Back to Journals » International Medical Case Reports Journal » Volume 14
Severe Pulmonary Mycobacterium abscessus Cases Due to Co-Infection with Other Microorganisms Well Treated by Clarithromycin and Sitafloxacin in Japan
Authors Takano K, Shimada D ![]() , Kashiwagura S, Kamioka Y, Hariu M, Watanabe Y
, Kashiwagura S, Kamioka Y, Hariu M, Watanabe Y ![]() , Seki M
, Seki M ![]()
Received 26 May 2021
Accepted for publication 4 July 2021
Published 12 July 2021 Volume 2021:14 Pages 465—470
DOI https://doi.org/10.2147/IMCRJ.S321969
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ronald Prineas
Kazuki Takano,1,2 Daishi Shimada,1 Shota Kashiwagura,1,3 Yasuhiro Kamioka,1,3 Maya Hariu,1,2 Yuji Watanabe,1,2 Masafumi Seki1
1Division of Infectious Diseases and Infection Control, Faculty of Medicine; 2Laboratory for Clinical Microbiology; 3Division of Pharmacy, Tohoku Medical and Pharmaceutical University Hospital, Sendai City, Miyagi, Japan
Correspondence: Masafumi Seki
Division of Infectious Diseases and Infection Control, Faculty of Medicine, Tohoku Medical and Pharmaceutical University, 1-15-1 Fukumuro, Miyagino-ku, Sendai City, Miyagi, 983-8612, Japan
Tel +81-22-259-1221
Fax +81-22-290-8956
Email [email protected]
Background: Mycobacterium abscessus frequently causes severe infections, yet its pathophysiological features and treatment regimens have not been established.
Case Report: We present five cases of severe pneumonia due to Mycobacterium abscessus infection in Japan. All cases were diabetic patients, with possible acceleration to pneumonia due to co-infection with other microorganisms. However, following a short period of hospitalization and combination therapy with intravenous imipenem/cilastatin and amikacin, all the cases were successfully treated as outpatients with oral clarithromycin and sitafloxacin.
Conclusion: M. abscessus infections can become severe in the presence of diabetes mellitus and co-infection with other chronic infectious organisms. Sitafloxacin might be a key drug in the treatment of M. abscessus infection in future.
Keywords: non-tuberculosis mycobacterium, macrolides, clarithromycin, fluoroquinolone, sitafloxacin
Background
Globally, infections caused by non-tuberculous mycobacteria (NTM) are increasing and are notoriously difficult to treat due to intrinsic resistance of these bacteria to many common antibiotics.1 Although NTM are ubiquitous and diverse in the environment, only a few species, including Mycobacterium abscessus, cause serious and often opportunistic infections in humans.2 This rapidly growing mycobacterium is one of the most commonly identified NTM species responsible for severe respiratory, skin and mucosal infections in humans, and is frequently found in immunocompromised patients with underlying diseases and complicated co-infections.3,4
Although M. abscessus is usually treated with a combination of antibiotics, including macrolides, carbapenems and aminoglycosides, it is often regarded as one of the most antibiotic-resistant mycobacteria, with few therapeutic options.5 Recently, some quinolones, including levofloxacin (LVFX), have demonstrated antimycobacterial activities and degrees of chemotherapeutic efficacy against certain types of mycobacterial infections, and are used as an alternative to and/or as combination agents with antimycobacterial agents, such as isoniazid, rifampicin and ethambutol, although the NTM are sometimes resistant.6,7
Here, we report five cases of definite M. abscessus-associated pneumonia that were treated and maintained with clarithromycin (CAM) and sitafloxacin (SFTX), a novel respiratory quinolone, with all the isolated M. abscessus showing susceptibility to this therapy. These cases might have been exacerbated by co-infection with other microorganisms, such as Pseudomonas aeruginosa, Aspergillus fumigatus, Staphylococcus aureus and Mycobacterium avium complex (MAC). All our patients had diabetes mellitus (DM), which might have led to their immunocompromised status.
This study was approved by the Committee for Clinical Scientific Research of Tohoku Medical and Pharmaceutical University Hospital on Oct 09, 2015 (approval no. ID2015-2-028) and the patients whose specimens were used provided written informed consent to have their case details and any accompanying images published.
Case Report
Case 1
A 51-year-old diabetic (HbA1c: 7.1%, National Glycohemoglobin Standardization Program (NGSP)) male patient developed severe M. abscessus pneumonia, although he had been treated with clarithromycin (CAM) 800 mg/day, minocycline (MINO) 100 mg/day and levofloxacin (LVFX) 500 mg /day orally for three years before the bacterium was isolated (Figure 1A). His initial white blood cell (WBC) count was 11,700/L, C-reactive protein (CRP) was 18.5 mg/dL, and HbA1c was 7.8 (NGSP). P. aeruginosa was also isolated from his sputum.
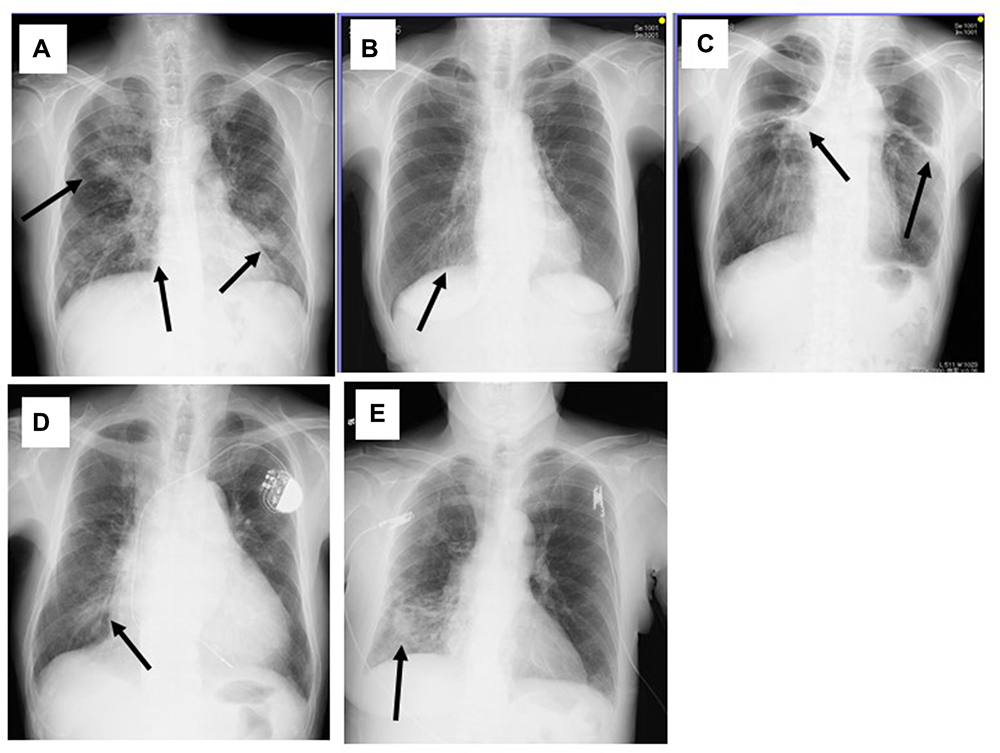 |
Figure 1 Chest X-ray findings in the five patients. Shadows suggestive of infiltration and/or bronchiectasis were observed (arrows). |
After admission, he received CAM 800 mg/day, intravenous imipenem/cilastatin (IPM/CS) 3 g/day and amikacin (AMK) 10 mg/kg/day, with improvement in his chest radiograph findings and inflammatory markers, such as WBC count (5400/L) and CRP level (0.86 mg/dL). His clinical parameters, such as inflammation, chest X-ray, and nutritional status have since been well controlled with outpatient administration of CAM 800 mg/day and SFTX 100 mg/day for a year, and M. abscessus has not been further isolated. Liver dysfunction and diarrhea, as side effects of SFTX, have also not occurred.
Case 2
A 78- year-old diabetic female (HbA1c: 6.6%, NGSP) was admitted due to exacerbation of Mycobacterium pulmonary infection (Figure 1B). She weighed less than 40 kg and was initially suspected to have MAC infection, although M. abscessus was isolated by bronchoscopic analysis after three weeks. S. aureus was also isolated from her sputum although she had been receiving erythromycin (EM) 200 mg/day as an immune-modulatory agent, along with the anti-diabetic agent, sitagliptin phosphate hydrate 50 mg/day. Subsequently, relatively low doses of CAM 600 mg/day and SFTX 50 mg/day were started as outpatient treatment, with no further recurrences of pneumonia or M. abscessus isolation from sputum. Liver dysfunction and severe diarrhea did not occur and her weight increased above 40 kg.
Case 3
A 63-year-old male with heart failure and DM (HbA1c: 6.1%, under observation without anti-diabetics), who had been receiving voriconazole 300 mg/day orally for chronic pulmonary aspergillosis, was admitted for follow-up because of exacerbation of pulmonary symptoms. He received oral LVFX 500 mg/day as outpatient therapy for pneumonia, but with no improvement. His chest x-ray worsened and M. abscessus was isolated from his sputum, although A. fumigatus was not isolated (Figure 1C). Combination therapy with CAM 800 mg/day, IPM/CS 3 g/day and AMK 10 mg/kg/day were started after admission, with significant improvement in his condition. He was effectively treated and has been maintained with CAM 800 mg/day and SFTX 100 mg/day, respectively for 6 months, with no liver dysfunction or diarrhea, and no further isolation of M. abscessus after SFTX commencement.
Case 4
A 54-year-old male patient with chronic heart failure with pacemaker implantation and DM was admitted because of suspected pneumonia (Figure 1D). His initial WBC count was 6400/L, C-reactive protein (CRP) was 6.8 mg/dL, and HbA1c was 6.4% (NGSP) on sitagliptin phosphate hydrate 50 mg/day. He received LVFX 500 mg/day intravenously, with no improvement. Subsequently, M. abscessus and P. aeruginosa were isolated from his sputum twice.
We changed the antibiotic regimen to CAM 800 mg/day, intravenous IPM/CS 3 g/day and AMK 10 mg/kg/day, which resulted in improvement in his chest radiograph findings and inflammatory markers: WBC (3400/L) and CRP (1.02 mg/dL). His condition has since been well controlled with CAM 800 mg/day and SFTX 100 mg/day as outpatient treatment. Although M. abscessus was subsequently isolated, recurrent pneumonia and side effects were not observed.
Case 5
A 74-year-old female patient under treatment for DM (HbA1c: 5.8%, NGSP) that was well controlled with sitagliptin phosphate hydrate 50 mg/day was admitted for sudden hemosputum, and underwent emergency bronchial artery embolization. Her chest X-ray showed infiltrative shadows with cavity formation (Figure 1E), and M. abscessus was isolated from her sputum. Her serum was strongly positive for MAC antibodies (6.8 U/mL), although MAC was not isolated from sputum. We started CAM 600 mg/day and SFTX 50 mg/day therapy, and her condition has been stable since then and hemosputum has not recurred, and with no further M. abscessus isolation. Her liver and gastrointestinal functions remained stable.
The M. abscessus isolated from all five patients had relatively high susceptibility/low minimum inhibitory concentration (MIC) to CAM, but lower susceptibility/higher MIC to IPM/CS and AMK in vitro, although all these agents were clinically effective (Table 1). For drug susceptibility analysis, the broth microdilution method was performed according to Clinical and Laboratory Standards Institute (CLSI) guidelines, using a 96-well round bottom microtiter plates kit (Kyokuto Co. Ltd. Tokyo, Japan). Briefly, the prepared MIC plates were incubated aerobically at 30°C. MICs were measured on day 3 or 4 and compared with control wells without antibiotics, showing sufficient bacterial growth.8 MIC was defined as the lowest drug concentration at which bacterial growth was not visualized. The isolated organisms were resistant to most of the other antibiotics, including levofloxacin and moxifloxacin. Clofazimine and SFTX were found to be effective against the isolated M. abscessus strains in all five cases.
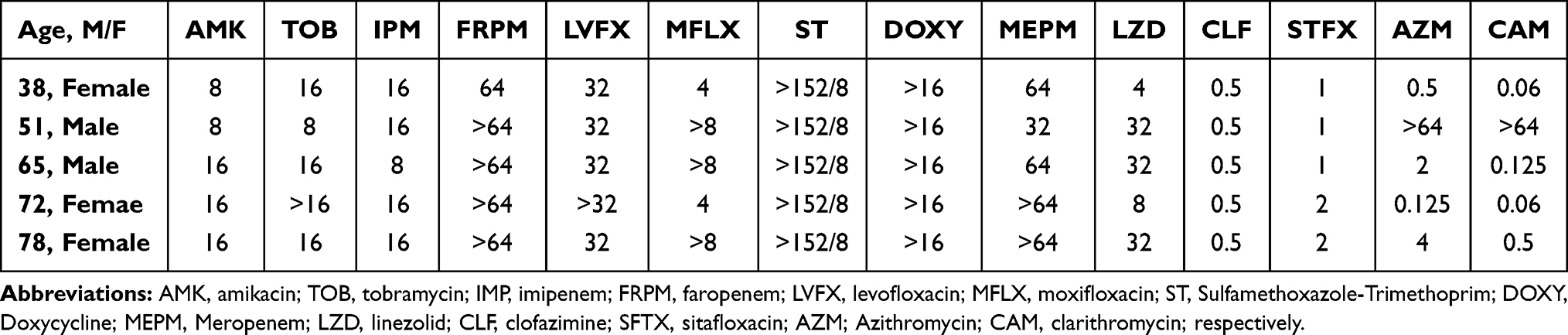 |
Table 1 Minimum Inhibitory Concentration (MIC) of Various Antibiotics for the Mycobacterium abscessus Isolated from the Five Patients |
Discussion
M. abscessus is the most important rapidly growing mycobacterium species; approximately 80% of chronic pulmonary diseases are caused by these rapid growth type mycobacteria, with the infections frequently becoming severe.2,5,9
Among our presented cases, almost all the cases were not controlled by oral antibiotics, including LVFX administered as outpatient treatment, and the patients required admission for intravenous administration of IPM/CS and AMK along with oral CAM. All five patients had DM as the underlying disease and co-infections with microorganisms in addition to M. abscessus infection. Our experience suggests that DM and/or co-infections might be the most important factors contributing to exacerbation of M. abscessus infection.
Immunocompromised patients, including those with HIV infection and some autoimmune diseases with steroid use, are known to develop severe mycobacterium infection, with disseminated infection in some cases. A 57-year-old Japanese male with Good’s syndrome and myasthenia gravis, who was treated with prednisolone and tacrolimus, was reported to have disseminated NTM infection caused by M. abscessus subsp. massiliense.10 He also had type 2 DM, and the correlation between an immunosuppressed status, including DM, and severe M. abscessus infection as an opportunistic infection was suggested. It was previously reported that non-classical monocytes from obesity-based DM and non-obese tuberculosis patients exhibit similar activation profiles (CD86/CD206/TLR-2 and TLR-4 expressions), and serum adiponectin levels increased similarly in tuberculosis and obesity-based DM patients.11 The authors found that monocytes from active tuberculosis patients and obesity-based DM were more permissive to mycobacterium growth, including M. abscessus, than in obese individuals without DM, suggesting that a background of DM might be unfavorable in terms of controlling the mycobacterium infection.
In contrast, it was reported that DM was not a risk factor for M. abscessus infection among cystic fibrosis (CF) patients, although a history of Stenotrophomonas maltophilia, one of the representative chronic infectious bacteria, was significantly more frequent among cases than among controls, and that there might be a correlation with A. fumigatus, an organism commonly found in CF patients with NTM infection, or that both might be signs of advanced lung damage that predisposes to mycobacterial disease.12 A. fumigatus was reported to worsen pulmonary inflammation and impact M. abscessus control in a mouse model.13 Furthermore, M. abscessus with P. aeruginosa and MAC were also suggested as risk factors for M. abscessus infection.6,14 This suggests that we should consider the co-existence of these other chronic infectious microorganisms, and treat or control them with other antibiotics, including macrolides, as immunomodulatory agents.15
CAM was one of the rare antibacterial agents used in our patients, although M. abscessus is intrinsically resistant to most antibacterial agents. Several studies have evaluated the efficiency of combined drug therapy in the treatment of M. abscessus infections according to the recommendations of guidelines, such as the treatment combining CAM, AMK, cefoxitin or IPM/CS, faropenem and linezolid (LZD).4,16,17 Although these drugs are relatively well tolerated, treatment failure was still observed in about 20 to 70% of cases.18,19 Although clofazimine is not available in Japan, use of inhaled amikacin, Arikayce (amikacin liposome inhalation suspension or ALIS), for refractory pulmonary NTM disease has recently been accepted.20 The use of Arikayce led to negative sputum cultures for NTM by month 6 in 29% of patients compared to 8.9% of patients treated with guideline-based therapy alone. The effectiveness of Arikayce thus holds promise. However, there is limited data on Arikayce’s safety in Japanese patients. Additionally, difficulty in outpatient control has been suggested because most of the recommended drugs are not oral agents, and because of the significant side-effects, including thrombocytopenia with LZD.4 Therefore, some other antimicrobial agents, including fluoroquinolones, were suggested as key agents for the long term treatment and maintenance follow up of M. abscessus infections.
Among the fluoroquinolones, SFTX is considered a favorable agent against M. abscessus because it shows high susceptibility/low MIC in contrast to the other fluoroquinolones, including LVFX.7 SFTX is a novel respiratory quinolone that is reportedly often used for patients with severe M. abscessus infection as an alternative and/or adjuvant to standard antibiotic regimens.10 SFTX generally shows 2- to 16-fold higher antimicrobial effects compared with previous new quinolones, such as LVFX and ciprofloxacin.7 In our cases, SFTX showed both microbiological susceptibility (Table 1) and clinical efficiency in all patients, suggesting its usefulness as outpatient treatment for M. abscessus infection in combination with CAM. Our cases also suggested synergistic effects between SFTX and CAM, as with d-cycloserine.8 Khosravi et al analyzed 714 positive acid fast-bacilli, and found the effect of d-cycloserine was better than that of CAM. In addition, a synergistic effect of d-cycloserine with CAM was observed against six (100%) and five (71.5%) strains of M. fortuitum and M. abscessus, respectively. Unfortunately, however, we could not analyze synergistic MIC changes in our cases, and further detailed analysis is required to assess the synergistic effects of SFTX and other antibiotics.
In conclusion, we experienced five severe M. abscessus cases, with disease exacerbation probably due to the presence of underlying DM, and co-infection with other chronic infectious organisms, including P. aeruginosa, S. aureus, A. fumigatus and MAC. The patients finally improved by administration of a combination of antibiotics, including CAM and other recommended intravenous drugs. Additionally, SFTX had good clinical and microbiological efficacy in outpatients with M. abscessus, suggesting synergistic effects between CAM and SFTX. Thus, SFTX might be a strong candidate drug in the outpatient treatment of M. abscessus infection not only in Japan, but also in other NTM endemic countries.
For Review
We present five cases of severe pneumonia due to Mycobacterium abscessus infection in Japan. All the patients were diabetic, with possible acceleration to pneumonia due to co-infection with other microorganisms. However, following a short period of hospitalization and combination therapy with intravenous imipenem/cilastatin and amikacin, all the cases were successfully treated as outpatients with oral clarithromycin and sitafloxacin, which might be a key drug for treatment of M. abscessus in future.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Johansen MD, Herrmann JL, Kremer L. Non-tuberculous mycobacteria and the rise of Mycobacterium abscessus. Nat Rev Microbiol. 2020;18:392–407. doi:10.1038/s41579-020-0331-1
2. Chen J, Zhao L, Mao Y, et al. Clinical efficacy and adverse effects of antibiotics used to treat mycobacterium abscessus pulmonary disease. Front Microbiol. 2019;10:1977. doi:10.3389/fmicb.2019.01977
3. Miyashita E, Yoshida H, Mori D, et al. Mycobacterium avium complex-associated peritonitis with CAPD after unrelated bone marrow transplantation. Pediatr Int. 2014;56:e96–e8. doi:10.1111/ped.12463
4. Seki M, Kamioka Y, Takano K, et al. Mycobacterium abscessus associated peritonitis with CAPD successfully treated using a linezolid and tedizolid containing regimen suggested immunomodulatory effects. Am J Case Rep. 2020;21. doi:10.12659/AJCR.924642.
5. Shen Y, Wang X, Jin J, et al. In vitro susceptibility of mycobacterium abscessus and mycobacterium fortuitum isolates to 30 antibiotics. Biomed Res Int. 2018;4902921. doi:10.1155/2018/4902941
6. Birmes FS, Wolf T, Kohl TA, et al. Mycobacterium abscessus subsp. abscessus is capable of degrading pseudomonas aeruginosa quinolone signals. Front Microbiol. 2017;8. doi:10.3389/fmicb.2017.00339.
7. Saito H, Tomioka H, Sato K, Dekio S. In vitro and in vivo antimycobacterial activities of a new quinolone, DU-6859a. Antimicrob Agents Chemother. 1994;38:2877–2882. doi:10.1128/AAC.38.12.2877
8. Khosravi AD, Mirsaeidi M, Farahani A, et al. Prevalence of nontuberculous mycobacteria and high efficacy of d-cycloserine and its synergistic effect with clarithromycin against mycobacterium fortuitum and mycobacterium abscessus. Infect Drug Resist. 2018;11:2521–2532. doi:10.2147/IDR.S187554
9. Bostan C, Slim E, Choremis J, et al. Successful management of severe post-LASIK Mycobacterium abscessus keratitis with topical amikacin and linezolid, flap ablation, and topical corticosteroids. J Cataract Refract Surg. 2019;45:1032–1035. doi:10.1016/j.jcrs.2019.03.001
10. Imoto W, Yamada K, Hajika Y, et al. Disseminated mycobacterium abscessus subsp. massiliense infection in a good’s syndrome patient negative for human immunodeficiency virus and anti-interferon-γ autoantibody: a case report. BMC Infect Dis. 2020;20. doi:10.1186/s12879-020-05136-x.
11. Resende DP, da Costa AC, de Souza Rosa LP, et al. Non-classical circulating monocytes in severe obesity and obesity with uncontrolled diabetes: a comparison with tuberculosis and healthy individuals. Tuberculosis (Edinb). 2019;114:30–42. doi:10.1016/j.tube.2018.11.003
12. Verregghen M, Heijerman HG, Reijers M, van Ingen J, van der Ent CK. Risk factors for mycobacterium abscessus infection in cystic fibrosis patients; a case-control study. J Cyst Fibros. 2012;11:340–343. doi:10.1016/j.jcf.2012.01.006
13. Monin L, Mehta S, Elsegeiny W, et al. Aspergillus fumigatus preexposure worsens pathology and improves control of mycobacterium abscessus pulmonary infection in mice. Infect Immun. 2018;86. doi:10.1128/IAI.00859-17.
14. Shin SH, Jhun BW, Kim SY, et al. Nontuberculous mycobacterial lung diseases caused by mixed infection with mycobacterium avium complex and mycobacterium abscessus complex. Antimicrob Agents Chemother. 2018;62. doi:10.1128/AAC.01105-18.
15. Seki M, Sakata T, Toyokawa M, Nishi I, Tomono K. A chronic respiratory pasteurella multocida infection is well-controlled by long-term macrolide therapy. Intern Med. 2016;55:307–310. doi:10.2169/internalmedicine.55.4929
16. Daley CL, Iaccarino JM, Lange C, et al. Treatment of nontuberculous mycobacterial pulmonary disease: an Official ATS/ERS/ESCMID/IDSA clinical practice guideline: executive summary. Clin Infect Dis. 2020;71:e1–e36. doi:10.1093/cid/ciaa241
17. Inoue T, Tsunoda A, Nishimoto E, et al. Successful use of linezolid for refractory Mycobacterium abcessus infection: a case report. Respir Med Case Rep. 2017;23:43–45. doi:10.1016/j.rmcr.2017.11.007
18. Jeon K, Kwon O, Lee NY, et al. Antibiotic treatment of mycobacterium abscessus lung disease: a retrospective analysis of 65 patients. Am J Respir Crit Care Med. 2009;180:896–902. doi:10.1164/rccm.200905-0704OC
19. Roux AL, Catherinot E, Soismier N, et al.; OMA group. Comparing mycobacterium massiliense and mycobacterium abscessus lung infections in cystic fibrosis patients. J Cyst Fibros. 2015;14:63–69. doi:10.1016/j.jcf.2014.07.004
20. Khan O, Chaudary N. The use of amikacin liposome inhalation suspension (Arikayce) in the treatment of refractory nontuberculous mycobacterial lung disease in adults. Drug Des Devel Ther. 2020;14:2287–2294. doi:10.2147/DDDT.S146111
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.