Back to Journals » International Medical Case Reports Journal » Volume 18
Severe Plasmodium Falciparum Malaria Mimicking Thrombotic Thrombocytopenic Purpura (TTP): A Case Report From China
Authors Wang C, Kong M, Huang M, Tang N, Mo H
Received 15 May 2025
Accepted for publication 1 August 2025
Published 13 August 2025 Volume 2025:18 Pages 1029—1034
DOI https://doi.org/10.2147/IMCRJ.S536982
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Cheng Wang,1,* Man Kong,2,* Ming Huang,3 Ning Tang,3 Hongmei Mo1
1Department of Clinical Laboratory, Shenzhen Luohu People’s Hospital, Shenzhen, People’s Republic of China; 2Department of Clinical Laboratory, Central Hospital of Wuhan, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China; 3Department of Clinical Laboratory, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hongmei Mo, Email [email protected]
Background: Plasmodium falciparum Malaria and Thrombocytopenic Purpura (TTP) are serious diseases associated with thrombotic microangiopathic anemia (TMA) pathogenesis. Therefore, clinical treatment is usually delayed because of the overlapping clinical manifestations. This case describes Plasmodium falciparus infection causing markedly elevated von Willebrand factor (vWF) levels but normal ADAMTS13 activity, which closely mimics the presentation of TTP.
Case Presentation: There is overlap in laboratory and clinical presentations, such as fever, thrombocytopenia, severe anemia, and intravascular coagulation between malaria and TTP. We present the case of a 51-year-old Chinese man who initially presented with fever that quickly progressed to a disturbance of consciousness. Laboratory tests showed a decreased platelet count, elevated lactate levels, and elevated indirect bilirubin levels. The patient’s PLASMIC score for TTP was 7, suggesting a high possibility of TTP. There was markedly elevated vWF, but normal ADAMTS13 activity. Therefore, TTP was excluded. However, we found a large amount of P. falciparus in the peripheral blood smears. The patient’s condition gradually improved after intravenous artesunate treatment.
Conclusion: Malaria and TTP have obvious laboratory and clinical resemblances, owing to the presence of TMA. It is important to quickly perform a differential laboratory diagnosis between malaria and TTP, which may lead to the early initiation of lifesaving treatment in some patients.
Keywords: plasmodium falciparum malaria, TTP, TMA, vWF
Introduction
Malaria is an infectious disease caused by parasites of the Plasmodium genus, transmitted primarily by female Anopheles mosquitoes in regions such as Africa and Southeast Asia. Although there are over 120 species within the Plasmodium genus, only five are known to cause malaria in humans.1 Among these, Plasmodium falciparum is particularly notable for its ability to cause multiple infections within individual red blood cells (RBCs) and to invade RBCs of any age. This capability facilitates rapid multiplication and increased virulence, often resulting in more severe manifestations of the disease.2 Thrombotic thrombocytopenic purpura (TTP) is a rare, life-threatening disorder characterized by microangiopathic hemolytic anemia, primarily caused by a severe deficiency in ADAMTS13, a specific protease responsible for cleaving von Willebrand factor (vWF).3 VWF is a large multimeric plasma glycoprotein that binds to exposed collagen at sites of vascular injury, subsequently activating platelets and adhering to collagen fibers to form a thrombus, thereby arresting bleeding.4,5 Plasmodium falciparum malaria presents with clinical manifestations similar to those of TTP, including microangiopathic hemolytic anemia, thrombocytopenia, fever, severe neuropsychiatric reactions, and acute kidney injury.6 Both Plasmodium falciparum malaria and TTP are severe conditions associated with the pathogenesis of thrombotic microangiopathy (TMA). Consequently, clinical treatment is often delayed due to the overlapping clinical presentations. This case report describes an infection with Plasmodium falciparum that resulted in significantly elevated vWF levels while maintaining normal ADAMTS13 activity, closely resembling the clinical presentation of TTP.
Case Presentation
A 51-year-old male of Chinese descent returned to Hubei Province, China, from Africa and remained at home for five days before traveling to Guangzhou, where he developed symptoms of fever, with a maximum body temperature of 39.9°C. He reported experiencing fatigue and nausea but did not exhibit a cough, chest tightness, or shortness of breath. Consequently, he was admitted to the hospital, where laboratory tests indicated thrombocytopenia and leukocytosis. The patient was advised to seek further evaluation at a higher-level medical facility. Subsequently, he presented to the emergency department of Tongji Hospital with a high fever during the night, altered consciousness, unresponsiveness to verbal stimuli, and was accompanied by convulsions and urinary incontinence. Electrocardiogram monitoring revealed a blood pressure of 80/60 mmHg, a respiratory rate of 26 breaths per minute, and an oxygen saturation level of 92%. Upon admission to the Intensive Care Unit, laboratory evaluations were conducted, revealing leukocytosis (11.71 × 109/L; reference range [RR] = 3.5–9.5 × 109/L), thrombocytopenia (27 × 109/L; RR = 125.0–350.0 × 109/L), normal hemoglobin levels (129 g/L; RR = 130.0–175.0 g/L), elevated lactate dehydrogenase (453 U/L; RR = 120–250 U/L), significantly elevated D-D dimer (> 21 μg/mL; RR < 0.5 μg/mL), increased free hemoglobin (> 400 mg/L; RR < 40 mg/L), and markedly elevated von Willebrand factor antigen (vWF:Ag) at 623.3% (RR = 50–200%) and von Willebrand factor activity (vWFACT) at 462.9% (RR = 50–200%). Initially, the clinician suspected severe fever with thrombocytopenia syndrome (SFTS), given the patient’s recent stay in a region endemic for SFTS during the current season. However, SFTS was ruled out due to negative Dabie-Banda RNA test results. Furthermore, the patient exhibited a high likelihood of TTP, with a PLASMIC score of 7. In relevant clinical scenarios, an ADAMTS13 activity level of less than 10% would further substantiate a TTP diagnosis. The patient was determined to be free of TTP based on the results of the ADAMTS13 activity assay, which indicated a level of 95.8% (reference range: 65.0–135.0%). Concurrently, a significant presence of Plasmodium falciparum was detected in erythrocytes via microscopy (Figure 1), correlating with the observed thrombocytopenia. Consequently, the patient was diagnosed with Plasmodium falciparum infection and severe cerebral malaria. At midnight, the patient exhibited symptoms of confusion, intermittent convulsions, dyspnea, and reduced oxygen saturation. Sedation and immediate intubation were administered, followed by treatment with intravenous artesunate. After 24 hours, the patient’s overall condition showed gradual improvement, and the parasitemia rate in erythrocytes decreased from 9.0% to 0.03% (Figure 2). Two days later, the patient, although still experiencing some cognitive disorientation, was verbally responsive and subsequently extubated. The patient was discharged upon request after the platelet count increased to 162 × 109/L. Changes in laboratory markers during the hospital stay are detailed in Table 1, which illustrates the progressive improvement and normalization of platelet counts, indirect bilirubin (IBIL), lactate dehydrogenase (LDH), free hemoglobin (HGB), and D-dimer levels following antimalarial treatment. However, the vWF:Ag and von Willebrand factor activity (vWF:AC) levels were markedly elevated.
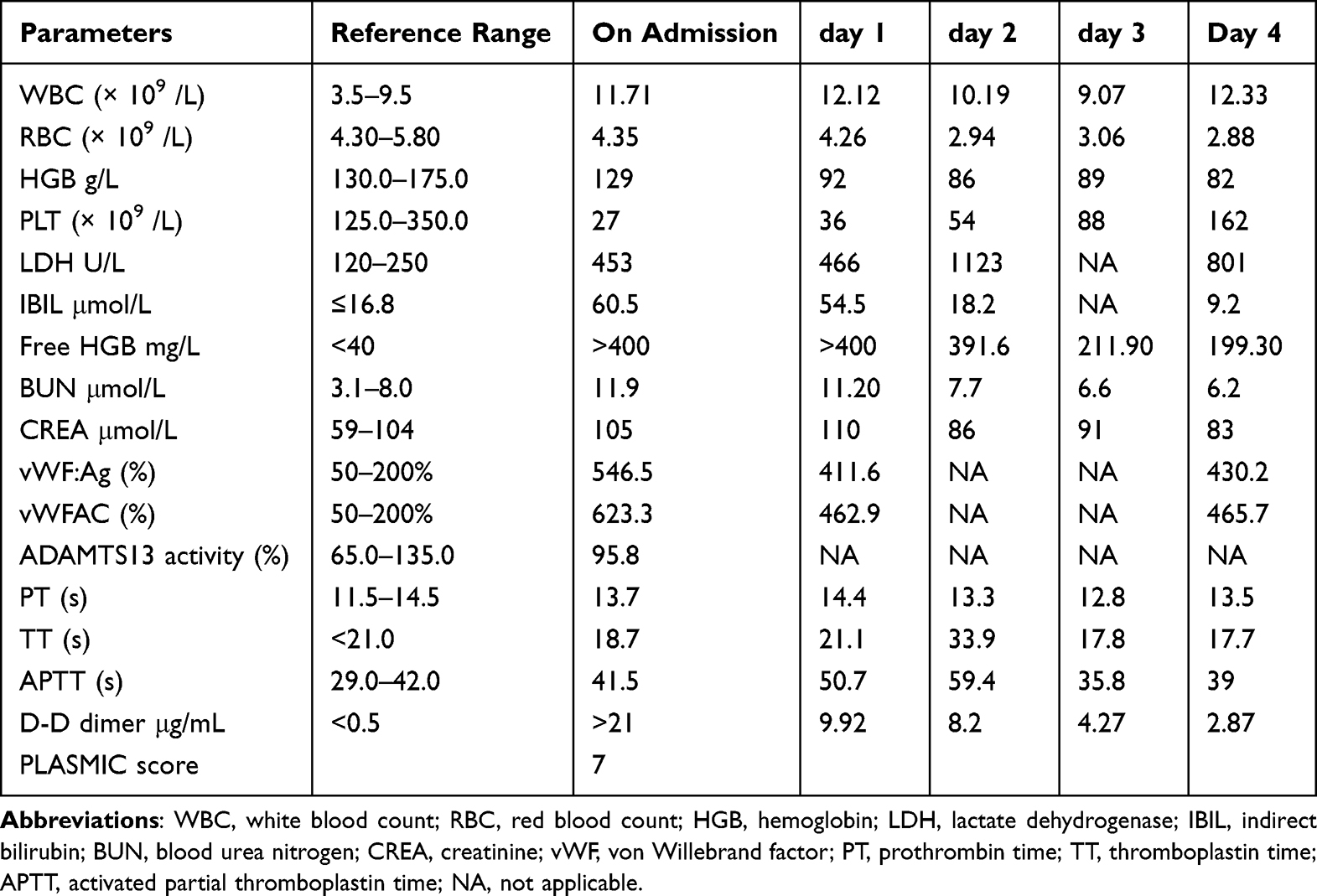 |
Table 1 Laboratory Marker Changes During Hospital Stay |
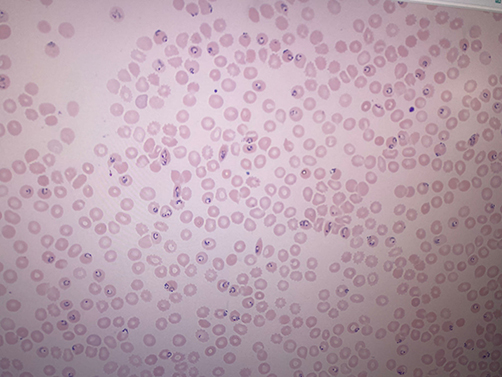 |
Figure 1 Plasmodium falciparum-infected red blood cells before intravenous artesunate administration. |
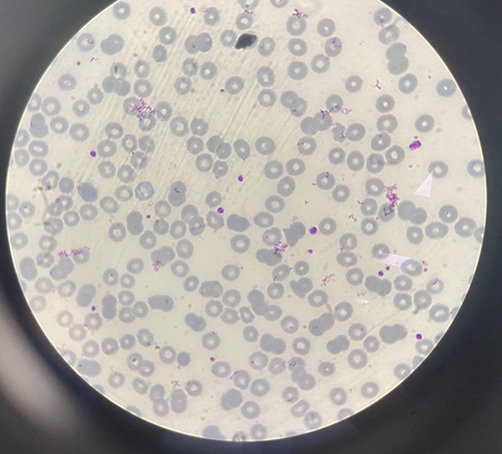 |
Figure 2 Plasmodium falciparum-infected red blood cells treated with intravenous artesunate 24 hours later. |
Discussion
The overlap in laboratory and clinical manifestations, including fever, thrombocytopenia, severe anemia, and intravascular coagulation, observed in both malaria and TTP, may be attributed to the presence of TMA in both conditions.6,7 Sinha et al8 documented that renal histopathology in cases of Plasmodium infection exhibited features characteristic of TMA. In a case analogous to ours, Kurek et al9 described a patient initially diagnosed with malaria but erroneously identified as having TTP. Malaria can manifest with TTP-like alterations; thus, administering treatment for TTP might ameliorate the patient’s condition even in instances of misdiagnosis. Recently, Kunwar et al10 reported a case involving a patient who had traveled to Nigeria and contracted malaria, with ADAMTS13 activity exceeding 10%. The patient received antimalarial therapy without undergoing plasmapheresis and was discharged approximately one week later following normalization of platelet counts and symptomatic improvement. Both cases demonstrated reduced ADAMTS13 activity, albeit greater than 10%, which contrasts with our findings. This discrepancy may be attributable to variations in disease stages and ethnic backgrounds. However, it is noteworthy that the von Willebrand factor antigen (vWF:Ag) and von Willebrand factor activity (vWF:AC) tests were not conducted in these cases.
In our study, the patient exhibited significantly elevated levels of vWF:Ag and vWF:AC, while maintaining normal ADAMTS13 activity. Serial measurements of vWF:Ag and vWFAC were conducted thrice during the patient’s hospitalization, revealing persistently elevated levels upon discharge. A review11 showed studies conducted on healthy volunteers infected with Plasmodium falciparum revealed that the elevation in plasma von Willebrand factor antigen (vWF:Ag) and vWF propeptide (vWFpp) was increased from the early stages post-infection and these levels correspond closely with the severity of the disease.Hollestelle et al12 have similarly reported that elevated levels of vWF and vWF propeptide (vWFPP) are most pronounced in patients with severe cerebral and non-cerebral malaria. Their study, which included 26 patients with cerebral malaria, assessed these levels after 24 hours and 3 days of treatment. They observed that vWFPP levels were significantly reduced compared to admission levels, with half of the patients returning to normal levels after three days of treatment. Although vWF levels did not significantly decrease after 24 hours of treatment, a significant reduction was noted by the third day. Nonetheless, vWF levels remained elevated in the majority of cases. These findings are consistent with our laboratory results, although we did not conduct vWFPP testing. Additional studies13,14 have demonstrated that elevated vWF levels can precede the appearance of parasites in peripheral blood smears. Meanwhile, we observed that the patient had a high level of D-dimer on the date admission. A review15 emphasizes a strong link between increased D-dimer levels and Plasmodium infections, particularly involving P. falciparum. Increased D-dimer levels were considerated as indicative of coagulation activation and fibrinolysis. And they were noted in a significant portion of malaria patients. This points to an underlying hypercoagulable state that may contribute to the development of complications.
Malaria and TTP exhibit notable laboratory and clinical similarities, primarily due to the presence of TMA. This observation suggests a potential mechanism wherein elevated levels of vWF may induce TMA in malaria. The activation of endothelial cells (ECs) occurs when erythrocytes infected with Plasmodium falciparum adhere to these cells.16 Subsequently, Weibel-Palade bodies (WPBs) release ultra-large vWF into the bloodstream. These ultra-large vWF strings facilitate the recruitment and sequestration of platelets, which in turn activate additional ECs, thereby enhancing WPB secretion. Mature P. falciparum parasites express the P. falciparum erythrocyte membrane protein 1 (PfEMP1), which is capable of binding to platelet-decorated vWF strings through platelet CD36. Consequently, the presence of ultra-large vWF increases endothelial cell permeability, leading to thrombosis.17,18 In a study conducted by O’Regan et al, Plasmodium berghei ANKA was used to infect mice, resulting in a model that accurately replicates cerebral malaria in humans. The findings of this study revealed that, in comparison to wild-type controls, vWF-deficient (vWF-/-) mice exhibited protection against Plasmodium berghei infection.19 These results suggest that vWF may play a critical role in the pathogenesis of cerebral malaria.
We also note some limitations of the study. Firstly, we cannot conduct vWFPP testing.
Maybe the level of vWFPP is more meaningful than vWF. Secondly, the patient recovered quickly so that the follow-up was short.
Conclusion
Malaria and thrombotic thrombocytopenic purpura (TTP) exhibit notable laboratory and clinical similarities due to the presence of thrombotic microangiopathy (TMA). Prompt differential laboratory diagnosis between malaria and TTP is crucial, as it may facilitate the early commencement of lifesaving interventions for certain patients. Therefore, it is essential to assess von Willebrand factor (vWF) levels and ADAMTS13 activity in individuals diagnosed with malaria.
Ethics Approval and Consent
Institutional approval is not required for publication, so informed written consent for using patient information and case report publication was obtained from the patient as long as identifying data are anonymous.The patient has provided informed consent for the publication of this case report and accompanying images.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Supported by Municipal Financial Subsidy of Shenzhen Medical Key Discipline Construction(No.SZXK054).
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Naing C, Whittaker MA, Nyunt Wai V, Mak JW. Is Plasmodium vivax malaria a severe malaria?: a systematic review and meta-analysis. PLoS Negl Trop Dis. 2014;8(8):e3071. doi:10.1371/journal.pntd.0003071
2. M DA, Desakorn V, Pongtavornpinyo W, et al. Estimation of the total parasite biomass in acute falciparum malaria from plasma PfHRP2. PLoS Med. 2005;2(8):e204. doi:10.1371/journal.pmed.0020204
3. U KK, Mahittikorn A, Wilairatana P, et al. An update on the pathogenesis and diagnosis of thrombotic thrombocytopenic purpura. Expert Rev Hematol. 2023;16(1):17–32. doi:10.1080/17474086.2023.2159803
4. Lenting PJ, Christophe OD, Denis CV. Denis, von Willebrand factor biosynthesis, secretion, and clearance: connecting the far ends. Blood. 2015;125(13):2019–2028. doi:10.1182/blood-2014-06-528406
5. Leebeek F, Eikenboom J. von Willebrand disease. N Engl J Med. 2017;376(7):701–702.
6. Varo R, Chaccour C, Bassat Q. Update on malaria. Med Clin. 2020;155(9):395–402. doi:10.1016/j.medcli.2020.05.010
7. Chiasakul T, Cuker A. Clinical and laboratory diagnosis of TTP: an integrated approach. Hematology Am Soc Hematol Educ Program. 2018;2018(1):530–538. doi:10.1182/asheducation-2018.1.530
8. Sinha A, Singh G, S BA, et al. Thrombotic microangiopathy and acute kidney injury following vivax malaria. Clin Exp Nephrol. 2013;17(1):66–72. doi:10.1007/s10157-012-0656-9
9. Kurek M, Pasieka P, Wludarczyk A, et al. When malaria imitates thrombotic thrombocytopenic purpura: importance of patient history and physician awareness of uncommon diseases. Pol Arch Intern Med. 2023;133(11). doi:10.20452/pamw.16569.
10. Kunwar K, Karki S, Jain M, et al. Plasmodium falciparum malaria presenting as a Thrombotic Thrombocytopenic Purpura (TTP) mimic: a case report. Cureus. 2024;16(3):e56181. doi:10.7759/cureus.56181
11. O’Donnell AS, Fazavana J, O’Donnell JS. The von Willebrand factor - ADAMTS-13 axis in malaria. Res Pract Thromb Haemost. 2022;6(1):e12641. doi:10.1002/rth2.12641
12. Hollestelle MJ, Donkor C, Mantey EA, et al. von Willebrand factor propeptide in malaria: evidence of acute endothelial cell activation. Br J Haematol. 2006;133(5):562–569. doi:10.1111/j.1365-2141.2006.06067.x
13. de Mast Q, Groot E, Lenting PJ, et al. Thrombocytopenia and release of activated von willebrand factor during early plasmodium falciparum malaria. J Infect Dis. 2007;196(4):622–628. doi:10.1086/519844
14. Kraisin S, Verhenne S, Pham TT, et al. von Willebrand factor in experimental malaria-associated acute respiratory distress syndrome. J Thromb Haemost. 2019;17(8):1372–1383. doi:10.1111/jth.14485
15. Sukati S, Kotepui KU, Masangkay FR, et al. Elevations in D-dimer levels in patients with Plasmodium infections: a systematic review and meta-analysis. Sci Rep. 2025;15(1):858. doi:10.1038/s41598-024-84907-x
16. Storm J, Craig AG. Pathogenesis of cerebral malaria--inflammation and cytoadherence. Front Cell Infects Microbiol. 2014;4:100.
17. Moxon CA, Grau GE, Craig AG. Malaria: modification of red blood cells and consequences in the human host. Br J Haematol. 2011;154(6):670–679. doi:10.1111/j.1365-2141.2011.08755.x
18. A.s O, J.s F, O’Donnell JS. O’ Donnell.The von Willebrand factor ADAMTS-13 axis in malaria. Res Pract Thromb Haemost. 2022;6(1):e12641.
19. O’Regan N, Gegenbauer K, M OJ, et al. A novel role for von Willebrand factor in the pathogenesis of experimental cerebral malaria. Blood. 2016;127(9):1192–1201. doi:10.1182/blood-2015-07-654921
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.