Back to Journals » Risk Management and Healthcare Policy » Volume 13
Sexual and Gender-Based Violence Among Refugees and Internally Displaced Persons in the Democratic Republic of the Congo: Post-Conflict Scenario
Authors Lugova H ![]() , Samad N
, Samad N ![]() , Haque M
, Haque M ![]()
Received 24 September 2020
Accepted for publication 23 November 2020
Published 9 December 2020 Volume 2020:13 Pages 2937—2948
DOI https://doi.org/10.2147/RMHP.S283698
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Halyna Lugova,1 Nandeeta Samad,2 Mainul Haque3
1Unit of Community Medicine, Faculty of Medicine and Defence Health, National Defence University of Malaysia, Kuala Lumpur, Malaysia; 2Department of Public Health, North South University, Dhaka, Bangladesh; 3Unit of Pharmacology, Faculty of Medicine and Defence Health, National Defence University of Malaysia, Kuala Lumpur, Malaysia
Correspondence: Mainul Haque
Faculty of Medicine and Defence Health, National Defence University of Malaysia, Kem Perdana Sugai Besi, Kuala Lumpur 57000, Malaysia
Tel +60109265543
Email [email protected]
Abstract: The ongoing humanitarian crisis in the Democratic Republic of the Congo has triggered sexual and gender-based violence, including rape, sexual slavery, trafficking, intimate partner violence, and sexual exploitation. Gender inequalities and abuse of power experienced by women and young girls at refugee settings further exacerbate their vulnerability to different forms of violence. This study aimed to offer an evidence-based approach to developing strategies in tackling the complex problem of sexual and gender-based violence among refugees and internally displaced persons in the Congo. We conducted a narrative review of all the relevant papers known to the authors to explore the origins of the problem, its implications on public health, and its impact on equity. The study revealed that sexual assault survivors face physical and psychological sufferings, excruciating emotions, and profound disruption of their social well-being since they are often stigmatized and ostracized by society. The analysis of current government policies revealed a lack of programs to address survivors’ specific concerns and policy enforcement problems. This study suggested strategic objectives and policy implementation steps. The proposed strategies address women empowerment and gender stigma, provision of effective health services, and adequate response action.
Keywords: SGBV, evacuees, post-conflict, policy, DRC
Background
I took refuge in a camp for displaced people where three armed men raped me. … physical and psychological pain was immense. …. distressed that I felt I could not look after my children after the attack. I felt like my family and community completely abandoned me.
– Gisèle, the mother of three.1
The Democratic Republic of the Congo (DRC) is one of the largest countries in Sub-Saharan Africa and home to over 86 million people as of 2019.2,3 Presently, safe drinking water is provided for 43% of the country’s households (69% in cities and 23% in the countryside). Sanitation is available to a mere 20% of the households. The fertility rate in DRC is 6.1 children per woman, which is higher than the average of 4.8 children per woman in Sub-Saharan Africa. The DRC has one of the highest early childbearing rates, with 125.24 births per 1000 adolescent girls aged between 15 and 19 years of age.2 Despite some progress in reducing extreme poverty over the last twenty years, the DRC still ranks as one of the poorest nations globally. In 2018, 72% of its population, especially in the north-western and central-southern regions, survived on less than US$ 1.90 a day.2
The DRC was colonized by Belgium in 1885 and granted its independence seventy-five years later in 1960. However, the legacy of colonization and current global post-colonial policies have underlain the government’s present failures to address the suffering of the Congolese people. The highest rates of poverty in the world, recurring conflicts, and the growing inequity has profoundly affected public health.3 The cost of colonization was the depopulation of an estimated ten million people under King Leopold II of Belgium. During this period, people faced enormous discrimination and severe ill-treatment from the colonizers.4 In the 20th century, the country achieved significant improvements, including advances in administration, economic development, and the healthcare services provision.5,6
Nevertheless, the Congolese faced difficulties in their endeavor with governing the country independently after the colonial rule. The predetermining factors included dependence on the colonizers’ guidance and technical expertise, loss of pre-colonial survival skills necessary for a balanced co-existence with the environment, and the years of suppression of human dignity and identity.5,7,8 The public health system developed by the Belgians, principally focused on maintaining the workforce’s productivity and gradually degraded after the DRC’s independence with the departure of most of their medical experts.5,9,10
Moreover, the cascading dynamics of civil conflicts and wars in the eastern DRC following the independence, was fueled mainly by neo-liberal politics in the pursuit of the country’s resources and resulted in the economic breakdown, massive forced migration, unprecedented violence, and deaths of thousands of people.11–13 Ultimately, the public health situation dramatically deteriorated with a significant increase in inequalities in health.14–18 The problem is especially alarming considering the 5.4 million refugees and internally displaced persons (IDPs) in the DRC, and over 800,000 Congolese refugees who fled outside the country.19 In the places where armed conflicts have come to an end, the process of rehabilitation at refugee settings should adequately address all population groups’ fundamental health rights to avoid the growth of inequalities in health.20,21
Martials and Methods
A review of literature concerning sexual and gender-based violence (SGBV) was conducted using PubMed, PsychINFO, Pre-CINAHL and Google Scholar. Terms used in each database search included the following: (exploitation, abuse OR violence) AND (refugee OR displaced person) AND Congo. Specific names of the policies and regulating documents were also searched. Scanning the references of found papers was also conducted. The following inclusion criteria were used: the article was written in the English language, the study focused on SGBV among refugees or IDPs in DRC. Exclusion criteria were set as studies on SGBV amongst the non-refugee populations. Information related to strategies identify, prevent, and respond to SGBV was extracted from the identified articles. The data gathered primarily focused on the prevalence and origins of SGBV, public health and equity implications, analysis of current policies, and policy evaluation. The three authors independently examined each of the articles. Any controversies were resolved by the authors through reaching a consensus in discussion.
Results
Sexual and Gender-Based Violence at Refugee Settings
Definition of the Problem
SGBV refers to acts inflicting mental, physical, or sexual suffering perpetrated against a person’s will and based on gender differences.22 In the DRC, the high levels of SGBV have affected women since the beginning of the conflict in 1998. It was recorded that 1000 women had been raped daily, whereas young girls below 18 years accounted for 65% of the victims.23–26 Rape is used as a weapon of war, but it plays an essential role in post-conflict societies when the intensity of a conflict is diminished significantly.27–30
At refugee settings, the Congolese women are often separated from other family members due to the disruption of social structures by armed conflict, making them more vulnerable to SGBV.31–33 Thus, the following types of SGBV occur at refugee and IDP camps: sexual attack or coercion, including by persons in authority; domestic violence; sexual assault while searching for essential needs for domestic purposes; survival sex or forced prostitution; and sexual exploitation in return for securing legal status or access to resources in asylum country.34,35 Furthermore, sexual abuse of young women and adolescent girls is an area of concern in the DRC.36–38 Girls in refugee camps are often forced to engage in sex in exchange for clothing and sanitary products, and teachers force female students to exchange sex for money or school exam grades.33,39,40
The Implications of the Problem for Public Health
In the DRC, the acts of SGBV are often perpetrated at the extreme level of brutality and tortures, such as gang rape, genital mutilation, forced abortion, etc.38,41 Survivors of SGBV face physical injuries, sexual and reproductive health (SRH) concerns, including HIV and other sexually-transmitted diseases, sterility and fistula, psychological and emotional sufferings, such as depression, anxiety, and post-traumatic stress disorder, and often cannot address them adequately due to a lack of access to (or inappropriate quality of) health care services.42–44 The acts of SGBV may result in long-term disabilities and even death and the social impacts of SGBV cannot be underestimated.41,45,46 Ultimately, there is a lack of knowledge about healing and recovery after SGBV, including the impact of sociocultural environment on healing processes and cultural nuances of healing goals following it.47
The USAID reported that HIV prevalence among women who survived SGBV in conflict and post-conflict areas in the DRC was much higher than among women in the general population (25.6% against 1.6%, respectively).48 A case-control study in Kinshasa found that SGBV was significantly associated with HIV infection and its behavioural risk factors, such as alcohol consumption and polygamy.49 Additionally, a mathematical model revealed that gang rapes in the DRC, Sudan, Burundi, Rwanda, Sierra Leone, Somalia, southern Sudan, and Uganda could have resulted in a 6–7% median increase in HIV incidence among girls and women aged 5 to 49 years.50 Besides, the prevalence of HIV infection among women in the IDP camps was significantly higher and more strongly associated with the history of SGBV than among women in the host population of the DRC and other conflict-prone African countries.51–53 Nevertheless, some researchers have argued that the data supporting the association between conflict-driven SGBV and the HIV prevalence and incidence rates at the population level is inconclusive.54–56
The Origins of the Problem and Impact on Equity
Globally, gender inequalities have a strong relationship with sexual violence.57–61 The vulnerability of women in refugee and IDP camps to SGBV is predetermined by pre-existing cultural gender inequalities and domestic violence and deterioration of traditional gender roles in society due to the destruction of households as a result of war and deaths of family members.34,62–67 Peacekeepers and aid workers have engaged in hegemonic masculinity practices that encourage sexual exploitation and abuse of the most marginalized in the communities – women and children.68,69 The harm suffered by survivors has hardly been addressed by any of the agencies, including the United Nations.70
Moreover, SGBV initiated by militants has been adopted by the civilians in refugee camps.31,71–73 The close relationship between sexual violence and masculinity implies “rape myths”74 based on beliefs of denial of sexual offenses and men’s dominance.75–78 Besides, most survivors or victims do not report their experiences due to the stigma associated with sexual violence in the DRC based on cultural perceptions. They fear being abandoned by husbands, primarily if (gang) rape resulted in pregnancy.71,79 Thus, social isolation and ostracism of rape victims by community members could harm women more so than the assault itself.33,80,81 Additionally, women’s social and economic marginalization in refugee settings implies growing inequities in health, such as SGBV, food insecurity, and a lack of access to health services.74,82,83 Finally, there is a lack of appropriate SRH services to address SGBV and high rates of maternal deaths, HIV, and illegal abortions among women in refugee camps, especially young women and adolescents.84–86
The conceptualization of SGBV in both scholarly and policy research is far from incorporating the complexity of the underlying causes of SGBV among refugees.87 Firstly, existing literature focuses mainly on women as victims and rarely addresses the experiences of other at-risk groups, such as men, the disabled, and LGBTI.88,89 Secondly, most of the studies highlight various aspects of physical violence and its context, and there is a lack of research on the causes and impacts of structural violence, including health, economic, cultural, political, and racial disparities.90,91 Thirdly, SGBV experiences are likely to differ dramatically across the continuum of conflict, refugee exile, and resettlement.87 There is little examination of SGBV in the context of resettlement.92
Building a Strategy
Analysis of Current Policies
The existing policies tailored to respond to SGBV provide only short-term relief for survivors and rarely offer comprehensive preventive interventions.93 National efforts to tackle the problem of SGBV in the DRC implied legislative criminalization of sexual violence and the government’s dedication to dealing with this problem.94 Additionally, the government adopted the 2009 UN Action on Sexual Violence in Conflict comprehensive strategy for the DRC.95,96 The plan focuses on strengthening national authorities’ capacities to prosecute SGBV crimes, especially those committed by militants. However, there is a lack of enforcement of the policy, and survivors often obtain justice through community mediation rather than the legal system.97 Other aspects of the program cover prevention and protection, assistance to survivors, security sector reform, and data mapping.98 Noteworthy, there is a lack of government programs to address specific concerns of SGBV among refugees and IDPs.37,38,99,100 UNHCR developed guidelines for SGBV prevention and response among these vulnerable groups.34 The work of the agency, in close cooperation with other humanitarian organizations, has contributed to achievements in the handling of SGBV cases, for example, through assistance in creating community centers for SGBV cases identification and referring support services, and training focal points among refugees and IDPs.101 On the contrary, the World Bank initiatives to prevent SGBV by investing money in the education sector of the DRC have not accounted for inequities in access to education.102–105 Arguably, global markets supported by neoliberal politics are linked to state-corporate crimes that induce sexual violence in the DRC.106–108
Therefore, the government’s insufficient commitment and the “collapse of public health services” have challenged the overall progress of the strategy.99 Noteworthy, the policy of provider-initiated HIV testing and counseling (PITC) has been proven to be highly successful in the DRC109 and could help address SGBV among displaced populations. However, its implementation is problematic because it depends on international support and resources, which are scarce and often earmarked due to political instability.24,110 Focus of international organizations has mainly been in response to SGBV rather than on prevention from its occurring.111–114
Strategic Objectives and Policy Implementation Steps
The guiding principles in tackling the complex problem of SGBV among displaced people include community engagement in behavioral change, a multi-sectoral approach by all actors, highlighting the issues of equity, and ensuring the equal participation of all community members (specifically, young women and adolescents), in planning, implementing, monitoring and evaluating processes.22 Economic and food security of displaced women is an essential determinant of social cohesion and women empowerment; in particular, it may prevent women from engaging in survival sex.115 Communication activities have proven to be effective in raising the solidarity of women.116,117 Engaging men and boys in SGBV prevention is another perspective approach to change male gender beliefs.118–120 Additionally, security reform in displaced settings is one of the crucial components of SGBV prevention.95,96
Implementation of comprehensive primary health care will address the needs of displaced populations by ensuring the equity and sustainability of the outcomes.121–125 Decentralizing SRH services and making them equally accessible for all population groups, including adolescents and young women, should be emphasized.126–129 Training of healthcare personnel to be sensitive to the needs of displaced women (including SGBV survivors),130,131 and creating adolescent-friendly environments,126 are essential components of prevention. The multi-sectoral approach will help address a broader spectrum of social determinants of health that lead to (gender) inequities.132,133
The actions should be based on the fundamental human rights and priority of women’s health and well-being as postulated in the Sustainable Development Goals (SDGs), in particular SDG 3 (good health and well-being) and SDG 5 (gender equality), SDG 4 (quality education) and SDG 10 (reduced inequality).134 Therefore, effective prevention and a response strategy should include engagement with communities and civic society, strong support from the government, and durable and coordinated international participation (Table 1).
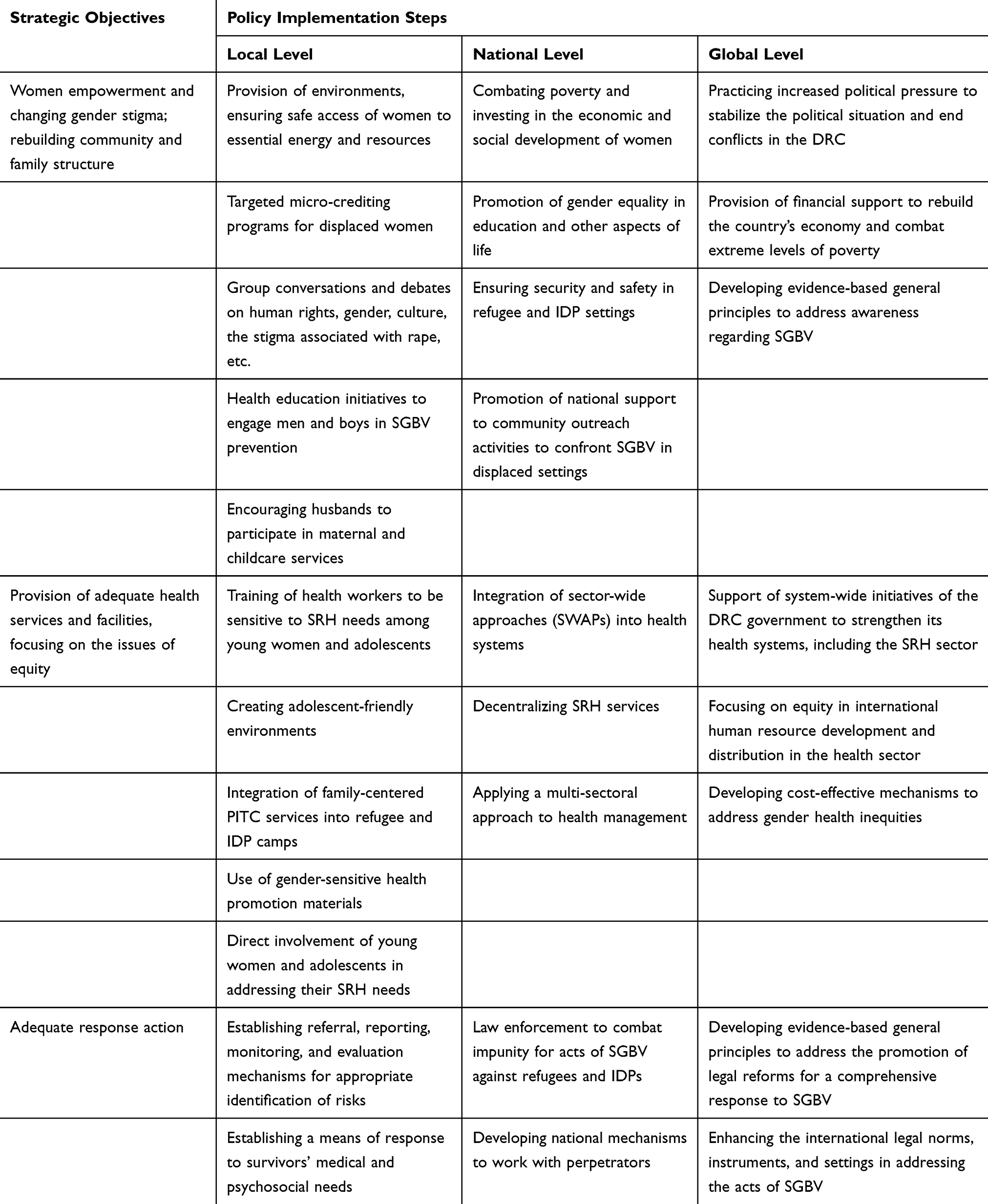 |
Table 1 Combating Sexual and Gender-Based Violence at Refugee Settings in the DRC During the Post-Conflict Scenario: Plan for Action by 2024 |
Expected Outcomes and Performance Measurement
Monitoring and reporting progress is crucial in ensuring that the prevalence of SGBV in refugee settings is decreasing.101,135 Evaluations will measure progress toward achieving a sustained reduction in SGBV by 2024. Specific indicators for critical interventions are listed below.
- The number of women groups that meet regularly
- The number of women involved in micro-enterprise development
- The number of initiated educational programs and a percent of those successfully implemented
- A percentage of people with a changed attitude towards SGBV (regular surveys)
- The number and percentage of women distributing food, water, and fuel among other women
- Types and quality of information materials
- The number of boys and men involved in health educational programs addressing SGBV
- The number and types of SRH services available, a percentage of adolescent friendly SRH services
- The percentage of health workers trained to respond to SGBV
- The number and type of psychosocial support services
- The number of incidences reported through informal and formal channels
- The number of offenders prosecuted
- The number of legal actions taken to protect the survivors
Limitations on Policy Implementation
Various internal and external forces may influence policy implementation. Time lags between adopting the policy and its practical application depend on the DRC’s government commitment, cooperative action of international partners, and activism of civil society. The proposed approach is designed with a long-term view; therefore, there is a risk that the stakeholders will be demotivated to invest resources without observing immediate effects following the implementation.136
In a conflict-affected setting of the DRC, the implementation of SGBV policy may be affected by lack of infrastructure, including little or no police coverage, which creates barriers for reporting SGBV cases. Other limitations include poor funding allocations, poor multi-sectoral coordination, dominance of customary law, discriminatory gender stereotypes and socio-cultural norms.137,138
Besides, the policy’s implementation may be influenced by external forces, such as globalization, characterized by the deterioration of social systems and problems for the government to invest in public health due to the focus on privatization.136 This may lead to more unpredictable and uncontrollable outcomes.
Conclusion
While in exile at refugee settings in the DRC, thousands of people suffer from the widespread SGBV. Women and young girls are the most vulnerable due to cultural gender inequalities aggravated by on-going conflicts, which have resulted in the destruction of family and community structures, deterioration of gender roles in society, and increase of impunity among militants and persons in authority. Public health implications of SGBV include physical and socio-psychological sufferings, which often cannot be adequately addressed due to the scarcity of relevant healthcare facilities. Current policies to address SGBV have failed due to the government’s insufficient commitment and a lack of political will and cooperation of the global players to support comprehensive prevention programs rather than focusing on targeted interventions in response to SGBV acts. The proposed strategic objectives in tackling SGBV at refugee settings focus on community and civic society engagement, government support, and international participation.
Recommendation
The proposed plan for action to combat SGBV against refugees in the DRC during the post-conflict scenario by 2024 includes strategies to address women empowerment, changing gender stigma, and rebuilding community structure; provision of effective health services focusing on equity; and adequate response action. Policy implementation steps are outlined at local, national, and global levels. Expected outcomes are based on the indicators of critical interventions.
Article Highlights
- Sexual and gender-based violence has a profound physical, psychological, and social impact on women and young girls in the DRC.
- Implementing current policies that address SGBV is problematic due to the government’s insufficient commitment and dependence on international support and resources.
- Most international organizations have focused on the response to SGBV rather than on prevention from its occurring.
- The proposed strategies and policy implementation steps at local, national, and international levels are offered.
- The proposed plan for action by 2024 addresses women empowerment and gender stigma, the provision of effective health services, and adequate response action.
Acknowledgment
The authors would like to thank the library of the National Defence University of Malaysia for its support in providing access to relevant manuscripts. The authors also would like to thank Vivienne Philip for her editorial support.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This paper was not funded.
Disclosure
The authors declare that they do not have any conflicts of interest for this work or financial involvement or affiliations with any organization, association, or entity directly or indirectly with the subject matter or materials presented in this article. This includes honoraria, expert testimony, employment, ownership of stocks or options, patents or grants received or pending, or royalties.
References
1. United Nations Development Program. Fighting sexual violence in the Democratic Republic of Congo; 2014. Available from: https://www.undp.org/content/undp/en/home/ourwork/ourstories/fighting-sexual-violence-in-the-democratic-republic-of-congo.html.
2. The World Bank. The World Bank in DRC; 2020. Available from: https://www.worldbank.org/en/country/drc/overview.
3. The World Bank. Democratic Republic of Congo; 2020. Available from: https://data.worldbank.org/country/CD.
4. Stanard MG. Belgium, the Congo, and imperial immobility: a singular empire and the historiography of the single analytic field. Fr Colon Hist. 2014;15:87–110. doi:10.14321/frencolohist.15.2014.0087
5. Le Billon P. Diamond wars? Conflict diamonds and geographies of resource wars. Ann Assoc Am Geogr. 2008;98(2):345–372.
6. Ntembwa HK, Lerberghe WV Improving health system efficiency. Democratic Republic of the Congo. Improving aid coordination in the health sector. Health Systems Governance & Financing. World Health Organization. WHO Press, World Health Organization: 20 Avenue Appia, 1211 Geneva 27, Switzerland. Available from: https://apps.who.int/iris/bitstream/handle/10665/186673/WHO_HIS_HGF_CaseStudy_15.4_eng.pdf;jsessionid=721FD1204FF2F8F15305332521372220?sequence=1.
7. Kingsley Atterh F Perceptions of contemporary effects of colonialism among educational professionals in Ghana. Open access dissertations. 732. University of Massachusetts: Amherst, Boston, USA; 2013. Available from: https://scholarworks.umass.edu/cgi/viewcontent.cgi?referer=https://www.google.com/&httpsredir=1&article=1737&context=open_access_dissertations.
8. Subramanian SM, Pisupati B. Traditional knowledge in policy and practice: approaches to development and human well-being. United Nations University Press, United Nations University: 53-70, Jingumae 5-Chome, Shibuya-ku, Tokyo 150-8925, Japan; 2010. Available from https://collections.unu.edu/eserv/UNU:2546/ebrary9789280811919.pdf.
9. Mock N, de Buhr E, Mukungo M, Wemakoy O Public health training in the Democratic Republic of Congo: a case study of the Kinshasa School of Public Health. Johns Hopkins Bloomberg School of Public Health, USAID (From The American People); 2006. Available from https://www.jhsph.edu/research/affiliated-programs/global-research-activity/Congo.pdf.
10. Rosoux V. The two faces of Belgium in the Congo: perpetrator and rescuer. Eur Rev Int Stud. 2014;1(3):16–38.
11. Birn AE, Pillay Y, Holtz TH. Textbook of International Health: Global Health in a Dynamic World.
12. Bavinck M, Pellegrini L, Mostert E, Eds. Conflicts Over Natural Resources in the Global South: Conceptual Approaches. (A Balkema Book). Boca Raton: CRC Press; 2014.
13. IOM, UN Migration. World migration report 2020. International Organization for migration, 17 route des Morillons, P.O. Box 17, 1211 Geneva 19, Switzerland; 2019. Available from: https://www.un.org/sites/un2.un.org/files/wmr_2020.pdf.
14. Kandala NB, Emina JB, Nzita PD, Cappuccio FP. Diarrhea, acute respiratory infection, and fever among children in the Democratic Republic of Congo. Soc Sci Med. 2009;68(9):1728–1736. doi:10.1016/j.socscimed.2009.02.004
15. Kandala NB, Madungu TP, Emina JB, Nzita KP, Cappuccio FP. Malnutrition among children under the age of five in the Democratic Republic of Congo (DRC): does geographic location matter? BMC Public Health. 2011;11:261. doi:10.1186/1471-2458-11-261
16. Kismul H, Acharya P, Mapatano MA, Hatløy A. Determinants of childhood stunting in the Democratic Republic of Congo: further analysis of demographic and health survey 2013–14. BMC Public Health. 2017;18(1):74. doi:10.1186/s12889-017-4621-0
17. Quentin W, Abosede O, Aka J, et al. Inequalities in child mortality in ten major African cities. BMC Med. 2014;12:95. doi:10.1186/1741-7015-12-95
18. Hosseinpoor AR, Bergen N, Schlotheuber A, et al. State of inequality in diphtheria-tetanus-pertussis immunization coverage in low-income and middle-income countries: a multicountry study of household health surveys. Lancet Glob Health. 2016;4(9):e617–e626. doi:10.1016/S2214-109X
19. UNHCR. The UN refugee agency. Global trends forced displacement in 2018. United Nations high commissioner for refugees, field information and coordination support section, division of program support and management, case postale 2500, 1211 Geneva, Switzerland; 2017. Available from: https://www.unhcr.org/5d08d7ee7.pdf.
20. Schockaert L, Venables E, Gil-Bazo MT, Barnwell G, Gerstenhaber R, Whitehouse K. Behind the scenes of South Africa’s asylum procedure: a qualitative study on long-term asylum-seekers from the Democratic Republic of Congo. Refug Surv Q. 2020;39(1):26–55. doi:10.1093/rsq/hdz018
21. Nicholson F, Kumin J A guide to international refugee protection and building state asylum systems. Jointly published by UNHCR, The UN Refugee Agency, Case Postale 2500, 1211 Geneva, Switzerland; and Inter-Parliamentary Union and the United Nations, Chemin du Pommier 5, Case Postale 330, 1218 Le Grand-Saconnex, Geneva – switzerland; 2017. Available from: https://www.unhcr.org/3d4aba564.pdf.
22. UNHCR. The UN refugee agency. action against sexual and gender-based violence: an updated strategy. Division of international protection; 2011 Available from: https://cms.emergency.unhcr.org/documents/11982/51689/UNHCR%2C+Action+Against+Sexual+and+Gender-based+Violence.+An+Updated+Strategy%2C+2011/4f9d2a1c-280e-4ac8-a832-1a789de63d46#:~:text=To%20assist%20operations%20in%20addressing,multi%2Dsectoral%20and%20interagency%20approach.
23. ITUC. Violence in DRC. ITUC, International Trade Union conference violence against women in Eastern Democratic Republic of Congo: whose responsibility? Whose complicity? 2011. Available from: https://www.ituc-csi.org/IMG/pdf/ituc_violence_rdc_eng_lr.pdf.pdf.
24. Home Office, UK. Country policy and information note Democratic Republic of Congo (DRC): women fearing gender-based harm or violence. 5th Floor, Globe House, 89 Eccleston Square, London, SW1V 1PN; 2017. Available from: https://www.refworld.org/pdfid/5954bb664.pdf.
25. Bleckner J. From rhetoric to reality: a pragmatic analysis of the integration of women into UN peacekeeping operations. J Int Peacekeeping. 2013;17(3–4):337–360. doi:10.1163/18754112-1704009
26. Peterman A, Palermo T, Bredenkamp C. Estimates and determinants of sexual violence against women in the Democratic Republic of Congo. Am J Public Health. 2011;101(6):1060–1067. doi:10.2105/AJPH.2010.300070
27. Truscott A. Congo ceasefire brings little relief for women. CMAJ. 2008;179(2):133–134. doi:10.1503/cmaj.080946
28. Baaz ME, Stern M Sexual violence as a weapon of war? Perceptions, prescriptions, problems in the Congo, and beyond. The Nordic Africa Institute, PO Box 1703, SE-751 47 Uppsala, Sweden. Zed Books Ltd, 7 Cynthia Street, London N1 9JF, UK and Room 400, 175 Fifth Avenue, New York, NY 10010, USA; 2013. Available from: https://uu.diva-portal.org/smash/get/diva2:1148245/FULLTEXT01.pdf.
29. Peltola L Rape as a weapon of war and genocide: an examination of its historical and contemporary tactical uses, effects on victims and societies and psychological explanations; 2012. Available from: https://www.cmc.edu/sites/default/files/humanrights/Rape%20as%20a%20tool%20of%20war.pdf.
30. Brown C. Rape as a weapon of war in the Democratic Republic of the Congo. Torture. 2012;22(1):24–37.
31. UNHCR. The UN refugee agency. Sexual and gender-based violence prevention and response in refugee situations in the Middle East and North Africa; 2015. Available from: https://www.refworld.org/pdfid/568f9a014.pdf.
32. Mootz JJ, Stabb SD, Mollen D. Gender-based violence and armed conflict: a community-informed socioecological conceptual model from Northeastern Uganda. Psychol Women Q. 2017;41(3):368–388. doi:10.1177/0361684317705086
33. International Rescue Committee. Experiences of refugee women and girls from the Democratic Republic of Congo (DRC): learning from IRC’s women’s protection and empowerment programs in DRC, Tanzania, Burundi, and Uganda; 2014. Available from: https://ethnomed.org/wp-content/uploads/2020/02/IRC-Backgrounder-on-Congolese-Women-and-Girls.pdf.
34. UNHCR. The UN refugee agency. Sexual and gender-based violence against refugees, returnees, and internally displaced persons. Guidelines for prevention and response; 2003. Available from: https://www.unhcr.org/en-my/protection/women/3f696bcc4/sexual-gender-based-violence-against-refugees-returnees-internally-displaced.html.
35. Simon-Butler A, McSherry B. Defining sexual and gender-based violence in the refugee context. IRiS, Institute for research into superdiversity, University of Birmingham, IRiS Working Paper Series, No.: 2/2019; 2019. Available from: https://socialequity.unimelb.edu.au/__data/assets/pdf_file/0020/3012176/Defining-Sexual-and-Gender-Based-Violence-in-the-Refugee-Context.pdf.
36. Malemo Kalisya L, Lussy Justin P, Kimona C, et al. Sexual violence toward children and youth in war-torn eastern Democratic Republic of Congo. PLoS One. 2011;6(1):e15911. doi:10.1371/journal.pone.0015911
37. Bartels SA, Scott JA, Leaning J, et al. Sexual violence trends between 2004 and 2008 in South Kivu, Democratic Republic of Congo. Prehosp Disaster Med. 2011;26(6):408–413. doi:10.1017/S1049023X12000179
38. Bartels S, Kelly J, Scott J, et al. Militarized sexual violence in South Kivu, Democratic Republic of Congo. J Interpers Violence. 2013;28(2):340–358. doi:10.1177/0886260512454742
39. Women ’s Refugee Commission. Refugee girls. The invisible faces of war. In memory of Mary Diaz 1960–2004. Pearson Foundation, 122 East 42nd Street New York, NY 10168-1289; 2009. Available from: https://www.refworld.org/pdfid/4a7835fa2.pdf.
40. Pittaway E. Making mainstreaming a reality – gender and the UNHCR policy on refugee protection and solutions in urban areas. A refugee perspective. center for refugee research, school of social science and international health, UNSW Sydney NSW 2052 Australia; 2010. Available from: https://www.unhcr.org/4b0bb83f9.pdf.
41. Inter-agency field manual on reproductive health in humanitarian settings: 2010 revision for field review. Geneva: inter-agency working group on reproductive health in crises; 2010. 8, gender-based violence. Available from: https://www.ncbi.nlm.nih.gov/books/NBK305160/.
42. Lincoln RS. Recent developments rule of law for whom? Strengthening the rule of law as a solution to sexual violence in the Democratic Republic of the Congo’. Berkeley J Gender Law Justice. 2011;26:139–167.
43. Harbishettar V, Math SB. Violence against women in India: comprehensive care for survivors. Indian J Med Res. 2014;140(2):157–159.
44. Linos N, Slopen N, Berkman L, Subramanian SV, Kawachi I. Predictors of help-seeking behavior among women exposed to violence in Nigeria: a multilevel analysis to evaluate the impact of contextual and individual factors. J Epidemiol Community Health. 2014;68(3):211–217. doi:10.1136/jech-2012-202187
45. Palermo T, Bleck J, Peterman A. Tip of the iceberg: reporting and gender-based violence in developing countries. Am J Epidemiol. 2014;179(5):602–612. doi:10.1093/aje/kwt295
46. Beydoun HA, Beydoun MA. Invited commentary: disclosure of gender-based violence in developing countries. Am J Epidemiol. 2014;179(5):613–618. doi:10.1093/aje/kwt296
47. Sinko L, Burns CJ, O’Halloran S, Saint Arnault D. Trauma recovery is cultural: understanding shared and different healing themes in Irish and American survivors of gender-based violence. J Interpers Violence. 2019;19:0886260519829284.
48. Anema A, Joffres MR, Mills E, Spiegel PB. Widespread rape does not directly appear to increase the overall HIV prevalence in conflict-affected countries: so now what? Emerg Themes Epidemiol. 2008;5:11. doi:10.1186/1742-7622-5-11
49. Spiegel PB, Bennedsen AR, Claass J, et al. Prevalence of HIV infection in conflict-affected and displaced people in seven sub-Saharan African countries: a systematic review. Lancet. 2007;369(9580):2187–2195. doi:10.1016/S0140-6736(07)61015-0
50. Bennett BW, Marshall BD, Gjelsvik A, McGarvey ST, Lurie MN. HIV incidence prior to, during, and after violent conflict in 36 Sub-Saharan African Nations, 1990–2012: an ecological study. PLoS One. 2015;10(11):e0142343. doi:10.1371/journal.pone.0142343
51. Burgueño E, Carlos S, Lopez-Del Burgo C, et al. Forced sexual intercourse and its association with HIV status among people attending HIV voluntary counseling and testing in a healthcare center in Kinshasa (DRC). PLoS One. 2017;12(12):e0189632. doi:10.1371/journal.pone.0189632
52. Supervie V, Halima Y, Blower S. Assessing the impact of mass rape on the incidence of HIV in conflict-affected countries. AIDS. 2010;24(18):2841–2847. doi:10.1097/QAD.0b013e32833fed78
53. USAID. From the American People. Democratic Republic of the Congo: global health; 2014. Available from: https://www.usaid.gov/democratic-republic-congo/global-health.
54. Kim AA, Malele F, Kaiser R, et al. HIV infection among internally displaced women and women residing in river populations along the Congo River, Democratic Republic of Congo. AIDS Behav. 2009;13(5):914–920. doi:10.1007/s10461-009-9536-z
55. Amodu OC, Richter MS, Salami BO. A scoping review of the health of conflict-induced internally displaced women in Africa. Int J Environ Res Public Health. 2020;17(4):1280. doi:10.3390/ijerph17041280
56. Mock NB, Duale S, Brown LF, et al. Conflict and HIV: a framework for risk assessment to prevent HIV in conflict-affected settings in Africa. Emerg Themes Epidemiol. 2004;1(1):6. doi:10.1186/1742-7622-1-6
57. Venis S, Horton R. Violence against women: a global burden. Lancet. 2002;359(9313):1172. doi:10.1016/S0140-6736(02)08251-X
58. Watts C, Zimmerman C. Violence against women: global scope and magnitude. Lancet. 2002;359(9313):1232–1237. doi:10.1016/S0140-6736(02)08221-1
59. Guruge S. Intimate partner violence: a global health perspective. Can J Nurs Res. 2012;44(4):36–54.
60. Slegh H, Barker G, Levtov R. Gender relations, sexual and gender-based violence and the effects of conflict on women and men in North Kivu, Eastern Democratic Republic of the Congo. Results from the international men and gender equality survey (images) final report – 2014; 2014. Available from: https://promundoglobal.org/wp-content/uploads/2014/12/Gender-Relations-Sexual-and-Gender-Based-Violence-and-the-Effects-of-Conflict-on-Women-and-Men-in-North-Kivu-Eastern-DRC-Results-from-IMAGES.pdf.
61. Lusey H, San Sebastian M, Christianson M, Edin KE. Prevalence and correlates of gender inequitable norms among young, church-going women and men in Kinshasa, Democratic Republic of Congo. BMC Public Health. 2018;18(1):887. doi:10.1186/s12889-018-5742-9
62. Trani JF, Bakhshi P. Vulnerability and mental health in Afghanistan: looking beyond war exposure. Transcult Psychiatry. 2013;50(1):108–139. doi:10.1177/1363461512475025
63. Muuo S, Muthuri SK, Mutua MK, et al. Barriers and facilitators to care-seeking among survivors of gender-based violence in the Dadaab refugee complex. Sex Reprod Health Matters. 2020;28(1):1722404. doi:10.1080/26410397.2020.1722404
64. Buvinic M, Gupta MD, Casabonne U, Verwimp P. Violent conflict and gender inequality: an overview. HiCN working paper 129. Households in conflict network, the Institute of Development Studies - at the University of Sussex - Falmer - Brighton - BN1 9RE. Available from: https://promundoglobal.org/wp-content/uploads/2014/12/Gender-Relations-Sexual-and-Gender-Based-Violence-and-the-Effects-of-Conflict-on-Women-and-Men-in-North-Kivu-Eastern-DRC-Results-from-IMAGES.pdf.
65. UNFPA, United Nations Populations Fund. The impact of armed conflict on women and girls. A consultative meeting on mainstreaming gender in areas of conflict and reconstruction. Bratislava, Slovakia; 2001. Available from: https://www.unfpa.org/sites/default/files/pub-pdf/impact_conflict_women.pdf.
66. Murthy RS, Lakshminarayana R. Mental health consequences of war: a brief review of research findings. World Psychiatry. 2006;5(1):25–30.
67. Vlassoff C. Gender differences in determinants and consequences of health and illness. J Health Popul Nutr. 2007;25(1):47–61.
68. Vojdik VK. Sexual violence against men and women in war: a masculinities approach. Nev LJ. 2013;14:923.
69. Kirschner S, Miller A. Does peacekeeping really bring peace? Peacekeepers and combatant-perpetrated sexual violence in civil wars. J Confl Resolut. 2019;63(9):2043–2070.
70. Ferstman C. Reparation for sexual exploitation and abuse in the (Post) conflict context: the need to address abuses by peacekeepers and humanitarian aid workers. In reparations for victims of genocide, war crimes and crimes against humanity. Brill Nijhoff. 2020;271–297.
71. Bartels S, Scott J, Leaning J, Mukwege D, Lipton R, VanRooyen M. Surviving sexual violence in the Eastern Democratic Republic of Congo. J Int Women Stud. 2010;11(4):37–49.
72. Burkhardt G, Scott J, Onyango MA, et al. Sexual violence-related pregnancies in eastern Democratic Republic of Congo: a qualitative analysis of access to pregnancy termination services. Confl Health. 2016;10:30. doi:10.1186/s13031-016-0097-2
73. Johnson K, Scott J, Rughita B, et al. Association of sexual violence and human rights violations with physical and mental health in territories of the Eastern Democratic Republic of the Congo. JAMA. 2010;304(5):553–562. doi:10.1001/jama.2010.1086
74. Mowafi H. Conflict, displacement and health in the Middle East. Glob Public Health. 2011;6(5):472–487. doi:10.1080/17441692.2011.570358
75. Walfield SM. “Men cannot be raped”: correlates of male rape myth acceptance. J Interpers Violence. 2018;886260518817777. doi:10.1177/0886260518817777
76. Fakunmoju SB, Abrefa-Gyan T, Maphosa N, et al. Rape myth acceptance: gender and cross-national comparisons across the United States, South Africa, Ghana, and Nigeria. Sex Cult. 2020. doi:10.1007/s12119-020-09755-z
77. Canan SN, Jozkowski KN, Crawford BL. Sexual assault supportive attitudes: rape myth acceptance and token resistance in Greek and Non-Greek College students from two university samples in the United States. J Interpers Violence. 2018;33(22):3502–3530. doi:10.1177/0886260516636064
78. Vonderhaar RL, Carmody DC. There are no “innocent victims”: the influence of just world beliefs and prior victimization on rape myth acceptance. J Interpers Violence. 2015;30(10):1615–1632. doi:10.1177/0886260514549196
79. van Wieringen K. To counter the rationality of sexual violence: existing and potential policies against the genocidal use of rape as a weapon of war in the Democratic Republic of Congo. Int J Humanitarian Action. 2020;5(8). doi:10.1186/s41018-020-00074-4
80. Jewkes R, Sen P, Garcia-Moreno C. Sexual Violence, Chapter 6. In: Krug EG, Dahlberg LL, Mercy JA, Zwi AB, Lozano R, editors. World Report on Violence and Health. Geneva, Switzerland: World Health Organization; 2002:147–182.
81. Kelly J, Albutt K, Kabanga J, Anderson K, VanRooyen M. Rejection, acceptance and the spectrum between: understanding male attitudes and experiences towards conflict-related sexual violence in eastern Democratic Republic of Congo. BMC Womens Health. 2017;17(1):127. doi:10.1186/s12905-017-0479-7
82. Reed E, Gupta J, Biradavolu M, Devireddy V, Blankenship KM. The context of economic insecurity and its relation to violence and risk factors for HIV among female sex workers in Andhra Pradesh, India. Public Health Rep. 2010;125(Suppl4):81–89. doi:10.1177/00333549101250S412
83. Food and Agriculture Organization of the United Nations (FAO), Dimitra Project. Guidance Note. Gender-based violence and livelihood interventions: focus on populations of humanitarian concern in the context of HIV; 2010. Available from: http://www.fao.org/fileadmin/templates/dimitra/pdf/guidance_note_gbv_livelihoods.pdf.
84. Austin J, Guy S, Lee-Jones L, McGinn T, Schlecht J. Reproductive health: a right for refugees and internally displaced persons. Reprod Health Matters. 2008;16(31):10–21. doi:10.1016/S0968-8080(08)31351-2
85. Orach CG, Musoba N, Byamukama N, et al. Perceptions about human rights, sexual and reproductive health services by internally displaced persons in northern Uganda. Afr Health Sci. 2009;9(Suppl2):S72–S80.
86. Duarte-Gómez MB, Cuadra-Hernández SM, Ruiz-Rodríguez M, Arredondo A, Cortés-Gil JD. Challenges of health services related to the population displaced by violence in Mexico. Rev Saude Publica. 2018;52:77. doi:10.11606/S1518-8787.2018052017094
87. Ozcurumez S, Akyuz S, Bradby H. The conceptualization problem in research and responses to sexual and gender-based violence in forced migration. J Gender Stud. 2020;1–3.
88. Anani G. Dimensions of gender-based violence against Syrian refugees in Lebanon. Forced Migr Rev. 2013;44.
89. Rettberg JW, Gajjala R. Terrorists or cowards: negative portrayals of male Syrian refugees in social media. Fem Media Stud. 2016;16(1):178–181.
90. Grabska K. Constructing ‘modern gendered civilised’women and men: gender-mainstreaming in refugee camps. Gend Dev. 2011;19(1):81–93.
91. Sturm G, Baubet T, Moro MR. Mobilising Social and Symbolic Resources in Transcultural Therapies with Refugees and Asylum Seekers: The Story of Mister Diallo. InVoices of Trauma. Boston, MA: Springer; 2007:211–231.
92. Keygnaert I, Dias SF, Degomme O, et al. Sexual and gender-based violence in the European asylum and reception sector: a perpetuum mobile? Eur J Public Health. 2015;25(1):90–96.
93. Phillimore J, Pertek S, Alidou L Sexual and gender-based violence and refugees. The impacts of and on integration domains’. IRiS Working Paper Series. 2018.
94. Presidency of The Republic. Law n ° 06/018 of July 20, 2006 modifying and supplementing the Decree of January 30, 1940 on the Congolese Penal Code DRC (2006). Kinshasa; 2006. Available from: http://www.leganet.cd/Legislation/DroitPenal/Loi.06.018.20.07.3006.htm.
95. United Nations. Consideration of reports submitted by States parties under article 18 of the convention on the elimination of all forms of discrimination against women. Combined sixth and seventh periodic report of States parties. Democratic Republic of the Congo (CEDAW/C/COD/6-7). Convention on the elimination of all forms of discrimination against women; 2011. Available from: https://www.refworld.org/docid/51dd39374.html.
96. United Nations Human Rights. Office of the High Commissioner. Committee on the elimination of discrimination against women examines the situation of women’s rights in the Democratic Republic of the Congo; 2019. Available from: https://www.ohchr.org/EN/NewsEvents/Pages/DisplayNews.aspx?NewsID=24820&LangID=E.
97. Medie PA. Fighting gender-based violence: the women’s movement and the enforcement of rape law in Liberia. Afr Aff (Lond). 2013;112(448):377–397.
98. United Nations Development Group. Tenth consolidated annual progress report on activities implemented under the UN action against sexual violence in conflict fund report of the administrative agent of the UN action against sexual violence in conflict fund for the period 1 January – 31 December 2018. Multi-Partner Trust Fund Office, Bureau of Management, United Nations Development Programme (UNDP); 2019. Available from: https://www.un.org/sexualviolenceinconflict/wp-content/uploads/2019/06/report/un-action-progress-report-2018/20190531-2018-UN-Action-Annual-Progress-Report.pdf.
99. Steiner B, Benner MT, Sondorp E, Schmitz KP, Mesmer U, Rosenberger S. Sexual violence in the protracted conflict of DRC programming for rape survivors in South Kivu. Confl Health. 2009;3:3. doi:10.1186/1752-1505-3-3
100. Bartels SA, Scott JA, Leaning J, et al. Demographics and care-seeking behaviors of sexual violence survivors in South Kivu province, Democratic Republic of Congo. Disaster Med Public Health Prep. 2012;6(4):393–401. doi:10.1001/dmp.2012.66
101. United Nations High Commissioner for Refugees, Policy Development and Evaluation Service (PDES). Evaluation of UNHCR’s efforts to prevent and respond to sexual and gender-based violence in situations of forced displacement. PDES/2008/08; 2008. Available from: https://www.unhcr.org/48ea31062.pdf.
102. The World Bank. World bank project aims to tackle gender-based violence in DRC by focusing on prevention; 2018. Available from: https://www.worldbank.org/en/news/press-release/2018/08/30/world-bank-project-aims-to-tackle-gender-based-violence-in-drc-by-focusing-on-prevention.
103. Elbert T, Hinkel H, Maedl A, et al. Sexual and gender-based violence in the Kivu Provinces of the Democratic Republic of Congo: insights from former combatants. World Bank, Washington, DC: © World Bank; 2013. Available from: https://openknowledge.worldbank.org/handle/10986/17852.
104. Bolton L Barriers to education for girls in the Democratic Republic of Congo. K4D helpdesk report 750. Brighton, UK: Institute of Development Studies; 2020. Available from: https://assets.publishing.service.gov.uk/media/5e9d7f36e90e07049b74becd/750_Barriers_to_education_for_girls_in_DRC.pdf.
105. Boumaiza IG Bridging the gender gap in the Democratic Republic of Congo. Global partnership for education. 1850 K Street N.W., Suite 625, Washington D.C., 20006, USA. 2020. Available from: https://www.globalpartnership.org/blog/bridging-gender-gap-democratic-republic-congo.
106. Bradshaw EA, Kramer RC. State-corporate crime. In: Bruinsma G, Weisburd D, editors. Encyclopedia of Criminology and Criminal Justice. New York, NY: Springer; 2014.
107. Mullins CW, Rothe DL. Gold, diamonds and blood: international state-corporate crime in the Democratic Republic of the Congo 1. J Contemp Justice Rev. 2008;11(2):81–90. doi:10.1080/10282580802057678
108. Elizabeth Glaser Pediatric AIDS Foundation. Review of the Democratic Republic of the Congo (DRC) by the Committee on the Elimination of Discrimination Against Women (CEDAW); 2013. Available from: https://tbinternet.ohchr.org/Treaties/CEDAW/Shared%20Documents/COD/INT_CEDAW_NGO_COD_13429_E.pdf.
109. UN Committee on the Elimination of All Forms of Discrimination Against Women. Gender-based violence and discrimination against women and girls in the Democratic Republic of the Congo. A report for the UN Committee on the elimination of all forms of discrimination against women; 2018. Available from: https://tbinternet.ohchr.org/Treaties/CEDAW/Shared%20Documents/COD/INT_CEDAW_ICO_COD_32830_E.pdf.
110. Tenai NK. Impoverishing and dehumanising violence against women: an opportunity for service by churches in Eastern Democratic Republic of Congo. Verbum Et Ecclesia. 2017;38(1):1–10. doi:10.4102/ve.v38i1.1634
111. Basile KC. A comprehensive approach to sexual violence prevention. N Engl J Med. 2015;372(24):2350–2352. doi:10.1056/NEJMe1503952
112. Garcia CM, Lechner KE, Frerich EA, Lust KA, Eisenberg ME. Preventing sexual violence instead of just responding to it: students’ perceptions of sexual violence resources on campus. J Foren Nurs. 2012;8(2):61–71. doi:10.1111/j.1939-3938.2011.01130.x
113. Freedman J. Treating Sexual Violence as a “Business”: Reflections on National and International Responses to Sexual and Gender-Based Violence in the Democratic Republic of Congo, Gendered Perspectives on Conflict and Violence: Part B (Advances in Gender Research). Vol. 18B. Emerald Group Publishing Limited; 2014:125–143. doi:10.1108/S1529-21262014000018B009
114. Freedman J. Gender, Violence and Politics in the Democratic Republic of Congo. 2 & 4 Park Square, Milton Park, Abingdon, OX14 4RN, UK: Routledge; Taylor & Francis Group; 2016.
115. Thabethe N, Magezi V, Nyuswa M. Micro-credit as a community development strategy: a South African case study. Commun Dev J. 2012;47(3):423–435. doi:10.1093/cdj/bsr042
116. de Wet A, Parker G. Communities in Conversation: opportunities for women and girls‘ self-empowerment. Gender Dev. 2014;22(1):109–125. doi:10.1080/13552074.2014.889341
117. Schmitt C 16 days of activism: countering sexual and gender-based violence across the Congo. UNHCR offices and some 10,000 people across the country spread awareness about the scourge in a series of events marking the annual 16 days campaign. UNHCR. Available from: https://www.unhcr.org/52a6d5e16.html.
118. Ditekemena J, Koole O, Engmann C, et al. Determinants of male involvement in maternal and child health services in sub-Saharan Africa: a review. Reprod Health. 2012;9(1):32. doi:10.1186/1742-4755-9-32
119. Manjate Cuco RM, Munguambe K, Bique Osman N, Degomme O, Temmerman M, Sidat MM. Male partners’ involvement in prevention of mother-to-child HIV transmission in sub-Saharan Africa: a systematic review. SAHARA J. 2015;12:87–105. doi:10.1080/17290376.2015.1123643
120. Koo K, Makin JD, Forsyth BWC. Barriers to male-partner participation in programs to prevent mother-to-child HIV transmission in South Africa. AIDS Educ Prev. 2013;25(1):14–24. doi:10.1521/aeap.2013.25.1.14
121. Magnussen L, Ehiri J, Jolly P. Comprehensive versus selective primary health care: lessons for global health policy. Health Aff (Millwood). 2004;23(3):167–176. doi:10.1377/hlthaff.23.3.167
122. Simwaka BN, Bello G, Banda H, Chimzizi R, Squire BS, Theobald SJ. The Malawi National Tuberculosis programme: an equity analysis. Int J Equity Health. 2007;6(1):24. doi:10.1186/1475-9276-6-24
123. White F. Primary health care and public health: foundations of universal health systems. Med Princ Pract. 2015;24(2):103–116. doi:10.1159/000370197
124. Thomas SL, Wakerman J, Humphreys JS. Ensuring equity of access to primary health care in rural and remote Australia - what core services should be locally available? Int J Equity Health. 2015;14(1):111. doi:10.1186/s12939-015-0228-1
125. Haque M, Islam T, Rahman NAA, McKimm J, Abdullah A, Dhingra S. Strengthening primary health-care services to help prevent and control long-term (chronic) non-communicable diseases in low- and middle-income countries. Risk Manag Healthc Policy. 2020;13:409–426. doi:10.2147/RMHP.S239074
126. United Nations Population Fund. Making reproductive rights and sexual and reproductive health a reality for all. Reproductive rights and sexual and reproductive health framework. UNFPA; 2011. Available from: https://www.unfpa.org/resources/making-reproductive-rights-and-sexual-and-reproductive-health-reality-all.
127. Narasimhan M, Loutfy M, Khosla R, Bras M. Sexual and reproductive health and human rights of women living with HIV. J Int AIDS Soc. 2015;18(6Suppl 5):20834. doi:10.7448/IAS.18.6.20834
128. Amin A. Addressing gender inequalities to improve the sexual and reproductive health and wellbeing of women living with HIV. J Int AIDS Soc. 2015;18(Suppl 5):20302. doi:10.7448/IAS.18.6.20302
129. Askew I, Berer M. The contribution of sexual and reproductive health services to the fight against HIV/AIDS: a review. Reprod Health Matters. 2003;11(22):51–73. doi:10.1016/s0968-8080(03)22101-7
130. Alzate MM. The sexual and reproductive rights of internally displaced women: the embodiment of Colombia’s crisis. Disasters. 2008;32(1):131–148. doi:10.1111/j.1467-7717.2007
131. Crisp J, Morris T, Refstie H. Displacement in urban areas: new challenges, new partnerships. Disasters. 2012;36(Suppl 1):S23–S42. doi:10.1111/j.1467-7717.2012
132. Vega J, Irwin A. Tackling health inequalities: new approaches in public policy. Bull World Health Organ. 2004;82(7):482.
133. Baker EA, Metzler MM, Galea S. Addressing social determinants of health inequities: learning from doing. Am J Public Health. 2005;95(4):553–555. doi:10.2105/AJPH.2005.061812
134. UN Women. The United Nations entity for gender equality and the empowerment of women. Women and sustainable development goals; 2015. Available from: https://sustainabledevelopment.un.org/content/documents/2322UN%20Women%20Analysis%20on%20Women%20and%20SDGs.pdf.
135. United Nations High Commissioner for Refugees (UNHCR). Sexual violence against refugees; 1995. Available from: https://www.refworld.org/pdfid/3ae6b33e0.pdf.
136. Birn AE, Pillay Y, Holtz T. Textbook of International Health: Global Health in a Dynamic World.
137. García-Moreno C, Zimmerman C, Morris-Gehring A, et al. Addressing violence against women: a call to action. Lancet. 2015;385(9978):1685–1695.
138. Read-Hamilton S, Marsh M. The communities care programme: changing social norms to end violence against women and girls in conflict-affected communities. Gend Dev. 2016;24(2):261–276.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.