Back to Journals » Journal of Asthma and Allergy » Volume 14
Serum YKL-40 Levels Predict Endotypes and Associate with Postoperative Recurrence in Patients with Chronic Rhinosinusitis with Nasal Polyps
Authors Wen S, Cheng S ![]() , Xie S, Zhang H, Xie Z, Jiang W
, Xie S, Zhang H, Xie Z, Jiang W ![]()
Received 30 August 2021
Accepted for publication 8 October 2021
Published 29 October 2021 Volume 2021:14 Pages 1295—1306
DOI https://doi.org/10.2147/JAA.S335964
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Luis Garcia-Marcos
Sihui Wen,* Shenghao Cheng,* Shaobing Xie, Hua Zhang, Zhihai Xie, Weihong Jiang
Department of Otolaryngology Head and Neck Surgery, Xiangya Hospital of Central South University & Hunan Province Key Laboratory of Otolaryngology Critical Diseases, Changsha, Hunan, 410008, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhihai Xie; Weihong Jiang
Department of Otolaryngology Head and Neck Surgery, Xiangya Hospital of Central South University & Hunan Province Key Laboratory of Otolaryngology Critical Diseases, Changsha, Hunan, 410008, People’s Republic of China
Email [email protected]; [email protected]
Background: Chronic rhinosinusitis with nasal polyps (CRSwNP) is a global health concern with high heterogeneity and rate of postoperative recidivation. YKL-40 is a pivotal pro-inflammatory mediator to promote Th2 immune response which is involved in many inflammatory diseases. This study aimed to investigate the predictive value of serum YKL-40 in CRSwNP endotypes and postoperative recurrence.
Methods: We recruited 80 primary CRSwNP, 40 recurrent CRSwNP patients and 40 healthy controls (HCs) in this study, and the serum and tissue specimens were collected. The middle turbinate mucosa tissue collected from patients undergoing septoplasty was used as control. Serum YKL-40 concentrations were detected by enzyme-linked immunosorbent assay (ELISA), and tissue YKL-40 mRNA and protein levels were examined using quantitative real-time polymerase chain reaction (qRT-PCR) and immunohistochemistry (IHC). The difference of YKL-40 expression was compared among different group. Multivariate analysis and receiver operating characteristic (ROC) curve were performed to evaluate the value of serum YKL-40 in discriminating eosinophilic CRSwNP (eCRSwNP) and predicting postoperative recurrence.
Results: The serum YKL-40 levels in CRSwNP patients were higher than HCs, especially in eCRSwNP patients (p < 0.05). The elevated YKL-40 levels positively correlated with blood eosinophil percentage, tissue eosinophil counts and percentages (p < 0.05). The serum YKL-40 levels in recurrent CRSwNP patients were markedly enhanced than primary CRSwNP patients (p < 0.05). The YKL-40 mRNA and protein levels were significantly elevated in CRSwNP patients compared to HCs, especially in eCRSwNP and recurrent CRSwNP group. Multivariate analysis and ROC curve exhibited that serum YKL-40 might be a promising indicator in distinguishing CRSwNP endotypes and predicting postoperative recurrence.
Conclusion: Our data suggested that YKL-40 might be unregulated in CRSwNP and associated with mucosal eosinophilia and recurrence. Serum YKL-40 appeared to a novel biomarker for predicting CRSwNP endotypes and postoperative recurrence of CRSwNP.
Keywords: YKL-40, chronic rhinosinusitis with nasal polyps, endotypes, recurrence
Introduction
Chronic rhinosinusitis (CRS) is a common chronic inflammatory disease of the upper airway, which affects about 15% of the adult population worldwide.1 Depending on the presence of polyp, CRS is divided into two subgroups: chronic rhinosinusitis with nasal polyps (CRSwNP) and chronic rhinosinusitis without nasal polyps (CRSsNP). Prior publications demonstrated that T helper 2 (Th2)-driven inflammation was predominant in the underlying pathomechanism of CRSwNP, while T helper 1 (Th1)-driven inflammation was precipitated in CRSsNP.2–4 CRSwNP can be further classified into eosinophilic (eCRSwNP) and non-eosinophilic (neCRSwNP) based on the degree of infiltration of eosinophils in nasal mucosa.1,5 Currently, most scholars considered that the tissue eosinophils percentage >10% of total inflammatory cells was regarded as eCRSwNP, otherwise defined as neCRSwNP.6,7 These two endotypes exhibited significant differences in clinical characteristics, disease symptoms, prognosis and postoperative recurrence rate. Given that, preoperatively distinguishing eCRSwNP from CRSwNP and predicting postoperative recurrence were essential to develop personalized treatments and improve follow-up protocols. It is urgent to find objective indicators or biomarkers that can be used for differentiating eCRSwNP from neCRSwNP and predicting for postoperative recurrence of CRSwNP before operation, which can provide optimal treatment strategies and improve the prognosis.
YKL-40, also known as human chitinase-3 like-1, belongs to a protein family containing an amino acid sequence that is similar to the 18-glycosyl hydrolase of bacterial chitinases.8 YKL-40 is secreted by a variety of inflammatory cells, such as macrophages, vascular smooth muscle cells, neutrophils,9 and it has been demonstrated to be involved in many inflammatory diseases, including chronic obstructive pulmonary disease (COPD),10 lung fibrosis,11 asthma12 and COVID infection.13 Recently, YKL-40 has been proved to be up-regulated in the nasal mucosa of moderate/severe persistent allergic rhinitis, associated with the remodeling of nasal mucosa.12 Moreover, Ma et al’s study found that the expression of YKL-40 in patients with CRSwNP was higher than those in healthy control and CRSsNP patients.14 Thus, we assumed that YKL-40 might play a vital role in the occurrence and development of CRSwNP and contribute to discriminating eCRSwNP from neCRSwNP, and predicting the postoperative recurrence.
In this study, we aim to explore the change of serum YKL-40 concentrations in primary CRSwNP and recurrent CRSwNP in comparison with healthy controls (HCs), and assess its predictive potential in distinguishing CRSwNP endotypes and predicting postoperative recurrence.
Materials and Methods
Participants and Settings
In the present study, 40 healthy controls and 120 CRSwNP patients including 80 primary (43 neCRSwNP and 37 eCRSwNP) and 40 recurrent patients were recruited between July 2019 and December 2019 in our department. All participants met the diagnostic criteria of CRSwNP according to the guidelines of the European Position Paper on Rhinosinusitis and Nasal Polyps 2012.15 Exclusion criteria for the study group included the following: 1) age <18 or >80 years; 2) patients with other nasal or sinus diseases, such as fungal sinusitis, allergic fungal rhinosinusitis, cystic fibrosis and malignancy; 3) patients with a diagnosis of inflammatory diseases, autoimmune diseases; 4) treated with immunotherapy, antibiotics, nasal or systemic corticosteroids, or anti-allergic drugs within 4 weeks before the surgery; 5) severe heart and kidney dysfunction; 6) aspirin intolerance and 7) pregnant condition. The diagnosis of recurrent CRSwNP was made when patients met both of two criteria: 1) presence of nasal polyps detected by nasal endoscopy and/or computed tomography (CT); 2) symptoms lasting for more than 1 week despite treating with normative intranasal corticosteroid.16 Forty age- and gender-matched HCs who undergoing septoplasty with no evidence of rhinitis or rhinosinusitis, diabetes mellitus, severe heart and kidney dysfunction, or inflammatory or autoimmune conditions were included as control group, and their middle turbinate mucosa tissues were collected and used as control. All subjects, except for the healthy controls, underwent routine preoperative examination, blood tests, nasal endoscopy, chest X-rays, electrocardiography and high-resolution computed tomography (HRCT) or magnetic resonance imaging (MRI). All CRSwNP patients scored their nasal symptoms using the widely accepted visual analogue scale (VAS) as previously described.17 Lund–Mackay scoring system was used for preoperative CT assessments.18
Diagnosis of eCRSwNP and neCRSwNP
The nasal polyps were obtained from patients with CRSwNP during the operation, then soaked in 10% formalin and embedded in paraffin. The embedded tissues were sectioned into 5-μm sections by microtome and stained with hematoxylin and eosin (H&E). Two independent observers who were blinded to the clinical data counted the numbers of eosinophils, lymphocytes, neutrophils and plasma cells in 10 randomly selected high-power fields (HPFs). eCRSwNP was diagnosed when the percentage of tissue eosinophils was higher than 10% of the total inflammatory cells, otherwise neCRSswNP was defined.7
Sample Collection and YKL-40 Levels Measurement
Five milliliter fresh venous blood was collected from all subjects and stored at room temperature for 1 hour. Then, the blood samples were centrifuged at 3000 g at 4° C for 10 minutes. The supernatants were collected and stored at −80 °C for subsequent experiments. Serum samples were thawed and centrifuged before use. Serum YKL-40 levels were detected by ELISA kit commercial (Multisciences, Hangzhou, China) according to the manufacturer’s instructions. All samples performed in duplicate to improve assay precision.
qRT-PCR Analysis
To further verify YKL-40 expression in tissue, we obtained 40 CRSwNP tissue specimens, including 20 primary nasal polyps and 20 recurrent nasal polyps from the middle meatus, and 40 middle turbinate mucosa samples from patients undergoing nasal septal surgery or cerebrospinal rhinorrhea surgery which were used as controls. Because the nasal polyps tissue originated from the middle meatus, which was anatomically adjacent to the middle turbinate, we collected middle turbinate mucosa as control. Tissue RNA was extracted with Trizol reagent (Thermo Fisher Scientific, Shanghai, China), and the RNA concentration was measured by Nanodrop 2000c (Thermo Fisher Scientific, Shanghai, China). RNA was reverse transcribed into cDNA using SureScript First-Strand cDNA Synthesis Kit (US EVERBRIGHT, Suzhou, China), according to the manufacturer’s instructions. qRT-PCR was performed using 100ng of cDNA with the SYBR Green qPCR Supermix (US EVERBRIGHT, Suzhou, China) to monitor DNA synthesis using specific primers. The primers used were shown in Table S1.
IHC of YKL-40
IHC was performed as previously described.19 Sections were incubated overnight at 4°C with primary antibody against YKL-40 with a dilution of 1:200 (Affinity Biosciences, Changzhou, Jiangsu, China). Each section was incubated with a secondary antibody and then with horseradish peroxidase-labeled streptavidin complex (Zhongshan-Jinqiao, Beijing, China). The distribution of peroxidase is revealed by incubating in a solution containing 3% 3,3-diaminophetamine tetrachloride, which is then dyed back and covered with sulphide. During these processes, endogenous peroxidase was blocked with 0.3% hydrogen peroxide. Two representative images were selected in each group and showed at 200× and 400× magnification.
Statistical Analysis
Continuous variables with normal distribution were described as mean ± standard deviation (SD). For normally distributed variables, one-way analysis of variance (ANOVA) or Student’s t-test was applied. On the contrary, Kruskal–Wallis H-test or Mann–Whitney U-test was used. To evaluate the correlation between serum YKL-40 levels and clinical variables, Spearman correlation test was conducted. Logistic regression analysis and receiver operating characteristic (ROC) curves were performed to determine the predictive value of serum YKL-40 and other indicators. All statistical analyses were conducted on SPSS statistics software version 19.0 (IBM, Chicago, IL, USA), and figures were constructed in GraphPad Prism 7.0 (Software Inc. La Jolla, CA, USA). For all tests, P < 0.05 was considered statistically significant.
Results
Demographic and Clinical Characteristics of Participants
Among 80 primary CRSwNP patients, 43 (53.8%) patients were categorized into neCRSwNP group, and 37 (46.2%) patients were classified into eCRSwNP group. Demographic and clinical characteristics of all participants are shown in Table 1. Significant differences were observed in the rate of allergic rhinitis, blood eosinophil counts and percentages among three groups (p < 0.001). No statistical difference was observed in age, gender, rate of smoking, drinking, BMI among three groups, and preoperative VAS score and Lund–Mackay score between eCRSwNP group and neCRSwNP group. Typical histological figures of neCRSwNP and eCRSwNP are listed in Figure 1A and B, the eosinophils counts and percentages were significantly higher in eCRSwNP patients than neCRSwNP (all p < 0.001, Figure 1C and D).
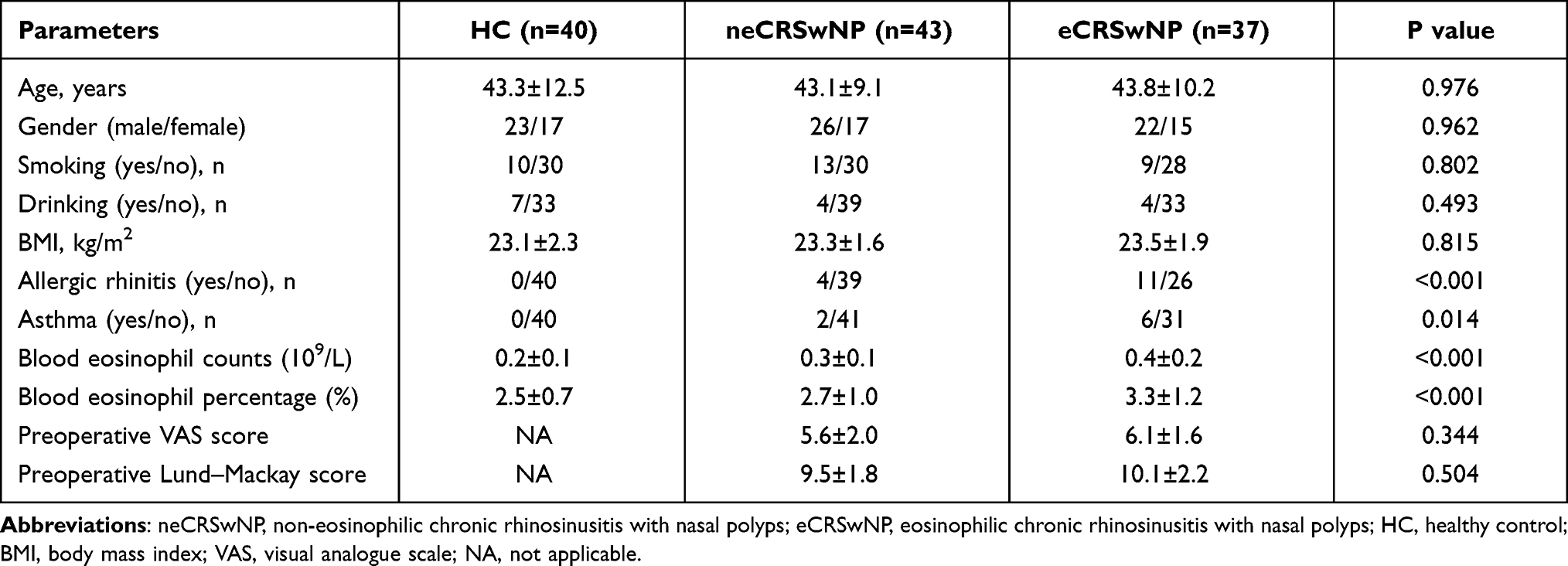 |
Table 1 The Demographic and Clinical Characteristics of Subjects |
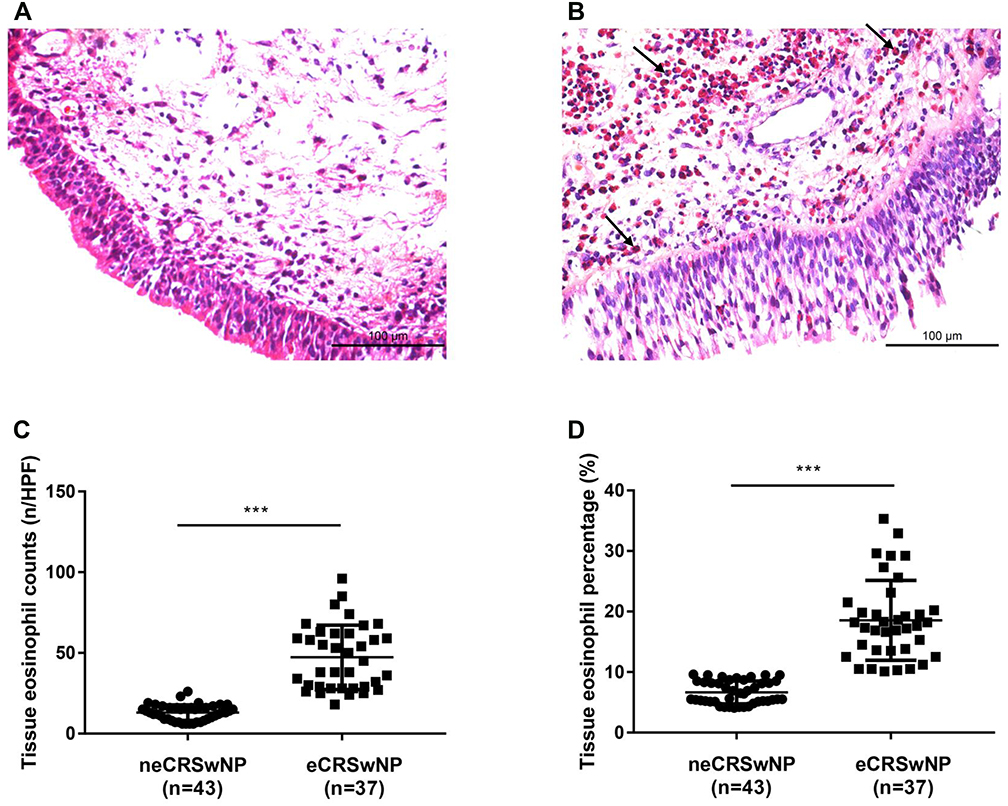 |
Figure 1 CRSwNP tissue specimens H&E staining and tissue eosinophil counts in HPF. (A and B) Typical histological figures of neCRSwNP and eCRSwNP. (C and D) The eosinophils counts and percentages were significantly higher in eCRSwNP patients than neCRSwNP. ***p < 0.001. Abbreviations: eCRSwNP, eosinophilic chronic rhinosinusitis with nasal polyps; neCRSwNP, non-eosinophilic chronic rhinosinusitis with nasal polyps; HPF, high-power field. Notes: All CRSwNP tissue specimens from nasal polyp tissue of undergoing functional endoscopic sinus surgery. Arrows point to eosinophils in the image. |
YKL-40 Levels in CRSwNP Patients and Its Predictive Value in CRSwNP Endotypes
As shown in Figure 2, the serum YKL-40 levels were markedly increased in eCRSwNP and neCRSwNP groups in comparison with control group, and the YKL-40 levels were higher in eCRSwNP groups than neCRSwNP groups. Moreover, the elevated serum YKL-40 concentrations positively correlated with blood eosinophil percentages (r = 0.221, p = 0.048), tissue eosinophil counts (r = 0.423, p = 0.005), tissue eosinophil percentages (r = 0.686, p < 0.001) (Table 2). Logistic regression analysis results revealed that serum levels of YKL-40 (OR = 3.019, p = 0.008), blood eosinophil percentages (OR = 2.537, p = 0.004) and counts (OR = 2.134, p = 0.030), and comorbid allergic rhinitis (OR = 1.532, p = 0.026) associated with CRSwNP endotypes (Table 3). To further verify accuracy and predictive values of the serum YKL-40 levels, ROC curve analysis was applied. ROC curves (Figure 3) and their parameters (Table 4) indicated that serum YKL-40 exhibited potential predictive ability in CRSwNP endotypes.
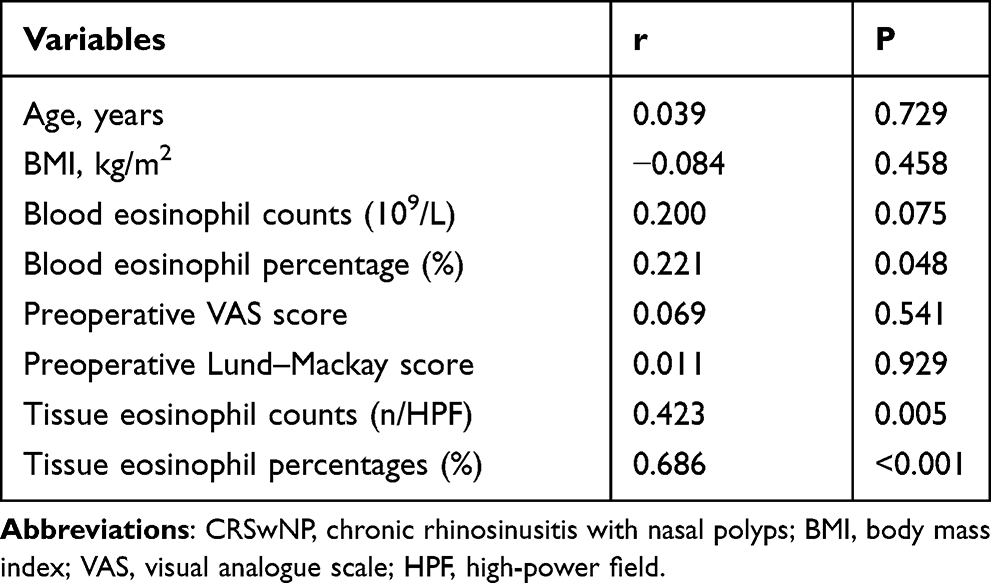 |
Table 2 Correlation Between Serum YKL-40 and Clinical Variables in CRSwNP Patients |
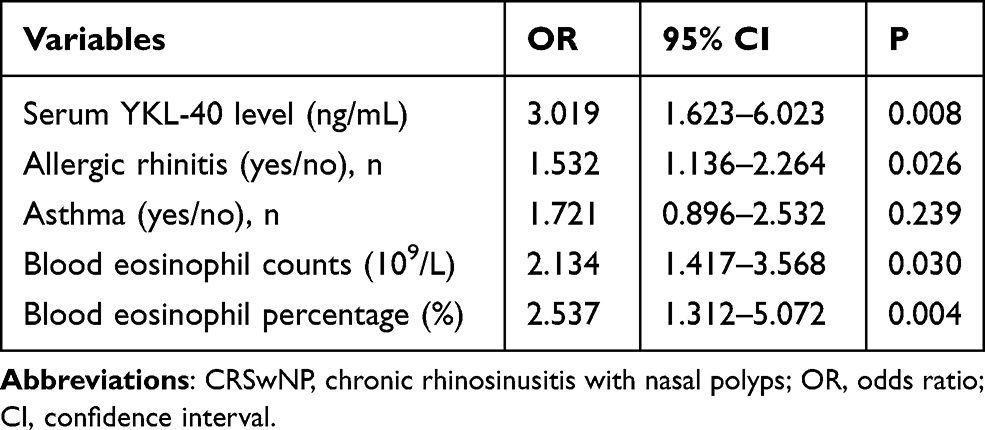 |
Table 3 Logistic Regression Analysis of Factors Associated with CRSwNP Phenotypes |
 |
Table 4 ROC Analysis Results of Different Variables for Distinguishing CRSwNP Phenotypes |
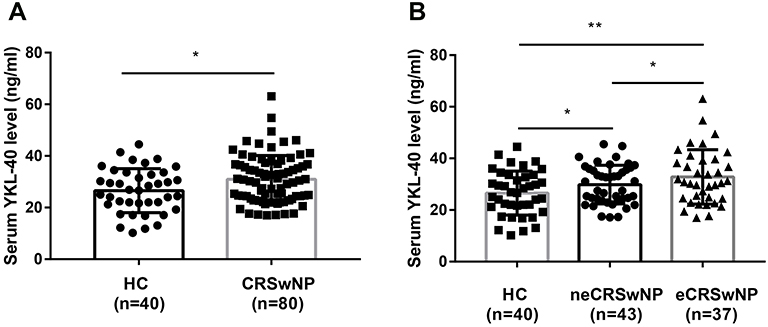 |
Figure 2 Comparison of serum YKL-40 level between HC and CRSwNP. (A) Serum YKL-40 levels were elevated in the CRSwNP than HC. (B) Serum YKL-40 levels were significantly increased in the eCRSwNP than HC and neCRSwNP. *p < 0.05; **p < 0.01. Abbreviations: HC, health control; CRSwNP, chronic rhinosinusitis with nasal polyps; eCRSwNP, eosinophilic chronic rhinosinusitis with nasal polyps; neCRSwNP, non-eosinophilic chronic rhinosinusitis with nasal polyps. |
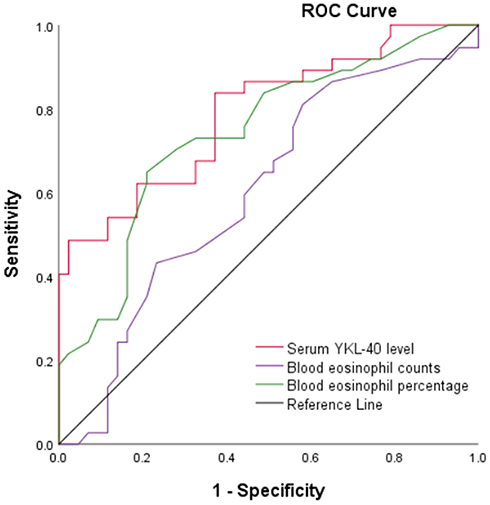 |
Figure 3 Receiver operating characteristics curves of serum YKL-40 level (red line), blood eosinophil counts (purple line), and blood eosinophil percentage (green line). |
YKL-40 Levels in Recurrent CRSwNP Patients and Its Predictive Value in Postoperative Recurrence
Demographic and clinical characteristics between primary CRSwNP group and recurrent CRSwNP group are displayed in Table 5. Statistical differences were observed in comorbid allergic rhinitis (p = 0.016), blood eosinophil counts and percentages (p < 0.001), tissue eosinophil counts and percentages (p < 0.001) and neCRSwNP/eCRSwNP (p = 0.007) between the two groups, no significant difference was found in preoperative VAS score and preoperative Lund–Mackay score. As shown in Figure 4A, serum YKL-40 levels were elevated in recurrent CRSwNP group in comparison with primary CRSwNP group (p < 0.01), particularly in recurrent eCRSwNP group (Figure 4B). The variables with statistical difference in Table 5 were further included into logistic regression analyses (Table 6), and the results suggested that blood eosinophil percentages (p = 0.009), tissue eosinophil counts (p = 0.024), tissue eosinophil percentages (p = 0.002), neCRSwNP/eCRSwNP (p = 0.033), serum YKL-40 levels (p < 0.001) were associated with postoperative recurrence. The ROC analysis results showed that serum YKL-40 levels (AUC = 0.813) exhibited better accuracy and practicability in predicting the postoperative recurrence than other factors (Figure 5, Table 7).
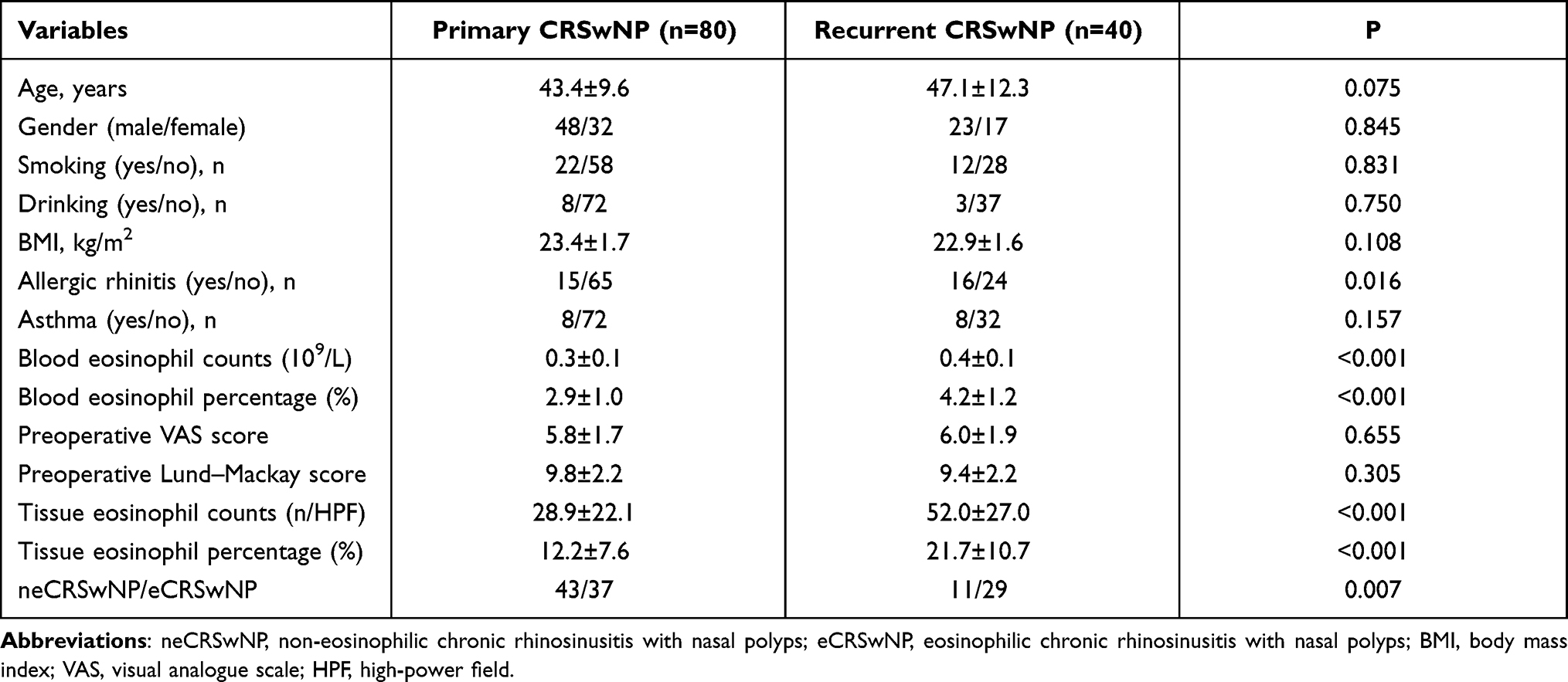 |
Table 5 Demographic Characteristics Between Primary and Recurrent CRSwNP Patients |
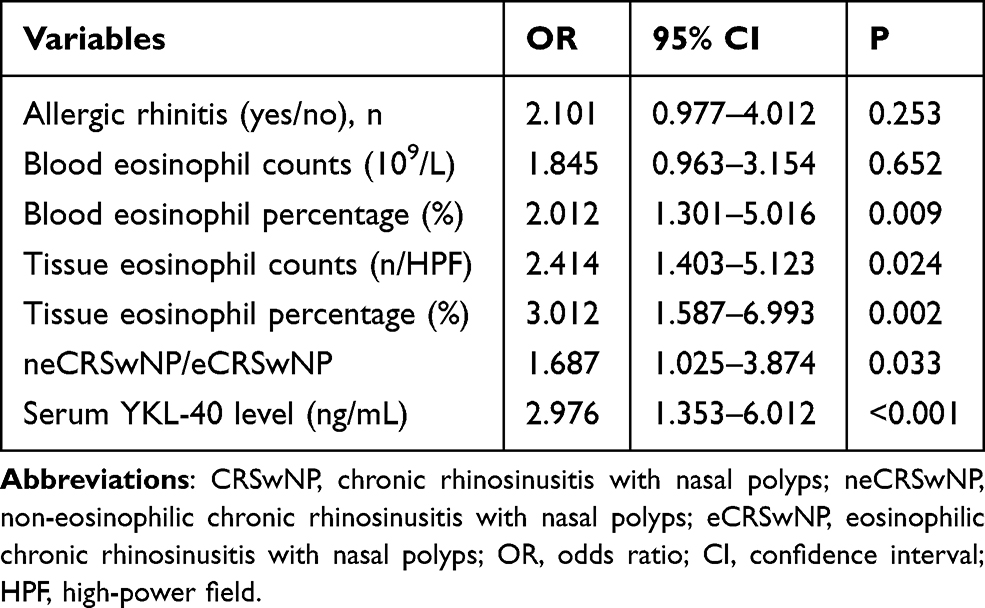 |
Table 6 Logistic Regression Analysis of Factors Affected the Rate of Recurrence in CRSwNP Patients |
 |
Table 7 ROC Analysis Results of Indicators for Predicting the Recurrence of CRSwNP |
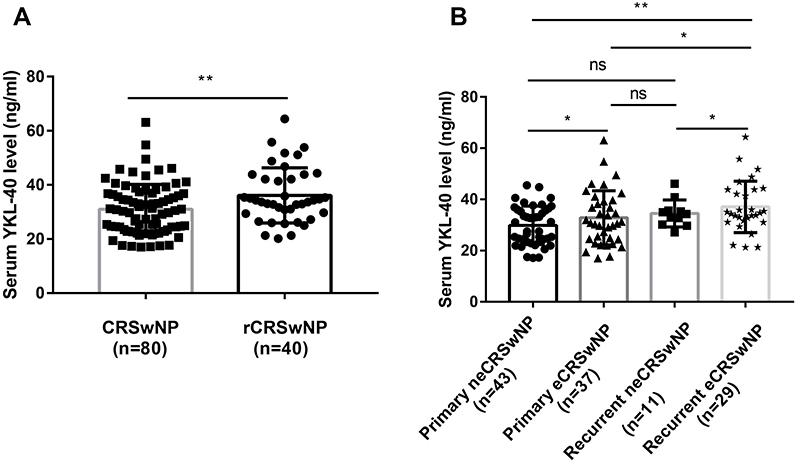 |
Figure 4 Comparison of serum YKL-40 level between CRSwNP and recurrent CRSwNP. (A) Serum YKL-40 levels were distinctly higher in the rCRSwNP than CRSwNP. (B) Serum YKL-40 levels were significantly increased in recurrent eCRSwNP compared with primary neCRSwNP, primary eCRSwNP, and recurrent neCRSwNP. *p < 0.05; **p < 0.01. ns, not significant. Abbreviations: CRSwNP, chronic rhinosinusitis with nasal polyps; rCRSwNP, recurrent chronic rhinosinusitis with nasal polyps; eCRSwNP, eosinophilic chronic rhinosinusitis with nasal polyps; neCRSwNP, non-eosinophilic chronic rhinosinusitis with nasal polyps. |
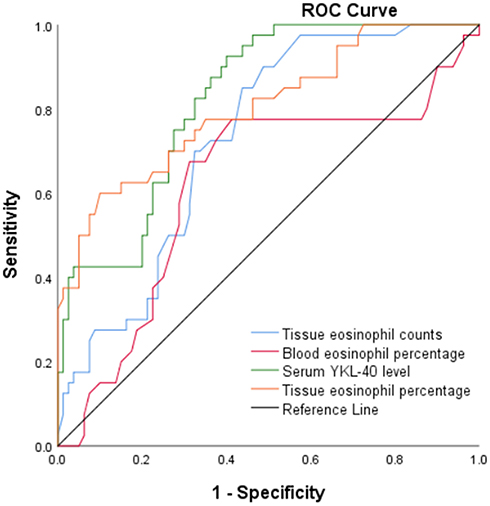 |
Figure 5 Receiver operating characteristics curves of serum YKL-40 level (green line), tissue eosinophil counts (blue line), blood eosinophil percentage (red line), and tissue eosinophil percentage (orange line). |
YKL-40 mRNA and Protein Levels in Nasal Tissues
The qRT-PCR result showed that the mRNA expression level of YKL-40 in CRSwNP patients was significantly higher than that in HCs (p < 0.0001), especially in eCRSwNP group (Figure 6A). No significant difference was seen between primary CRSwNP patients and recurrent CRSwNP patients (p > 0.05, Figure 6B). As IHC staining shown (Figure 7), the expression of YKL-40 was significantly up-regulated in CRSwNP group in comparison with HCs, especially in eCRSwNP and recurrent CRSwNP group, and YKL-40 protein was mainly located at the nasal epithelium and submucosa areas.
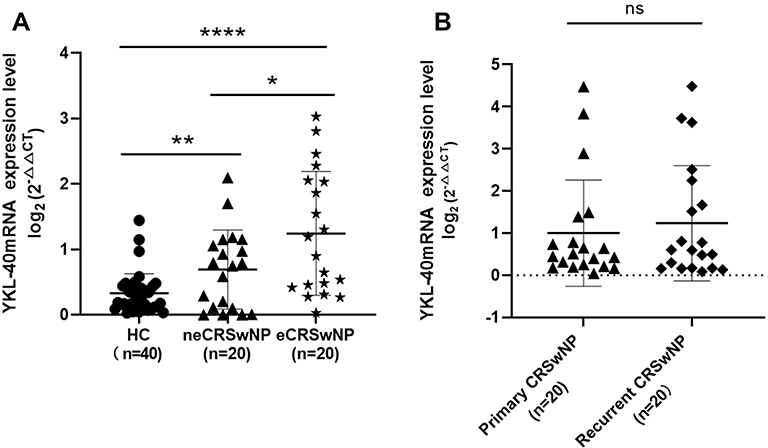 |
Figure 6 The mRNA expression levels of YKL-40 in the tissue of CRSwNP patient and health controls. The mRNA expression levels of YKL-40 among healthy controls, eCRSwNP and neCRSwNP patients. (A) The mRNA expression levels of YKL-40 in primary CRSwNP and recurrent CRSwNP patients. (B) *p < 0.05, **p < 0.01, ****p < 0.0001. ns, not significant. Abbreviations: HC, health control; CRSwNP, chronic rhinosinusitis with nasal polyps; eCRSwNP, eosinophilic chronic rhinosinusitis with nasal polyps; neCRSwNP, non-eosinophilic chronic rhinosinusitis with nasal polyps. |
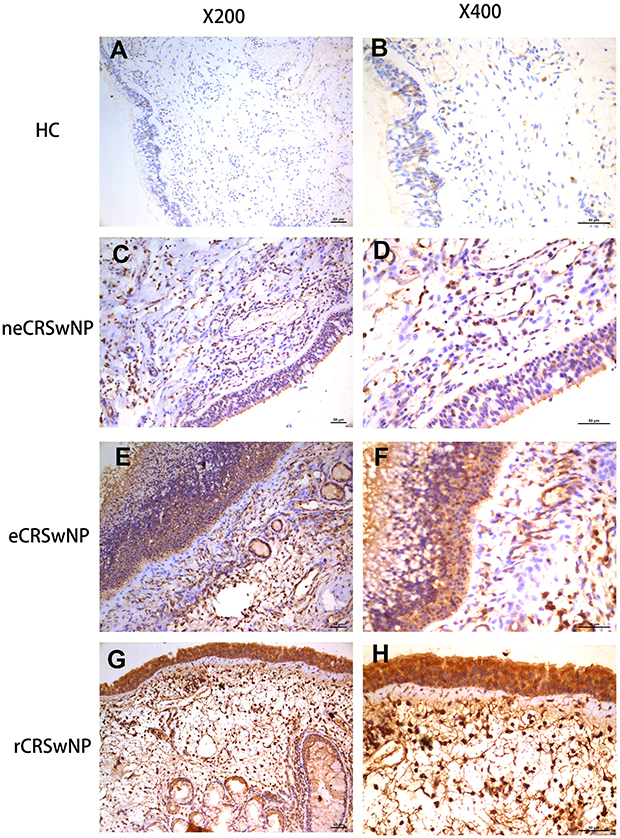 |
Figure 7 Immunohistochemical staining of YKL-40 in HC, eCRSwNP, neCRSwNP and rCRSwNP patients. (×200 and ×400 magnification). (A and B) HC group. (C and D) neCRSwNP group. (E and F) eCRSwNP group. (G and H) rCRSwNP group. Abbreviations: HC, healthy control; CRSwNP, chronic rhinosinusitis with nasal polyps; neCRSwNP, non-eosinophilic chronic rhinosinusitis with nasal polyps; eCRSwNP, eosinophilic chronic rhinosinusitis with nasal polyps; rCRSwNP, recurrent chronic rhinosinusitis with nasal polyps. Notes: HC group specimen from the middle turbinate of same region. Each CRSwNP groups specimens from the nasal polyps of undergoing functional endoscopic sinus surgery. |
Discussion
The present study firstly demonstrated that serum YKL-40 levels were increased in CRSwNP and associated with peripheral blood eosinophil counts and percentages, tissue eosinophil counts and percentages, and ROC curves and multivariate regression analysis showed that serum YKL-40 was closely associated with CRSwNP endotypes. The results of the qRT-PCR shown that the YKL-40 mRNA level was significantly increased in CRSwNP patients compared with HCs, and eCRSwNP group was significantly higher than neCRSwNP group. Interestingly, while YKL-40 expression level was higher in recurrent CRSwNP group than primary CRSwNP group, it was no significant difference, which may due to the small sample size. Furthermore, IHC analysis showed that YKL-40 was high expressed in nasal tissue of CRSwNP compared to HCs, especially in eCRSwNP and recurrent CRSwNP groups, which may involve in the course of CRS disease and associate with disease recurrence. Besides, serum YKL-40 were enhanced in recurrent CRSwNP patients in comparison with primary patients, and serum YKL-40 was a risk factor for postoperative recurrence. Taken together, these results indicated that serum YKL-40 may be an important biomarker for distinguishing CRSwNP endotypes and predicting recidivation.
YKL-40 is a pluripotent cytokine, which is expressed by immune as well as non-immune cells and tissues and secreted by neutrophils, B cells, monocytes, macrophages and epithelial cells.9,20 YKL-40 has been reported to be involved in the pathogenesis of various inflammatory and allergic diseases such as psoriasis, coronary artery atherosclerotic heart disease, asthma.21–23 Prior studies demonstrated that elevated YKL-40 levels activated dendritic cells and promoted CD4+ T cells polarization, then aggravated airway remodeling in asthma patients.24–27 A recent study demonstrated that inhibition of the YKL-40 gene expression in asthmatic mice could alleviate eosinophilic airway inflammation, airway hyperreactivity, airway mucus secretion and significantly reduce the mRNA levels of IL-5, IL-13 and eotaxin.28 In another study, Kang et al found that YKL-40 contributed to the activation of Th2 inflammation and inhibited Th1 inflammation in comparison with YKL-40 null mutant (−/−) mice.29 In the present study, we observed that serum YKL-40 levels of CRSwNP patients were significantly higher compared to HCs, and elevated YKL-40 levels associated with the severity of eosinophilic inflammation in peripheral blood and tissues. We found that YKL-40 mRNA levels were significantly increased in CRSwNP patients; meanwhile, we were able to observe the fact that compared with HCs and neCRSwNP groups, YKL-40 protein expression levels in the nasal epithelium and submucosa areas were significantly increased in eCRSwNP and recurrent CRSwNP through IHC results, which may further support it as a useful and credible marker for clinical testing. These results were in line with most previous publications.29–31 Therefore, we speculated that YKL-40 acted as crucial role in the pathogenesis of CRSwNP, but the specific mechanism remains unclear. Previous studies clarified that eCRSwNP is Th2 cytokines mediated chronic inflammatory response, and tissue eosinophils infiltration served as a main pathological feature of eCRSwNP.1,32–34 It has been reported that YKL-40 could be released by neutrophils, epithelial cells, eosinophils, macrophages, and IL-4 could significantly increase the YKL-40 production in human nasal epithelial cells in vitro.21,30 More importantly, the expression levels of YKL-40 were positively correlated with the levels of IL-5 and eotaxin in the ovalbumin treated epithelial cells, which were potent chemotactic factors for the recruitment of eosinophils, and promoted recruitment of inflammatory progenitor cells into tissues.35,36 Interestingly, we discovered that serum YKL-40 levels were higher in eCRSwNP group than neCRSwNP group, and the tissue mRNA and protein level of YKL-40 were significantly increased in eCRSwNP compared to neCRSwNP. ROC curves and multivariate regression analysis showed that serum YKL-40 level was a reliable indicator to distinguish eCRSwNP from neCRSwNP. Hence, we have reasons to believe that YKL-40 may play a pivotal role in eCRSwNP and can serve as an objective indicator for discriminating CRSwNP endotypes. Preoperative detection of serum YKL-40 may contribute to predicting CRSwNP endotypes and developing individualized therapy.
Although endoscopic sinus surgery bright significantly improved symptoms and quality of life in CRSwNP patients, most patients still suffered a high risk of recurrence.37 Mendelsohn et al found that CRSwNP patients accompanied with asthma suffered a high polyps recurrence rate at 5 years (45%),38 and other researchers reported that the short-term recurrence rates of CRSwNP ranged from 21% to 66%.39 Prior publications showed that the degree of inflammation and eosinophil infiltration in nasal polyps were closely associated with postoperative recurrence.40,41 Van Zele et al described that patients with elevated eosinophil counts, IL-5 and IgE levels in nasal biopsy specimens were more likely to undergo revision surgery.42 In the present study, we found that serum YKL-40 levels were elevated in recurrent CRSwNP group in comparison with primary CRSwNP group, particularly in recurrent eCRSwNP group, and increased YKL-40 levels correlated with tissue and peripheral blood eosinophils. Furthermore, we discovered that tissue mRNA expression level of YKL-40 was elevated in recurrent CRSwNP group in contrast with primary CRSwNP group. Meanwhile, IHC analysis demonstrated that YKL-40 protein expression was significantly increased in recurrent CRSwNP. These results were consistent with our serological results. Accordingly, circulating YKL-40 levels were positively correlated with the productions of IL-5 and eotaxin, which were effective chemokines for eosinophils recruitment.36 The high concentrations of YKL-40 in peripheral blood would promote eosinophils maturation and proliferation, and enhanced tissue infiltration of eosinophils, leading to poor prognosis and higher risk of recidivation of CRSwNP.43 Collectively, we deemed that serum YKL-40 levels can be proposed as an objective biomarker to predict postoperative recurrence in patients with CRSwNP.
However, the present work is a preliminary study to explore the role of YKL-40 in CRSwNP, and further researches are needed to explore the accurate mechanisms of YKL-40, which will provide a theoretical foundation to develop therapeutic target and new drugs based on YKL-40, and contribute to achieving individualized and precise treatment for CRSwNP.
Our study has some limitations. First, the sample size is relatively small, and the participants are recruited from a single medical center, which may increase the risk of selection bias, and we did not perform a subgroup analysis to explore the effect of presence of aspirin intolerance and asthma on the YKL-40 expression. Second, there is no unified criterion regarding the diagnostic criteria of eCRSwNP and recurrent CRSwNP, which may limit the applicability of our findings. Third, due to the difficulty of recruiting a control group with exactly similar age during clinical practice, the inflammation may vary with age. Lastly, we only measured the circulating and tissue levels of YKL-40, and its concentration in nasal lavage fluid was not detected. Further multicenter prospective studies with larger sample size and unified diagnostic criteria are needed to confirm and support our findings in the future.
In summary, we firstly indicated the association between YKL-40 and CRSwNP, and demonstrated that YKL-40 expression was up-regulated in CRSwNP and associated with mucosal eosinophilia and recurrence. We also found that serum YKL-40 might be a potential candidate biomarker for preoperative distinguishing CRSwNP endotypes and predicting its recurrence. These findings contributed to understanding the underlying pathogenesis of eCRSwNP and recurrent CRSwNP, which could provide a novel and effective intervention target and improve precise treatment.
Abbreviations
CRS, chronic rhinosinusitis; CRSwNP, chronic rhinosinusitis with polyps; CRSsNP, chronic rhinosinusitis without nasal polyps; HCs, healthy controls; ELISA, enzyme-linked immunosorbent assay; qRT-PCR, quantitative real-time polymerase chain reaction; IHC, immunohistochemistry; ROC, receiver operating characteristic; eCRSwNP, eosinophilic chronic rhinosinusitis with polyps; neCRSwNP, non-eosinophilic chronic rhinosinusitis with polyps; Th1, T helper 1; Th2, T helper 2; COPD, chronic obstructive pulmonary disease; CT, computed tomography; HRCT, high-resolution computed tomography; MRI, magnetic resonance imaging; VAS, visual analogue scale; H&E, hematoxylin and eosin; HPF, high-power field; SD, standard deviation; ANOVA, one-way analysis of variance.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the recommendations of Declaration of Helsinki. The Human Ethical Committee of Xiangya Hospital of Central South University approved this study, and the approval number is “201907812”. All participants provided informed consent.
Acknowledgments
This work was supported by National Natural Science Foundation of China (No. 81770985, No. 81800917 and No. 81873695) and Natural Science Foundation of Hunan Province (No. 2020JJ4910).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors have declared that there is no competing interest in relation to this study.
References
1. Abbas EE, Li C, Xie A, et al. Distinct clinical pathology and microbiota in chronic rhinosinusitis with nasal polyps endotypes. Laryngoscope. 2021;131(1):E34–e44. doi:10.1002/lary.28858
2. Avdeeva K, Fokkens W. Precision medicine in chronic rhinosinusitis with nasal polyps. Curr Allergy Asthma Rep. 2018;18(4):25. doi:10.1007/s11882-018-0776-8
3. Han JK. Subclassification of chronic rhinosinusitis. Laryngoscope. 2013;123(Suppl 2):S15–S27. doi:10.1002/lary.23979
4. Staudacher AG, Peters AT, Kato A, Stevens WW. Use of endotypes, phenotypes, and inflammatory markers to guide treatment decisions in chronic rhinosinusitis. Ann Allergy Asthma Immunol. 2020;124(4):318–325. doi:10.1016/j.anai.2020.01.013
5. Ikeda K, Shiozawa A, Ono N, et al. Subclassification of chronic rhinosinusitis with nasal polyp based on eosinophil and neutrophil. Laryngoscope. 2013;123(11):E1–E9. doi:10.1002/lary.24154
6. Hu Y, Cao PP, Liang GT, Cui YH, Liu Z. Diagnostic significance of blood eosinophil count in eosinophilic chronic rhinosinusitis with nasal polyps in Chinese adults. Laryngoscope. 2012;122(3):498–503. doi:10.1002/lary.22507
7. Zhong B, Yuan T, Du J, et al. The role of preoperative blood eosinophil counts in distinguishing chronic rhinosinusitis with nasal polyps phenotypes. Int Forum Allergy Rhinol. 2021;11(1):16–23. doi:10.1002/alr.22636
8. Pouyafar A, Heydarabad MZ, Mahboob S, Mokhtarzadeh A, Rahbarghazi R. Angiogenic potential of YKL-40 in the dynamics of tumor niche. Biomed Pharmacother. 2018;100:478–485. doi:10.1016/j.biopha.2018.02.050
9. Abd El-Fattah AA, Sadik NAH, Shaker OG, Mohamed Kamal A. Single nucleotide polymorphism in SMAD7 and CHI3L1 and colorectal cancer risk. Mediators Inflamm. 2018;2018:9853192. doi:10.1155/2018/9853192
10. Lai T, Wu D, Chen M, et al. YKL-40 expression in chronic obstructive pulmonary disease: relation to acute exacerbations and airway remodeling. Respir Res. 2016;17(1):31. doi:10.1186/s12931-016-0338-3
11. Zhou Y, Peng H, Sun H, et al. Chitinase 3-like 1 suppresses injury and promotes fibroproliferative responses in Mammalian lung fibrosis. Sci Transl Med. 2014;6(240):240ra276. doi:10.1126/scitranslmed.3007096
12. Park SJ, Jun YJ, Kim TH, et al. Increased expression of YKL-40 in mild and moderate/severe persistent allergic rhinitis and its possible contribution to remodeling of nasal mucosa. Am J Rhinol Allergy. 2013;27(5):372–380. doi:10.2500/ajra.2013.27.3941
13. Schoneveld L, Ladang A, Henket M, Frix AN, Cavalier E, Guiot J. YKL-40 as a new promising prognostic marker of severity in COVID infection. Crit Care. 2021;25(1):66. doi:10.1186/s13054-020-03383-7
14. Ma Y, Wu S, Cai X, Li X, Feng X. [Expression of YKL-40 and TLR4 in patients with chronic rhinosinusitis]. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2015;50(4):300–305. Chinese.
15. Fokkens WJ, Lund VJ, Mullol J, et al. EPOS 2012: European position paper on rhinosinusitis and nasal polyps 2012. A summary for otorhinolaryngologists. Rhinology. 2012;50(1):1–12. doi:10.4193/Rhino50E2
16. Qi S, Yan B, Liu C, Wang C, Zhang L. Predictive significance of Charcot-Leyden crystal mRNA levels in nasal brushing for nasal polyp recurrence. Rhinology. 2020;58(2):166–174.
17. Zhu Z, Wang W, Zhang X, et al. Nasal fluid cytology and cytokine profiles of eosinophilic and non-eosinophilic chronic rhinosinusitis with nasal polyps. Rhinology. 2020;58(4):314–322.
18. Lund VJ, Mackay IS. Staging in rhinosinusitus. Rhinology. 1993;31(4):183–184.
19. Wen W, Liu W, Zhang L, et al. Increased neutrophilia in nasal polyps reduces the response to oral corticosteroid therapy. J Allergy Clin Immunol. 2012;129(6):1522–1528.e1525. doi:10.1016/j.jaci.2012.01.079
20. Long X, He X, Ohshimo S, et al. Serum YKL-40 as predictor of outcome in hypersensitivity pneumonitis. Eur Respir J. 2017;49(2):1501924. doi:10.1183/13993003.01924-2015
21. Deng Y, Li G, Chang D, Su X. YKL-40 as a novel biomarker in cardio-metabolic disorders and inflammatory diseases. Clin Chim Acta. 2020;511:40–46. doi:10.1016/j.cca.2020.09.035
22. Kong Y, Zhang S, Su X, Peng D, Su Y. Serum levels of YKL-40 are increased in patients with psoriasis: a meta-analysis. Postgrad Med. 2019;131(6):405–412. doi:10.1080/00325481.2019.1643634
23. Wang J, Lv H, Luo Z, et al. Plasma YKL-40 and NGAL are useful in distinguishing ACO from asthma and COPD. Respir Res. 2018;19(1):47. doi:10.1186/s12931-018-0755-6
24. Konradsen JR, James A, Nordlund B, et al. The chitinase-like protein YKL-40: a possible biomarker of inflammation and airway remodeling in severe pediatric asthma. J Allergy Clin Immunol. 2013;132(2):328–335.e325. doi:10.1016/j.jaci.2013.03.003
25. Lee CG, Da Silva CA, Dela Cruz CS, et al. Role of chitin and chitinase/chitinase-like proteins in inflammation, tissue remodeling, and injury. Annu Rev Physiol. 2011;73(1):479–501. doi:10.1146/annurev-physiol-012110-142250
26. Lee CG, Hartl D, Lee GR, et al. Role of breast regression protein 39 (BRP-39)/chitinase 3-like-1 in Th2 and IL-13-induced tissue responses and apoptosis. J Exp Med. 2009;206(5):1149–1166. doi:10.1084/jem.20081271
27. Watson B, Gauvreau GM. Thymic stromal lymphopoietin: a central regulator of allergic asthma. Expert Opin Ther Targets. 2014;18(7):771–785. doi:10.1517/14728222.2014.915314
28. Wang L, Bao A, Zheng Y, et al. Adenovirus vector-mediated YKL-40 shRNA attenuates eosinophil airway inflammation in a murine asthmatic model. Gene Ther. 2021;28(3–4):177–185. doi:10.1038/s41434-020-00202-0
29. Kang MJ, Yoon CM, Nam M, et al. Role of chitinase 3-like-1 in interleukin-18-induced pulmonary type 1, type 2, and type 17 inflammation; alveolar destruction; and airway fibrosis in the Murine lung. Am J Respir Cell Mol Biol. 2015;53(6):863–871. doi:10.1165/rcmb.2014-0366OC
30. Ma Y, Zheng C, Shi L. The role of YKL40 in the pathogenesis of CRS with nasal polyps. Eur Arch Otorhinolaryngol. 2018;275(2):431–438. doi:10.1007/s00405-017-4859-2
31. Peng J, Yu Q, Fan S, et al. High blood eosinophil and YKL-40 levels, as well as low CXCL9 levels, are associated with increased readmission in patients with acute exacerbation of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2021;16:795–806. doi:10.2147/COPD.S294968
32. Ouyang Y, Fan E, Li Y, Wang X, Zhang L. Clinical characteristics and expression of thymic stromal lymphopoietin in eosinophilic and non-eosinophilic chronic rhinosinusitis. ORL J Otorhinolaryngol Relat Spec. 2013;75(1):37–45. doi:10.1159/000346929
33. Shah SA, Ishinaga H, Takeuchi K. Pathogenesis of eosinophilic chronic rhinosinusitis. J Inflamm. 2016;13(1):11. doi:10.1186/s12950-016-0121-8
34. Xu M, Chen D, Zhou H, Zhang W, Xu J, Chen L. The role of periostin in the occurrence and progression of eosinophilic chronic sinusitis with nasal polyps. Sci Rep. 2017;7(1):9479. doi:10.1038/s41598-017-08375-2
35. Allakhverdi Z, Delespesse G. Hematopoietic progenitor cells are innate Th2 cytokine-producing cells. Allergy. 2012;67(1):4–9. doi:10.1111/j.1398-9995.2011.02703.x
36. Ben SQ, Qiu YL, Zhou J, et al. Ovalbumin enhances YKL-40, IL-5, GM-CSF, and eotaxin expression simultaneously in primarily cultured mouse tracheal epithelial cells. In Vitro Cell Dev Biol Anim. 2014;50(3):243–250. doi:10.1007/s11626-013-9698-x
37. Zhang L, Zhang Y, Gao Y, et al. Long-term outcomes of different endoscopic sinus surgery in recurrent chronic rhinosinusitis with nasal polyps and asthma. Rhinology. 2020;58(2):126–135.
38. Mendelsohn D, Jeremic G, Wright ED, Rotenberg BW. Revision rates after endoscopic sinus surgery: a recurrence analysis. Ann Otol Rhinol Laryngol. 2011;120(3):162-166
39. Morrissey DK, Bassiouni A, Psaltis AJ, Naidoo Y, Wormald PJ. Outcomes of modified endoscopic Lothrop in aspirin-exacerbated respiratory disease with nasal polyposis. Int Forum Allergy Rhinol. 2016;6(8):820–825. doi:10.1002/alr.21739
40. Tosun F, Arslan HH, Karslioglu Y, Deveci MS, Durmaz A. Relationship between postoperative recurrence rate and eosinophil density of nasal polyps. Ann Otol Rhinol Laryngol. 2010;119(7):455–459. doi:10.1177/000348941011900705
41. Vlaminck S, Vauterin T, Hellings PW, et al. The importance of local eosinophilia in the surgical outcome of chronic rhinosinusitis: a 3-year prospective observational study. Am J Rhinol Allergy. 2014;28(3):260–264. doi:10.2500/ajra.2014.28.4024
42. Van Zele T, Holtappels G, Gevaert P, Bachert C. Differences in initial immunoprofiles between recurrent and nonrecurrent chronic rhinosinusitis with nasal polyps. Am J Rhinol Allergy. 2014;28(3):192–198. doi:10.2500/ajra.2014.28.4033
43. Brescia G, Contro G, Giacomelli L, Barion U, Frigo AC, Marioni G. Blood eosinophilic and basophilic trends in recurring and non-recurring eosinophilic rhinosinusitis with nasal polyps. Am J Rhinol Allergy. 2021;35(3):296–301. doi:10.1177/1945892420953960
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.