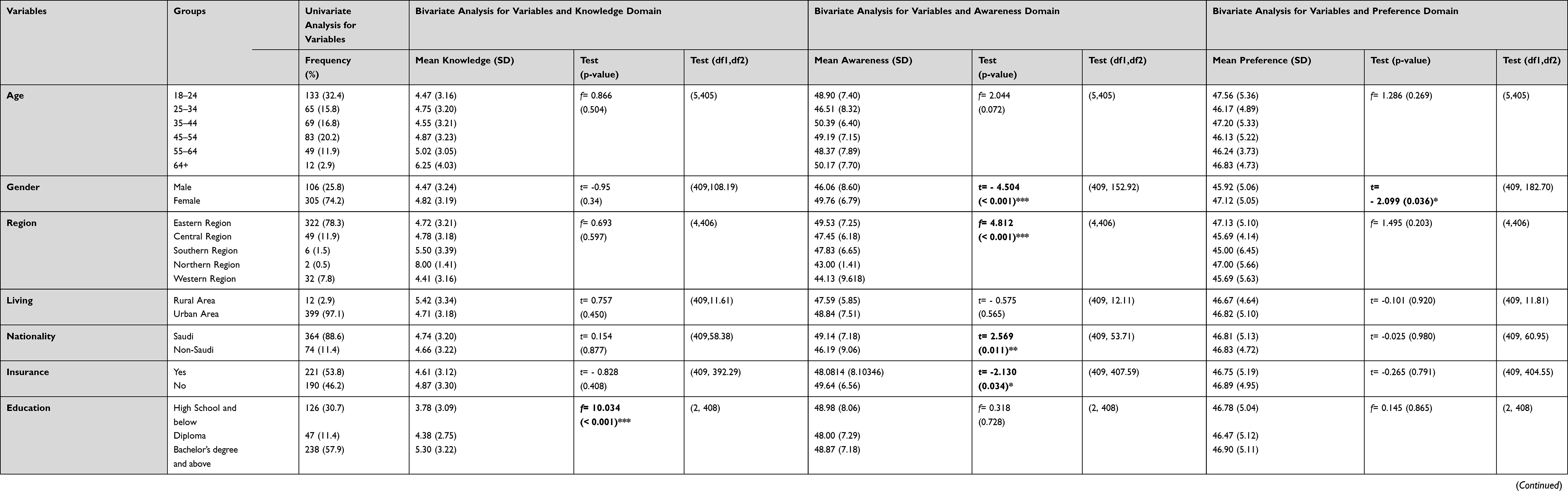 |
Table 1 For Univariate and Bivariate Analysis for Variables |
Many of the participants were from the Eastern Province (n = 322, 78.3%). In addition, almost all participants lived in urban areas (n = 399, 97.1%), and most participants were Saudis (n = 364, 88.6%).
Almost half of the participants had health insurance (n = 221, 53.8%), and most of the participants did not have any chronic disease (n = 294, 71.5%). Almost all participants indicated that their last medical consultation with their doctor was face-to-face (n = 374, 91%) as opposed to an online consultation (n = 37, 9%). Moreover, half of the participants denoted that they usually got their treatment during the past six months in private hospitals (n = 205, 49.9%), and only 5.1% were visited primary care (n = 21) (Table 1).
Bivariate Analysis for Variables and Knowledge Domain
The only variable that significantly influences the participant’s knowledge about SDM is their education level. Participants with a bachelor’s degree or above have significantly higher mean scores in their knowledge about SDM compared with participants with no degree, ie, high school or below, and those with a diploma (f = 10.034, P < 0.001) (Table 1).
Bivariate Analysis for Variables and Awareness Domain
Several variables significantly influence the participant’s scores in awareness about the SDM domain. These are gender, the participant’s region, nationality, and whether they have insurance (Table 1). The mean of awareness of SDM score for the female is significantly higher than males (t = - 4.504, P < 0.001).
Saudi participants have significantly higher mean scores in the awareness of SDM compared to non-Saudis (t = 2.569, P = 0.011). Participants without health insurance had significantly higher mean scores in the awareness of SDM (t = −2.130, P = 0.034). In addition, participants from the eastern region have higher mean scores in the awareness of SDM compared to participants from other regions in Saudi Arabia (f = 4.812, P < 0.001).
Bivariate Analysis for Variables and Preference Domain
As for the final domain, the participant’s gender and the type of hospital where patients received their last medical consultation were significantly influenced participants’ preference of SDM practice (Table 1). Female participants showed higher mean scores in preference of SDM compared to males (t = −2.099, P = 0.036). Also, participants who indicated that their type of organization was a primary health-care setting had significantly lower mean scores in preferences compared to governmental, private, or quasi-government health-care settings (f = 2.653, P = 0.048).
Correlation Between the Three Domains in the Study
Furthermore, correlation analysis between the study domains showed a significant linear correlation between the preference domain and the awareness domain (r = 0.385, P < 0.001) (Table 2).
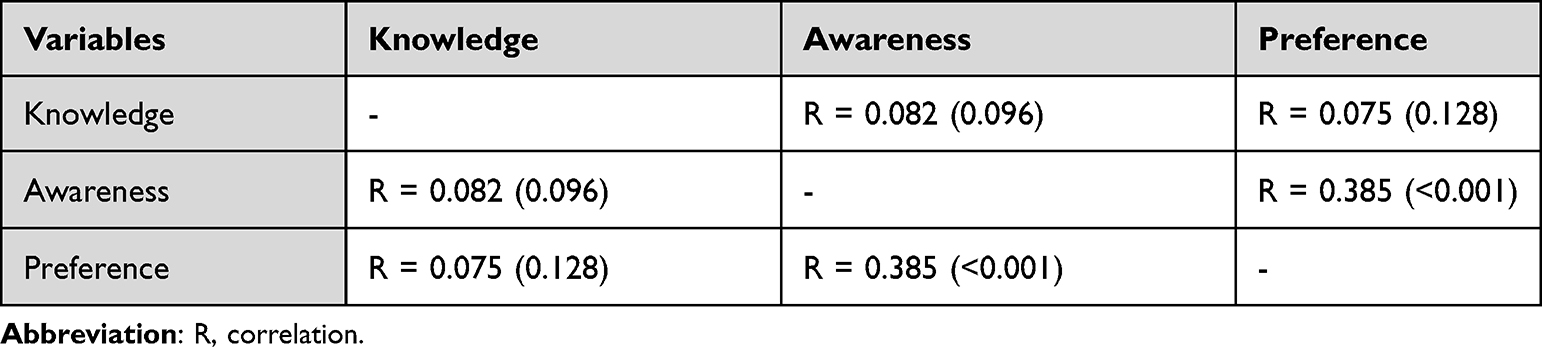 |
Table 2 Correlation Between the Three Domains in the Study |
Discussion
This is the first study that assessed the relationship between awareness and patient preference of SDM. A significant positive relationship was found, the more aware a patient is, the more likely they prefer to be engaged in SDM.
One study used SDM-Q-9 questionnaire and aimed to assess the degree of SDM from urological patients’ perspective and to identify possible predictors.32 The study revealed that, to participate in the decision-making process, patients must be aware of the appropriate clinical decisions that must be made. To fully involve patients, physicians should also consider their participation preferences.32,33 Another study used Ford et al questionnaire.25,34 The study aimed to attain insight into cancer patients’ preferences and the reasons for patients’ preferred role in treatment decision-making at the end of life.34 The study revealed that the patient’s preferences vary according to his/her condition and level.34 However, the results of the present study showed that patients’ preferences for being involved in SDM depend on their awareness.
Regarding the first research question, which is “What are the factors affecting patients’ awareness of SDM in Saudi Arabia?” The results clearly indicate that the four variables that showed a significant difference in the awareness domain, which are gender, participant’s region, nationality, and health insurance status. As for gender, the female participants showed a higher awareness level compared to males. Furthermore, participants living in the eastern region have the highest level of awareness compared to other regions. Saudi participants showed a higher level of awareness about SDM compared to non-Saudis. Participants without health insurance also showed a higher level of awareness about SDM compared to insured participants. The result of this study contradicts the study by Kunneman et al, which stated that there are no significant differences between the awareness of SDM and gender.16 This contradiction might occur because of the fact that the study collected the data using video-recorded clinical encounters, while the current study relied solely on the participants’ subjective judgment about their level of awareness.16
With regard to the association between educational level and awareness level of SDM, Légaré, and Thompson-Leduc findings were aligned with the current study’s result which all of them showed no significance.2 Because of the scarcity of resources tackling the awareness of SDM topic and its association with nationality, region, and insurance variables, it cannot be compared and linked with other studies. This makes this study the first to tackle these variables with the awareness of SDM.
Regarding the knowledge domain, which can be considered as a fundamental part of awareness, the level of education shows a significant relationship with the knowledge domain. Based on the Levinson et al study, the results are consistent with the study results showing the positive relationship between education level and knowledge.35 A study was done by Adisso et al that made interventions to enhance public awareness about SDM using workshops in public libraries and to measure participants’ awareness and knowledge before and after the intervention.17 It demonstrated that before the workshop, participants had little knowledge of SDM (4.7/10). The workshop increased their average level of knowledge by 4.0 (8.7/10). Interestingly, the mean of knowledge before the workshop is the same as the result of the current study.
With regard to the second research question, which is “What are the patients’ preferences in applying SDM during clinical encounters in Saudi Arabia?” Female participants and gender showed significant relations with the preference domain. A study conducted in Saudi Arabia found that female participants reported higher preference scores compared to male participants, which is consistent with this study’s finding.1 Also, this finding may be explained by the fact that female participants are more interested in seeking physical and mental health than male participants.36 Even though Alrawiai et al found that the type of hospital is not significantly associated with the preference of SDM, this study found that it was highly significant in private hospitals.1 This variation can be justified because of the differences in sample size between the two studies, where the current study has a larger sample size, ensuring more valid results.37
In relation to the third research question which is “Is there an association between patients’ awareness and preference of SDM?”. Because of the scarcity of resources and the lack of the previous study that combines the awareness and preferences of SDM among patients in Saudi Arabia. This study was conducted to measure the association between both.
Based on the results, the factors that showed no association with the patients’ level of awareness and preferences in SDM are age, living area, marital status, language barrier, chronic disease, and type of the last consultation.
The lack of association between some of these factors and the patients’ level of awareness and preferences in SDM has been found in many different studies, which demonstrate that age and marital status are not associated with the preference of SDM as shown in Alrawiai et al study.1 Concerning age, the sample size might not have been large enough to detect whether or not there is an association. We assume it is worthwhile to see if our results will be replicated in a wider group of patients regarding different age groups.37,38 Likewise, the Ghodsian et al study emphasizes that there is no significant relationship between the SDM and living areas.10,39 This is likely a result of the variation in the number of responses in the rural area compared to the urban area.37
Bias
Recall bias could have been introduced as the data relies solely on the patients’ recollection of their latest visit to a health facility. The questionnaire was circulated online via a variety of social media platforms, which may have resulted in sample bias by excluding groups with limited Internet access.
Limitation
The findings of this research may have some limitations. Firstly, the practical application of the study is limited as some of the characteristic groups have a low number of participants, such as non-Saudis and participants in the southern and northern regions. This can be explained by the fact that all the researchers in this study lived in the eastern province and most of the participants were from the same province.
Secondly, since the questionnaire was distributed online, elderly and poor patients were less likely to access and participate in the study. Thirdly, the study used a convenience sampling method, resulting in a possibly biased and less reliable sample. All these factors affected the generalizability of the current study. On the other hand, the strong point lies in the large number of responses, which are 411 participants in the study’s questionnaire.
Conclusion
To conclude, the study aims to measure the awareness and preferences of SDM among patients in Saudi Arabia. The current research found a significant linear association between SDM’s awareness and preference, which indicates that the more aware a patient is, the more they will prefer applying SDM in clinical encounters. While the knowledge showed no correlation with awareness nor preference of SDM.
We hope this would further lead to new researches and investigations, resulting in implementing new interventions and policies to promote SDM practice during the health-care journey and thus better adherence to treatment plans, which might positively affect health outcomes in KSA. This is especially important as the Saudi healthcare system is shifting to privatization and the new model of care currently being implemented in KSA focuses on patient-centered care.
It is recommended to consider conducting a qualitative study in the future in order to dig deeper into the reasons for patients’ preferences of SDM. Moreover, it is recommended to aid health-care professionals, especially doctors, in implementing SDM in clinics through means such as SDM checklists, educational brochures targeting patients, or establishing workshops to enhance doctors’ level of knowledge in applying the SDM concept in their practice.14,17
Declaration
This study was conducted in accordance with the Declaration of Helsinki.
Ethical Approval
Ethical approval was obtained from the institutional review board at Imam Abdulrahman Bin Faisal University [IRB-UGS-2021-03-024]. Written informed consent was obtained at the beginning of the survey.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Alrawiai S, Aljaffary A, Al-Rayes S, Alumran A, Alhuseini M, Hariri B. The OPTION scale: measuring patients’ perceptions of shared decision-making in the Kingdom of Saudi Arabia. J Multidiscip Healthc. 2020;13:1337–1346. doi:10.2147/JMDH.S273340
2. Légaré F, Thompson-Leduc P. Twelve myths about shared decision making. Patient Educ Couns. 2014;96(3):281–286. doi:10.1016/j.pec.2014.06.014
3. Elwyn G, Frosch D, Thomson R, et al. Shared decision making: a model for clinical practice. J Gen Intern Med. 2012;27(10):1361–1367. doi:10.1007/s11606-012-2077-6
4. Health Information Technology (Health IT). Shared decision making; 2013. Available from: https://www.healthit.gov/sites/default/files/nlc_shared_decision_making_fact_sheet.pdf.
5. NICE. Shared decision making; 2016. Available from: https://www.nice.org.uk/about/what-we-do/our-programmes/nice-guidance/nice-guidelines/shared-decision-making.
6. Bot AG, Bossen JK, Herndon JH, Ruchelsman DE, Ring D, Vranceanu AM. Informed shared decision-making and patient satisfaction. Psychosomatics. 2014;55(6):586–594. doi:10.1016/j.psym.2013.12.013
7. Oshima Lee E, Emanuel EJ. Shared decision making to improve care and reduce costs. N Engl J Med. 2013;368(1):6–8. doi:10.1056/NEJMp1209500
8. Mavis B, Holmes Rovner M, Jorgenson S, et al. Patient participation in clinical encounters: a systematic review to identify self‐report measures. Health Expect. 2015;18(6):1827–1843. doi:10.1111/hex.12186
9. Bunn F, Goodman C, Russell B, et al. Supporting shared decision making for older people with multiple health and social care needs: a realist synthesis. BMC Geriatr. 2018;18(1):165. doi:10.1186/s12877-018-0853-9
10. Godolphin W. Shared decision-making. Healthc Quart. 2009;12:e186–e190. doi:10.12927/hcq.2009.20947
11. A.H.R.Q. Shared decision making to improve patient safety, education, and empowerment. AHRQ.Gov; 2016. Available from: https://www.ahrq.gov/sites/default/files/wysiwyg/professionals/quality-patient-safety/patient-family-engagement/pfeprimarycare/shareddec-1.pdf.
12. Chewning B, Bylund CL, Shah B, Arora NK, Gueguen JA, Makoul G. Patient preferences for shared decisions: a systematic review. Patient Educ Couns. 2012;86(1):9–18. doi:10.1016/j.pec.2011.02.004
13. Nelson WA, Donnellan JJ, Elwyn G, Edwards A, Thomson R. Implementing shared decision making: an organizational imperative. Shared decision making in health care: achieving evidence-based patient choice. 2016:3.
14. Coulter A. National strategies for implementing shared decision making (48th and 19 ed. ed.) [E-book]; 2018. Available from: https://www.bertelsmann-stiftung.de/fileadmin/files/Projekte/Patient_mit_Wirkung/VV_Studie_National_Strategies_SDM_en_final.pdf.
15. Padilla Garrido N, Aguado Correa F, Bayo Lozano E, Bayo Calero J, Ortega Moreno M. Physicians’ awareness and assessment of shared decision making in oncology practice. Spanish Magaz Public Health. 2019;93:e201910066.
16. Kunneman M, Branda ME, Hargraves I, Pieterse AH, Montori VM. Fostering choice awareness for shared decision making: a secondary analysis of video-recorded clinical encounters. Mayo Clin Proc. 2018;2(1):60–68. doi:10.1016/j.mayocpiqo.2017.12.002
17. Adisso EL, Borde V, Saint-Hilaire MÈ, et al. Can patients be trained to expect shared decision making in clinical consultations? Feasibility study of a public library program to raise patient awareness. PLoS One. 2018;13(12):e0208449. doi:10.1371/journal.pone.0208449
18. Stiggelbout AM, Van der Weijden T, De Wit MP, et al. Shared decision making: really putting patients at the centre of healthcare. BMJ. 2012;344. doi:10.1136/bmj.e256
19. Bailo L, Vergani L, Pravettoni G. Patient preferences as guidance for information framing in a medical shared decision-making approach: the bridge between nudging and patient preferences. Patient Prefer Adherence. 2019;13:2225–2231. doi:10.2147/PPA.S205819
20. AlHaqwi AI, AlDrees TM, AlRumayyan A, et al. Shared clinical decision making. A Saudi Arabian perspective. Saudi Med J. 2015;36(12):1472–1476. doi:10.15537/smj.2015.12.13682
21. Bailey RA, Shillington AC, Harshaw Q, Funnell MM, VanWingen J, Col N. Changing patients’ treatment preferences and values with a decision aid for type 2 diabetes mellitus: results from the treatment arm of a randomized controlled trial. Diabetes Ther. 2018;9(2):803–814. doi:10.1007/s13300-018-0391-7
22. Weber K. Is informed consumerism your biggest marketing problem? Response Mine Health; 2018. Available from: https://responseminehealth.com/2018/02/08/informed-consumerism-biggest-marketing-problem/.
23. Nijhuis F, van den Heuvel L, Bloem BR, Post B, Meinders MJ. The patient’s perspective on shared decision-making in advanced parkinson’s disease: a cross-sectional survey study. Front Neurol. 2019;10:896. doi:10.3389/fneur.2019.00896
24. Stacey D, Légaré F, Lewis K, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2017;4(4):CD001431. doi:10.1002/14651858.CD001431.pub5
25. Ford S, Schofield T, Hope T. Are patients’ decision-making preferences being met? Health Expect. 2003;6(1):72–80. doi:10.1046/j.1369-6513.2003.00211.x
26. Flynn KE, Smith MA, Vanness D. A typology of preferences for participation in healthcare decision making. Soc Sci Med. 2006;63(5):1158–1169. doi:10.1016/j.socscimed.2006.03.030
27. Rungtusanatham M. Let’s not overlook content validity. Decision Line, 29, 10–13. - References - Scientific Research Publishing. Scientific Research; 1998. Available from: https://www.scirp.org/(S(351jmbntvnsjt1aadkposzje))/reference/ReferencesPapers.aspx?ReferenceID=741316.
28. Rubio D, Berg-Weger M, Tebb SS, et al. Objectifying content validity: conducting a content validity study in social work research. Soc Work Res. 2003;27(2):94–104. doi:10.1093/swr/27.2.94
29. Rodrigues IB, Adachi JD, Beattie KA, MacDermid JC. Development and validation of a new tool to measure the facilitators, barriers and preferences to exercise in people with osteoporosis. BMC Musculoskelet Disord. 2017;18. doi:10.1186/s12891-017-1914-5
30. Comrey AL, Lee HB. A First Course in Factor Analysis. Hillsdale, NJ: Erlbaum; 1992.
31. West SG, Finch JF, Curran PJ. Structural equation models with nonnormal variables: problems and remedies. Curran Web; 1995. Available from: https://curran.web.unc.edu/wp-content/uploads/sites/6785/2015/03/WestFinchCurran1995.pdf.
32. Grüne B, Köther AK, Büdenbender B, Michel MS, Kriegmair MC, Alpers GW. Patients’ perspective on shared decision-making in urology: a prospective study at a university hospital. World J Urol. 2021;39(12):4491–4498. doi:10.1007/s00345-021-03794-3
33. Stacey D, Hill S, McCaffery K, Boland L, Lewis KB, Horvat L. Shared decision making interventions: theoretical and empirical evidence with implications for health literacy. Stud Health Technol Inform. 2017;240:263–283.
34. Brom L, Pasman HRW, Widdershoven GAM, et al. Patients’ preferences for participation in treatment decision-making at the end of life: qualitative interviews with advanced cancer patients. PLoS One. 2014;9(6):e100435–e100435. doi:10.1371/journal.pone.0100435
35. Levinson W, Kao A, Kuby A, Thisted RA. Not all patients want to participate in decision making: a national study of public preferences. J Gen Intern Med. 2005;20(6):531–535. doi:10.1111/j.1525-1497.2005.04101.x
36. Thompson AE, Anisimowicz Y, Miedema B, Hogg W, Wodchis WP, Aubrey-Bassler K. The influence of gender and other patient characteristics on health care-seeking behaviour: a QUALICOPC study. BMC Fam Pract. 2016;17(1):38. doi:10.1186/s12875-016-0440-0
37. Faber J, Fonseca LM. How sample size influences research outcomes. Dental Press J Orthod. 2014;19(4):27–29. doi:10.1590/2176-9451.19.4.027-029.ebo
38. Hamelinck VC, Bastiaannet E, Pieterse AH, van de Velde C, Liefers GJ, Stiggelbout AM. Preferred and perceived participation of younger and older patients in decision making about treatment for early breast cancer: a prospective study. Clin Breast Cancer. 2018;18(2):e245–e253. doi:10.1016/j.clbc.2017.11.013
39. Ghodsian S, Ghafourifard M, Ghahramanian A. Comparison of shared decision making in patients undergoing hemodialysis and peritoneal dialysis for choosing a dialysis modality. BMC Nephrol. 2021;22(1):67. doi:10.1186/s12882-021-02269-2
40. Mathijssen, E.G., van den Bemt, B.J., Wielsma, S., van den Hoogen, F.H. and Vriezekolk, J.E., 2020. Exploring healthcare professional’s knowledge, attitudes and experiences of shared decision making in rheumatology. RMD open. 6(1):p.e001121.
41. Simon, D., Kriston, L., Loh, A., Spies, C., Scheibler, F., Wills, C. and H rter, M., 2010. Confirmatory factor analysis and recommendations for improvement of the Autonomy-Preference-Index (API). Health expectations. 13(3):pp.234-243.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.