Back to Journals » International Medical Case Reports Journal » Volume 19
Severe Hypokalemia Complicated by Wernicke’s Encephalopathy and Hypoxic–Ischemic Brain Injury in Pregnancy: A Case from a Resource-Limited ICU
Authors Tahajud OA ![]() , Elmi AH
, Elmi AH ![]() , Ahmed OH, Ali HA
, Ahmed OH, Ali HA
Received 21 January 2026
Accepted for publication 17 April 2026
Published 21 April 2026 Volume 2026:19 597732
DOI https://doi.org/10.2147/IMCRJ.S597732
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Osman Ahmed Tahajud,1 Abdullahi Hassan Elmi,2 Omar Hassan Ahmed,3 Hamdi Abdi Ali1
1Department of Internal Medicine, Dr.Sumait Hospital, Faculty of Medicine and Health Sciences, SIMAD University, Mogadishu, Somalia; 2Department of Nursing and Midwife, Dr.Sumait Hospitals, Faculty of Medicine and Health Sciences, SIMAD University, Mogadishu, Somalia; 3Department of Radiology, Dr. Sumait Hospitals, Faculty of Medicine and Health Sciences, SIMAD University, Mogadishu, Somalia
Correspondence: Osman Ahmed Tahajud, Email [email protected]
Introduction: Pregnancy is a metabolically vulnerable state in which electrolyte disturbances, nutritional deficiencies, and hypoxic events can rapidly lead to severe neurological complications. Wernicke’s encephalopathy and hypoxic–ischemic brain injury are uncommon but potentially devastating conditions that are frequently underdiagnosed, particularly in resource-limited intensive care settings. To our knowledge, the coexistence of profound hypokalemia, Wernicke’s encephalopathy, and hypoxic–ischemic brain injury during pregnancy has been rarely reported, particularly from resource-limited intensive care settings.
Case Presentation: We report the case of a 22-year-old previously healthy pregnant woman at 18 weeks’ gestation who presented with prolonged vomiting, progressive lower-limb weakness, and acute respiratory failure requiring mechanical ventilation. Laboratory evaluation revealed severe hypokalemia with associated acute kidney injury. Despite correction of electrolyte abnormalities, she developed persistent neuromuscular weakness, recurrent respiratory failure, and hemodynamic instability. Fluctuating mental status and ophthalmoplegia raised suspicion for Wernicke’s encephalopathy, and high-dose parenteral thiamine was initiated. Brain magnetic resonance imaging later demonstrated hypoxic–ischemic changes. Her clinical course was further complicated by rhabdomyolysis, hepatic dysfunction, thrombocytopenia, and intrauterine fetal demise. Following prolonged ventilatory support and tracheostomy, she achieved partial neurological recovery and was discharged with ongoing rehabilitation needs.
Conclusion: This case highlights the complex interplay between severe electrolyte disturbances, thiamine deficiency, and hypoxic brain injury during pregnancy. Early recognition of nutritional and metabolic causes of neurological deterioration, prompt empiric thiamine therapy, and aggressive prevention of hypoxic events are critical to improving maternal outcomes, particularly in resource-limited settings.
Keywords: pregnancy, hypokalemia, Wernicke’s encephalopathy, hypoxic–ischemic brain injury, resource-limited ICU, quadriparesis
Introduction
Pregnancy is a physiologically vulnerable state in which metabolic, nutritional, and electrolyte imbalances may rapidly evolve into life-threatening neurological and respiratory complications if not promptly recognized and managed. Severe electrolyte disturbances are well-established but often underappreciated causes of acute encephalopathy, neuromuscular weakness, and respiratory failure, particularly in critically ill patients and in resource-limited settings where diagnostic and therapeutic delays are common.1 Hypokalemia, in particular, can precipitate profound muscle weakness, paralysis, and respiratory compromise, while also contributing to secondary organ dysfunction, including rhabdomyolysis and acute kidney injury.1
Wernicke’s encephalopathy (WE) is an acute, potentially reversible neuropsychiatric syndrome caused by thiamine deficiency and classically characterized by the triad of altered mental status, ophthalmoplegia, and ataxia. Although traditionally associated with chronic alcoholism, WE is increasingly recognized in non-alcoholic populations, including pregnant women with hyperemesis gravidarum, malnutrition, and prolonged critical illness.2–4 The diagnosis is frequently missed due to its variable and incomplete clinical presentation, leading to delayed treatment and irreversible neurological injury. Early recognition and prompt parenteral thiamine administration are therefore essential to prevent permanent deficits and mortality.2–4
Hypoxic–ischemic brain injury (HIBI) represents another devastating neurological complication that may arise secondary to prolonged hypoxia due to neuromuscular weakness and respiratory failure. In critically ill patients, especially in low-resource intensive care units, limited access to advanced monitoring, neuroimaging, and standardized neurocritical care protocols further increases the risk of delayed diagnosis and poor neurological outcomes.5,6 While hypoxic–ischemic encephalopathy is extensively studied in neonatal populations, adult and maternal cases, particularly those occurring in conjunction with metabolic derangements, remain underreported and mortality poorly characterized.6
The coexistence of severe electrolyte imbalance, Wernicke’s encephalopathy, and hypoxic–ischemic brain injury during pregnancy represents a rare but catastrophic clinical scenario with complex diagnostic and therapeutic challenges. This is especially true in resource-limited settings, where shortages of imaging modalities, laboratory support, and critical care infrastructure may complicate management and worsen outcomes.5,7 Reporting such cases is essential to raise awareness, highlight diagnostic pitfalls, and emphasize the importance of early metabolic correction and empiric thiamine therapy in high-risk patients.7
In this report, we describe a young pregnant woman who developed prolonged quadriparesis and respiratory failure due to severe electrolyte disturbances, complicated by Wernicke’s encephalopathy and hypoxic–ischemic brain injury, managed in a resource-limited intensive care unit. This case underscores the need for heightened clinical suspicion, early nutritional intervention, and multidisciplinary care to prevent irreversible neurological injury in vulnerable populations.
Case Presentation
A 22-year-old previously healthy pregnant woman at 18 weeks’ gestation was transferred to our emergency department and intubated from another facility. She had suffered from nausea and vomiting for four weeks (mostly secondary to hyperemesis gravidarum), progressive lower limb weakness for two weeks, and an acute loss of consciousness with respiratory distress six hours before admission. There was no history of thyroid disease, periodic paralysis, neuromuscular disorders, medication use, or herbal intake.
Intubation at the referring hospital was reported as technically difficult, complicated by a small left-sided pneumothorax (Figure 1). A repeat X-ray following day revealed resolution of the pneumothorax but expanding subcutaneous emphysema (Figure 2). She was manually ventilated with an ambubag during transfer. On arrival, she was admitted to the ICU and mechanically ventilated. Neurological examination revealed a Glasgow Coma Scale score of E1 VT M2. She was afebrile with no neck stiffness. Muscle tone was normal, deep tendon reflexes were brisk bilaterally, and plantar responses were downgoing. Chest examination showed extensive subcutaneous emphysema from the infraclavicular region to the neck, with vesicular breath sounds bilaterally. Cardiac and abdominal examinations were unremarkable except for tachycardia and abdominal distension consistent with gestational age.
 |
Figure 1 Frontal chest radiograph obtained after difficult endotracheal intubation at the referring facility, demonstrating a small left-sided pneumothorax with associated subcutaneous emphysema extending into the lower neck. These findings are clinically relevant because they reflect an early airway-related complication that contributed to the patient’s respiratory instability during transfer and initial intensive care management. |
 |
Figure 2 (A) Follow-up frontal chest radiographs obtained during the early intensive care course. (A) Image obtained approximately 24 hours after the initial study shows interval resolution of the left-sided pneumothorax. (B) Subsequent radiograph demonstrates progressive pneumomediastinum and worsening subcutaneous emphysema extending into the lower neck, supraclavicular regions, and axillae. These serial findings illustrate progression of thoracic air dissection despite resolution of the pneumothorax and help explain the patient’s ongoing respiratory complexity. |
Initial laboratory evaluation demonstrated profound hypokalemia (1.83 mmol/L), mild acute kidney injury (creatinine 1.89 mg/dL), elevated transaminases (AST 173.2 U/L, ALT 106.5 U/L), normal sodium at presentation (140.6 mmol/L), normal inflammatory markers (CRP <2.50 mg/L), and a normal platelet count (291 ×109/L). Magnesium was low early in the course (1.22 mg/dL) and later normalized with treatment. Key laboratory and clinical findings at admission and at discharge / late recovery period are summarized in (Table 1). Because severe hypokalemia was considered a major contributor to her weakness and respiratory compromise, urgent potassium replacement was initiated with ongoing clinical and biochemical monitoring.
 |
Table 1 Key Laboratory and Clinical Findings at Admission and at Discharge/Late Recovery Period. The Table Highlights the Severity of Metabolic Derangement at Presentation and the Patient’s Subsequent Partial Biochemical and Clinical Recovery During Hospitalization. Parameters Not Retrievable From the Accessible Medical Record are Reported Transparently as Unavailable |
Over 48 hours, her consciousness partially improved, but quadriparesis persisted (power MRC grade 1/5 in both upper and lower limbs). She was extubated on day three but quickly deteriorated with respiratory distress, hypotension (70/40 mmHg), and confusion, requiring re-intubation and vasopressor support. Despite correction of electrolytes, respiratory muscle weakness persisted. Because the persistence of quadriparesis and ventilatory failure was not fully explained by correction of hypokalemia alone, alternative neuromuscular diagnoses, including Guillain-Barré syndrome, were also considered clinically. However, confirmatory investigations such as nerve conduction studies, cerebrospinal fluid analysis, and electromyography were not available during the acute phase in our resource-limited setting.
Her ICU course was complicated by hypernatremia, rhabdomyolysis (creatinine kinase 2742), progressive thrombocytopenia, hepatic dysfunction with jaundice, pulmonary bleeding causing recurrent endotracheal tube obstruction, and worsening subcutaneous emphysema (Figure 3). Obstetric ultrasonography revealed intrauterine fetal demise, and delivery was induced without complication.
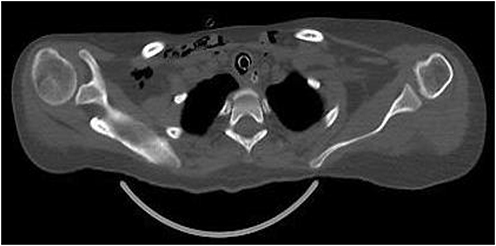 |
Figure 3 Coronal computed tomography image of the chest (Bone window) demonstrating extensive subcutaneous emphysema involving the lower neck, supraclavicular regions, and upper mediastinum. This imaging finding is clinically important because it confirms the extent of thoracic air leakage and helps account for the patient’s complicated respiratory course following difficult airway management and recurrent ventilatory deterioration. |
Fluctuating mental status and ophthalmoplegia raised strong clinical suspicion for Wernicke’s encephalopathy in the context of prolonged vomiting, pregnancy, and likely nutritional depletion. High-dose parenteral vitamin B complex containing thiamine was started empirically as soon as this diagnosis was suspected, because isolated parenteral thiamine was not immediately available. Intravenous thiamine was administered separately once it became available, approximately two days later. Arterial blood gas values and detailed electrocardiographic findings were not consistently available in the accessible medical record and therefore could not be reported reliably in this case.
Brain MRI was obtained later in the clinical course, after recurrent respiratory deterioration and hemodynamic instability, and demonstrated findings interpreted as more consistent with hypoxic–ischemic brain injury than with a classic isolated imaging pattern of Wernicke’s encephalopathy (Figure 4). Following prolonged ventilatory support and tracheostomy, she gradually improved. Respiratory strength recovered sufficiently for decannulation. Neurological recovery was partial, with upper limb strength improving to grade 4 and lower limb to grade 2 at discharge. She was sent home with physiotherapy and psychological support.
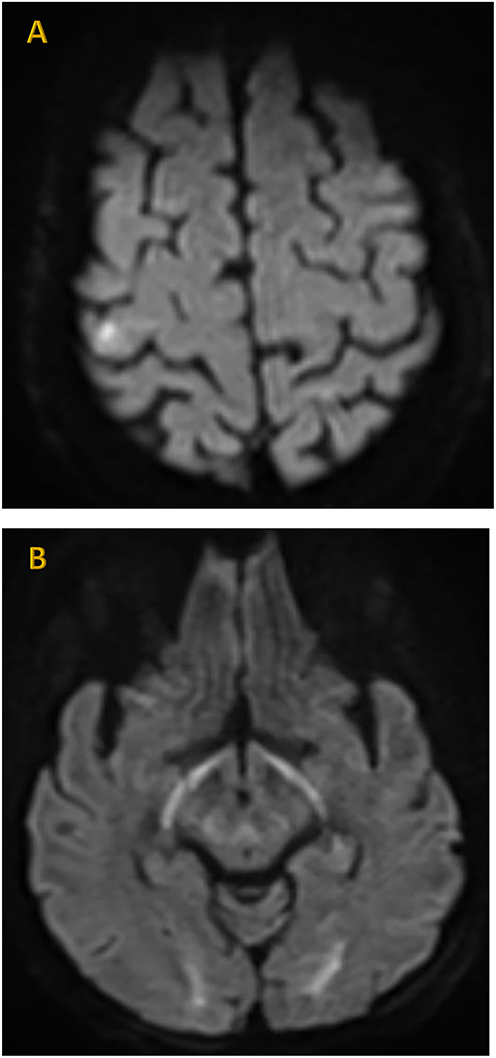 |
Figure 4 (A and B) Axial brain magnetic resonance imaging diffusion-weighted imaging sequences demonstrating multifocal areas of diffusion restriction involving the external capsules, posterior limbs of the internal capsules, postcentral gyri, and splenium of the corpus callosum. In the context of recurrent respiratory failure, hypotension, and delayed neurological recovery, these findings were interpreted as being more consistent with hypoxic–ischemic brain injury. Although neuroimaging may contribute to the assessment of Wernicke’s encephalopathy, the diagnosis in this case remained primarily clinical and was based on the combination of prolonged vomiting, altered mental status, ophthalmoplegia, and a high-risk nutritional state during pregnancy. |
Discussion
This case is clinically and educationally important because it illustrates a rare but life-threatening overlap of severe electrolyte disturbance, nutritional deficiency, and hypoxic neurological injury during pregnancy. Although each of these conditions may be encountered individually, their coexistence in a single pregnant patient created major diagnostic and therapeutic complexity, particularly in a resource-limited intensive care setting. The case also demonstrates how prolonged vomiting, delayed presentation, and evolving multisystem complications can rapidly progress from a potentially reversible metabolic problem to sustained neurological disability if early warning signs are not recognized. For clinicians, the central lesson is that acute weakness and respiratory failure in pregnancy should prompt urgent evaluation not only for electrolyte abnormalities, but also for concurrent nutritional and hypoxic complications that may require immediate empiric treatment.1,7
Severe hypokalemia is a well-established cause of acute flaccid paralysis and respiratory muscle weakness due to impaired membrane excitability at the neuromuscular junction. In extreme cases, it may progress to life-threatening respiratory failure and cardiac instability, as well as secondary complications such as rhabdomyolysis and acute kidney injury. Although hypokalemic periodic paralysis was initially suspected, the persistence of quadriparesis despite correction of potassium levels suggests that electrolyte disturbance alone did not fully explain the neurological deficits in this case.1 This highlights the importance of reassessing the diagnosis when neurological recovery is delayed after metabolic normalization.1 An important differential diagnosis in this case was Guillain-Barré syndrome, given the presence of progressive limb weakness, respiratory failure, and autonomic instability. Other considerations included hypokalemic periodic paralysis, myasthenia gravis, and critical illness-related neuromuscular weakness. Guillain-Barré syndrome was considered because of the pattern of weakness and ventilatory compromise; however, several features made it less convincing as the primary explanation. The onset followed prolonged vomiting with profound biochemical derangement, severe hypokalemia was documented at presentation, and part of the neurological picture was plausibly explained by metabolic and nutritional factors. In addition, the clinical course evolved in parallel with multisystem complications, including encephalopathy, ophthalmoplegia, and hypoxic events, which suggested a more complex overlapping process rather than an isolated peripheral neuropathy alone. Nevertheless, Guillain-Barré syndrome could not be definitively excluded because cerebrospinal fluid analysis, nerve conduction studies, and electromyography were not available during the acute illness. This limitation should be acknowledged when interpreting the diagnostic pathway in this case.1,5,7
In this patient, prolonged vomiting during pregnancy, fluctuating mental status, and ophthalmoplegia supported a clinical working diagnosis of Wernicke’s encephalopathy and justified empiric parenteral thiamine administration without waiting for definitive confirmation. In this case, the clinical suspicion for Wernicke’s encephalopathy was based on prolonged vomiting, altered mental status, and ophthalmoplegia in a high-risk pregnant patient, which is compatible with established clinical diagnostic frameworks such as the Caine criteria, even in the absence of a complete classic triad or definitive early imaging findings.2–4 Delayed recognition of Wernicke’s encephalopathy is strongly associated with irreversible neurological injury, which may explain the incomplete neurological recovery observed. Although neuroimaging can support the diagnosis of Wernicke’s encephalopathy, the diagnosis in this case remained primarily clinical, and the MRI findings were interpreted more cautiously in view of concurrent hypoxic–ischemic injury.4
The subsequent identification of hypoxic–ischemic brain injury further clarified the patient’s prolonged neurological deficits. Episodes of respiratory failure, hypotension, difficult airway management, and possible hypoventilation during transport likely contributed to global cerebral hypoxia. Hypoxic–ischemic brain injury in adults remains under recognized outside of cardiac arrest, particularly in low-resource intensive care units where advanced neuromonitoring and timely neuroimaging may be unavailable. MRI confirmation in this case underscores the importance of considering hypoxic injury when neurological recovery is disproportionate to metabolic correction.5,6
In addition, some investigations that would have further strengthened diagnostic characterization, including full electrophysiologic assessment and complete contemporaneous documentation of all critical care parameters, were either unavailable or incompletely documented during the acute phase. Resource limitations played a significant role in shaping both diagnosis and outcome. Delayed referral, limited access to imaging, absence of standardized neocritical care pathways, and constraints in laboratory monitoring are common challenges in low- and middle-income settings and are associated with worse neurological outcomes. These systemic factors may have delayed recognition of thiamine deficiency and hypoxic injury, prolonging exposure to potentially reversible insults.5–7 This case underscores how structural healthcare limitations can amplify disease severity despite appropriate clinical suspicion and supportive care.
The occurrence of intrauterine fetal demise highlights the profound maternal–fetal consequences of severe maternal illness. Sustained maternal hypoxia, hypotension, metabolic derangements, and critical illness are well-recognized contributors to fetal compromise and death. While hypoxic–ischemic encephalopathy has been extensively studied in neonatal populations, maternal hypoxic brain injury during pregnancy remains poorly described in the literature, particularly in low-resource contexts. This case adds to the limited evidence emphasizing the need for aggressive maternal stabilization to improve both maternal and fetal outcomes.5,8
For clinicians working in low-resource settings, the case is particularly relevant because it illustrates how delayed recognition of reversible metabolic and nutritional insults may contribute to preventable neurological disability.5,7
Overall, this case offers several practical lessons for clinicians caring for pregnant patients with acute neurological and respiratory deterioration. First, severe electrolyte abnormalities in pregnancy should not be viewed in isolation, particularly when weakness, altered mental status, or respiratory compromise persist despite biochemical correction. Second, prolonged vomiting and critical illness should raise early suspicion for thiamine deficiency, and empiric parenteral thiamine should be administered promptly when Wernicke’s encephalopathy is clinically suspected. Third, recurrent hypoxic episodes may substantially worsen neurological outcomes and should be actively anticipated and prevented. These lessons are especially relevant in resource-limited intensive care units, where delays in diagnosis and limited access to advanced investigations may increase the risk of preventable maternal and fetal harm.1–7
Clinical Teaching Points
- In pregnant patients with prolonged vomiting, weakness, and respiratory compromise, profound electrolyte abnormalities may coexist with nutritional and neurological complications.
- Persistent weakness after potassium correction should prompt reconsideration of the differential diagnosis rather than assuming a purely metabolic paralysis.
- Wernicke’s encephalopathy should be considered early in high-risk pregnant patients with altered mental status or ophthalmoplegia, even in the absence of alcohol use.
- Empiric parenteral thiamine should not be delayed when clinical suspicion is high.
- In resource-limited intensive care settings, early recognition and prevention of hypoxic events are essential to reduce irreversible neurological injury.
Conclusion
This case highlights the potentially catastrophic consequences of overlapping metabolic, nutritional, and hypoxic insults during pregnancy, particularly when they present with acute weakness, respiratory failure, and altered mental status. Although profound hypokalemia was a major contributor to the initial presentation, the persistence of neurological deficits despite electrolyte correction underscored the need to consider a broader differential diagnosis, including nutritional and neuromuscular causes, as well as secondary hypoxic brain injury.
In resource-limited intensive care settings, delayed referral, restricted diagnostic capacity, and limited access to advanced neurocritical care may further complicate recognition of these overlapping conditions. Clinicians should therefore maintain a broad and cautious diagnostic approach in pregnant or critically ill patients with evolving neurological deterioration, and should consider metabolic, nutritional, neuromuscular, and hypoxic etiologies in parallel rather than in isolation. Early correction of electrolyte abnormalities, prompt empiric parenteral thiamine when deficiency is suspected, and aggressive prevention of hypoxic events remain essential to reducing preventable neurological injury and improving maternal outcomes.
Ethics and Consent
Written informed consent was obtained from the patient for the publication of this case report and the accompanying images. Ethical approval was not required for case reports at our institution.
Acknowledgments
This research was supported by SIMAD University, Mogadishu, Somalia. We would like to express our sincere appreciation to the Center for Research and Development at SIMAD University for their valuable support, guidance, and constructive recommendations.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that there are no conflicts of interest related to this study.
References
1. Samuels MA, Seifter JL. Encephalopathies caused by electrolyte disorders. Semin Neurol. 2011;31(02):135–9. doi:10.1055/s-0031-1277983
2. Sinha S, Kataria A, Kolla BP, Thusius N, Loukianova LL. Wernicke encephalopathy—clinical pearls. Mayo Clin Proc. 2019;94(6):1065–1072. doi:10.1016/j.mayocp.2019.02.018
3. Habas E, Farfar K, Errayes N, Rayani A, Elzouki AN. Wernicke encephalopathy: an updated narrative review. Saudi J Med Med Sci. 2023;11(3):193–200. doi:10.4103/sjmms.sjmms_416_22
4. Sechi G, Serra A. Wernicke’s encephalopathy: new clinical settings and recent advances in diagnosis and management. Lancet Neurol. 2007;6(5):442–455. PMID: 17434099. doi:10.1016/S1474-4422(07)70104-7
5. Garcia-Alix A, Arnaez J, Arca G, Martinez-Biarge M. Hypoxic-ischaemic encephalopathy code: a systematic review for resource-limited settings. Anales de Pediatría. 2024;100(4):275–286. doi:10.1016/j.anpede.2024.04.001
6. Nicks B, Henley J, Mfinanga J, Manthey D. Neurologic emergencies in resource-limited settings: a review of stroke care considerations. Afr J Emergency Med. 2015;5(1):37–44. doi:10.1016/j.afjem.2014.06.002
7. Ryan ET, Hill DR, Solomon T, Aronson N, Endy TP. Hunter’s Tropical Medicine and Emerging Infectious Diseases e-Book. Elsevier Health Sciences; 2019.
8. Aker K, Støen R, Eikenes L, et al. Therapeutic hypothermia for neonatal hypoxic-ischaemic encephalopathy in India (THIN study): a randomised controlled trial. Arch Dis Child Fetal Neonatal Ed. 2020;105(4):405–411. PMID: 31662328; PMCID: PMC7363785. doi:10.1136/archdischild-2019-317311
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.