Back to Journals » International Medical Case Reports Journal » Volume 19
Severe Ectopic ACTH–Dependent Cushing Syndrome Due to a Neuroendocrine Tumor of Occult Primary Origin Presenting with Widespread Metastases and Early Vertebral Fractures: A Rare Case Report
Authors Aria MN, Rasikh AS ![]() , Tayeb AJ, Aram MM
, Tayeb AJ, Aram MM ![]() , Hassan AJ, Ferdaws MK
, Hassan AJ, Ferdaws MK
Received 24 April 2026
Accepted for publication 9 June 2026
Published 10 June 2026 Volume 2026:19 619542
DOI https://doi.org/10.2147/IMCRJ.S619542
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Tanvi Dhere
Mohammad Nabi Aria,1,* Ahmad Shekaib Rasikh,2,* Ahmad Jawad Tayeb,1 Mohammad Maroof Aram,1 Abdul Jalil Hassan,2 Mohammad Khalid Ferdaws1
1Department of Internal Medicine, Ali Abad Teaching Hospital, Kabul University of Medical Sciences, Kabul, Afghanistan; 2Department of Infectious Diseases, Ali Abad Teaching Hospital, Kabul University of Medical Sciences, Kabul, Afghanistan
*These authors contributed equally to this work
Correspondence: Ahmad Shekaib Rasikh, Department of Infectious Diseases, Ali Abad Teaching Hospital, Kabul University of Medical Sciences, Kabul, 1001, Afghanistan, Tel +93791906514, Email [email protected]
Abstract: Ectopic adrenocorticotropic hormone (ACTH)-dependent Cushing syndrome is an uncommon cause of hypercortisolism, often associated with neuroendocrine tumors and challenges in localizing the primary source. We report a 30-year-old woman presenting with progressive lower limb weakness, generalized pain, and difficulty walking, along with recently diagnosed hypertension and diabetes. Clinical and biochemical findings were consistent with severe ACTH-dependent Cushing syndrome. Imaging revealed no definite pituitary lesion but demonstrated pulmonary and hepatic metastases with vertebral pathological fractures. Liver biopsy confirmed a metastatic neuroendocrine tumor of intermediate grade, with immunohistochemistry suggesting a possible pancreatic origin; however, the primary tumor remained occult, with no pancreatic lesion identified on imaging. Management included treatment of diabetes and hypertension, ketoconazole and osilodrostat for hypercortisolism, and supportive care for vertebral fractures, resulting in partial clinical improvement. This case highlights the aggressive presentation and diagnostic challenges of ectopic ACTH syndrome, particularly in low-resource settings, and underscores the importance of a multidisciplinary approach.
Keywords: hypercortisolism, ectopic ACTH syndrome, neuroendocrine tumor, occult primary tumor, vertebral fractures
Introduction
Cushing syndrome is a clinical disorder resulting from prolonged exposure to excessive levels of glucocorticoids. It may arise from exogenous corticosteroid use or endogenous overproduction.1,2 Endogenous Cushing syndrome is broadly classified into adrenocorticotropic hormone (ACTH)-dependent and ACTH-independent causes, with ACTH-dependent forms accounting for approximately 80–85% of cases.3 Among these, pituitary corticotroph adenomas (Cushing disease) represent the most common etiology, whereas ectopic ACTH secretion constitutes a smaller but clinically significant subset.4
Ectopic ACTH syndrome is characterized by non-pituitary tumors producing ACTH, leading to excessive cortisol secretion and hypercortisolism. It accounts for approximately 10–20% of endogenous Cushing syndrome cases and is frequently associated with neuroendocrine tumors.5 These tumors may arise from various anatomical sites, including the lungs, pancreas, thymus, and gastrointestinal tract, and in some cases remain occult despite extensive diagnostic evaluation, posing a significant clinical challenge.6
Neuroendocrine tumors are a heterogeneous group of neoplasms capable of secreting biologically active peptides and hormones. While many are indolent, some exhibit aggressive behavior with early metastasis and systemic manifestations due to hormone overproduction.7 Ectopic ACTH production by neuroendocrine tumors often results in severe, rapidly progressive Cushing syndrome with metabolic complications such as hypokalemia, metabolic alkalosis, hypertension, and diabetes mellitus.8,9
The diagnosis of ectopic ACTH syndrome requires biochemical confirmation of hypercortisolism, determination of ACTH dependency, and localization of the source. Imaging modalities such as computed tomography (CT), magnetic resonance imaging (MRI), and functional imaging are essential, although identifying the primary tumor may be difficult, particularly in occult cases.5 Histopathological and immunohistochemical analysis can confirm the neuroendocrine nature of the tumor but may not reliably identify the primary site in metastatic disease.10
Skeletal complications, including osteoporosis and pathological fractures, are well-recognized consequences of hypercortisolism. However, vertebral fractures as an initial presenting feature are rarely reported, especially in the presence of an occult primary tumor with widespread metastases.11,12
Herein, we report a rare case of ectopic ACTH–dependent Cushing syndrome secondary to a metastatic neuroendocrine tumor of unknown primary origin, presenting with severe hypercortisolism, widespread metastases, and early vertebral pathological fractures in a young woman. This case highlights the diagnostic and management challenges in low-resource settings and underscores the importance of a multidisciplinary approach.
Case Presentation
On 7 February 2026, a 30-year-old woman from Baghlan Province, Afghanistan, presented to the emergency department of Ali Abad Teaching Hospital, Kabul, with progressive lower limb weakness and difficulty walking for the past two weeks. She also reported generalized body pain, nausea, vomiting, abdominal pain, and generalized weakness for the past month, along with headache for the past four months. The patient had documented polydipsia and polyuria. She had been diagnosed with hypertension and diabetes mellitus approximately four months prior to presentation.
On admission, her vital signs revealed a blood pressure of 160/110 mmHg, pulse rate of 80 beats per minute, respiratory rate of 18 breaths per minute, and oxygen saturation of 95% on room air. Physical examination revealed clinical features suggestive of Cushing syndrome, including hirsutism, abdominal striae, facial rounding (moon facies), and skin hyperpigmentation. Neurological examination revealed reduced deep tendon reflexes in the lower extremities.
Serum electrolyte analysis demonstrated marked hypernatremia (serum sodium: 162 mmol/L; reference range: 135–145 mmol/L), severe hypokalemia (serum potassium: 2.1 mmol/L; reference range: 3.5–5.0 mmol/L), hyperchloremia (serum chloride: 125 mmol/L; reference range: 98–107 mmol/L), and a slight decrease in ionized serum calcium (1.12 mmol/L; reference range 1.13–1.32 mmol/L). Given these significant electrolyte abnormalities, the patient was admitted to the intensive care unit, where appropriate management was initiated. Laboratory investigations revealed hyperglycemia, with a random blood glucose level of 326 mg/dL (reference range: 70–140 mg/dL). Arterial blood gas analysis revealed alkalemia, with a pH of 7.65 (reference range: 7.35–7.45) and markedly elevated bicarbonate of 41.1 mmol/L (reference range: 22–26 mmol/L), consistent with metabolic alkalosis. Additional laboratory results are summarized in Table 1.
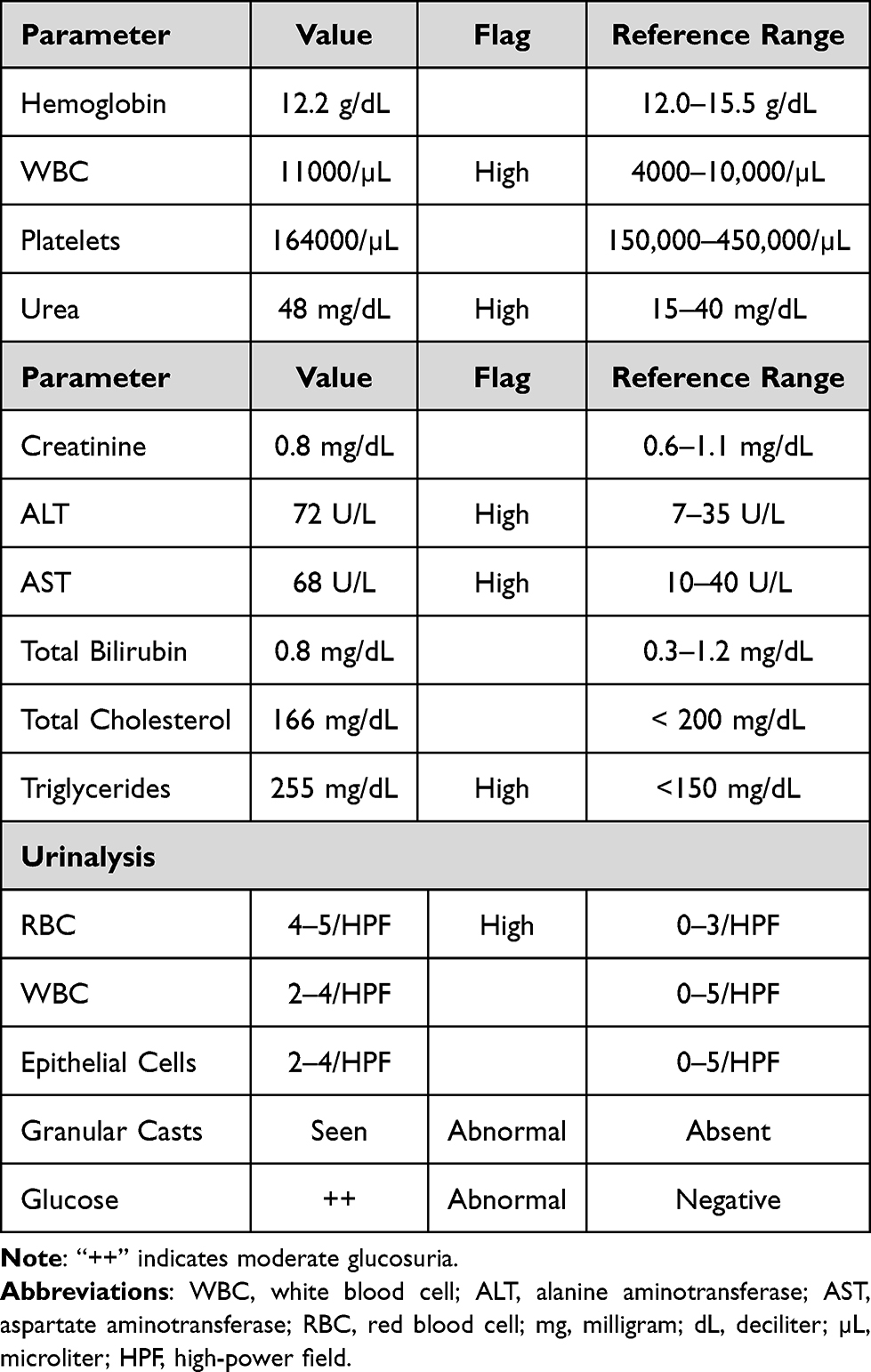 |
Table 1 Laboratory Findings of the Patient at Presentation |
Hormonal evaluation demonstrated markedly elevated morning serum cortisol levels of 91.9 µg/dL (reference range: 4.2–38.4 µg/dL). After two days of dexamethasone administration (0.5 mg every 6 hours), 24-hour urinary free cortisol remained markedly elevated at 27,971 µg/24 hours (reference range: 30–350 µg/24 hours), indicating lack of suppression consistent with Cushing syndrome. Serum adrenocorticotropic hormone (ACTH) was elevated (141.92 pg/mL; reference range: 6–48 pg/mL) and was inappropriately non-suppressed in the setting of marked hypercortisolism, consistent with ACTH-dependent Cushing syndrome. Thyroid function tests, including triiodothyronine (T3), thyroxine (T4), and thyroid-stimulating hormone (TSH), were within normal limits.
Magnetic resonance imaging (MRI) of the brain revealed no significant abnormalities in the cranial fossa, with no evidence of a pituitary adenoma; incidental findings included chronic bilateral maxillary and ethmoid sinusitis (Figure 1).
 |
Figure 1 Sagittal magnetic resonance imaging (MRI) of the brain demonstrating no evidence of a pituitary mass or intracranial lesion. |
Contrast-enhanced computed tomography (CT) of the abdomen revealed multiple (at least eight) well-defined solid masses within the liver, the largest measuring approximately 10×5.9×8.3 cm, consistent with hepatic metastasis. The remainder of the abdominal scan was unremarkable, with normal adrenal glands and pancreas and no identifiable primary lesion. Compression fractures were noted in the T12 and L3 vertebral bodies (Figure 2).
 |
Figure 2 Contrast-enhanced computed tomography (CT) of the abdomen showing hepatic metastasis (arrow). |
Magnetic resonance imaging (MRI) of the spine confirmed vertebral pathological fractures and demonstrated an anterior wedge fracture of the T12 vertebra and a central wedge fracture of the L3 vertebra, both associated with marrow edema. A subtle posterior disc bulge at the L4–L5 level causing thecal sac indentation was also noted (Figure 3).
 |
Figure 3 Sagittal magnetic resonance imaging (MRI) of the dorso-lumbar spine demonstrating anterior wedge fracture of the T12 vertebra and central wedge fracture of the L3 vertebra (arrows). |
In view of the vertebral fractures, an orthopedic consultation was obtained. The patient was managed conservatively, with advice for external spinal support using a brace (belt) and analgesia with meloxicam and gabapentin, with no indication for surgical intervention.
Contrast-enhanced CT of the chest reported a 10 mm pleural-based soft tissue attenuation nodule with lobulated margins in the anterior segment of the right upper lobe, suspicious for metastatic involvement. Associated findings included collapse-consolidation in the anterior basal segment of the right lower lobe and mild bilateral pleural effusions.
An ultrasound-guided liver biopsy was performed. Histopathological examination reported a “poorly differentiated malignant neoplasm, either primary or metastatic.” Serum alpha-fetoprotein level was within normal limits at 9.45 ng/mL (reference range: 0–10 ng/mL), making hepatocellular carcinoma less likely. Histopathological evaluation of the liver core needle biopsy, based on hematoxylin and eosin (H&E) staining and immunohistochemistry (IHC), demonstrated findings consistent with a metastatic neuroendocrine tumor, with a probable pancreatic origin (Figure 4). However, contrast-enhanced computed tomography (CT) of the abdomen showed a normal pancreas, with no identifiable primary lesion.
 |
Figure 4 Histopathological examination of liver core biopsy. Combined Hematoxylin and Eosin-stained sections and immunohistochemical findings are consistent with metastatic neuroendocrine tumor, favoring a pancreatic primary. (A) Low-power overview of the biopsy core. (B) Tumor infiltration of hepatic parenchyma. (C) Sheets of neoplastic cells within the liver tissue. (D) High-power view showing pleomorphic polygonal to spindle-shaped tumor cells with eosinophilic cytoplasm, hyperchromatic nuclei, and prominent nucleoli. |
Immunohistochemical analysis demonstrated tumor cells positive for cytokeratin (AE1/AE3), synaptophysin, and CD56, supporting neuroendocrine differentiation, with p63 showing focal positivity. The tumor cells were negative for TTF-1, CDX2, PAX8, GATA3, CK20, CK19, Glypican-3, S-100, and Mammaglobin, making common primary sites such as lung, gastrointestinal tract, kidney, breast, and hepatocellular origin less likely. The Ki-67 proliferation index was approximately 10%, consistent with an intermediate-grade (G2) neuroendocrine tumor.
Localization of the primary tumor was limited by the unavailability of advanced functional imaging. In particular, Gallium-68 DOTATATE PET/CT, which is considered a highly sensitive modality for detecting Neuroendocrine tumors, was not available in the country and therefore could not be performed.
Overall, the clinical, biochemical, radiological, and histopathological findings were consistent with severe ectopic ACTH–dependent Cushing syndrome secondary to a metastatic Neuroendocrine tumor.
The patient was managed with a combination of electrolyte correction, antihypertensive therapy, glycemic control, and supportive care. Potassium replacement was administered intravenously with potassium chloride. Blood pressure was controlled with spironolactone (200 mg/day). In view of hypercortisolism, ketoconazole (400 mg/day) and osilodrostat (5 mg/day) therapy was initiated. For glycemic management, metformin and sitagliptin were prescribed, with adjustments made based on blood glucose monitoring. Gastroprotection was provided with pantoprazole. An oncology consultation was obtained, and a chemotherapy regimen consisting of cisplatin and etoposide administered on days 1 through 3 of a 21-day cycle, for a total of six cycles, was recommended.
The patient remained hospitalized for 25 days, during which she received supportive and medical management, and was subsequently discharged in a relatively improved clinical condition. One month after discharge, at the time of the initial preparation of this report, her condition remained stable without significant deterioration. At the time of this revised report, the patient was still alive, remained compliant with her prescribed medications, and was regularly attending the oncology department to receive her chemotherapy regimen. However, despite ongoing treatment, her general clinical condition had gradually worsened in the setting of advanced metastatic disease.
Discussion
Ectopic ACTH syndrome caused by a neuroendocrine tumor of occult primary origin is an uncommon condition and poses significant diagnostic and therapeutic challenges. Ectopic ACTH secretion accounts for a minority of ACTH-dependent Cushing syndrome cases, with neuroendocrine tumors being a major cause; however, identification of the primary tumor remains elusive in some patients despite extensive evaluation.6 The coexistence of an occult primary tumor with pulmonary and hepatic metastases and vertebral pathological fractures at presentation, as observed in this case, represents a rare and complex clinical scenario. Compared to previously reported cases, our patient demonstrated extreme hypercortisolism with life-threatening metabolic derangements, indicating a more aggressive hormonal phenotype.13
A key challenge in ACTH-dependent Cushing syndrome is distinguishing pituitary from ectopic sources and localizing the tumor. Although pituitary MRI was unremarkable, this does not exclude Cushing disease. Both etiologies are associated with inappropriately elevated ACTH levels in the presence of hypercortisolism; however, ectopic ACTH syndrome typically follows a more aggressive course, with markedly elevated cortisol levels and severe metabolic derangements.14 In this case, profound hypercortisolism, severe hypokalemia, metabolic alkalosis, hyperglycemia, and hypertension, together with metastatic disease and a negative pituitary MRI, strongly supported an ectopic source. Inferior petrosal sinus sampling, the gold standard for differentiation, was not performed due to resource limitations.15
The biochemical abnormalities observed are consistent with the pathophysiology of severe hypercortisolism. Excess cortisol overwhelms 11β-hydroxysteroid dehydrogenase type 2, allowing activation of mineralocorticoid receptors and resulting in hypokalemia and metabolic alkalosis.16 These features are particularly prominent in ectopic ACTH syndrome and may aid in distinguishing it from pituitary disease.9
Imaging demonstrated multiple hepatic lesions and a pulmonary nodule suggestive of metastatic disease; however, the primary tumor could not be identified, highlighting the challenge of occult ectopic ACTH-secreting tumors. Functional imaging, such as Gallium-68 DOTATATE positron emission tomography, has high sensitivity but was unavailable in this setting, underscoring diagnostic limitations in resource-constrained environments.17
Histopathological and immunohistochemical evaluation confirmed a metastatic neuroendocrine tumor of intermediate grade. While neuroendocrine differentiation was established, only a possible pancreatic origin was suggested, with no identifiable primary lesion on imaging. This reflects a known limitation of histopathology in metastatic neuroendocrine tumors, where the primary site may remain uncertain.18
A notable feature of this case is the presence of widespread metastases at initial presentation. Although many neuroendocrine tumors are indolent, some exhibit aggressive progression with early dissemination.7 The coexistence of an occult primary tumor and extensive metastases complicates both diagnosis and management.
Skeletal complications are well-recognized consequences of hypercortisolism, resulting in osteoporosis and fractures. Although vertebral compression fractures are described in Cushing syndrome, they are less commonly the presenting feature.11,12 Vertebral fractures were a key component of this patient’s presentation, highlighting the need to consider both endocrine and malignant causes in cases of unexplained pathological fractures with metabolic abnormalities. Unlike prior reports, our case presented with early vertebral fractures as a major initial manifestation, reflecting severe skeletal involvement from hypercortisolism.13
Management of ectopic ACTH syndrome requires a multidisciplinary approach focused on rapid control of hypercortisolism, treatment of the underlying malignancy, and management of complications.19 In this patient, ketoconazole and osilodrostat were initiated alongside supportive measures. Given metastatic disease and the absence of a localized primary tumor, curative surgery was not feasible. Management was further complicated by resource limitations within our setting. In severe cases, additional options such as intravenous etomidate or bilateral adrenalectomy may be considered, although not pursued here.20 Supportive management of vertebral fractures was also essential in improving functional status.
The prognosis of Ectopic ACTH syndrome associated with metastatic disease is generally poor and is largely determined by tumor burden and complications of severe hypercortisolism, including infections, sepsis, thromboembolic events, and metabolic disturbances.21
This case highlights several important clinical lessons. Vertebral fractures may serve as an initial manifestation and should prompt evaluation for underlying endocrine and malignant etiologies. Although histopathology is crucial for confirming neuroendocrine differentiation, it may not reliably establish the primary site, necessitating a multimodal diagnostic approach. These diagnostic challenges are particularly pronounced in resource-limited settings, underscoring the need for coordinated multidisciplinary care.
Conclusion
Severe ectopic ACTH syndrome due to a neuroendocrine tumor of unknown primary origin is a rare condition, particularly when presenting with widespread metastases and atypical manifestations such as vertebral fractures. This case emphasizes the importance of recognizing severe hypercortisolism and its associated metabolic complications. Early multidisciplinary management is essential, although the prognosis remains poor in advanced disease.
AI Statement
ChatGPT (OpenAI, GPT-5 mini) was used solely for language editing and improvement of clarity in this manuscript.
Ethical Statement
This report was approved by the ethics committee of the Department of Internal Medicine, Kabul University of Medical Sciences, under protocol number 95-2026. Written informed consent was obtained from the patient for participation and for publication of this case report.
Acknowledgment
We sincerely acknowledge the Department of Histopathology at the French Medical Institute for Mothers and Children (FMIC) for providing the histopathological images included in this report.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. John TA, Anastasopoulou C. Hypercortisolism (Cushing Syndrome). In: StatPearls. StatPearls Publishing; 2025:2–9.
2. Sharma ST, Nieman LK. Cushing’s Syndrome: all variants, detection, and treatment. Endocrinol Metab Clin North Am. 2011;1109(8):1–13.
3. Sharma ST, Nieman LK, Feelders RA. Cushing’s syndrome: epidemiology and developments in disease management. Clin Epidemiol. 2015;7:281–293. doi:10.2147/CLEP.S44336
4. Pokrzywa A, Pachucki J. Case Report: ectopic CRH production by adrenal adenoma as a unique cause of the ACTH-dependent Cushing’s syndrome. Front Endocrinol. 2025;1–9.
5. Paleń-Tytko JE, Przybylik-Mazurek EM, Rzepka EJ, et al. Ectopic ACTH syndrome of different origin — diagnostic approach and clinical outcome. Experience of one Clinical Centre. PLoS One. 2020;1–19.
6. Venugopal H, Griffin K, Amer S. A case of severe ectopic ACTH syndrome from an occult primary – diagnostic and management dilemmas. Endocrinol Diabetes Metab. 2015.
7. Oronsky B, Ma PC, Morgensztern D, Carter CA. Nothing But NET: a review of neuroendocrine tumors and carcinomas. Neoplasia. 2017;19(12):991–1002. doi:10.1016/j.neo.2017.09.002
8. Doi M, Sugiyama T, Izumiyama H, Yoshimoto T, Hirata Y. Clinical features and management of ectopic ACTH syndrome at a single institute in Japan. Endocr J. 2010;57(12):1061–1069. doi:10.1507/endocrj.K10E-265
9. Torun C, Eken E, Cakır B, Uzunlulu M. Hypokalemic metabolic alkalosis as a clinical clue to ectopic ACTH syndrome: two cases of neuroendocrine carcinoma. Endocr Regul. 2025;59:265–270. doi:10.2478/enr-2025-0031
10. Juhlin CC, Zedenius J, Höög A. Metastatic neuroendocrine neoplasms of unknown primary: clues from pathology workup. Cancers. 2022;15:1–15. doi:10.3390/cancers15010001
11. Briot K, Roux C. Glucocorticoid-induced osteoporosis. Rheum Musculoskelet Dis. 2015.
12. Leszczyńska D, Szatko A, Papierska L, Zgliczyński W, Glinicki P. Musculoskeletal complications of Cushing syndrome. Reumatologia. 2023;61:271–282. doi:10.5114/reum/169889
13. Bostan H, Duger H, Akhanli P, Calapkulu M, Taskin T. Cushing’s syndrome due to adrenocorticotropic hormone ‑ secreting metastatic neuroendocrine tumor of unknown primary origin: a case report and literature review. Hormones. 2022;21:147–154. doi:10.1007/s42000-021-00316-z
14. Hayes AR, Grossman AB. Distinguishing Cushing’s disease from the ectopic ACTH syndrome: needles in a haystack or hiding in plain sight? J Neuroendocrinol. 2022:1–8.
15. Valizadeh M, Abiri B, Hosseinpanah F, Grossman A. Bilateral inferior petrosal sinus sampling in the differential diagnosis of ACTH-dependent Cushing’s syndrome: a reappraisal. J Intern Med. 2024;296(1):2–23. doi:10.1111/joim.13789
16. Alsaadoun SA, Alrasheedi AT, Gazar SH, Alsallum GA. Apparent mineralocorticoid excess syndrome: case report. Int Med Case Rep J. 2025;671–676.
17. Tirosh A, Kebebew E. The utility of 68 Ga-DOTATATE positron-emission tomography/computed tomography in the diagnosis, management, follow-up and prognosis of neuroendocrine tumors. Futur Oncol. 2018;14:111–122. doi:10.2217/fon-2017-0393
18. Schmidt M, Hinterleitner C, Singer S, Lauer UM, Zender L, Hinterleitner M. Diagnostic approaches for Neuroendocrine Neoplasms of Unknown Primary (Nen-UPs) and their prognostic relevance-a retrospective, long-term single-center experience. Cancers. 2023;15(17):4316. doi:10.3390/cancers15174316
19. Fernández LG, Maricel A, Montenegro R, et al. Ectopic Cushing’s syndrome: clinical, diagnostic, treatment and follow-up outcomes of 12 cases of lung ectopic ACTH. Endocrinol Diabetes Metab Case Rep. 2023;2023(3).
20. Carroll TB, Peppard WJ, Herrmann DJ, et al. Continuous etomidate infusion for the management of severe cushing syndrome: validation of a standard protocol. J Endocr Soc. 2019;3:1–12. doi:10.1210/js.2018-00269
21. Piasecka M, Papakokkinou E, Ragnarsson O, Piasecki A, Falhammar H. Survival probabilities in patients with ectopic Cushing’s syndrome — a systematic review and a single-arm meta-analysis. Eur J Endocrinol. 2025;192(6):53–65. doi:10.1093/ejendo/lvaf114
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.