Back to Journals » Psychology Research and Behavior Management » Volume 15
Sexual Function, Self-Esteem, and Quality of Life in Infertile Couples Undergoing in vitro Fertilization: A Dyadic Approach
Authors Wang JY, Lv XQ, Wu JM, Tang WQ, Luo GY, Liang CM, Wang DN, Hong JF, Cao YX
Received 25 June 2022
Accepted for publication 29 August 2022
Published 6 September 2022 Volume 2022:15 Pages 2449—2459
DOI https://doi.org/10.2147/PRBM.S378496
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Igor Elman
Jie-Yu Wang,1,2 Xiao-Qing Lv,2 Jing-Mei Wu,2 Wang-Qin Tang,2 Gui-Ying Luo,1 Chun-Mei Liang,1 Dan-Ni Wang,3 Jing-Fang Hong,2 Yun-Xia Cao1,4,5
1Reproductive Medicine Center, Department of Obstetrics and Gynecology, The First Affiliated Hospital of Anhui Medical University, Hefei, People’s Republic of China; 2School of Nursing, Anhui Medical University, Hefei, People’s Republic of China; 3Teaching Center for Preventive Medicine, School of Public Health, Anhui Medical University, Hefei, People’s Republic of China; 4NHC Key Laboratory of Study on Abnormal Gametes and Reproductive Tract, Hefei, People’s Republic of China; 5Key Laboratory of Population Health Across Life Cycle (Anhui Medical University), Ministry of Education of the People’s Republic of China, Hefei, People’s Republic of China
Correspondence: Jing-Fang Hong; Yun-Xia Cao, Email [email protected]; [email protected]; [email protected]
Purpose: Infertility has adverse effects on the quality of life (QoL) of infertile couples. Previous studies found important associations between sexual function, self-esteem and QoL, but mainly focused on one individual’s approach rather than both partners. This study adopted a dyadic approach to evaluate the relationship between sexual function and QoL in couples with infertility through mediation and improving self-esteem.
Patients and Methods: Between October 2020 and January 2021, 428 couples with infertility (n=856) undergoing in-vitro fertilization (IVF) at a tertiary hospital in Hefei, China, were registered for the current descriptive cross-sectional research. The dyads’ sociodemographic and clinical features, as well as their sexual function, self-esteem, and QoL were evaluated. The Fertility quality of life scale (FertiQoL), Rosenberg Self-Esteem Scale (RSES), Female Sexual Function Index (FSFI), and International Index of Erectile Function-15 (IIEF-15) were used to evaluate the participants. The Actor-Partner Interdependence Mediation Model (APIMeM) was utilized to examine data from the dyadic relationships.
Results: According to the APIMeM analysis, sexual function of individuals with infertility was directly and indirectly connected with their QoL, mediated through their self-esteem. The women’s sexual function was found to be positively associated with their partner’s QoL, with the women’s self-esteem acting as a complete mediator. The men’s sexual function was found to be positively associated with partner’s QoL, with the men’s self-esteem acting as a complete mediator.
Conclusion: The findings suggest that boosting participants’ self-esteem can help them and their partners have a better QoL. Also, therapies aimed at improving and sustaining self-esteem of couples with infertility could help mitigate the negative influence of low sexual function on their QoL.
Keywords: in-vitro fertilization, dyad, quality of life, self-esteem, sexual function
Introduction
Infertility is defined by the World Health Organization (WHO) as a reproductive system disorder, characterized by the inability to conceive following 12 months or more of intercourse without contraception.1 It has evolved into a global public health concern that endangers public health and affects over 50 million couples (8–12%) worldwide.2 Many couples seek assisted reproductive technology (ART) after being diagnosed with infertility; hence, the number of couples with infertility seeking in-vitro fertilization (IVF) processing has been steadily rising across the world.3 Based on the Chinese Society of Reproductive Medicine survey, the count of IVF cycles in China has topped 0.32 million, which comprises data from 263 reproductive clinics.4
Quality of life (QoL) is a person’s assessment of his or her current situation in life, as seen through the perspective of their own cultural and societal value systems.5 Anxiety, sadness, insomnia, and eating disorders are just few of the mental health issues that can arise as a result of infertility treatment.6 It is also essential to emphasize that IVF is a lengthy procedure, and its consequences are unpredictable Many people with infertility who have tried IVF have gone through multiple diagnostic procedures and have had therapeutic failures that left them feeling discouraged, adding to their psychological impact. Couples with infertility who pursue IVF have been demonstrated to have a low QoL.7 Many factors including physiological, psychological, and social factors would affect the QoL of individuals with infertility.8–10
First, it has been shown that lower QoL is linked to sexual dysfunction.11,12 Studies have also found that sexual satisfaction and sexual activity were positively correlated with infertiles’ QoL.13,14 For example, Camil et al have confirmed that the decrease in the QoL was related with disorders in the sexual sphere of women with polycystic ovary syndrome (PCOS) which is one of the most common infertility diseases.15 Second, self-esteem has a wide-ranging and far-reaching impact on health.16 The integrative theoretical framework of the effects of self-esteem on health and well-being suggests that high self-esteem, combined with adaptive processes to gain and maintain self-esteem, can promote overall health outcomes.17 There is a considerable association between infertile couples’ QoL and self-esteem.13 Besides, in previous studies, it was found that infertile individuals tended to have lower self-esteem.18 Further, sex and self-esteem have been found to be significantly related.19 According to the sociometer theory, individuals’ self-esteem is a reflection of their existing social interactions, and if they satisfy another individual’s relationship benchmark (such as, by means of sexual behavior), they feel higher level of self-esteem.20 However, there are rarely study on the relationship between sexual function and self-esteem in couple with infertility.
With the rise of positive psychology, several studies have delved into the positive psychological factors of individuals. Self-esteem is an individual’s evaluation of his or her own value.21 Self-esteem can be used as a mediator variable to alleviate the risk factors caused by infertility. For example, Cui et al found that self-esteem can mediate the effects of infertility, such as stress, depression, and anxiety.21 Self-esteem can also act as a mediator to buffer the impact of the physiological indicators of QoL. Treating migraine and tension-type headache in adolescents can lead to an improved QoL as a result of increased self-esteem.22 The degree of self-esteem of individuals with infertility may influence the link between physiological parameters and QoL; that is, the effect of sexual function on QoL in these individuals may be influenced by their level of self-esteem.
The interdependence theory considered a strong interpersonal engagement between two individuals in a close relationship.23 According to Kenny et al, a person’s behavior in a relationship is influenced by their partner’s behavior.23 They anticipated that a person’s behaviour, mood, or intellect can readily be communicated on a dual level, with long-term implications for both partners’ health. Some studies on infertility have even begun to explore the association between husbands and wives.24,25 As such, in studies on infertility, the interaction between a husband and wife should be discussed as a couple and not as individuals.26
To date, previous literature has not yet linked these three variables (sexual function, self-esteem, and QoL) in patients with infertility from a dyadic perspective. Moreover, there are no empirical studies exploring whether the sexual function of women and men with infertility is associated with their own and their partners’ QoL, directly or indirectly, through the mediation of their self-esteem by adopting a dyadic approach using the Actor-Partner Interdependence Mediation Model (APIMeM). Further studies exploring the above-mentioned dyadic relationships in couples with infertility are warranted, and the present study was conducted with this aim.
Materials and Methods
Design and Participants
The convenience sample approach was used to perform cross-sectional research on couples with infertility in Anhui province, China. The Assisted Reproductive Center Clinic of a tertiary hospital in Hefei randomly chose 428 dyad samples between October 2020 and January 2021 to answer a structured, self-reported survey questionnaire. Couples who were diagnosed with infertility based on the WHO definition and were undergoing IVF therapy were involved in this research.1 The exclusion criteria included (a) disorders that may influence sexual function, (b) usage of medicines or psychiatric medications that may interfere with sex life, and (c) ongoing therapy for sexual difficulties. The sample size was calculated using the following formula: n=Z2α/2σ2/δ2 (α=0.05, Zα/2=1.96).27 Before the formal survey of this study, a pre-survey was conducted with 30 dyads samples. The mean score of QoL in the pre-survey were 52.39 and a standard deviation (SD) of 24.69. Based on the QoL score of preliminary survey data, a sample size of 342 was determined to be sufficient for the current investigation, with a σ (ie, the variance of population) of 24.69 and a δ (ie, permitted error) of 5% of the average score (52.39) with n =1.962* 24.692/(52.39*0.05)2=342. Using a 20% non-response rate as a guide, a sample size of 428 was determined to be adequate. In total, 452 dyads of couples with infertility were approached, 15 dyads refused (due to lack of interest, being busy with IVF treatment, or no reason given) to participate and nine were eliminated due to unsatisfactory questionnaire responses (five had missing data in the questionnaire and four had same answers to the whole questionnaire). As a result, 428 couples with infertility took part in the study and completed the questionnaires.
Participants were recruited via convenience sampling method. Data collection was performed by a trained researcher at the reproductive center clinic. The study staff described the survey’s objective, and participants were asked to participate voluntarily, anonymously, and confidentially. Before the collection of data, each participant signed an informed consent form. The questionnaire was encoded and provided directly to the participants by researchers using standardized instructions, and when necessary, the questionnaire items were explained to the participants. It took 10–15 min for the participants to complete the questionnaire. The questionnaire was completed independently by each partner. Either husbands and/or wives failed to complete the questionnaire or choose the same options in the whole questionnaire, the questionnaire would be eliminated in dyads.
Measures
Sociodemographic and Clinical Features
The self-reported questionnaires included information on sociodemographic factors and clinical characteristics, which consisted of age; duration of marriage; level of education; status of occupation; period, cause, and type of infertility, and whether the couple had living children.
Fertility Quality of Life Scale (FertiQoL)
The FertiQoL scale was utilized to assess the QoL of couples with infertility.28 The FertiQoL scale, developed by the European Society for Human Reproduction and Embryology and the American Society for Reproductive Medicine in 2011, is the gold standard for assessing QoL associated with fertility among individuals with infertility. The Chinese version of FertiQoL, which has excellent validity and reliability in Chinese populations, can be downloaded from http://www.fertiqol.org/.29 It is divided into two sections: treatment-FertiQoL and core-FertiQoL. The FertiQoL questionnaire contains 34 items classified as mind-body, emotional, social, tolerance, relational, and environmental. A 5-point Likert scale with a range of 0 to 4 was used, which was mathematically transformed to a 0–100 scale. Increased scores suggested a better QoL. Herein, Cronbach’s alpha coefficients of the FertiQoL for women and men were 0.898 and 0.907, respectively.
Rosenberg Self-Esteem Scale (RSES)
The RSES was designed by Rosenberg in 1965 to identify subjective emotions of self-importance and self-worth in individuals.30 The Chinese version of RSES was translated by Chen.31 It is a self-assessment instrument comprising ten items. It has been graded on a Likert scale of 1–4 on a 4-point scale. The overall score is between 10 and 40, with one item counted in reverse. A greater total score suggests a higher sense of self-worth. The Chinese version of this scale has been psychometrically assessed, with a Cronbach’s alpha of 0.83–0.89 indicating high reliability.31 Cronbach’s alpha coefficient of self-esteem in our study for women and men was 0.836 and 0.870, respectively.
Female Sexual Function Index (FSFI)
Rosen et al developed the FSFI for evaluating sex functionality in heterosexual women over the preceding 4 weeks.32 It is a self-assessment questionnaire consisting of 19 items that identify satisfaction, discomfort, orgasm, lubrication, arousal, and sexual desire. Four items contain five response options and are reverse-scored (5–1 points); the remaining items are scored on a six-point Likert scale (0–5 points). For each dimension, the score is calculated by multiplying the score for each item by the factor weight. The higher the score, the more is the sexual function. Sun et al translated and validated a reliable Chinese version of the scale with a Cronbach’s alpha coefficient of 0.69–0.94.33 Cronbach’s alpha coefficient for women’s sexual function was 0.974 in our study.
International Index of Erectile Function (IIEF)-15
The IIEF was developed by Rosen et al to assess men’s sex functionality.34 The index is primarily used to assess men’s erectile performance over the preceding 4 weeks. It has 15 items assessing five characteristics of male erectile function namely: intercourse satisfaction, overall satisfaction, sexual desire, orgasmic function, and erectile function. The first five items are assessed on a 5-point Likert scale (1–5), while the rest assessed on a 6-point Likert scale (0–5). The overall score is between 5 and 75. A higher score reflects improved sexual function. The Chinese version of the IIEF is valid and reliable, with a Cronbach’s alpha coefficient of 0.83.35 Cronbach’s alpha coefficient for men’s sexual function was 0.956 in our study.
Statistical Analysis
Data analysis was performed using Mplus version 8.3 (USA) and SPSS version 26.0 (USA). Sociodemographic and clinical features were described via descriptive statistics. Pearson correlations were calculated between the research variables in couples with infertility. The APIMeM was employed for investigating the relationship sexual function (independent variables), self-esteem (possible mediator variables), and QoL (findings variables) between women and men with infertility. The variables pertaining to the women and men were distinguishable dyads. The APIMeM enables estimation of the direct effects of the infertile individuals’ independent variables on their own and their partners’ findings variables, as well as the indirect effects on their own and their partners’ possible mediator variables.
In our investigation, structural equation modeling (SEM) was carried out utilizing the maximum likelihood robust estimation approach. Additionally, the SEM is the most straightforward data assessment approach for APIMeM evaluations, which is helpful since it enables the incorporation of constraint models into the APIMeM framework.36 The bootstrap approach was utilized to determine direct and indirect impacts.37 Based on 5000 bootstrap samples, we assessed bias-corrected 95% confidence intervals (CI) for the unstandardized influences.38 To determine the model’s fit, the following indices were utilized: Chi-square to the degree of freedom ratio (χ2/df)≤3, Comparative Fit Index (CFI)>0.95, Tucker–Lewis Index (TLI)>0.90, and standardized root-mean-square residual (SRMR)<0.08.38
Before the calculation, the assessment invariance between biological sexes was tested using path constraint, and female and male path sets were confirmed to be equal. To calculate the path coefficients for men and women with infertility, considerable chi-square variances between the free prediction and comparable constraint models were determined. The p<0.05 was regarded as statistically considerable.
Results
Features of Participants
Table 1 summarises the individuals’ sociodemographic and clinical features. The mean age of the subject women was 31.00 (SD = 1.24) while the mean age of the subject men was 32.42 (SD = 5.19) years. The majority of the women (50.9%) and men (52.3%) demonstrated a higher education than a college degree. Over half of the women (52.3%) were jobless, whereas over eighty percent of the men (81.5%) were working. Marriage lasted 5.27 years (SD = 3.61) and infertility period was 4.44 years (SD = 3.21). Female factor infertility accounted for 46.3%.
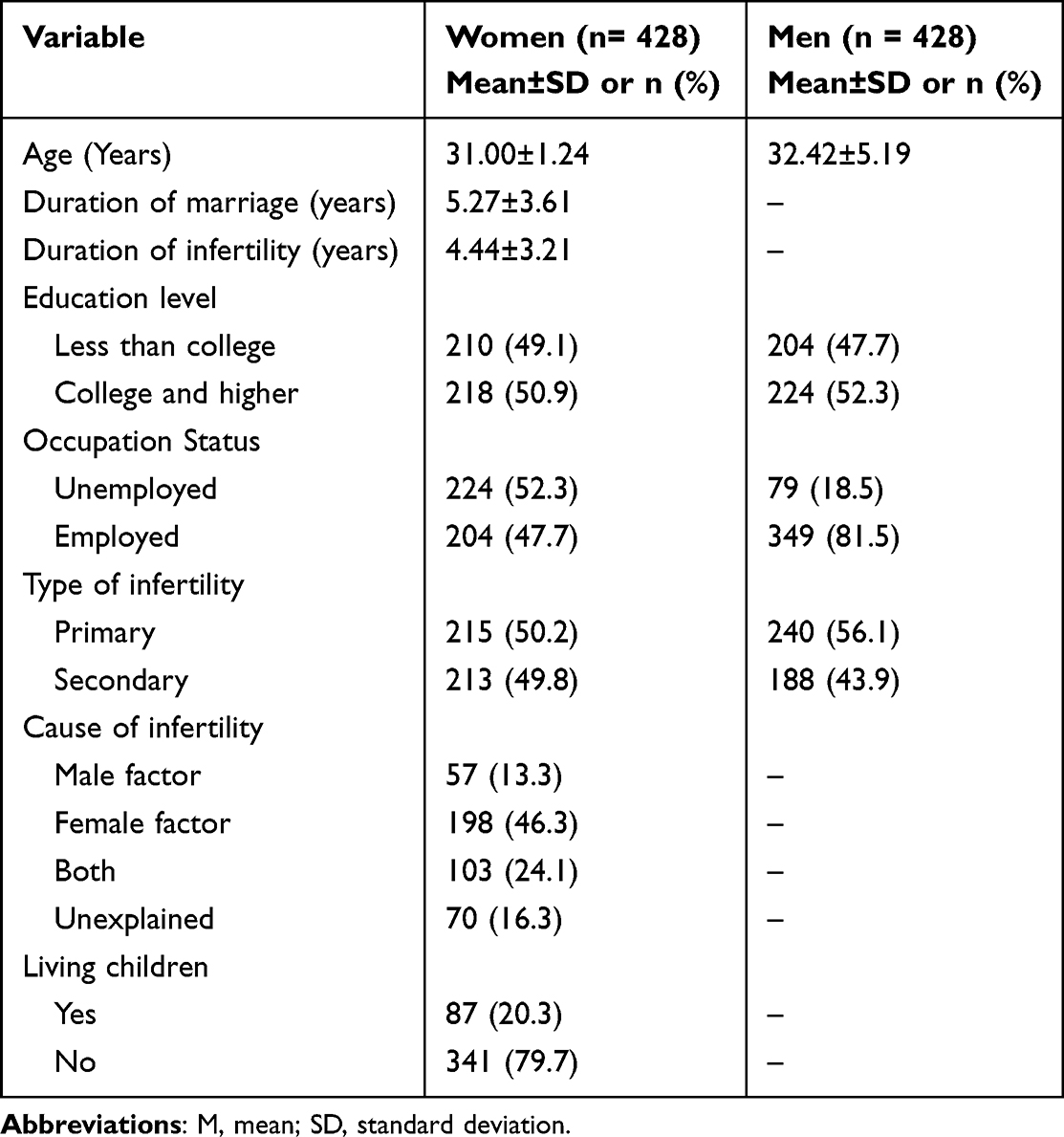 |
Table 1 Sociodemographic and Clinical Characteristics of the Couples (n = 428) |
Table 2 shows that each variable was considerably linked (r = 0.10–0.56, p<0.05) except for the men’s sexual function with women’s QoL, the men’s sexual function with women’s self-esteem, and women’s sexual functions with men’s self-esteem (according to Pearson’s correlation analysis). Women’s self-esteem was similar to their men’s self-esteem (Table 3), but the QoL was significantly worse for women than for men (t(428) = −5.795, p<0.001).
 |
Table 2 Pearson’s Correlations of the Study Variables (n = 428) |
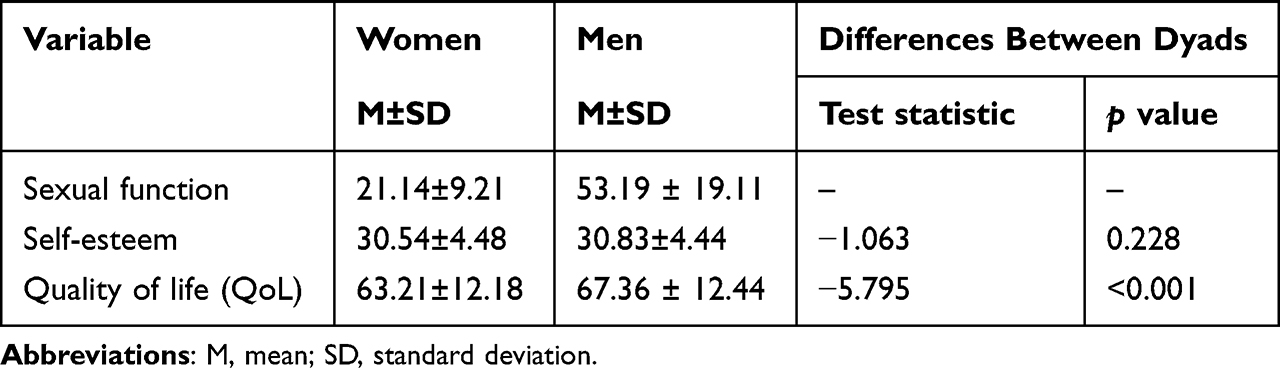 |
Table 3 The Mean Values, Paired-Samples Differences, Between Infertile Women and Men in Sexual Function, Self-Esteem, and QoL (n =428) |
APIMeM Analyses
The non-meaningful chi-square variation between the restricted model and the free estimation model was used to identify measurement invariance between biological sexes (Δχ2 (6) = 4.62, p>0.05). In the APIMeM, both actor and partner influences were limited to be equal, and the suggested model fit the data well: χ2/df = 2.55, CFI = 0.953, TLI= 0.934, SRMR = 0.072.
Figure 1 depicts the path estimations. Actor effects from sexual function of women and men with infertility to their own QoL, their self-esteem to their own QoL were found. Actor effects from sexual function of women and men with infertility to their own self-esteem were also found. Partner effect was found from self-esteem of individuals with infertility to their partner’s QoL.
 |
Figure 1 The Actor-Partner Interdependence Mediation Model of sexual function on QoL through self-esteem. Standardized path estimates and standard errors are reported. Dotted lines represent nonsignificant paths. ***p <0 0.001. |
Indirect effects are reported in Table 4. The sexual function of women and men with infertility was linked with their own QoL through the partial mediating effect of their own self-esteem. The men’s sexual function was linked with their partner’s QoL through the complete mediating effect of men’s self-esteem. The women’s sexual function was linked with their partner’s QoL through the complete mediating effect of women’s self-esteem.
 |
Table 4 Total, Direct, and Indirect Effects in the APIMeM |
Discussion
The present study is based on the sociometer theory and the effects of self-esteem on health and well-being integrative theoretical framework. It aims to determine the association between sexual functions and QoL in infertility-affected couples through a dyadic approach and to clarify the strategies through which sexual functions may influence QoL via self-esteem.
Reported investigations have indicated that women with infertility had lower self-esteem than men with infertility;39 however, there were no significant differences in self-esteem scores between women and men with infertility in this research. This could be due to the fact that the women with infertility in our study had higher levels of education, as previous studies have shown that education levels are positively connected with self-esteem levels.40 In addition, the self-esteem of individuals from different cultural environments differs. In western culture, individuals are unique and have an separate sense of identity, while Chinese self-esteem not only involves individuals, but also others closely related to the individuals, such as wives or husbands, having to share honor and disgrace.41 Thus, the self-esteem of wives and husbands are similar. In comparison to a prior study, both women and men in our study had lower QoL scores.42 Cultural factors may have played a role in this. In China, the concept of family inheritance is deeply rooted. Children are an important part of maintaining family stability. Childlessness would lead to poor QoL. Furthermore, in this study, women’s QoL was lower than that of men, which was consistent with prior research findings.43,44 This may be because men see infertility as a generic problem, but women see it as a major life setback.45 Furthermore, studies indicated that women with infertilty are more impacted by stressful events including IVF processing failure and financial pressures, which can lead to a decrease in their QoL.46 The QoL is related to psychological factors, such as depression with the level of depression of the husbands lower than that of the wives.47 Therefore, the QoL of the husbands was higher than that of the wives.48 These findings emphasize the importance of implementing tailored treatments to enhance QoL in the influenced populations.
This is the first research to utilize the APIMeM model in examining the mediating roles of self-esteem in the association between QoL and sexual functions in couples with infertility. According to our findings, both men and women had a positive impact on their QoL via their self-esteem. Reported research has backed up the findings of our investigation. Individuals with lower sexual function are more anxious, according to a study by Youseflu et al, which has an indirect effect on self-esteem, and eventually on QoL.49 Based on the sociometer hypothesis, self-esteem is an internal reflection of one’s interpersonal interaction with others.50 The stronger an individual’s self-esteem is, the more accepted and liked they are by others. On the other hand, when a person has interpersonal relationship issues, his or her self-esteem as a sociometer drops, generating a negative emotional response and so reducing quality of relationship.50 As a result, patients with low sexual function may find it difficult to be accepted or liked by their partners, thereby lowering their self-esteem. Low self-esteem can lead to bad emotional experiences, which can lead to a lower QoL.13,51
We observed that sexual functions of women with infertility positively influenced men’s QoL via the women’s self-esteem and that sexual functions of men with infertility positively influenced women’s QoL via the men’s self-esteem. This finding could suggest that couples with infertility undergoing IVF treatment have a similar process by which sexual functions affects QoL via self-esteem. This contrasts with prior results showing sexual function of couples with infertility influenced their own and their partner’s QoL.7 Furthermore, we found that the influence of an infertile person’s sexual function on their partners’ QoL was entirely mediated by the person’s self-esteem. Individuals with infertility with better sexual function had higher self-esteem, which was linked to their spouses’ QoL. Türkben et al (2021) had found that sexual QoL has a positive correlation with self-esteem.52 Self-esteem, as a positive psychological state, affects not just an individual’s QoL but also that of their partners, as demonstrated in a study by Ha et al (2020) which found that positive psychological characteristics have actor and partner effects on couples with infertility.53 Furthermore, people with higher self-esteem have better social acceptability and interpersonal relationships.51 As a result, self-esteem is vital in assisting people to maintain positive interpersonal interactions.50 In addition, partners receive more social support, resulting in a higher QoL.54 Health care providers may want to consider ways to improve a client’s self-esteem, such as cognitive behavioral therapy, which includes self-compassionate thought diaries and behavioral tests, to help these people improve their self-esteem.55
To summarize the study’s key finding, the sexual function of dyad members may improve both partners’ QoL by enhancing their self-esteem. The partner’s self-esteem, in particular, was revealed to be just as strong a protective factor in promoting the individual’s QoL as the individual’s self-esteem. When couples face hardships together, their bond is strengthened by their shared experiences. Infertility is thus perceived as a shared problem or trauma in these situations.
Limitations
The limitations of the methods used in this study must be taken into account. First, this was a single-center research, which could have led to selection bias; further multicenter investigations should be performed. A cross-sectional study did not allow us to determine if the relationship between the variables was causative. Third, this study used a self-rating scale to assess sexual function, which may not be a reliable indicator because patients may have underestimated or overestimated their present condition, and recollection bias may have been present.
Conclusion
The dyadic relationship between sexual function, self-esteem, and QoL in couples with infertility demonstrate the critical nature of healthcare practitioners considering the couples with infertility as a unit. Several recommendations for clinical practice are necessary to improve QoL of couples with infertility, based on our findings. Medical professionals and public health advocates should examine couples’ self-esteem and utilize it as a resource for resolving their sexual problems. Self-esteem enhancements may benefit not only the individual’s QoL but their partners’ too. Throughout IVF treatment, couples with infertility should participate in joint health education to build self-esteem, which contributes significantly to relieving sexual pressure and thus improving QoL.
Data Sharing Statement
The data presented in this study are available on request due to privacy restrictions.
Ethics Approval and Informed Consent
The study followed the 1975 Declaration of Helsinki and its subsequent revisions as a guideline. All patients provided their written informed consent prior to responding to the survey. Ethical approval was obtained from the institutional Ethics Committee at Anhui Medical University (ID:20200961) prior to the collection of data.
Acknowledgments
We would like to thank all the patients who voluntarily participated in this study.
Author Contributions
Conceptualization: JYW, XQL, and JFH. Data curation: JYW and XQL.Software: JYW, CML and DNW. Investigation: WQT and JMW. Resources: YXC and GYL. Writing—original draft preparation JYW. Writing—review, and editing: JYW and XQL. Supervision: JFH and YXC. Project administration: JFH. Funding acquisition: JFH and DNW. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Special Project of National Natural Science Foundation of China (72004001), Central Government for Local Science and Technology Development Project (ID: 2019b11030010), Major Science and Technology Projects in Anhui Province (ID: SK2020ZD13) and Qingmiao Project of School of Nursing, Anhui Medical University (ID: hlqm2021018).
Disclosure
Jingfang Hong and Yunxia Cao should be considered joint senior author. The authors declare no conflict of interest.
References
1. Zegers-Hochschild F, Adamson GD, de Mouzon J, et al. International Committee for Monitoring Assisted Reproductive Technology (ICMART) and the World Health Organization (WHO) revised glossary of ART terminology, 2009. Fertil Steril. 2009;92(5):1520–1524. doi:10.1016/j.fertnstert.2009.09.009
2. World Health Organization. Infertility: a tabulation of available data on prevalence of primary and secondary infertility. Available from: http://apps.who.int/iris/handle/10665/59769.
3. Adamson GD, de Mouzon J, Chambers GM, et al. International Committee for Monitoring Assisted Reproductive Technology: world report on assisted reproductive technology, 2011. Fertil Steril. 2018;110(6):1067–1080. doi:10.1016/j.fertnstert.2018.06.039
4. Yang JW, Deng CY, Huang XF, et al. Annual report on assisted reproductive technology of Chinese Society of Reproductive Medicine in 2018. J Reprod Med. 2021;30(4):419–425. doi:10.12677/AP.2015.59068
5. Whoqol Group. The World Health Organization Quality of Life assessment (WHOQOL): position paper from the World Health Organization. Soc Sci Med. 1995;41(10):1403–1409. doi:10.1016/0277-9536(95)00112-k
6. Szkodziak F, Krzyżanowski J, Szkodziak P. Psychological aspects of infertility. A systematic review. J Int Med Res. 2020;48(6):300060520932403. doi:10.1177/0300060520932403
7. Lo SS, Li RH, Kok WM, Wong GC, Ng EH, Chan CH. Sexual function and quality of life in Chinese couples undergoing assisted reproductive treatment: a prospective cohort study. Hum Fertil. 2021;1–13. doi:10.1080/14647273.2020.1871518
8. Swift A, Reis P, Swanson M. Infertility stress, cortisol, coping, and quality of life in U.S. women who undergo infertility treatments. J Obstet Gynecol Neonatal Nurs. 2021;50(3):275–288. doi:10.1016/j.jogn.2020.12.004
9. Ni Y, Tong C, Huang L, Zhou W, Zhang A. The analysis of fertility quality of life and the influencing factors of patients with repeated implantation failure. Health Qual Life Outcomes. 2021;19(1):32. doi:10.1186/s12955-021-01666-3
10. Makara-Studzińska M, Limanin A, Anusiewicz A, et al. Assessment of Quality of Life in Men Treated for Infertility in Poland. Int J Environ Res Public Health. 2022;19(5):2950. doi:10.3390/ijerph19052950
11. Coward RM, Stetter C, Kunselman A, et al. Fertility related quality of life, gonadal function and erectile dysfunction in male partners of couples with unexplained infertility. J Urol. 2019;202(2):379–384. doi:10.1097/JU.0000000000000205
12. Starc A, Trampuš M, Pavan Jukić D, Rotim C, Jukić T, Polona Mivšek A. Infertility and sexual dysfunctions: a systematic literature review. Acta Clin Croat. 2019;58(3):508–515. doi:10.20471/acc.2019.58.03.15
13. Xiaoli S, Mei L, Junjun B, et al. Assessing the quality of life of infertile Chinese women: a cross sectional study. Taiwan J Obstet Gynecol. 2016;55(2):244–250. doi:10.1016/j.tjog.2015.06.014
14. Keramat A, Masoomi SZ, Mousavi SA, Poorolajal J, Shobeiri F, Hazavhei SM. Quality of life and its related factors in infertile couples. J Res Health Sci. 2014;14(1):57–63.
15. Castelo-Branco C, Naumova I. Quality of life and sexual function in women with polycystic ovary syndrome: a comprehensive review. Gynecol Endocrinol. 2020;36(2):96–103. doi:10.1080/09513590.2019.1670788
16. Orth U, Robins RW. Is high self-esteem beneficial? Revisiting a classic question. Am Psychol. 2022;77(1):5–17. doi:10.1037/amp0000922
17. DuBois DL, Flay BR. The healthy pursuit of self-esteem: comment on and alternative to the Crocker and Park (2004) formulation. Psychol Bull. 2004;130(3):415–434. doi:10.1037/0033-2909.130.3.415
18. Jamil S, Shoaib M, Aziz W, Ather MH. Does male factor infertility impact on self-esteem and sexual relationship? Andrologia. 2020;52(2):e13460. doi:10.1111/and.13460
19. Sakaluk JK, Kim J, Campbell E, Baxter A, Impett EA. Self-esteem and sexual health: a multilevel meta-analytic review. Health Psychol Rev. 2020;14(2):269–293. doi:10.1080/17437199.2019.1625281
20. Leary MR. Making sense of self-esteem. Curr Dir Psychol Sci. 1999;8(1):32–35. doi:10.1111/1467-8721.00008
21. Cui C, Wang L, Wang X. Effects of self-esteem on the associations between infertility-related stress and psychological distress among infertile Chinese women: a cross-sectional study. Psychol Res Behav Manag. 2021;14:1245–1255. doi:10.2147/PRBM.S326994
22. Uçar HN, Tekin E, Tekin U. Pain severity and psychosocial quality of life in adolescents with migraine and tension-type headache: mediation by perceived expressed emotion and self-esteem. J Oral Facial Pain Headache. 2021;35(1):62–71. doi:10.11607/ofph.2768
23. Kenny DA, Cook W. Partner effects in relationship research: conceptual issues, analytic difficulties, and illustrations. Pers Relationships. 1999;6(4):433–448.
24. Nakić Radoš S, Soljačić Vraneš H, Tomić J, Kuna K. Infertility-related stress and sexual satisfaction: a dyadic approach. J Psychosom Obstet Gynaecol. 2022;43(1):18–25. doi:10.1080/0167482X.2020.1752658
25. Yamanaka-Altenstein M, Rauch-Anderegg V, Heinrichs N. The link between infertility-related distress and psychological distress in couples awaiting fertility treatment: a dyadic approach. Hum Fertil. 2021;1–15. doi:10.1080/14647273.2021.1948112
26. Ying L, Wu LH, Wu X, Shu J, Loke AY. Endurance with partnership: a preliminary conceptual framework for couples undergoing in vitro fertilisation treatment. J Reprod Infant Psychol. 2018;36(2):144–157. doi:10.1080/02646838.2017.1416335
27. Li Z, Liu Y. Nursing Research Methods. Beijing, China: People’s. Health Press; 2012.
28. Boivin J, Takefman J, Braverman A. The fertility quality of life (FertiQoL) tool: development and general psychometric properties. Hum Reprod. 2011;26(8):2084–2091. doi:10.1093/humrep/der171
29. Li Y, Zhang X, Shi M, Guo S, Wang L. Resilience acts as a moderator in the relationship between infertility-related stress and fertility quality of life among women with infertility: a cross-sectional study. Health Qual Life Outcomes. 2019;17(1):38. doi:10.1186/s12955-019-1099-8
30. Rosenberg M. Society and the Adolescent Self-Image. Sociology. 1965;2:458.
31. Chen FF. The reliability and validity of the Chinese version of the revised-positive version of rosenberg self-esteem scale. Adv Psychol. 2015;05(9):531–535. doi:10.12677/AP.2015.59068
32. Rosen R, Brown C, Heiman J, et al. The Female Sexual Function Index (FSFI): a multidimensional self-report instrument for the assessment of female sexual function. J Sex Marital Ther. 2000;26(2):191–208. doi:10.1080/009262300278597
33. Sun X, Li C, Jin L, Fan Y, Wang D. Development and validation of Chinese version of female sexual function index in a Chinese population-A pilot study. J Sex Med. 2011;8(4):1101–1111. doi:10.1111/j.1743-6109.2010.02171.x
34. Rosen RC, Riley A, Wagner G, Osterloh IH, Kirkpatrick J, Mishra A. The international index of erectile function (IIEF): a multidimensional scale for assessment of erectile dysfunction. Urology. 1997;49(6):822–830. doi:10.1016/s0090-4295(97)00238-0
35. Tang DD, Li C, Peng DW, Zhang XS. Validity of premature ejaculation diagnostic tool and its association with International Index of Erectile Function-15 in Chinese men with evidence-based-defined premature ejaculation. Asian J Androl. 2018;20(1):19–23. doi:10.4103/aja.aja_9_17
36. Kenny DA, Kashy DA, Cook WL. Dyadic Data Analysis. New York: Guilford Press; 2006.
37. MacKinnon DP, Lockwood CM, Hoffman JM, West SG, Sheets V. A comparison of methods to test mediation and other intervening variable effects. Psychol Methods. 2002;7(1):83–104. doi:10.1037/1082-989x.7.1.83
38. Hu LT, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model Multidiscip J. 1999;6:1–55. doi:10.1080/10705519909540118
39. Lee TY, Sun GH. Psychosocial response of Chinese infertile husbands and wives. Arch Androl. 2000;45(3):143–148. doi:10.1080/01485010050193913
40. Yamada T, Sakisaka K, Bermúdez Rodríguez LN, Yamaoka K. Self-esteem, socioeconomic status and social participation of persons with disabilities living in areas affected by armed conflict in Colombia. Int J Environ Res Public Health. 2021;18(8):4328. doi:10.3390/ijerph18084328
41. Huang XT, Yin TZ. Start with cultural differences in self-esteem. J Psy Sci. 2012;35(1):2–8. doi:10.16719/j.cnki.1671-6981.2012.01.004
42. Casu G, Ulivi G, Zaia V, Fernandes Martins MDC, Parente Barbosa C, Gremigni P. Spirituality, infertility-related stress, and quality of life in Brazilian infertile couples: analysis using the actor-partner interdependence mediation model. Res Nurs Health. 2018;41(2):156–165. doi:10.1002/nur.21860
43. Goker A, Yanikkerem E, Birge O, Kuscu NK. Quality of life in Turkish infertile couples and related factors. Hum Fertil. 2018;21(3):195–203. doi:10.1080/14647273.2017.1322223
44. Zurlo MC, Della C, Volta MF, Vallone F. Predictors of quality of life and psychological health in infertile couples: the moderating role of duration of infertility. Qual Life Res. 2018;27(4):945–954. doi:10.1007/s11136-017-1781-4
45. Andrews FM, Abbey A, Halman LJ. Is fertility-problem stress different? The dynamics of stress in fertile and infertile couples. Fertil Steril. 1992;57(6):1247–1253. doi:10.1016/s0015-0282(16)55082-1
46. Sahin BM, Gursoy E. The social and psychological consequences of women getting pregnant with fertility treatment: a qualitative study. Perspect Psychiatr Care. 2021;57(2):463–472. doi:10.1111/ppc.12641
47. Massarotti C, Gentile G, Ferreccio C, Scaruffi P, Remorgida V, Anserini P. Impact of infertility and infertility treatments on quality of life and levels of anxiety and depression in women undergoing in vitro fertilization. Gynecol Endocrinol. 2019;35(6):485–489. doi:10.1080/09513590.2018.1540575
48. Maroufizadeh S, Hosseini M, Rahimi Foroushani A, Omani-Samani R, Amini P. The effect of depression on quality of life in infertile couples: an actor-partner interdependence model approach. Health Qual Life Outcomes. 2018;16(1):73. doi:10.1186/s12955-018-0904-0
49. Youseflu S, Jahanian Sadatmahalleh S. Psycho-sexual influence of sterilization on women’s quality of life: a path model. Health Qual Life Outcomes. 2021;19(1):89. doi:10.1186/s12955-021-01733-9
50. Leary MR, Tambor ES, Terdal SK, Downs DL. Self-esteem as an interpersonal monitor: the sociometer hypothesis. J Pers Soc Psychol. 1995;68:518–530. doi:10.1037/0022-3514.68.3.518
51. Alirezaei S, Ozgoli G, Alavi Majd H. Evaluation of factors associated with sexual function in infertile women. Int J Fertil Steril. 2018;12(2):125–129. doi:10.22074/ijfs.2018.5193
52. Türkben Polat H, Kaplan Serin E. Self-esteem and sexual quality of life among obese women. Perspect Psychiatr Care. 2021;57(3):1083–1087. doi:10.1111/ppc.12660
53. Ha JY, Ban SH. Effect of resilience on infertile couples’ quality of life: an actor-partner interdependence model approach. Health Qual Life Outcomes. 2020;18(1):295. doi:10.1186/s12955-020-01550-6
54. Shin H, Lee J, Kim SJ, Jo M. Associations of symptoms of depression, social support, and quality of life among Korean women who experience infertility. J Obstet Gynecol Neonatal Nurs. 2021;50(6):e1–e12. doi:10.1016/j.jogn.2021.06.007
55. Langford K, McMullen K, Bridge L, Rai L, Smith P, Rimes KA. A cognitive behavioural intervention for low self-esteem in young people who have experienced stigma, prejudice, or discrimination: an uncontrolled acceptability and feasibility study. Psychol Psychother. 2022;95(1):34–56. doi:10.1111/papt.12361
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Study on the Current Situation of Stigma and Its Influencing Factors Among Chinese Patients with Port-Wine Stains
Ran X, Yang X, Lin X, Yu W, Shang Y, Liang J, Shen L
Clinical, Cosmetic and Investigational Dermatology 2025, 18:1297-1308
Published Date: 26 May 2025