Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 13
Severity of Acne Vulgaris: Comparison of Two Assessment Methods
Authors Alsulaimani H ![]() , Kokandi A
, Kokandi A ![]() , Khawandanh S
, Khawandanh S ![]() , Hamad R
, Hamad R
Received 10 June 2020
Accepted for publication 8 September 2020
Published 28 September 2020 Volume 2020:13 Pages 711—716
DOI https://doi.org/10.2147/CCID.S266320
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Hadeel Alsulaimani,1 Amal Kokandi,2 Shahad Khawandanh,1 Rahf Hamad1
1Faculty of Medicine, King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia; 2Department of Dermatology, Faculty of Medicine, King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia
Correspondence: Hadeel Alsulaimani Tel +966503296353
Fax +966126952437
Email [email protected]
Purpose: Numerous tools are available to assess acne severity. It is important to have an acceptable and easy to use tool for acne assessment for many reasons, such as initial assessment and follow-ups, clinical trials, and comparisons of clinical studies. The aim was to investigate the agreement between different observers (inter-observer variation) in the evaluation using the Global Acne Grading System (GAGS) and Investigator Global Assessment of Acne (IGA). Besides, to investigate the correlation between the assessment scores and its relation to the quality of life scales Dermatology Life Quality Index (DLQI) and the Cardiff Acne Disability Index (CADI).
Patients and Methods: This was a prospective study. Four investigators involved to evaluate the study subject surveyed 54 patients complaining of acne using IGA and GAGS scores (DLQI and CADI).
Results: A significant relation was seen between GAGS and IGA (Pearson chi-square test p= 0.001), and they demonstrated excellent inter-rater reliability. There was no correlation between IGA and quality of life measures (CADI nor DLQI). However, there was a significant weak correlation between GAGS and CADI.
Conclusion: The two methods for acne severity assessment are reliable, and they are correlated. Quality of life concerning acne is not correlated with the severity of the disease.
Keywords: acne, severity, assessment
Introduction
Acne vulgaris is a common skin disorder affecting societies worldwide.1 The estimated prevalence of acne between the age of 12 to 24 is 85%.2 In some studies, it reaches up to 100% comedonal acne in both sexes during adolescence. It accounts for 73.3% in the population older than 20.3,4 Furthermore, The prevalence of acne in our area of study among medical students in Jeddah Saudi Arabia, King Abdulaziz University, is 58.8%.5 Acne is a chronic inflammatory process that presents with tow types of lesions clinically;non-inflammatory (closed and open) and inflammatory lesions (papules, nodules pustules, besides, post-inflammatory pigmentary changes.6 In severe acne, nodules, and cysts can cause scarring and psychological effect.7 It usually affects the face, shoulders, and upper trunk.8 It can lead to substantial psychological distress, including low self-esteem, depression, and anxiety.9,10 Despite being a common disease treated by a physician, there is no ideal Objective assessment method.11,12 Numerous methods have been used, some of these methods depend on photographs representing different grades of severity; some of them depends on the text description of lesions. The later assumes overall assessment or regional assessment with an equation to calculate a severity grade. Currently, no universal acne grading system is recommended.13 Few of these tools have gained popularity. It is essential to have an acceptable and easy to use tool for acne assessment for many reasons; initial evaluations and follow-ups, medications, clinical trials, and comparisons of clinical studies.14 However, One of these tools is the Investigator Global Assessment of acne (IGA), which is accepted by the American Food and Drug Administration (FDA) in 2018, recommended the addition of lesion count as it is a global assessment as the name implies.15 The other method is the global acne grading system (GAGS) that gives a weight to each region (face and back) with a severity score.16 The aim of this study is to investigate the agreement between different observers (intra-rater variation) in the assessment of the severity of acne using GAGS and IGA and the correlation between the two-scoring system. Additional, to evaluate its relation to the quality of life scales Cardiff Acne Disability Index (CADI) and Dermatology Life Quality Index (DLQI)
Patients and Methods
Study Subjects
This was a prospective cross-sectional study conducted among patients suffering from acne, attending the dermatology outpatient clinics at King Abdulaziz University Hospital (KAUH), Jeddah, Saudi Arabia. Also, faculty students suffering from acne invited by invitation messages distributed through social media to participate in the study. The study took place during the period between March 2019- February 2020, as each 5–6 participant attends the clinic one day per week. Demographic data (age and gender) and clinical data (history of any chronic diseases, any medications (systemic or topical), history, and current cleansing products) were collected approval obtained from the unit of biomedical ethics in KAUH. Willing patients and students signed a consent form.
Acne Severity Assessment
For the evaluation of acne severity, four investigators were engaged, one of them was a dermatologist, and the other three were a medical student that receive multiple training sessions for 1-hour in terms of interpretation of both scores and understanding types of acne before starting evaluation settings.
Participants were examined in the outpatient clinics KAUH. The examination sessions are 7–8 clinic visits included 5–6 patients each appointment for a one-hour evaluation each patient individually.
Briefly; GAGS consider six locations of the face and chest/upper back with a factor for each location based on surface area (forehead = 2, Right cheek = 2, Left Cheek =2, Nose = 1, Chin = 1, Chest and Upper back = 3), distribution and density of pilosebaceous units. Each region would be given a score depending on the type of lesions (No lesion =0, One comedone = 1, Papule=2, One pustule = 3, One nodule = 4) and the sum of scores multiplied by the factors (Local score = Factor × Grade from 0 to 4), the sum of local scores gives the global score (0–52). The severity is graded as mild if the score was 1–18, moderate with scores form 19–30, severe with scores form 31–38, and as very severe if the score is more than 38 following the author’s recommendation.16
IGA score graded from 0–4 depending on the descriptive criteria of facial acne only. No account on the chest, back, or shoulders considered here. In addition to lesion count of inflammatory and non-inflammatory ones, are reported.15
Quality of Life Assessment
Study subjects completed the Arabic version of both the Cardiff Acne Disability Index (CADI).17 And the Dermatology Life Quality Index (DLQI).18
CADI is a tool to assess the effect of acne on quality of life with a possible maximum score of 15 and a minimum of 0. (grade of impairment; 0 no impairment, 1–5 mild impairment, 6–10 moderate impairment, and 11–15 severe impairment). The higher the score, the more the quality of life is impaired.
DLQI a ten items questionnaire that assesses the effect of skin disease in general on quality of life. The total score ranges from 0 (no impact of skin disease in quality of life) to 30 (maximum implications for quality of life). The grades are 0–1 no effect at all on patient’s life, 2–5 small effect, 6–10 moderate, 11–20 very large, 21–30 extremely large impact on patient’s life.
Statistical Analysis
The data were reviewed, coded, and analyzed using Microsoft Excel and Statistical Package for the Social Sciences (SPSS) version 18.0. Continuous variables were tested for normality using the Shapiro–Wilk test. Mann–Whitney U-test was used to investigate whether the two scores GAGS and IGA were having the same distribution. Categorical variables presented as frequency and percentage. Significant differences between the two scores (GAGS and IGA) was assessed by Pearson Chi-square (t-test) using the average of the four investigators. Spearman correlation test used to determine the correlation between IGA and GAGS scores was obtained from the evaluation of the four investigators. The reliability (internal consistency) of both GAGS and IGA were evaluated by (Alpha Cronbach). The correlation between two acne severity scoring systems (GAGS and IGA) and quality of life measures (CADI and DLQI) were assessed using two-tailed Spearman’s roh and scatter plot.
Results
A total of Fifty-four participants suffering from acne were evaluated. Most of them were females (44, 81.5%) and (10, 18.5%) were males. Forty-nine (90.7%) of the participants were between the ages of 18–24 years, and 5 (9.3%) were between 25–30 years.
GAGS and IGA
For the IGA scoring system, most of the participants 34 (63%) were mild in severity, as shown in Table 1.
 |
Table 1 Frequency of GAGS and IGA |
The mean score of GAGS was (16.19±5.09) by using the values of the four evaluators.
There was evidence of adequate Internal consistency that found for GAGS was (Cronbach’s Alpha 0.947) as well as IGA (Cronbach’s Alpha 0.871).
Most of the four investigators score patients as mild to almost clear in both IGA and GAGS scoring systems as compared in Figure 1.
 |
Figure 1 Comparison between the four investigators in GAGS and IGA frequencies. |
For the intra-rater reliability both GAGS [ICC 0.946, 95% confidence interval (CI) 0.918–0.966; p>0.0001] and IGA [ICC 0.873, 95% confidence interval (CI) [0.807–0.920; p>0.0001]] demonstrated excellent reliability.
There was a significant relation between GAGS and IGA (Pearson Chi-square test p= 0.0001). A significant correlation assessed by a Spearman Correlation Test comparing both scores for each investigator apart, as shown in Figure 2.
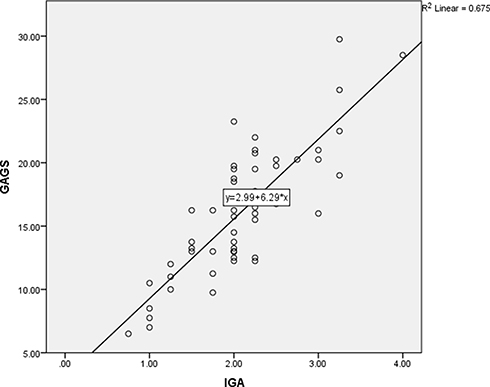 |
Figure 2 Correlation between the severity scores (GAGS and IGA). |
CADI and DLQI
The mean score for CADI was (4.52 ± 2.919), and DLQI was (3.78 ± 4.17). For the DLQI, the majority of study population acne has either no effect (19, 35.2%) or only a small effect (22, 40.7%) on patient life. Similarly, the majority of study population acne caused mild impairment of quality of life (34, 63%) or moderate impairment (14, 25.9%), as shown in Table 2.
 |
Table 2 Frequencies of DLQI and CADI |
There was no correlation between IGA and CADI nor DLQI at the level of p=0.01. Additionally, there was no correlation between GAGS and DLQI. Although there was a significant correlation between GAGS and CADI, it was a weak one [Table 3 and Figure 3]. DLQI and CADI were significantly correlated (r=0.649, p<0.0001).
 |
Table 3 Correlations Between Severity Scores Assessed by an Experienced Physician and Quality of Life Measures |
 |
Figure 3 Correlation between severity scores and quality of life scores. (A) correlation between IGA and CADI. (B) Correlation between IGA and DLQI. (C) correlation between GAGS and CADI. (D) correlation between GAGS and DLQI. |
Discussion
There are many tools to assess acne severity, but none of them considered as a universally accepted one.19,20 Furthermore, they are not interchangeable as they do not measure the same components of the disease. Measuring disease severity is essential for clinical practice in terms of evaluation and follow-ups, and in comparing studies in the literature. Measures are usually subjective ones. One of the commonly used methods is lesion counting, which is time-consuming but might represent a more accurate method. Other methods use grading systems.11 A multi-rater validation study found that acne lesion counting has excellent reliability if done by the trained rater, and reliability can be higher by raters training and using of standard template.21
Global Acne Grading System (GAGS) was first originated by Doshi et al One of the most detailed acne grading systems comparing with others, with keeping simplicity.16 On the other hand, IGA is a global assessment method recommended by the FDA.
This study shows an excellent agreement between investigators of severity using GAGS in terms of intra-rater reliability. Both methods do not take into account the scaring or post-inflammatory pigmentation aspects of the disease. They only measure the active lesions (comedones and inflammatory lesions). To our knowledge, no study has compared these two methods previously. Each method has its application. IGA is a rapid assessment method, but the changes in the values or grades are limited, which might limit the meaning of the changes reported with treatments. GAGS has a broader scale and more detailed description of the disease, but more elaborate and time-consuming. GAGS seems to be more appropriate for research purposes.
Recently the use of validated DLQI and CADI have been utilized frequently, and forms in many languages are existing.22 In this study, there was no correlation between IGA and CADI nor DLQI at the level of p=0.01 level. Additionally, there was no correlation between GAGS and DLQI. Although there was a significant correlation between GAGS and CADI, it was a weak one. This is in agreement with many previous studies.7,23,24 In contrast, a significant positive correlation between total GAGS score and both CADI and DLQI reported in a study from turkey.25 CADI is more appropriate and easier to be used rather than DLQI due to the greater number of items in DLQI and its specificity to the disease in this case.
Conclusion
In Conclusion, the two methods for acne severity assessment (GAGS and IGA) are reliable, and they are correlated. Quality of life concerning acne is not correlated with the severity of the disease.
Abbreviations
KAUH, King Abdulaziz University Hospital; GAGS, Global Acne Grading System; IGA, Investigator Global Assessment; DLQI, Dermatology Life Quality Index; CADI, Cardiff Acne Disability Index; FDA, Food and Drug Administration; SPSS, Statistical Package for the Social Sciences; ICC, internal consistency; CI, confidence interval.
Data Sharing Statement
All data is presented in the results section, and if any more is required, the author can provide them.
Ethics Approval and Informed Consent
The study was conducted in accordance with Declaration of Helsinki for human volunteers. The study protocol was approved by the ethics committee in the institution, the study process was explained to each participant, they were free to refuse or agree to participate in the study and they signed informed consent form.
Consent for Publication
Informed consent was obtained for publishing.
Acknowledgments
We would like to thank Mohammed Safhi for the valuable statistical review that was needed for accomplishment.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was not sponsored by anyone and received no funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. O’Neill AM, Gallo RL. Host-microbiome interactions and recent progress into understanding the biology of acne vulgaris. Microbiome. 2018;6(1):177. doi:10.1186/s40168-018-0558-5
2. Asai Y, Baibergenova A, Dutil M, et al. Management of acne: canadian clinical practice guideline. Can Med Assoc J. 2016;188(2):118–126.
3. Stathakis V, Kilkenny M, Marks R. Descriptive epidemiology of acne vulgaris in the community. Australas J Dermatol. 1997;38(3):115–123. doi:10.1111/j.1440-0960.1997.tb01126.x
4. Collier CN, Harper JC, Cafardi JA, et al. The prevalence of acne in adults 20 years and older. J Am Acad Dermatol. 2008;58(1):56–59. doi:10.1016/j.jaad.2007.06.045
5. Ibrahim N, Nagadi S, Idrees H, Alghanemi L, Essa R, Gari W. Acne vulgaris: prevalence, predictors, and factors influencing quality of life of female medical students at King Abdulaziz University, Jeddah. J Dermatol Dermatol Surg. 2019;23:1. doi:10.4103/jdds.jdds_39_18
6. Rocha MA, Costa CS, Bagatin E. Acne vulgaris: an inflammatory disease even before the onset of clinical lesions. Inflamm Allergy Drug Targets. 2014;13(3):162–167. doi:10.2174/1871528113666140606110024
7. Purdy S, de Berker D. Acne vulgaris. BMJ Clin Evid. 2011;2011:1714.
8. Lehmann HP, Robinson KA, Andrews JS, Holloway V, Goodman SN. Acne therapy: a methodologic review. J Am Acad Dermatol. 2002;47(2):231–240. doi:10.1067/mjd.2002.120912
9. Dalgard F, Gieler U, Holm JO, Bjertness E, Hauser S. Self-esteem and body satisfaction among late adolescents with acne: results from a population survey. J Am Acad Dermatol. 2008;59(5):746–751. doi:10.1016/j.jaad.2008.07.013
10. Yazici K, Baz K, Yazici AE, et al. Disease-specific quality of life is associated with anxiety and depression in patients with acne. J Eur Acad Dermatol Venereol. 2004;18(4):435–439. doi:10.1111/j.1468-3083.2004.00946.x
11. Adityan B, Kumari R, Thappa DM. Scoring systems in acne vulgaris. Indian J Dermatol Venereol Leprol. 2009;75(3):323–326. doi:10.4103/0378-6323.51258
12. Tan JKL, Jones E, Allen E, Pripotnev S, Raza A, Wolfe B. Evaluation of essential clinical components and features of current acne global grading scales. J Am Acad Dermatol. 2013;69(5):754–761.
13. Zaenglein AL, Pathy AL, Schlosser BJ, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2016;74(5):945–973 e933. doi:10.1016/j.jaad.2015.12.037
14. Hayashi N, Akamatsu H, Kawashima M, Acne Study G. Establishment of grading criteria for acne severity. J Dermatol. 2008;35(5):255–260.
15. Guidance for industry acne vulgaris: developing drugs for treatment. Available from: www.fda.gov/downloads/Drugs/Guidances/UCM071292.pdf.
16. Doshi A, Zaheer A, Stiller MJ. A comparison of current acne grading systems and proposal of a novel system. Int J Dermatol. 1997;36(6):416–418.
17. Motley RJ, Finlay AY. Practical use of a disability index in the routine management of acne. Clin Exp Dermatol. 1992;17(1):1–3. doi:10.1111/j.1365-2230.1992.tb02521.x
18. Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI)–a simple practical measure for routine clinical use. Clin Exp Dermatol. 1994;19(3):210–216. doi:10.1111/j.1365-2230.1994.tb01167.x
19. Zarchi K, Jemec GBE, Assessment S. Outcome measures in acne vulgaris. Curr Dermatol Rep. 2012;1(3):131–136. doi:10.1007/s13671-012-0016-8
20. Agnew T, Furber G, Leach M, Segal L. A comprehensive critique and review of published measures of acne severity. J Clin Aesthetic Dermatol. 2016;9(7):40–52.
21. Lucky AW, Williams J, Ratterman J, Barber BL, Girman CJ, Waldstreicher J. A multirater validation study to assess the reliability of acne lesion counting. J Am Acad Dermatol. 1996;35(4):559–565.
22. Swathylekshmy JLJSDSDJ. Impact of acne vulgaris on the quality of life. J Evol Med Dent Sci. 2017;6(35):2865–2868. doi:10.14260/Jemds/2017/618
23. Kokandi A. Evaluation of acne quality of life and clinical severity in acne female adults. Dermatol Res Pract. 2010;2010:1–3. doi:10.1155/2010/410809
24. Law MPM, Chuh AAT, Lee A, Molinari N. Acne prevalence and beyond: acne disability and its predictive factors among Chinese late adolescents in Hong Kong. Clin Exp Dermatol. 2010;35(1):16–21. doi:10.1111/j.1365-2230.2009.03340.x
25. Aslı T, Berna A, Ayşe Serap K. Which quality of life scale should be used to evaluate acne vulgaris patients? CADI or DLQI? A prospective study. Arch Clin Exp Med. 2019;2:90.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.