Back to Journals » Clinical and Experimental Gastroenterology » Volume 15
Sexual Dysfunction in Female Patients with Inflammatory Bowel Disease: An Overview
Authors Boyd T, de Silva PS, Friedman S
Received 26 July 2022
Accepted for publication 22 November 2022
Published 14 December 2022 Volume 2022:15 Pages 213—224
DOI https://doi.org/10.2147/CEG.S359367
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Santosh Shenoy
Taylor Boyd,1 Punyanganie S de Silva,1,2 Sonia Friedman1,2
1Harvard Medical School, Boston, MA, USA; 2Center for Crohn’s and Colitis, Brigham and Women’s Hospital, Boston, MA, USA
Correspondence: Sonia Friedman, 850 Boyston Street, Chestnut Hill, Center for Crohn’s and Colitis, Brigham and Women’s Hospital, Boston, MA, 02467, USA, +1 617-732-6389, Email [email protected]
Abstract: Sexual dysfunction is common among females with inflammatory bowel disease and may result in issues involving intimacy, sexual activity, and satisfaction, as well both the formation and preservation of personal relationships. Risk factors for sexual dysfunction include select surgical interventions, medications, mental illnesses, and IBD-related intestinal and extraintestinal comorbidities. In addition, certain demographic factors such as age, disease type and activity may influence the severity of sexual dysfunction. Evaluation of sexual dysfunction may include the use of validated sexual functioning questionnaires, a brief mental health assessment, initial inquiry into vulvovaginal or perineal symptoms, and a gynecologic and GI-focused physical exam. An interdisciplinary care team involving IBD specialists, obstetrician-gynecologists, pelvic floor physical therapists, and primary care physicians may be best suited to provide optimal care and treatment recommendations for patients with sexual dysfunction. Options for management often include pelvic floor physical therapy, biofeedback, and mental health support. Further research is necessary to delineate the impact of IBD activity on sexual dysfunction, to determine if health outcome differences exist depending on surgical approaches utilized during J-pouch operations, and finally to evaluate the care and perceptions of patients with IBD who identify as sexual and gender minorities.
Keywords: inflammatory bowel disease, ulcerative colitis, Crohn’s disease, sexual dysfunction
Introduction
Inflammatory bowel disease (IBD) is a class of gastrointestinal immune-mediated inflammatory diseases encompassing ulcerative colitis (UC) and Crohn’s disease (CD), both of which have been shown to significantly impact health-related quality of life.1 A number of physical, psychological and social factors contribute to the burden of disease faced by patients with IBD. Both classes of IBD are characterized by relapsing intestinal inflammation frequently resulting in abdominal pain, fatigue, weight loss, and diarrhea. These physical symptoms are often compounded by stress and fear of progression of disease due to the unpredictability and chronicity of IBD.2
Among females, IBD is often diagnosed between the ages of 20 and 40, a timeline which is in alignment with peak years for body image formation, fostering of intimate relationships, searching for long-term partners, and making decisions regarding family planning.3 These important milestones may be interrupted by the significant impact of sexual dysfunction (SD), another common complication of IBD. Challenges in sexual health among patients with IBD are complex and multifactorial. Improved clinician awareness and understanding of the etiology, risk factors, and impact of sexual dysfunction for women with IBD may result in improved diagnosis, care, and ultimately better health and wellbeing for this patient population.
Screening Tools for Diagnosis of Sexual Dysfunction
Sexual dysfunction has three main classifications including impairment in sexual desire, arousal or orgasm, and/or sexual pain.4 Identification of dysfunction in one or more of these categories requires completion of a thorough physical exam, a detailed medical history and a trusting patient-physician relationship. In addition to these core elements, multiple screening tools are available which may assist in the initial assessment. One tool widely used within the general population is the Female Sexual Function Index (FSFI).5 The FSFI consists of 19 items and utilizes a 5-point Likert scale to assess 6 primary domains of female sexual function including desire, arousal, lubrication, orgasm, satisfaction, and pain. This scale has been validated in numerous clinical and research settings.6 The Female Sexual Distress Scale–Revised (FSDS-R) is an alternative screening tool which has demonstrated high test–retest reliability and internal consistency in measuring sexually related personal distress among women.7 This questionnaire has the added benefit of brevity, with 13 Likert scale questions inquiring about patients’ experiences of sexual distress in the past month. Both scales are psychometrically sound and clinically interpretable, however neither are specific for measuring sexual dysfunction in patients with IBD. The IBD-Specific Female Sexual Dysfunction Scale (IBD-FSDS) correlates positively with the FSFI and FSDS-R and was the first tool developed to directly assess the psychosexual impact of IBD on women (Figure 1).8 The IBD-FSDS includes questions which address the impact of IBD-specific medications, symptoms, and surgical procedures on sexual functioning. Finally, the Body Image Scale (BIS) is a 9-item, single-factor scale designed to assess body image in patients with IBD. While separate from sexual dysfunction, there is significant overlap between body image and female sexual wellbeing.9
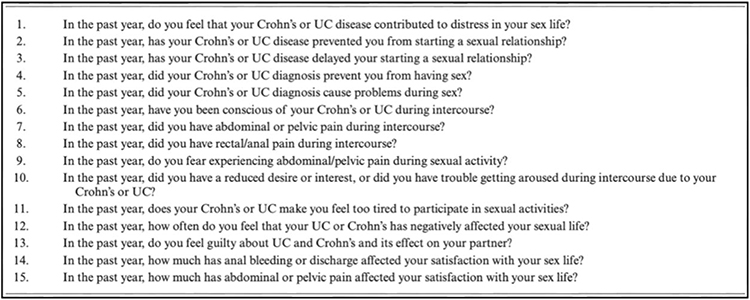 |
Figure 1 Displays the 15 questions included in the IBD-Specific Female Sexual Dysfunction Scale (IBD-FSDS). Each question assesses for the impact of IBD-specific symptoms on sexual functioning and/or relationships. Notes: Reproduced from de Silva PS, O’Toole A, Marc LG, et al. Development of a sexual dysfunction scale for women with inflammatory bowel disease. Inflamm Bowel Dis. 2018;24(11):2350–2359; with permission from Oxford University Press.8 |
Prevalence of Sexual Dysfunction
The prevalence of sexual dysfunction among premenopausal women in the general population is estimated at approximately 40%.10 Substantial study-dependent variation exists among reported SD rates specifically for females with IBD, however there is a strong consensus for a prevalence which is greater than that of the general population. Studies reporting SD rates ranging from approximately 50–90% have been described. A prospective cohort study involving 130 women with newly diagnosed, active IBD demonstrated an SD rate of 97% based on FSFI score results.11 In contrast, two cross-sectional studies, the first involving 192 patients and the second including 166 patients found significantly lower sexual dysfunction prevalence for females with IBD, reporting SD rates of 54 and 52% respectively.12,13 Considerable heterogeneity among SD prevalence is likely due to variation in research methodology including differences in specific screening tools used and decisions regarding patient stratification during the data analysis process.
In addition to impacting the overall sexual health of women, IBD may contribute to impairment in specific domains of SD. For example, a study carried out by Marin et al demonstrated findings of reduced sexual functioning scores in all measured domains among a cohort of 202 women, while a separate case-control study found that amongst 222 women with IBD, decreased frequency of intercourse was the only commonality in comparison to controls.14,15 Similar findings were demonstrated in a multi-center, case-control survey study where decreased sexual satisfaction and desire among patients with IBD was observed.14 Interest in intercourse is likely impaired in this population, as demonstrated by a survey study completed by Knowles et al in which 83.6% of females with IBD reported experiencing some level of lack of sexual interest.17 In summary, while there is variation in the exact incidence of sexual dysfunction among women with IBD, the prevalence is higher than that of the general female population both overall and at the level of individual sexual function domains.
Patient Demographics and Sexual Dysfunction
Certain patient demographic features may contribute to a disruption of normal sexual functioning in those with IBD including age and disease type (CD vs UC). In the general population, evidence suggests that for women, there is an overall decline in sexual desire, frequency of orgasm, and intercourse occurring as early as the third and fourth decade of life.18 This gradual change holds true for women with IBD, as older age has been identified as an independent risk factor for sexual dysfunction.11 Interestingly, among women with IBD, SD may also be observed across the age spectrum.11,19 When stratified by mean age, one study reported that women younger than 40 years old with IBD exhibited a significantly increased odds of SD in comparison to controls.20
When considering the impact of disease type on sexual functioning, there is mixed data on whether differences exist between women with ulcerative colitis compared to those with Crohn’s disease. Two studies in which women with IBD were found to have significantly worse sexual functioning than the control population, showed no variation in levels of SD severity between those with UC and those with Crohn’s disease.11,21 Differences in SD were however noted in studies which more closely explored both the individual disease characteristics present among subgroups of the two patient populations, in addition to the specific domains of sexual dysfunction most significantly impacted. Greater rates of dyspareunia were identified among patients with perianal fistulas than those without.22 The results of a cross-sectional study which included a population-based cohort of Danish women showed similar findings where patients with CD reported more frequent dyspareunia, specifically deep dyspareunia, and difficulty in achieving orgasm than women with UC and those without IBD.23
Risk Factors for Sexual Dysfunction
Disease Activity
Disease activity, IBD-related comorbidities, surgery, and medications are important factors which may contribute to sexual dysfunction risk among women with IBD. Data regarding the influence of disease activity is varied, with most evidence suggesting either impaired sexual function regardless of disease activity or a moderate accompanying increase in SD as disease activity and severity increases. A study of 181 female patients who completed the Brief Index of Sexual Function in Women (BISF-W), showed that for those with SD, symptoms of impaired sexual health were present irrespective of disease activity as compared to healthy controls.15 Several other studies found a lack of association with disease when age and medication use were controlled for.11,12,14,21 One contrasting research report identified a moderate decrease specifically in sexual interest and satisfaction experienced by patients with greater disease activity as measured by the short Crohn’s Disease Activity Index (sCDAI) for CD and the Simple Clinical Colitis Activity Index (SCCAI) for UC.16 Fatigue, abdominal pain and fear of incontinence during intercourse may increase in parallel with worsening disease activity and have been cited as reasons for a reduction in intercourse frequency.22 Further research is warranted to delineate the impact of disease severity and activity on sexual functioning.
Related Health Comorbidities
Both intestinal and extraintestinal IBD-related comorbidities may contribute to impairment of normal sexual functioning. Chronic fatigue syndrome is known to be associated with sexual dysfunction and is prevalent among patients with IBD, especially those with Crohn’s disease.14,24 Other extraintestinal manifestations include joint pain, skin lesions, and decreased energy, all symptoms which may also contribute to sexual functioning impairment.25 Draining cutaneous fistulae and perianal complications may also worsen SD as perianal disease has been shown to have a negative impact on sexual desire and body image.26
Medications
Corticosteroids, immunosuppressants, and biologic agents targeted at reducing intestinal inflammation and inducing mucosal healing are highly effective in the management of IBD, however potential accompanying adverse effects may be detrimental to sexual functioning among female patients. Corticosteroids are a mainstay of treatment for active IBD and multiple studies have demonstrated a significant association between SD and use of this class of medications.27 A cross-sectional study found that corticosteroids were the only independently associated factor for female SD when age, hospitalizations, perianal disease, and depression were controlled for.14 Similarly, the results of a survey study of 336 women with IBD demonstrated that corticosteroid use was associated with decreased scores in the domains of both sexual pleasure and orgasm.21 Corticosteroids are often prescribed during induction therapy or as a component of management for an acute flare, thus they may serve as an indirect marker of IBD severity, at least partially explaining the positive association with SD. In addition, corticosteroid side effects such as depression, acne, fluid retention, increased facial hair, and weight gain which accompany long-term use may indirectly contribute to issues with body image and sexual dysfunction.28
Biologic therapy development is a rapidly expanding area of IBD disease management research, however data regarding the influence of this class of medication on sexual functioning is highly varied. Kanar et al reported that the use of immunomodulators or biologic agents does not affect sexual health, while Shmidt et al identified a significant positive association between SD in women with newly diagnosed IBD and the use of biological therapy in multivariate analysis.11,29 In a more recent longitudinal cohort study of 123 patients started on a new biologic or small molecule therapy, those who responded to therapy were found to have an improvement in SD.30 Based on the differences in findings, it may be hypothesized that similar to corticosteroid use, biologics, at least when used during the initiation phase for women with rapidly developing IBD, may serve as a surrogate for disease severity, contributing to the association with sexual dysfunction observed in some studies.
Despite inconclusive evidence for a robust association between SD and a subset of the medications used for IBD, for many patients the perceived influence of medications on sexual function alone is pervasive enough to interfere with medication adherence. Muller et al found that 40% of patients believed that their IBD medications had a negative impact on their libido or sexual activity.31 Further, 10% of patients sometimes or frequently discontinued their IBD medications due to perceived effects on libido.
Surgery
UC and CD are dynamic diseases which may advance in extent and behavior over time. Disease progression despite medical management may ultimately require surgical intervention. Ileocecal resection is the most common procedure for patients with CD. In a study completed by Nøhr et al, women with CD who underwent surgery had an increased risk of difficulties in achieving orgasm as well as dyspareunia in comparison to women without CD surgery, however none of these estimates reached statistical significance.23 The ileoanal pouch anastomosis (IPAA), also known as a J-pouch, is one of the most common surgical procedures performed in the management of UC.32 There are several important considerations of J-pouch surgery, as pelvic dissection may put patients at risk of adhesion formation, scarring and damage to the delicate network of autonomic and somatic nerves which control the female genitalia.33 Despite these potential risks and complications of J-pouch formation, most evidence-based consensus is suggestive of an overall improvement in sexual functioning following surgical operation. Davies et al found that for women, rates of reported SD decreased from 73.1% before J-pouch surgery to 25% twelve months after surgery.34 Similarly, when 23 women were interviewed regarding details of their preoperative and postoperative social and sexual functions as well as quality of life, significant improvement was reported after J-pouch surgery.35 Among women who were initially unable to achieve orgasm preoperatively, in the postoperative period, none of the women from the group reported a disturbance in this domain of sexual functioning, and 16% of women experienced an increased quality of orgasm. In a separate study involving the evaluation of 25 women at baseline and 6 months after proctocolectomy or J-pouch surgery, women reported improvements in both general and IBD-specific quality of life, as well as improved sexual desire.36 Surgical management may result in the resolution of complications such as abscesses, fistulas, and perianal disease, likely contributing to the improvement seen in patients postoperatively. Of note, most studies investigating SD and J-pouch surgical outcomes to date have had relatively small cohort sizes and larger studies are needed for more robust confirmation of surgical benefit. Further, research in this area has most often reported on surgeries which resulted in successful J-pouches. Problems specific to J-pouch failure including fecal incontinence and/or increased stool frequency may affect several domains of sexual dysfunction including desire, arousal, and satisfaction.37 Complications related to proctocolectomies may negatively influence sexual function, as parasympathetic nerve damage can result in decreased lubrication and dyspareunia.37–39 Alterations in anatomical structure including changes in the angle of the vagina following pelvic dissection may also serve as contributing factors to dyspareunia.37
While J-pouch surgery is often the procedure of choice for patients with IBD requiring surgery, proctocolectomy with the construction of an ileostomy may be lifesaving for patients who do not respond to medical therapy or for those who may not be candidates for a J-pouch.32 Studies which have employed the Rating Form of IBD Patient Concerns (RFIPC) to investigate patients’ primary IBD-related worries report that the potential need for an ileostomy is of greatest concern for many patients.40–42 Issues related to intimacy, loss of sexual drive, and ability to perform sexually due to ostomy formation have been frequently cited.43 One study demonstrated that 52% of women experienced a decrease in sense of sexual attractiveness following ileostomy formation, while 60% of women felt less desirable.34
Research studies investigating surgical technical differences such as open surgery in comparison to minimally invasive surgery (laparoscopic and robotic surgery) are sparse. Thus far however, robotic proctectomy has been shown to be comparable to laparoscopic procedures in terms of operative time, return of bowel function and postoperative outcomes.44 Sexual function was found to be equivalent in the two groups based on results of a pre and post assessment of both sexual desire and ability to achieve orgasm.44
Mental Health
In most studies, mental health issues are among the primary determinants of sexual dysfunction for patients with IBD, with depression serving as a particularly strong predictor.8,13,15,17,21 There is a 20% prevalence of anxiety and an estimated 15% prevalence of depression among patients with IBD, approximately double that of the general US population.45 IBD patients with depression are more likely to report difficulty achieving orgasm as well as reduced sexual desire, satisfaction, and intercourse frequency.21
Vulvovaginal Disorders and IBD
As with non-IBD patients, vulvovaginal disorders may lead to significant disruption of sexual function, however among women with IBD there are a number of specific conditions which may be a direct result of IBD or its therapy that affect the vulvovaginal area. For the purposes of this review, vulvovaginal disorders in IBD can chiefly be divided into (a) extraintestinal manifestations of IBD and (b) side effects of IBD specific therapy.
Extraintestinal Manifestations of IBD
Crohn’s disease of the vulva has been described in the pediatric and adolescent literature, and although rarer in adult women, is a well-recognized clinical entity.46 Patients may present with relapsing and remitting symptoms of pruritus, vulvar redness, swelling or pain, vulvar bumps, labial hypertrophy (particularly in the labia majora), knife-like fissures, ulcerations, abscesses, and fistulae.47–50 Vulvar Crohn’s disease may be contiguous or noncontiguous with the gastrointestinal tract. If noncontiguous with the gastrointestinal tract, it is also known as cutaneous Crohn’s of the vulva/vulvo-perineum, or metastatic Crohn’s disease (MCD). Metastatic CD involving the vulva and perineum is rare and thus often is difficult to diagnose. A variety of clinical presentations have been described, including widespread nonspecific pain and swelling, erythematous papules and plaques, and nonhealing ulcers. Vulvar Crohn’s may precede, coincide with, or develop after the initial diagnosis of intestinal disease.51 However, not all cases of vulvar Crohn’s proceed to gastrointestinal disease. The provider should maintain a suspicion of possible vulvar Crohn’s involvement in adult patients with a longstanding history of IBD dating back to childhood and a history of vulvar pain, edema, and ulcerations not otherwise explained. The differential diagnoses includes lichen planus, lichen sclerosis, vulvar intraepithelial neoplasia, and acquired lymphangiectasia. In addition to the physical limitations and discomfort from vulvar, perineal and gluteal disease, many women with IBD suffer psychologically due to these lesions. Fear of pain, embarrassment, anxiety or depression regarding lesion appearance may all contribute to sexual dysfunction. Treatment with a biologic with extraintestinal receptor blocking potential has been shown to be effective in the management of vulvar Crohn’s.
Health care providers should also be mindful of the possible presence of concomitant autoimmune disease such as Sjogren’s syndrome which is known to cause symptoms of pruritus and dyspareunia due to dry secretions.52 Hidradenitis suppurativa (HS) is another concomitant autoimmune skin disease seen in patients with IBD. It is a chronic, inflammatory, recurrent, debilitating skin disease of the terminal hair follicle, which usually presents after puberty with painful, deep-seated, inflamed lesions in the apocrine gland-bearing areas of the body, such as the axillary, inguinal, and anogenital regions.52 In addition, follicles of vulvar pubic hair may be affected leading to vulvovaginal lesions. This can lead to draining sinuses, multiple abscesses, and multiple nodules. In a recent nationwide cohort study, HS was significantly associated with an increased risk of CD (HRCD =1.23; 1.03–1.46) but not UC (HRUC =1.01; 0.89–1.14).53 Given the significant comorbidity associated with this condition, it is unsurprising that a recent systematic review of 12 epidemiological studies noted that sexual dysfunction was significantly increased in HS patients.54
Vulvovaginal Side-Effects of IBD Specific Therapy
Immunosuppressive therapy with azathioprine, 6-mercaptopurine, and anti-TNF biologics have been linked to an increase in certain infections, which in turn can lead to vulvovaginal lesions.55 Herpes zoster infection secondary to immunosuppressive therapy can manifest in the vulvovaginal area as dispersed and coalescing vesicular lesions extending to the right lower limb involving sacral dermatomes and associated with severe pain.55 It is well recognized that immunosuppressive medication also increases the risk of infection with human papilloma virus (HPV). In a study of 209 women with HPV-related pre-malignant lesions, women with vulvar lesions were most likely to worry about infertility, being sexually less attractive, or infecting a sexual partner.56 The presence of setons, drains, and other vulvovaginal surgery for Crohn’s disease can also contribute to sexual dysfunction in women due to discomfort, pain, vulvar, and vaginal irritation and anxiety regarding appearance.
Evaluation and Management
Due to the wide range of potential etiologies of sexual dysfunction among women with IBD, a holistic and interdisciplinary approach to diagnosis and management is often warranted (Figure 2).19 The initial consultation may include a gynecologic and GI-focused physical exam, an assessment of mood, self-image, stressors, and relationship issues. Incorporating screening questions for sexual dysfunction into routine visits for patients with IBD may reduce barriers to providing necessary management (Table 1). For example, integrating questions discerning how often and to what degree a patient is bothered by dyspareunia, inhibition of sexual dysfunction due to ostomy bags, or fear of passing stool during intercourse, may be helpful in identifying the current impact of IBD symptoms on a woman’s sexual life.19 The options for SD management are highly dependent on a patients’ specific symptoms and features of disease, however most treatment choices target the abnormal contractions and dyssynergy of the pelvic floor muscles which may lead to decreased sexual response or pain.19 Options in management may include pelvic floor physical therapy carried out by an experienced therapist. Myofascial release may be beneficial for specific pelvic or vaginal trigger points.19 Biofeedback may also be a useful tool in therapeutic management. Finally, given the significant association of mental health with sexual functioning, based on the presence of psychological symptoms, depression screening with a PHQ-9 may be beneficial, in addition to follow-up with a referral to a mental health specialist as necessary.
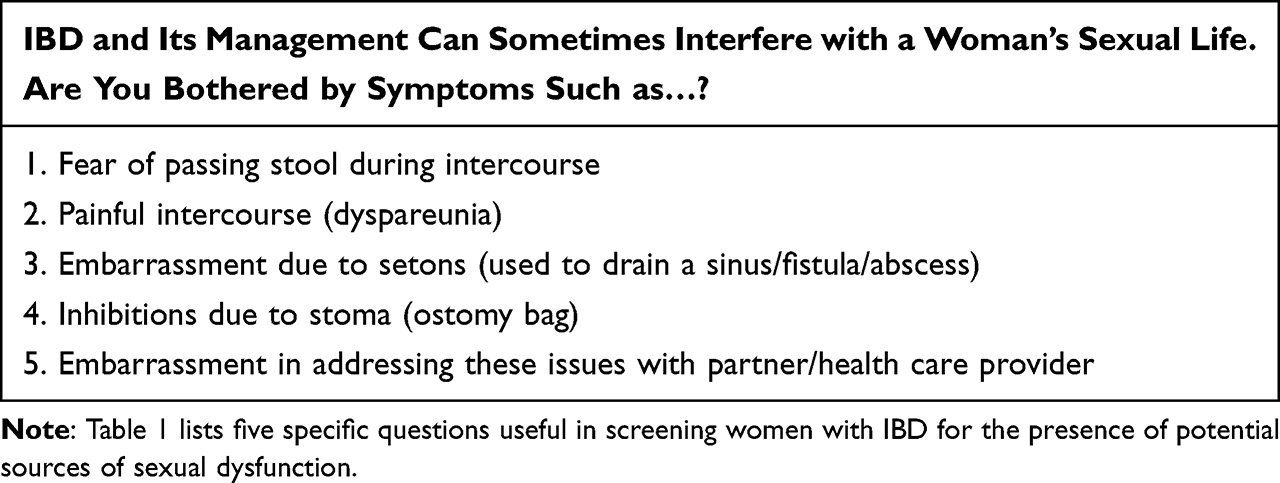 |
Table 1 Screening Women with IBD for Sexual Dysfunction |
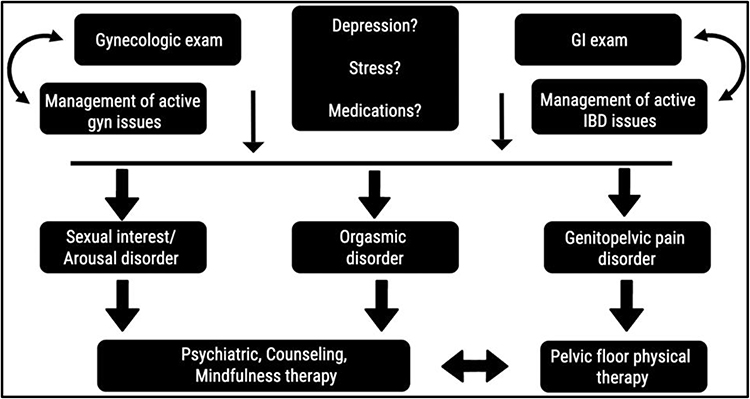 |
Figure 2 Depicts an overview of the approach to the diagnosis and management of sexual dysfunction among women with IBD who present with GI and/or gynecologic symptoms. Notes: Reprinted from American Journal of Obstetrics and Gynecology, Vol 215/ Issue 1, Sanders JN, Gawron LM, Friedman S, Sexual satisfaction and inflammatory bowel diseases:an interdisciplinary clinical challenge, Pages No. 58-62, Copyright (2016), with permission from Elsevier.19 |
Conversations Regarding Sexual Dysfunction
Prioritizing time during routine visits with IBD patients to engage in open conversations on the topic of sexual health may reduce challenges in the identification, diagnosis, and management of sexual dysfunction. Barriers to disclosure arise both on part of the health care provider and patient. Only 14% of gastroenterologists report routinely inquiring about sexual health for patients with IBD, citing reasons such as a lack of time, deficiency in knowledge on the matter, and personal discomfort with the topic of sexual dysfunction.57 An additional barrier is a lack of consensus regarding which clinical specialty should be responsible for IBD-related sexual health conversations. For patients, engaging in these conversations may be difficult due to the sensitive nature of the topic, limited time for discussion or perceived low level of interest from health care providers in having these discussions.57 In a multi-center prospective cross-sectional study of 454 female patients in the United States or Denmark, it was found that only 12.8% of women from the US cohort and 6% of women from the Denmark cohort had already discussed sexual function with their gastroenterologist.8 Shame and embarrassment are reported as factors which inhibit discussions of sexual dysfunction and may be especially prevalent among individuals who identify as sexual minorities.58 In a study of patients between the ages of 17–64, those who identified as belonging to a sexual minority group found it especially difficult to discuss the topic of sexual dysfunction, even when sexual orientation had been previously disclosed to the clinical team.58 Despite the significant existing challenges in discussion initiation, a large proportion of patients expressed the opinion that information regarding the impact of IBD on intimacy and sexuality should be given at IBD diagnosis.57 Patients also expressed preferences in the specifics of sexual health information delivery, with 53 to 67% of women stating that they preferred talking about sex with a female provider whereas the remainder felt comfortable with either a male or female provider.8 Further, many patients felt that this information should be delivered by their IBD specialist.57
IBD and the Gynecological Exam
When assessing a female patient with IBD, it is appropriate for the gastroenterologist to undertake an IBD specific perineal exam, and if appropriate, refer a patient to a gynecologist for a more detailed physical evaluation. An initial inquiry into symptoms, specifically vulvovaginal or perineal symptoms such as dyspareunia is appropriate. Female IBD patients have previously indicated that they prefer to discuss sexual function and are agreeable to their gastroenterologist initiating this discussion.8,59
Prior to the examination, it is important for the clinician to put the patient at ease. Sensitive inquiry regarding any history of sexual abuse and current menstrual status can be helpful in preparing both the patient and clinician for the exam. Informed verbal consent should be obtained, and a chaperone should be present. It is also important to determine if there is any evidence of vulvar or perianal infection, infestation, or foreign body present. Asking the patient if she experiences any irritation or soreness in the vulvovaginal and perineal region, or tension in the pelvic floor area is helpful.60
The gynecological exam including inspection is ideally performed in the lithotomy position. Wearing non-sterile, non-latex gloves the clinician should gently part the labia and examine the patient’s perineal area, checking it for erythematous, excoriated skin, infections, piercings, labial edema and thickening of the labia majora and minora. Scarring, fistulae, abscesses and sinuses in the genital, perineal and perianal area, skin tags, and/or urinary leakage should also be noted. Assessment of the vulva and associated perineal area for the presence of immunosuppression-related skin conditions such as candidiasis, HPV lesions, herpes zoster rash, and flesh-colored papules consistent with genital subcutaneous granulomatosis which may be a manifestation of IBD61 is also recommended. Asking the patient to cough will allow the clinician to evaluate for tissue protrusion that may indicate a degree of prolapse and/or leakage of urine or feces. Although not IBD-specific, pelvic prolapses may contribute to sexual dysfunction. To assess for enteroceles and rectoceles, retract the anterior vaginal wall while patients are in the lithotomy position, and during rectovaginal examination, ask patients to strain. Asking the patient to tighten (pull in) their pelvic floor muscles will allow the clinician to observe whether there is contraction and thereby evaluate the strength of the muscles.
During the exam it is also useful for the gastroenterologist to identify the presence, location, and tightness of any setons which have been placed as this may contribute to pelvic pain and dysfunction. Once inspection is complete, the clinician can then proceed to the rectal exam. During the routine rectal exam, the clinician may then proceed to assess for any posterior vaginal prolapse by asking the patient to bear down as if having a bowel movement. Bearing down may cause the posterior vaginal prolapse to bulge, thereby enabling its size and location.
Mechanics of Pelvic Floor Physical Therapy
The pelvic floor physical therapist will first evaluate pelvic floor muscle activity during the process of squeezing and contraction. She will observe the perineum and introital area in the dorsal lithotomy position as the patient performs a Kegel squeeze. Patients with pelvic floor hypertonic dysfunction often have significant muscle
tension at “rest” such that they are unable to increase contractile strength and cannot produce an effective squeeze. Often patients will be unable to relax completely or demonstrate a rebound tightening of the pelvic floor. Spontaneous muscle fasciculation can be seen in some patients during attempts at squeeze and relax maneuvers.62
A lubricated cotton tip applicator is then used to carefully evaluate for signs of allodynia (pain from stimuli that are not normally painful) and vulvodynia (unexplained pain around the area of the vaginal opening). At this point the physical therapist will place a generously lubricated single finger in the vagina to assess pelvic floor awareness and the ability to squeeze and relax the levator ani. Determining the degree of pelvic floor muscle tenderness is important so the physical therapist can assess the presence and location of myofascial pain. This is done by applying gentle pressure to the levator muscles and assessing whether the patient’s reported pain is reproduced with downward pressure against the pelvic floor musculature. During a pelvic floor physical therapy session, the therapist will perform internal soft tissue and myofascial release therapy. She may also employ biofeedback or ultrasound therapy and will educate the patient regarding daily pelvic floor relaxation, rest and heat therapies as well as avoidance of triggers and management of fluids and stool.62
Pelvic floor physical therapists will often work in conjunction with the patient’s gynecologist in the treatment of pelvic floor dysfunction. In settings where a pelvic floor physical therapist is not available, a one-time teaching of pelvic floor muscle exercises may be completed by the gynecologist at the time of gynecologic exam and pelvic floor muscle assessment. Research has shown that patient teaching of pelvic floor exercises led by OB/GYN specialists may serve as a cost-effective, low-resource tool to improve patient symptoms of pelvic floor dysfunction.63
Impact of Sexual Dysfunction
Quality of Life
Sexual dysfunction resulting from IBD may influence multiple aspects of a woman’s health and wellbeing. Personal relationships, decisions regarding family planning, and overall quality of life may be directly or indirectly impacted. While several studies have investigated both quality of life in addition to levels of sexual dysfunction among women with IBD, there is little data available which specifies associations between these two measures. The 32-item Inflammatory Bowel Disease Questionnaire (IBDQ-32) is the most frequently used instrument to capture disease-specific quality of life in randomized clinical trials for ulcerative colitis.64 Using the IBDQ-32, one study evaluated quality of life 6 months following J-pouch surgery. When asked about the extent to which patients’ bowel problems had limited sexual activity over the past two weeks, patients with higher IBDQ scores were found to also have higher scores for questions relating to sexual functioning suggesting a potential association between these two measures.65
Relationships
Impaired sexual functioning may have a significant adverse effect on patients’ existing relationships in addition to posing challenges during the formation of new ones. In a study by Knowles et al, one quarter of women stated that IBD was a key barrier in starting a sexual relationship.17 Research by De Silva et al showed that for two-thirds of women, IBD caused distress in their sexual relationships.8 Further results from a survey study involving 347 patients from a hospital-based IBD database revealed that over half of respondents felt that IBD had negatively affected their relationship status. Primary reasons provided for the impact on relationship status included impaired body image, problems with mood, inability to go out, and the effect of IBD on sexual activity.31 The influence of IBD on sexual functioning may further permeate into family planning decisions for women, as both SD and impaired body image have been shown to have a direct impact on voluntary childlessness.65
Conclusion and Future Directions
Sexual dysfunction is common among females with IBD and the overall impact on a woman’s quality of life may be extensive, often resulting in challenges with sexual activity, intimacy and the formation of personal relationships (Figure 3).2 Several risk factors may contribute to the development of SD for women with IBD and certain demographic factors, comorbidities, and IBD management strategies may influence the presence or severity of SD. A thorough health evaluation and physical examination are required to diagnose sexual dysfunction, and there are a number of treatment options available to help improve outcomes and quality of life of patients with IBD and SD.
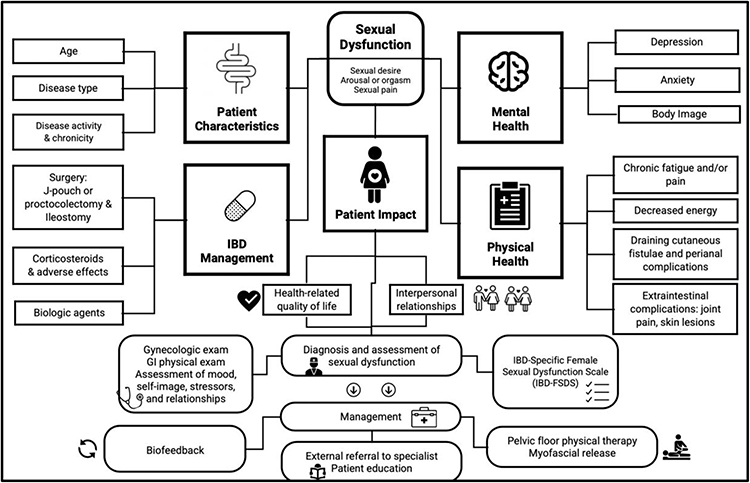 |
Figure 3 Displays a comprehensive overview of the factors which contribute to sexual dysfunction among women with IBD, including patient mental and physical health comorbidities, IBD disease characteristics and surgical and medical management of IBD. Downstream effects of sexual dysfunction, diagnostics and management options are also depicted. |
Patient demographics including age and disease type may influence the presence and/or severity of IBD. Both intestinal and extraintestinal IBD-related comorbidities including chronic fatigue, joint pain, skin lesions, decreased energy, cutaneous fistulae, and perianal complications may contribute to impairment of normal sexual functioning. Additionally, there are a number of specific conditions which may be a direct result of IBD or its therapy that impact the vulvovaginal area, thereby contributing to sexual dysfunction. Other risk factors may include select surgical interventions, mental and physical health comorbidities as well as certain classes of medications.
In addition to treating the GI-specific symptoms of IBD with prescription medications, options for management of associated SD may include pelvic floor physical therapy, biofeedback, and mental health support. To provide adequate care, a holistic treatment approach is considered optimal and requires significant patient-physician trust, open conversations, and the engagement of an interdisciplinary care team involving IBD specialists, OBGYNs and primary care physicians.
There are multiple areas for future research in developing a better understanding of the overall impact and potential solutions for sexual dysfunction as it relates to IBD. Further investigation is warranted to further clarify whether differences in sexual functioning exist for patients with active or inactive IBD as current data is relatively inconclusive. In addition, comparative, longitudinal investigations of patients’ post-surgical sexual functioning following minimally invasive J-pouch surgical procedures is necessary. Finally, research regarding the impact of IBD on sexual dysfunction among sexual minorities and members of the LGBTQ (lesbian, gay, bisexual, transgender, and queer) community is scarce. Existing data suggests that the psychosocial influence of sexual dysfunction may disproportionately impact this group.
Abbreviations
IBD, Inflammatory bowel disease; SD, Sexual Dysfunction; IBD-FSDS, IBD-Specific Female Sexual Dysfunction Scale.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Drossman DA, Patrick DL, Mitchell CM, Zagami EA, Appelbaum MI. Health-related quality of life in inflammatory bowel disease. Functional status and patient worries and concerns. Dig Dis Sci. 1989;34(9):1379–1386. doi:10.1007/bf01538073
2. Casati J, Toner BB, de Rooy EC, Drossman DA, Maunder RG. Concerns of patients with inflammatory bowel disease: a review of emerging themes. Dig Dis Sci. 2000;45(1):26–31. doi:10.1023/a:1005492806777
3. Connelly TM, Berg AS, Harris L 3rd, Brinton D, Deiling S, Koltun WA. Genetic determinants associated with early age of diagnosis of IBD. Dis Colon Rectum. 2015;58(3):321–327. doi:10.1097/dcr.0000000000000274
4. Walton B, Thorton T. Female sexual dysfunction. Curr Womens Health Rep. 2003;3(4):319–326.
5. Rosen R, Brown C, Heiman J, et al. The Female Sexual Function Index (FSFI): a multidimensional self-report instrument for the assessment of female sexual function. J Sex Marital Ther. 2000;26(2):191–208. doi:10.1080/009262300278597
6. Neijenhuijs KI, Hooghiemstra N, Holtmaat K, et al. The Female Sexual Function Index (FSFI)-A systematic review of measurement properties. J Sex Med. 2019;16(5):640–660. doi:10.1016/j.jsxm.2019.03.001
7. Derogatis L, Clayton A, Lewis-D’Agostino D, Wunderlich G, Fu Y. Validation of the female sexual distress scale-revised for assessing distress in women with hypoactive sexual desire disorder. J Sex Med. 2008;5(2):357–364. doi:10.1111/j.1743-6109.2007.00672.x
8. de Silva PS, O’Toole A, Marc LG, et al. Development of a sexual dysfunction scale for women with inflammatory bowel disease. Inflamm Bowel Dis. 2018;24(11):2350–2359. doi:10.1093/ibd/izy202
9. McDermott E, Healy G, Mullen G, et al. Patient education in inflammatory bowel disease: a patient-centred, mixed methodology study. J Crohns Colitis. 2018;12(4):419–424. doi:10.1093/ecco-jcc/jjx175
10. McCool ME, Zuelke A, Theurich MA, Knuettel H, Ricci C, Apfelbacher C. Prevalence of female sexual dysfunction among premenopausal women: a systematic review and meta-analysis of observational studies. Sex Med Rev. 2016;4(3):197–212. doi:10.1016/j.sxmr.2016.03.002
11. Shmidt E, Suárez-Fariñas M, Mallette M, et al. A longitudinal study of sexual function in women with newly diagnosed inflammatory bowel disease. Inflamm Bowel Dis. 2019;25(7):1262–1270. doi:10.1093/ibd/izy397
12. Rivière P, Zallot C, Desobry P, et al. Frequency of and factors associated with sexual dysfunction in patients with inflammatory bowel disease. J Crohns Colitis. 2017;11(11):1347–1352. doi:10.1093/ecco-jcc/jjx100
13. Bel LG, Vollebregt AM, Van der Meulen-de Jong AE, et al. Sexual dysfunctions in men and women with inflammatory bowel disease: the influence of IBD-related clinical factors and depression on sexual function. J Sex Med. 2015;12(7):1557–1567. doi:10.1111/jsm.12913
14. Marín L, Mañosa M, Garcia-Planella E, et al. Sexual function and patients’ perceptions in inflammatory bowel disease: a case-control survey. J Gastroenterol. 2013;48(6):713–720. doi:10.1007/s00535-012-0700-2
15. Timmer A, Bauer A, Dignass A, Rogler G. Sexual function in persons with inflammatory bowel disease: a survey with matched controls. Clin Gastroenterol Hepatol. 2007;5(1):87–94. doi:10.1016/j.cgh.2006.10.018
16. Eluri S, Cross RK, Martin C, et al. Inflammatory bowel diseases can adversely impact domains of sexual function such as satisfaction with sex life. Dig Dis Sci. 2018;63(6):1572–1582. doi:10.1007/s10620-018-5021-8
17. Knowles SR, Gass C, Macrae F. Illness perceptions in IBD influence psychological status, sexual health and satisfaction, body image and relational functioning: a preliminary exploration using structural equation modeling. J Crohns Colitis. 2013;7(9):e344–50. doi:10.1016/j.crohns.2013.01.018
18. Hayes R, Dennerstein L. The impact of aging on sexual function and sexual dysfunction in women: a review of population-based studies. J Sex Med. 2005;2(3):317–330. doi:10.1111/j.1743-6109.2005.20356.x
19. Sanders JN, Gawron LM, Friedman S. Sexual satisfaction and inflammatory bowel diseases: an interdisciplinary clinical challenge. Am J Obstet Gynecol. 2016;215(1):58–62. doi:10.1016/j.ajog.2016.01.188
20. Zhao S, Wang J, Liu Y, et al. Inflammatory bowel diseases were associated with risk of sexual dysfunction in both sexes: a meta-analysis. Inflamm Bowel Dis. 2019;25(4):699–707. doi:10.1093/ibd/izy345
21. Timmer A, Kemptner D, Bauer A, Takses A, Ott C, Fürst A. Determinants of female sexual function in inflammatory bowel disease: a survey based cross-sectional analysis. BMC Gastroenterol. 2008;8:45. doi:10.1186/1471-230x-8-45
22. Moody G, Probert CS, Srivastava EM, Rhodes J, Mayberry JF. Sexual dysfunction amongst women with Crohn’s disease: a hidden problem. Digestion. 1992;52(3–4):179–183. doi:10.1159/000200951
23. Nøhr EA, Nielsen J, Nørgård BM, Friedman S. Sexual health in women with inflammatory bowel disease in the Danish national birth cohort. J Crohns Colitis. 2020;14(8):1082–1089. doi:10.1093/ecco-jcc/jjaa038
24. Tsai SY, Chen HJ, Lio CF, et al. Increased risk of chronic fatigue syndrome in patients with inflammatory bowel disease: a population-based retrospective cohort study. J Transl Med. 2019;17(1):55. doi:10.1186/s12967-019-1797-3
25. Malik TF, Aurelio DM. Extraintestinal Manifestations of Inflammatory Bowel Disease. In: StatPearls. StatPearls Publishing Copyright © 2022, StatPearls Publishing LLC; 2022..
26. Kappelman M, Martin C, Weinfurt K, et al. P-70 sexual interest and satisfaction in an internet cohort of patients with inflammatory bowel diseases. Inflamm Bowel Dis. 2012;18(suppl_1):S43–S44. doi:10.1097/00054725-201212001-00103
27. Ho GT, Chiam P, Drummond H, Loane J, Arnott ID, Satsangi J. The efficacy of corticosteroid therapy in inflammatory bowel disease: analysis of a 5-year UK inception cohort. Aliment Pharmacol Ther. 2006;24(2):319–330. doi:10.1111/j.1365-2036.2006.02974.x
28. Buchman AL. Side effects of corticosteroid therapy. J Clin Gastroenterol. 2001;33(4):289–294. doi:10.1097/00004836-200110000-00006
29. Kanar O, Berry AC, Nakshabendi R, et al. Effects of immunomodulators and biologic agents on sexual health in patients with inflammatory bowel disease. Ochsner J Summer. 2017;17(2):150–156.
30. Castillo G, Beaty W, Miller J, et al. S911 sexual dysfunction improves with biologic therapy in men and women with IBD. Off J Am Coll Gastroenterol. 2021;116:S430. doi:10.14309/01.ajg.0000777176.28012.0a
31. Muller KR, Prosser R, Bampton P, Mountifield R, Andrews JM. Female gender and surgery impair relationships, body image, and sexuality in inflammatory bowel disease: patient perceptions. Inflamm Bowel Dis. 2010;16(4):657–663. doi:10.1002/ibd.21090
32. Sica GS, Biancone L. Surgery for inflammatory bowel disease in the era of laparoscopy. World J Gastroenterol. 2013;19(16):2445–2448. doi:10.3748/wjg.v19.i16.2445
33. Izanec J, Nagle D. Impact of proctectomy on continence and sexual function in women. Am J Gastroenterol. 2006;101(12 Suppl):S618–24. doi:10.1111/j.1572-0241.2006.00964.x
34. Davies RJ, O’Connor BI, Victor C, MacRae HM, Cohen Z, McLeod RS. A prospective evaluation of sexual function and quality of life after ileal pouch-anal anastomosis. Dis Colon Rectum. 2008;51(7):1032–1035. doi:10.1007/s10350-008-9248-x
35. Damgaard B, Wettergren A, Kirkegaard P. Social and sexual function following ileal pouch-anal anastomosis. Dis Colon Rectum. 1995;38(3):286–289. doi:10.1007/bf02055604
36. Wang JY, Hart SL, Wilkowski KS, et al. Gender-specific differences in pelvic organ function after proctectomy for inflammatory bowel disease. Dis Colon Rectum. 2011;54(1):66–76. doi:10.1007/DCR.0b013e3181fd48d2
37. Ogilvie JW
38. Bengtsson J, Lindholm E, Nordgren S, Berndtsson I, Oresland T, Börjesson L. Sexual function after failed ileal pouch-anal anastomosis. J Crohns Colitis. 2011;5(5):407–414. doi:10.1016/j.crohns.2011.04.002
39. Freeha K, Bo S. Complications related to J-Pouch surgery. Gastroenterol Hepatol (N Y). 2018;14(10):571–576.
40. Abdalla MI, Sandler RS, Kappelman MD, et al. The impact of ostomy on quality of life and functional status of Crohn’s disease patients. Inflamm Bowel Dis. 2016;22(11):2658–2664. doi:10.1097/mib.0000000000000930
41. Drossman DA, Leserman J, Li ZM, Mitchell CM, Zagami EA, Patrick DL. The rating form of IBD patient concerns: a new measure of health status. Psychosom Med. 1991;53(6):701–712. doi:10.1097/00006842-199111000-00010
42. Stjernman H, Tysk C, Almer S, Ström M, Hjortswang H. Worries and concerns in a large unselected cohort of patients with Crohn’s disease. Scand J Gastroenterol. 2010;45(6):696–706. doi:10.3109/00365521003734141
43. Carlsson E, Bosaeus I, Nordgren S. What concerns subjects with inflammatory bowel disease and an ileostomy? Scand J Gastroenterol. 2003;38(9):978–984. doi:10.1080/00365520310004687
44. Miller AT, Berian JR, Rubin M, Hurst RD, Fichera A, Umanskiy K. Robotic-assisted proctectomy for inflammatory bowel disease: a case-matched comparison of laparoscopic and robotic technique. J Gastrointest Surg. 2012;16(3):587–594. doi:10.1007/s11605-011-1692-6
45. Barnes EL, Nestor M, Onyewadume L, de Silva PS, Korzenik JR. High dietary intake of specific fatty acids increases risk of flares in patients with ulcerative colitis in remission during treatment with aminosalicylates. Clin Gastroenterol Hepatol. 2017;15(9):1390–1396.e1. doi:10.1016/j.cgh.2016.12.036
46. Kakiuchi T, Yoshiura M, Nagata-Hashimoto M, Nagata‐Hashimoto M, TanakaK. Pediatric case of Crohn’s disease with preceding vulvitis granulomatosa. Clin Case Rep. 2022;10(4):e05676. doi:10.1002/ccr3.5676
47. Dayan R, Sadownik L, Reutter J. Vulvar Crohn disease. Cmaj. 2021;193(11):E379. doi:10.1503/cmaj.190112
48. Barret M, de Parades V, Battistella M, Sokol H, Lemarchand N, Marteau P. Crohn’s disease of the vulva. J Crohns Colitis. 2014;8(7):563–570. doi:10.1016/j.crohns.2013.10.009
49. Boxhoorn L, Stoof TJ, de Meij T, et al. Clinical experience and diagnostic algorithm of vulval Crohn’s disease. Eur J Gastroenterol Hepatol. 2017;29(7):838–843. doi:10.1097/meg.0000000000000879
50. Feller ER, Ribaudo S, Jackson ND. Gynecologic aspects of Crohn’s disease. Am Fam Physician. 2001;64(10):1725–1728.
51. Andreani SM, Ratnasingham K, Dang HH, Gravante G, Giordano P. Crohn’s disease of the vulva. Int J Surg. 2010;8(1):2–5. doi:10.1016/j.ijsu.2009.09.012
52. Capriello P, Barale E, Cappelli N, Lupo S, Teti G. Sjögren’s syndrome: clinical, cytological, histological and colposcopic aspects in women. Clin Exp Obstet Gynecol. 1988;15(1–2):9–12.
53. Schneeweiss MC, Kirchgesner J, Wyss R, et al. Occurrence of inflammatory bowel disease in patients with chronic inflammatory skin diseases: a cohort study. Br J Dermatol. 2022;187:692–703. doi:10.1111/bjd.21704
54. Seetan K, Al-Zubi M, Al-Omari R. Sexual dysfunction in patients with hidradenitis suppurativa: a systematic review and meta-analysis. J Clin Aesthet Dermatol. 2021;14(8):61–65.
55. Martins MM, Ferreira P, Maciel R, Costa C. Vulvar herpes zoster infection: a rare and challenging diagnosis. BMJ Case Rep. 2021;14(12):Dec. doi:10.1136/bcr-2021-246797
56. Nagele E, Reich O, Greimel E, Dorfer M, Haas J, Trutnovsky G. Sexual activity, psychosexual distress, and fear of progression in women with human papillomavirus-related premalignant genital lesions. J Sex Med. 2016;13(2):253–259. doi:10.1016/j.jsxm.2015.12.012
57. Christensen B. Inflammatory bowel disease and sexual dysfunction. Gastroenterol Hepatol (N Y). 2014;10(1):53–55.
58. Fourie S, Norton C, Jackson D, Czuber-Dochan W. These discussions aren’t happening’: experiences of people living with inflammatory bowel disease and talking about sexual well-being with health care Professionals. J Crohns Colitis. 2021;15(10):1641–1648. doi:10.1093/ecco-jcc/jjab043
59. Jedel S, Hood MM, Keshavarzian A. Getting personal: a review of sexual functioning, body image, and their impact on quality of life in patients with inflammatory bowel disease. Inflamm Bowel Dis. 2015;21(4):923–938. doi:10.1097/mib.0000000000000257
60. Yates A. Female Pelvic Floor 2: assessment and Rehabilitation. Nurs Times. 2019;115(6):30–33.
61. Sager R, Frei P, Steiner UC, Fink D, Betschart C. Genital dysplasia and immunosuppression: why organ-specific therapy is important. Inflamm Intest Dis. 2019;4(4):154–160. doi:10.1159/000502687
62. Butrick CW. Pelvic floor hypertonic disorders: identification and management. Obstet Gynecol Clin North Am. 2009;36(3):707–722. doi:10.1016/j.ogc.2009.08.011
63. Armstrong AA, Nguyen MM, Wieslander CK, Tarnay CM. All levels of providers can effectively and efficiently teach pelvic floor strength assessment at time of pelvic examination. Female Pelvic Med Reconstr Surg. 2019;25(2):154–156. doi:10.1097/spv.0000000000000665
64. Yarlas A, Maher S, Bayliss M, et al. The inflammatory bowel disease questionnaire in randomized controlled trials of treatment for ulcerative colitis: systematic review and meta-analysis. J Patient Cent Res Rev. 2020;7(2):189–205. doi10.17294/2330-0698.1722
65. Walldorf J, Pijan E, Greinert R, Riesner-Wehner A, Michl P. Family planning with inflammatory bowel disease: the challenge of childlessness and parent concerns. Familienplanung bei chronisch entzündlichen darmerkrankungen: kinderlosigkeit ist erhöht – sorgen und wissen der patienten haben hierauf unterschiedlichen einfluss. Z Gastroenterol. 2021;59(8):841–850. doi:10.1055/a-1404-3610
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.