Back to Journals » Clinical Optometry » Volume 18
Sex Differences in Preferred Under-Correction of Contact Lenses and Their Potential Relevance to Presbyopia Management
Authors Ayaki M ![]() , Hanyuda A, Negishi K
, Hanyuda A, Negishi K ![]()
Received 21 October 2025
Accepted for publication 24 February 2026
Published 27 February 2026 Volume 2026:18 575883
DOI https://doi.org/10.2147/OPTO.S575883
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Chris Lievens
Masahiko Ayaki,1,2 Akiko Hanyuda,1 Kazuno Negishi1
1Department of Ophthalmology, Keio University School of Medicine, Shinjuku-ku, Tokyo, Japan; 2Otake Eye Clinic, Yamatoshi, Kanagawa, Japan
Correspondence: Masahiko Ayaki, Department of Ophthalmology, Keio University School of Medicine, 35 Shinanomachi, Shinjuku-ku, Tokyo, 160-8582, Japan, Email [email protected] Kazuno Negishi, Department of Ophthalmology, Keio University School of Medicine, 35 Shinanomachi, Shinjuku-ku, Tokyo, 160-8582, Japan, Email [email protected]
Purpose: The aim of this study was to determine sex differences in preferred refraction for presbyopic correction in daily life, determined by the power of prescribed contact lenses.
Patients and methods: Near add power and preferred contact lens power were examined in participants aged from 20 to 79 years who were divided into three age groups (20– 39, 40– 59, and 60– 79 years). The difference (Δ) in lens power (preferred corrective power of contact lens – full correction power) was compared between both sexes in each age group. Regression analysis was conducted to explore the relationship between Δ lens power and ocular parameters.
Results: A total of 768 men and 2314 women were enrolled in the study. Sex differences were prominent in the 40– 59 year age group; namely Δ lens power was larger (P < 0.05) and visual acuity with contact lenses was lower in women than men (P < 0.05), whilst astigmatic errors and anisometropia were greater in men than women. Mean near add power was similar between both sexes in all age groups. Ocular surface parameters were worse in women compared with men, except for the Shirmer test. The results of regression analyses indicated that Δ lens power for women was associated with myopic spherical equivalent, astigmatic errors, anisometropia, near add power, contact lens power, and visual acuity with contact lenses. For men, Δ lens power was associated with myopic spherical equivalent, astigmatic errors, visual acuity with contact lenses, and tear break-up time. Age was not a significant factor for either sex.
Conclusion: The current results revealed sex differences in the preferred power of contact lenses for presbyopic correction for optimal daily living. The magnitude of under-correction was significantly greater in women than men aged 40 to 59 years.
Keywords: presbyopia, near add power, accommodation, near vision, sex differences
Introduction
Presbyopia is a natural aging process involving the gradual loss of the eye’s ability to focus on nearby objects, and its symptoms generally occur in the early to mid-40s.1 This condition arises due to lens hardening and ciliary muscle dysfunction.2,3 There are several corrective options available for presbyopia, such as reading glasses, bifocal lenses, progressive lenses, or contact lenses. Additionally, surgical interventions, including corneal and lens surgery, can provide effective results in some cases.4 Suggested risk factors for presbyopia include age,5 smoking,6 diabetes,7 the female sex,8 dry eye,9 and glaucoma.10–12 However, apart from age and glaucoma, evidence confirming these risk factors is still scarce.
Sex differences in presbyopia have been discussed in terms of work at arm’s length and habitual near work8; however, data of actual visual acuity and refraction are lacking to quantify the magnitude of presbyopia difference between men and women. For millions of years since ancient times, men have used far vision for hunting and women have used near vision for agriculture, housekeeping, and babysitting.13 Recently, smartphones and digitalization have been introduced, and both sexes now use near vision equally in daily life. The mean percentages of time dedicated to distance, intermediate, and near vision is currently reported to be 27.25% ± 11.93% (range, 5%–65%), 30.23% ± 9.36% (range, 12%–50%), and 42.53% ± 14.96% (range, 13%–78%), respectively, indicating that near vision in both men and women is most frequently used in daily life.14 In addition, clinical investigations have suggested that there is no difference in near add power between men and women.1 Soler et al assessed differences in visual working distance and mobile phone usage distance and found working distance was significantly longer than mobile phone usage distance (82.5 ± 150.6 cm vs 31.9 ± 6.3 cm, P < 0.001), whereas no significant differences were found between arm length (74.3 ± 4.8 cm) and working distance.15 Leffler et al explored clinical predictors of the optimal spectacle correction for comfort when performing desktop tasks and found, using univariate analyses, a significant predictor of the most comfortable correction was age, while arm length and accommodative amplitude were not significant predictors.16 Thus, further investigation of the preferred refraction for men and women in modern society is necessary.
Contact lens power is a relevant indicator of habitual visual acuity for the general population because contact lenses are used for housekeeping, business, and driving during the whole day, even if near glasses are sometimes used in cases of focusing difficulty. Recent contact lens technologies are based on geometric and physiological optics. Vertex distance is important especially for prescription of high power. The perceived power is what the patient experiences on-eye and the compensated power is the mathematically adjusted contact lens power required for the same perceived effect. This is especially relevant for powers beyond ±4.00 D where vertexing errors become visually significant. There are relevant options for presbyopic strategy with contact lenses. Monovision is to correct one eye for distance vision and the fellow eye for near vision. Enhanced monovision modifies monovision by using a multifocal lens in one or both eyes. This approach preserves binocular visual function maintaining relatively stable distance visual acuity. Multifocal contact lenses use simultaneous-vision optics to deliver distance, intermediate, and near power at the same time. Across all presbyopic modalities, accurate vertex compensation ensures that the intended optical profile is delivered on-eye preventing over- or under-correction that could degrade multifocal performance or disrupt the delicate balance required for monovision strategies. Under-correction is used to intentionally reduce the lens power to the minimum level with acceptable distance vision while offering satisfactory near vision in both eyes. It is favored as an inexpensive and practical option.
The aim of this study was to determine any sex differences in preferred refraction during daily life, as determined by the power of prescribed contact lenses. We examined refraction, best corrected visual acuity, the power of contact lenses for daily use, distance visual acuity with contact lenses, and near add power. In addition, dry eye-related ocular parameters and retinal thickness were also compared since they are known to be associated with presbyopia.17
Methods
Study Design and Participants
This retrospective study was conducted at the Otake Eye Clinic in Kanagawa, Japan, and involved healthy individuals attending the clinic. The Institutional Review Board and Ethics Committee of the Kanagawa Medical Association approved the study (approval date: November 12, 2018; permission number: krec2059006), ensuring compliance with the Declaration of Helsinki. Consent requirements were waived by the Institutional Review Board of the Kanagawa Medical Association due to the opt-out nature of the study. The study involved a retrospective review of patient charts for consecutive patients visiting the eye clinic between December 2018 and April 2024. Additionally, the Institutional Review Board and Ethics Committee of Keio University School of Medicine approved this study (approval date: May 31, 2024; approval number: 20241019) to allow authorship by affiliated researchers (KN, AH, and MA) from Keio University School of Medicine. This study protocol was registered in the UMIN Clinical Trials Registry (UMIN000051891) on August 15, 2023.
Inclusion and Exclusion Criteria
Participants aged between 20 and 79 years with bilateral phakic eyes and a best-corrected distance visual acuity greater than 20/30 were included. Exclusion criteria encompassed prior corneal or intraocular surgeries, including ocular laser treatments and refractive or cataract procedures, moderate-to-severe cataracts, glaucoma, and macular diseases.
Ophthalmological Examinations
Ophthalmological evaluations included assessments of best-corrected visual acuity (Vision Chart, SSC-370R; Nidek Co., Ltd., Gamagori, Aichi, Japan), autorefractometry, intraocular pressure (TonorefTM II; Nidek Co., Ltd)., slit-lamp biomicroscopy, funduscopy, and automated perimetry (Humphrey Visual Field Analyzer Swedish Interactive Threshold Algorithm–Standard 24–2 program; Carl Zeiss Meditec, Dublin. CA, USA). Binocular near add power was measured at 30 cm using a Bankoku near-acuity chart (Handaya Inc., Tokyo, Japan). After determining the participant’s distance refractive correction, the minimal additional power required to achieve near acuity of 20/25 or better at 30 cm was recorded in increments of 0.25 D. The full correction power of the contact lens was converted under a corneal vertex distance of 13 mm, and the difference (Δ) in lens power was calculated as follows: [preferred corrective power of contact lens – full correction power]. Preferred refraction of the contact lens was defined as the perceived contact lens power selected by the patient during the clinic visit based on the refraction that provided optimal daily vision with the lens.
Dry eye assessments included the tear break-up time, Schirmer test, and corneal staining test. Tear break-up time was measured using a fluorescein filter paper strip (Ayumi Pharmaceutical, Tokyo, Japan) as the interval between the third blink and the appearance of the first dark spot on the cornea, averaged over three measurements. Corneal staining detected epitheliopathy.
Optical coherence tomography (RS-3000; Nidek Co., Ltd.) was used to assess the macular retinal nerve fiber layer (mRNFL), ganglion cell layer/inner plexiform layer, and combined mRNFL+ganglion cell layer/inner plexiform layer thickness across macular cube scans of a 6 × 6 mm area centered on the fovea. Peripapillary RNFL imaging involved raster scanning a 6 × 6 mm area around the optic disc at a scan density of 512 horizontal × 128 vertical A-scans. Measurements along a 3.45-mm diameter circle around the optic disc were automated.
Statistical Analysis
Patients were divided into three age groups: 20–39 years, 40–59 years, and 60–79 years. Demographics and ophthalmological parameters are presented as mean ± standard deviation for continuous variables and percentages for categorical variables in each group. Group comparisons based on sex were conducted using t-tests and chi-squared tests, as appropriate. Spearman correlation analyses evaluated the relationship between ophthalmic parameters and Δ lens power. Scatter plots visualized age-specific relationships between age and near add power, with regression lines and slopes computed using the least-squares method. Differences in slope ratios and correlation coefficients were compared between sexes using t-tests. Analyses were performed with StatFlex (Atech, Osaka, Japan), and a two-sided P-value < 0.05 was considered to indicate a significant difference.
Results
The patient charts of 3082 individuals (2314 women and 768 men) were analyzed, and the number of participants in each age group is indicated in Table 1. There was no sex difference in age, spherical equivalent, or near add power. Sex differences in refraction and visual acuity with contact lens were prominent in the 40–59-year age group; namely Δ lens power was larger (P < 0.05) and visual acuity with contact lenses was worse in women than men (P < 0.05), whilst astigmatic errors and anisometropia were greater in men than women (P < 0.01; Table 1). Ocular surface parameters were worse in women compared with men except for the Shirmer test. Sex differences in intraocular pressure and retinal thickness varied between age groups.
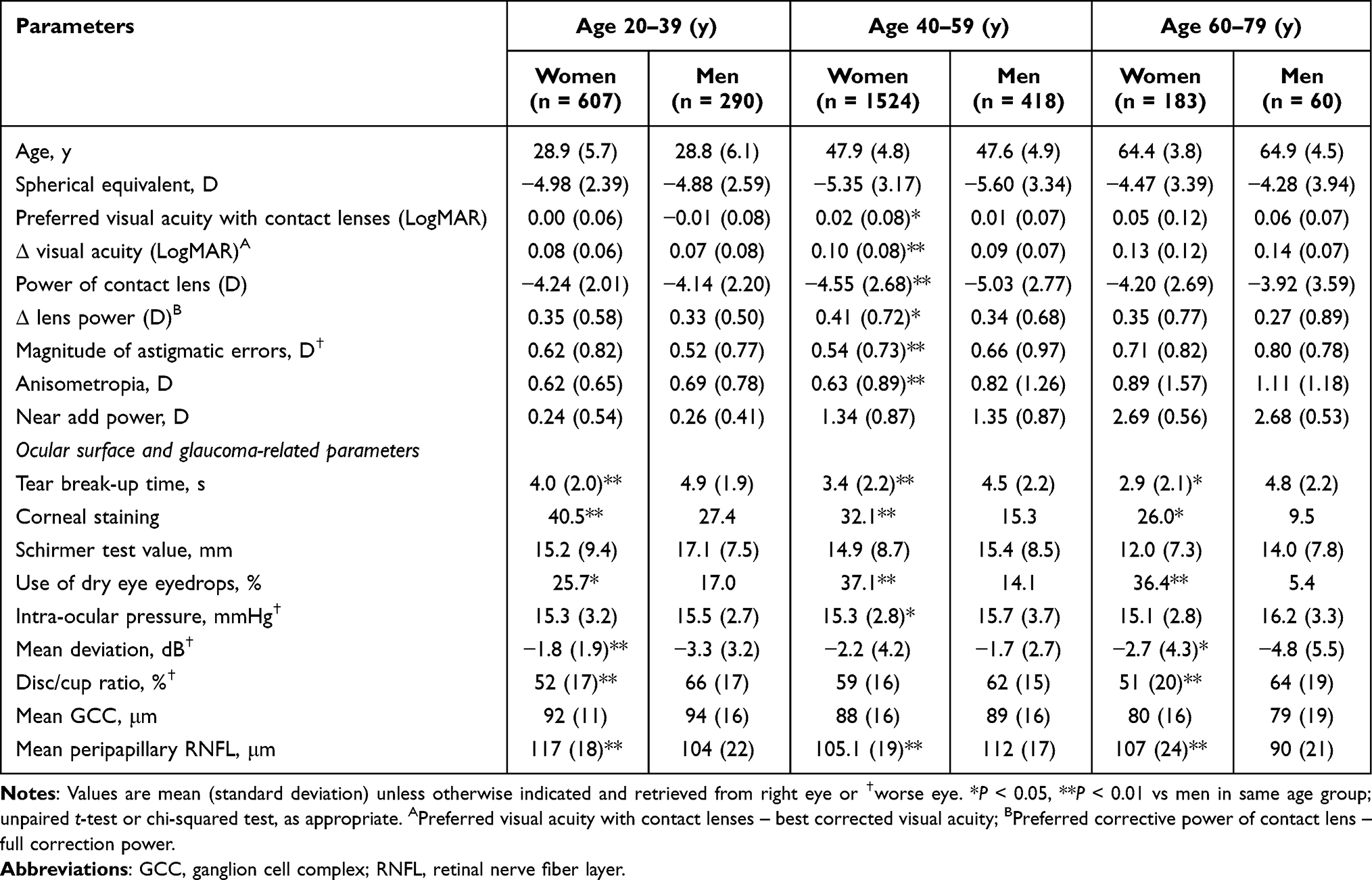 |
Table 1 Patient Demographics and Refractive Parameters |
Regression analyses indicated that Δ lens power in women was associated with myopic spherical equivalent, astigmatic errors, anisometropia, near add power, contact lens power, and visual acuity with contact lenses (Table 2). For men, Δ lens power was associated with myopic spherical equivalent, astigmatic errors, visual acuity with contact lenses, and tear break-up time. Age was not a significant factor for either sex. Scatter plots of age and near add power indicated the annual progression of near add power was similar in men (0.08 D/y) and women (0.08 D/y, P = 0.72). The correlation coefficient for men (r = 0.73) was similar to women (r = 0.72; P = 0.80; Figure 1). Ocular surface parameters were worse in women compared with men except for the Shirmer test. Sex differences in intraocular pressure and retinal thickness varied between age groups.
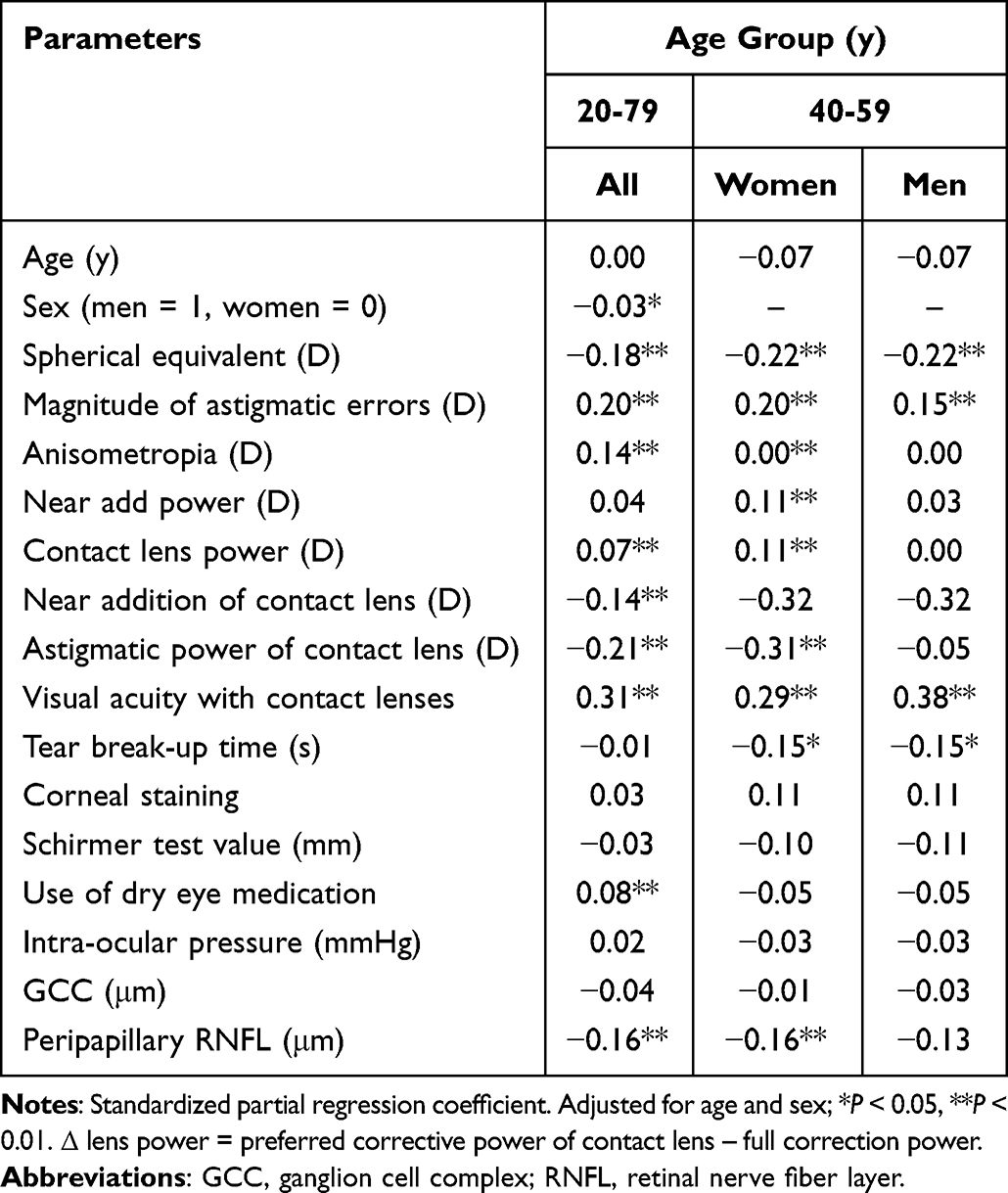 |
Table 2 Association Between Δ Lens Power and Patient Parameters |
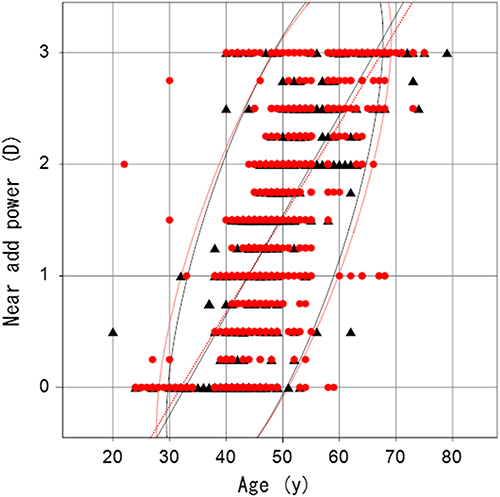 |
Figure 1 Scatter plots of age and near add power with regression lines and 95% probability eclipses. Annual progression of near add power was similar in men (0.08 D/y; black triangles, black regression line) and women (0.08 D/y; red circles, red regression line; P = 0.72). The correlation coefficient for men (r = 0.73) was similar to women (r = 0.72; P =0.80). Symbol overlap may cause an inaccurate representation of the number of participants. |
Regression analyses indicated that Δ lens power in women was associated with myopic spherical equivalent, astigmatic errors, anisometropia, near add power, contact lens power, and visual acuity with contact lenses (Table 2). For men, Δ lens power was associated with myopic spherical equivalent, astigmatic errors, visual acuity with contact lenses, and tear break-up time. Age was not a significant factor for either sex. Scatter plots of age and near add power indicated the annual progression of near add power was similar in men (0.08 D/y) and women (0.08 D/y, p=0.27). The correlation coefficient for men (r = 0.73) was similar to women (r = 0.72; P=0.80).
Discussion
The current results demonstrate sex differences in the under-correction of contact lenses for habitual refraction and distant visual acuity despite the near add power and the annual increase in near add power being similar in men and women (Table 1, Figures 1 and 2). The calculated under-correction (Δ lens power) of contact lenses compared with full correction power ranged from 0.41 to 0.27 D, depending on sex but not on age (Figure 2). A previous study1 compared Δ lens power between 106 men and 113 women aged from 40 to 59 years when presbyopia linearly progresses,12,17 and the Δ lens power was 0.26 ± 0.51 D for men and 0.51 ± 0.57 D for women (P < 0.01) which is similar to our current results. The sex difference in Δ lens power of 0.07 D in the current study is larger than a previous survey18 reporting the mean near addition in women to be 0.05–0.06 D higher than in men at the age of 45, 50, 55, and 60 years. Their results were from 888 optometrists responding to a mail-out survey relating to the near add power of spectacles sold to customers. This difference may be due to the results applying to spectacles rather than contact lenses, and there may also be racial and cultural differences.
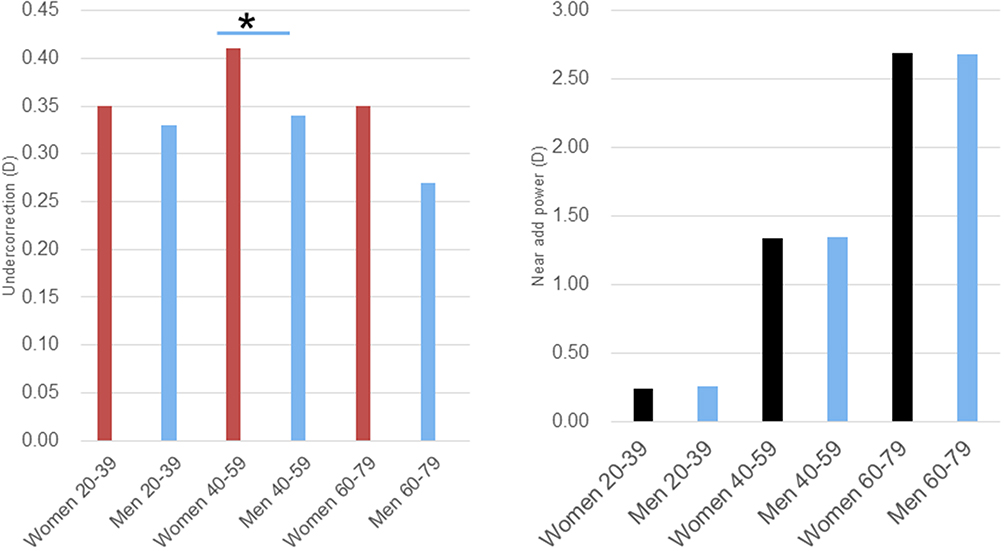 |
Figure 2 Sex differences in under-correction (left panel) and near add power (right panel) among the three age groups. There was a general tendency for the under-correction [preferred corrective power of contact lens – full correction power] of women to be greater than men, and this reached significance in the 40–59-year age group (*P < 0.05, significant difference between sexes). Mean near add power was similar for men and women in all age groups. |
Under-correction is a strategy designed for comfortable near vision to reduce eye strain and accommodation stress. This demand may be stronger in women than men due to habitual vision and not due to accommodation amplitude or arm length since near add power at the same distance is similar between men and women, and previous investigations indicated arm length was not associated with actual working distance15,16 despite the mean arm length of Japanese women being 6 cm shorter than men.19 In Japan, a higher proportion of men (54.0%) hold a driving license compared with women (46.0%; P < 0.01),20 suggesting demand for far vision may be stronger in men than women. Accordingly, sex differences may develop according to visual habits. Women at ages 40 to 59 years experience menopause and they suffer many ocular symptoms.21 Additionally, regression analysis indicated Δ lens power of women was associated with more ocular parameters than men, suggesting women’s near vision may be more susceptible to ocular conditions than men’s. Ocular surface results were worse in women compared with men which could exacerbate near add power in women.
The strength of this study was the wide age distribution of the recruited participants, ranging from 20 to 79 years, allowing the exploration of age-specific differences between men and women. In addition, the number of participants was much larger than prior studies. The current results may be helpful in daily practice showing that women prefer less myopic correction power for daily use contact lenses particularly at the age of 40 to 59 years.21 These results are informative for ocular health care personnel showing them that women aged 40 to 59 may suffer from focusing difficulty more seriously than men and prefer under correction. Additionally, dry eye care should also be considered for these women. The present study has several limitations. Objective measurements of accommodation, lifestyle, and working distance should have been evaluated to determine the daily demand for habitual vision. Consecutive individuals visiting the eye clinic were recruited, and there was a difference in the detection power between women and men due to the number of participants and the results may be biased, however enough men participated for statistical analysis. A more broad-based study including the perspectives and awareness of presbyopia in the population may be warranted to confirm the current results.
Conclusion
The current results reveal sex differences in the preferred power of contact lenses to achieve comfortable habitual visual acuity. The magnitude of under-correction was significantly greater in women than men aged 40 to 59 years. This difference may be due to preference and women’s habitual visual work rather than arm length, refractive, or accommodation status. Additionally, a larger number of women with severe dry eye may also contribute to this difference. These results show that vision care specialists should pay attention to sex differences when managing presbyopic individuals.
Acknowledgments
We appreciate the professional assistance of Miyuki Kubota, Shunsuke Kubota, Sachiko Masui, and Eriko Toda.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Negishi K, Ayaki M, Kawashima M, Tsubota K. Sleep and subjective happiness between the ages 40 and 59 in relation to presbyopia and dry eye. PLoS One. 2021;16(4):e0250087. doi:10.1371/journal.pone.0250087
2. Kaufman PL, Lütjen Drecoll E, Croft MA. Presbyopia and glaucoma: two diseases, one pathophysiology? The 2017 Friedenwald lecture. Invest Ophthalmol Vis Sci. 2019;60(5):1801–7. doi:10.1167/iovs.19-26899
3. Hipsley AM. Dynamic range of focus of the eye: understanding biomechanics and kinematics: Part I. Presbyopia Physician. 2023;3:25–28.
4. Schnider C, Yuen L, Rampat R, et al. BCLA CLEAR presbyopia: management with intraocular lenses. Cont Lens Anterior Eye. 2024;47(4):102253. doi:10.1016/j.clae.2024.102253
5. Markoulli M, Fricke TR, Arvind A, et al. BCLA CLEAR presbyopia: epidemiology and impact. Cont Lens Anterior Eye. 2024;47(4):102157. doi:10.1016/j.clae.2024.102157
6. Ide T, Negishi K, Yamaguchi T, Hara S, Toda I, Tsubota K. New compact accommodometer to measure accommodation amplitude as a biomarker. Asia Pac J Ophthalmol. 2012;1(1):24–27. doi:10.1097/APO.0b013e31823f1a69
7. Srinivasan R, Paramasivan G, Sharma A, Surya J, Sharma T, Raman R. Prevalence, risk factors and association with glycemic levels of presbyopia in South Indian population. Indian J Ophthalmol. 2021;69(11):3173–3177. doi:10.4103/ijo.IJO_1407_21
8. Hickenbotham A, Roorda A, Steinmaus C, Glasser A. Meta-analysis of sex differences in presbyopia. Invest Ophthalmol Vis Sci. 2012;53(6):3215–3220. doi:10.1167/iovs.12-9791
9. Ayaki M, Negishi K. Short tear break-up time could exacerbate the progression of presbyopia in women. Biomed Res Int. 2022;2022(1):8159669. doi:10.1155/2022/8159669
10. Ayaki M, Tsuneyoshi Y, Yuki K, Tsubota K, Negishi K. Latanoprost could exacerbate the progression of presbyopia. PLoS One. 2019;14(1):e0211631. doi:10.1371/journal.pone.0211631
11. Ayaki M, Ichikawa K. Near add power of glaucoma patients with early presbyopia. J Clin Med. 2024;13(19):5675. doi:10.3390/jcm13195675
12. Ayaki M, Hanyuda A, Negishi K. Presbyopia progression from the age of 40 to 79 years in glaucoma patients treated with prostaglandin F receptor agonists. Trans Vision Sci Technol. 2025;14(5):25. doi:10.1167/tvst.14.5.25
13. Sato H. Hunting of the Boyela, slash-and-burn agriculturalists, in the central Zaire Forest. Afr Study Monograp. 1983;4:1–54.
14. Ribeiro F, Ferreira TB, Silva D, Matos AC, Gaspar S, Piñero DP. Analysis of daily visual habits in a presbyopic population. J Ophthalmol. 2023;2023(1):6440954. doi:10.1155/2023/6440954
15. Soler F, Sánchez-García A, Molina-Martin A, de Fez D, Díaz V, Piñero DP. Differences in visual working and mobile phone usage distance according to the job profile. Curr Eye Res. 2021;46(8):1240–1246. doi:10.1080/02713683.2020.1867751
16. Leffler CT, Davenport B, Rentz J, Miller A, Benson W. Clinical predictors of the optimal spectacle correction for comfort performing desktop tasks. Clin Exp Optom. 2008;91(6):530–537. doi:10.1111/j.1444-0938.2008.00288.x
17. Ayaki M, Hanyuda A, Negishi K. Increased near add power in pre-presbyopic glaucoma patients treated with medication. Clin Exp Optom. 2025;12:1–6. doi:10.1080/08164622.2025.2564693
18. Kragha IK, Hofstetter HW. Bifocal adds and environmental temperature. Am J Optom Physiol Opt. 1986;63(5):372–376. doi:10.1097/00006324-198605000-00009
19. Japanese arm length. Average-arm-length. Available from: https://qitano.com.
20. Cabinet Office Japan, Driving license. Available from: https://www8.cao.go.jp/koutu/taisaku/r06kou_haku/zenbun/genkyo/h1/h1b1s2_3.html#:~:text.
21. Ayaki M, Hanyuda A, Negishi K. Presbyopia, dry eye, and retinal thickness in the middle-aged population: focusing on sex differences. Clin Optom. 2024;16:223–231. doi:10.2147/OPTO.S481279
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Presbyopia, Dry Eye, and Retinal Thickness in the Middle-Aged Population: Focusing on Sex Differences
Ayaki M, Hanyuda A, Negishi K
Clinical Optometry 2024, 16:223-231
Published Date: 2 September 2024
Comparison of Presbyopia Between Glaucoma Patients Using Prostaglandin F Receptor Agonists and Fixed Combination Therapy
Ayaki M, Hanyuda A, Negishi K
Clinical Optometry 2025, 17:163-171
Published Date: 27 June 2025
Drinking Habit Could Exacerbate the Progression of Presbyopia in Men
Ayaki M, Hanyuda A, Negishi K
Clinical Optometry 2026, 18:603879
Published Date: 12 May 2026