Back to Journals » Journal of Asthma and Allergy » Volume 19
Serum Midkine as a Potential Biomarker Associated with Disease Severity and Remodeling-Related Mediators in Children with Asthma
Authors Xu Y, Zhao L, Mi Y, Ge Y, Guo Y
Received 17 October 2025
Accepted for publication 12 January 2026
Published 20 January 2026 Volume 2026:19 570351
DOI https://doi.org/10.2147/JAA.S570351
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Luis Garcia-Marcos
Yongtian Xu,* Lixia Zhao,* Yingying Mi, Yi Ge, Yanfang Guo
Department of Pediatrics, Shanghai University of Medicine and Health Science Affiliated Gongli Hospital, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yanfang Guo, Department of Pediatrics, Shanghai University of Medicine and Health Science Affiliated Gongli Hospital, No. 219 Miaopu Road, Pudong New District, Shanghai, 200135, People’s Republic of China, Tel +86-15221709828, Email [email protected]
Introduction: Asthma is a heterogeneous inflammatory airway disease in children, for which reliable circulating biomarkers reflecting disease severity and remodeling-associated inflammation remain limited. Midkine, a heparin-binding growth factor involved in inflammatory and fibrotic processes, has emerged as a potential biomarker; however, its clinical relevance in pediatric asthma remains unclear. This study aimed to investigate the association between serum midkine levels and disease severity in children with asthma.
Methods: We enrolled 109 children with asthma (classified into mild, moderate, and severe groups) and 110 healthy controls. Children with asthma were classified into mild, moderate, and severe groups according to the Global Initiative for Asthma (GINA) criteria, and serum midkine levels were measured by ELISA, along with clinical and lung function assessments.
Results: Serum midkine levels were significantly higher in children with asthma than in healthy controls and increased progressively with disease severity. Receiver operating characteristic analysis demonstrated good diagnostic performance of serum midkine for asthma (AUC = 0.949), with a sensitivity of 87.2% and specificity of 94.5% at a cutoff value of 948 pg/mL. Additionally, serum midkine levels were negatively correlated with lung function parameters (FEV1, FEV1/FVC, and PEF) and positively correlated with eosinophilia, total immunoglobulin E (IgE), fractional exhaled nitric oxide (FeNO), pro-inflammatory cytokines, and remodeling-related mediators.
Conclusion: These findings highlight midkine as a promising biomarker and potential therapeutic target for asthma.
Keywords: asthma, midkine, inflammation, lung function, airway remodeling, biomarker
Introduction
Asthma is a chronic inflammatory airway disease characterized by variable airflow obstruction, bronchial hyperresponsiveness, and progressive structural changes collectively referred to as airway remodeling.1 In children, asthma remains a leading cause of chronic morbidity, and severe or poorly controlled disease is associated with impaired lung growth and long-term respiratory dysfunction.2 Airway remodeling, including subepithelial fibrosis, airway smooth muscle hypertrophy, angiogenesis, and extracellular matrix deposition, contributes to persistent airflow limitation and reduced responsiveness to standard anti-inflammatory therapies such as inhaled corticosteroids.3,4
Despite its clinical importance, direct assessment of airway remodeling is challenging in pediatric populations. High-resolution computed tomography and invasive procedures such as bronchoscopy or biopsy are not suitable for routine monitoring in children. Consequently, there is a critical unmet need for noninvasive biomarkers that can reflect remodeling activity, facilitate early risk stratification, and support personalized management strategies in pediatric asthma.5
Midkine is a heparin-binding growth factor that is minimally expressed in healthy adult tissues but markedly upregulated under inflammatory and fibrotic conditions.6 Previous studies have demonstrated elevated midkine levels in several inflammatory and fibrotic diseases, including pulmonary fibrosis, rheumatoid arthritis, and malignancies.7 In experimental models, midkine has been shown to promote eosinophil recruitment, Th2-biased immune responses, angiogenesis, epithelial injury, and fibroblast activation, all of which are key processes implicated in asthma pathophysiology and airway remodeling.8–10
In the context of asthma, limited evidence primarily from adult cohorts and animal studies suggests that midkine expression is increased in severe disease and may contribute to airway inflammation and smooth muscle proliferation.11,12 However, the role of midkine in pediatric asthma, particularly its association with disease severity and remodeling-related mediators, remains poorly defined. Moreover, few studies have explored circulating biomarkers that simultaneously reflect inflammatory burden and structural airway changes in children with asthma.
Given midkine’s established roles in epithelial injury, fibroblast activation, extracellular matrix regulation, and Th2 cytokine signaling, elevated serum midkine levels may represent a biological link between airway inflammation and remodeling progression. To date, no pediatric studies have comprehensively examined serum midkine in relation to both lung function impairment and multiple circulating remodeling markers.
Therefore, the present study aimed to evaluate serum midkine levels in children with asthma and to investigate their associations with disease severity, pulmonary function, inflammatory indices, and airway remodeling-related mediators. We hypothesized that serum midkine levels would be elevated in children with asthma, correlate with disease severity, and associate with biomarkers of airway remodeling, thereby supporting its potential utility as a noninvasive biomarker in pediatric asthma.
Method
Study Population
This case-control study included 109 children with asthma recruited from the pediatric outpatient and inpatient services of our hospital between July 2022 and December 2024. All children with asthma were diagnosed according to the diagnostic criteria of the Global Initiative for Asthma (GINA).13 According to the measured lung function results and severity of the condition, the children with asthma were further divided into mild, moderate, and severe groups. The inclusion criteria were as follows: (i) Age 3–12 years old; (ii) first-onset asthma at the time of initial diagnosis with no prior exposure to asthma-specific treatments (treatment-naïve); (iii) complete clinical data; and (iv) high treatment compliance. Exclusion criteria included: (i) upper respiratory tract infection or systemic corticosteroid use within the preceding 8 weeks; (ii) critically ill asthma; (iii) respiratory symptoms attributable to other causes; and (iv) comorbid conditions such as rheumatoid arthritis or allergic rhinitis. During the same study period, 110 age- and sex-matched healthy children were recruited from those attending routine health examinations to serve as the control group. Healthy controls had no history of asthma or other chronic respiratory, inflammatory, or allergic diseases and had not experienced recent respiratory infections or corticosteroid exposure. The study protocol complied with the Declaration of Helsinki and was approved by the Medical Ethics Committee of our university (GLYY1s2024-052).
Sample Size Calculation
GPower 3.1 software was used to calculate sample size. The significance level (alpha error) was set to 0.05, statistical power (1-β) was set to 0.95, and effect size was set a median effect of 0.5. A two-sided test was chosen, and the sample size ratio was 1:1. The calculation result shows that each group requires at least 88 samples.
Clinical Data Collection
Clinical and laboratory data, including age, sex, body mass index (BMI), duration of the current asthma exacerbation (disease duration), fever duration during the current exacerbation, presence of allergies, minor upper respiratory tract symptoms, and cough, were collected from both children with asthma and healthy control subjects. Patients with severe or ongoing respiratory infections requiring hospitalization or systemic antibiotics were excluded. Five milliliters (5 mL) of peripheral venous blood was collected upon admission and sent to the hospital’s laboratory for measurement of neutrophil count and total IgE.
Pulmonary function tests were performed using standardized spirometry in accordance with the American Thoracic Society/European Respiratory Society (ATS/ERS) guidelines for pediatric lung function testing. Spirometry was conducted using a calibrated Spirolab® spirometer (MIR, Italy) operated by trained respiratory technicians experienced in testing young children. The device was calibrated daily according to the manufacturer’s instructions. For each subject, at least three technically acceptable maneuvers were obtained, and the highest reproducible values were recorded. Acceptability and reproducibility criteria were applied according to ATS/ERS recommendations, with age-appropriate coaching provided to ensure reliable performance. Forced expiratory volume in one second (FEV1), forced vital capacity (FVC), and peak expiratory flow rate (PEF) were measured, and the FEV1/FVC ratio was calculated.
Fractional Exhaled Nitric Oxide (FeNO) Measurement
Fractional exhaled nitric oxide (FeNO) was measured using a nitric oxide analyzer (Sunvou-CA2122 system, China) in accordance with the American Thoracic Society/European Respiratory Society (ATS/ERS) recommendations. Measurements were performed at a constant expiratory flow rate of 50 mL/s. Before testing, children were instructed to avoid eating, drinking, strenuous exercise, and nitrate-rich foods for at least 1 hour, and short-acting bronchodilators were withheld in accordance with guideline recommendations. Each subject performed the maneuver under the supervision of trained technicians, maintaining a stable exhalation for an age-appropriate duration. At least two reproducible measurements within acceptable limits were obtained, and the mean value was recorded. Results were expressed as parts per billion (ppb).14
Enzyme‑linked Immunosorbent Assay (ELISA)
ELISA was used to measure serum levels of tumor necrosis factor-alpha (TNF-α; DTA00D, R&D Systems; lower limit of detection [LoD]: 0.5 pg/mL), interleukin-1 beta (IL-1β; DLB50, R&D Systems; LoD: 1.0 pg/mL), interleukin-4 (IL-4; D4050, R&D Systems; LoD: 0.11 pg/mL), transforming growth factor beta 1 (TGF-β1; DY240, R&D Systems; LoD: 31.2 pg/mL), matrix metalloproteinase 9 (MMP-9; DMP900, R&D Systems; LoD: 0.156 ng/mL), stromal cell-derived factor-1 alpha (SDF-1α; ml038196, Shanghai Enzyme-linked Biotechnology; LoD: 18 pg/mL), hyaluronan (DHYAL0, R&D Systems; LoD: 0.2 ng/mL), and midkine (DY258, R&D Systems; LoD: 78.1 pg/mL) in both children with asthma and healthy control subjects, according to the manufacturers’ instructions. Serum samples were processed within 2 hours of collection and stored at −80 °C, with a maximum of two freeze-thaw cycles before analysis. All assays were performed in duplicate by personnel blinded to group allocation. Intra-assay and inter-assay coefficients of variation were within the ranges specified by the kit manufacturers, ensuring reproducibility and reliability of measurements.
Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics version 20.0. Continuous variables with a normal distribution are presented as mean ± standard deviation (SD). Comparisons between two groups were performed using the independent-samples t-test, and comparisons among multiple groups were conducted using one-way analysis of variance (ANOVA). Categorical variables are presented as frequencies and percentages and were analyzed using the chi-square test. Pearson’s correlation coefficient was used to assess the relationships between serum midkine levels and other continuous clinical, inflammatory, and remodeling-related variables. Receiver operating characteristic (ROC) curve analysis was performed to evaluate the diagnostic performance of serum midkine and to determine the optimal cut-off value for distinguishing children with asthma from healthy controls. To account for multiple comparisons in the analysis of serum biomarkers, P-values were adjusted using an appropriate correction method, as specified in the revised analysis. A two-sided P value < 0.05 was considered statistically significant.
Results
Demographic and Clinical Characteristics
The clinical and spirometric characteristics of children with asthma and healthy controls are summarized in Table 1. No significant differences were observed between the two groups for age, sex, or body mass index (BMI) (P > 0.05). In contrast, children with asthma exhibited significantly impaired lung function, as evidenced by lower forced expiratory volume in 1 second (FEV1), FEV1/forced vital capacity (FEV1/FVC), and peak expiratory flow (PEF) than healthy controls (all P < 0.001).
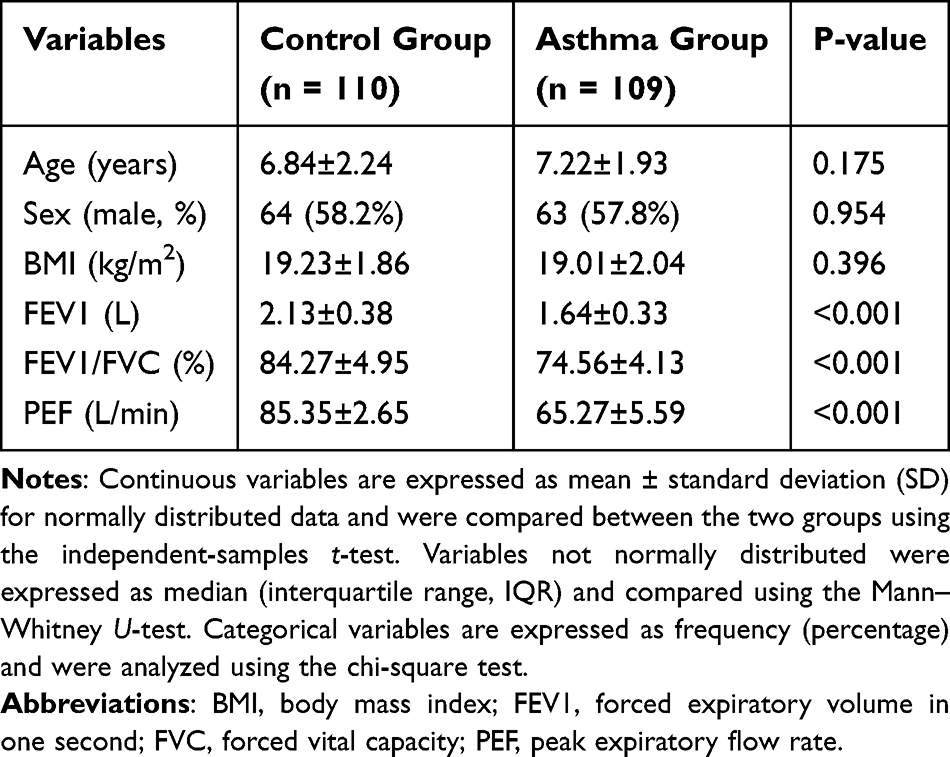 |
Table 1 Demographic and Spirometric Characteristics of the Healthy Controls and Asthma Patients |
Following the clinical assessment, analysis of inflammatory and immune parameters demonstrated that children with asthma had significantly elevated eosinophil counts, total immunoglobulin E (IgE), fractional exhaled nitric oxide (FeNO), and circulating cytokines, including TNF-α, IL-1β, and IL-4, as well as higher levels of airway remodeling markers (TGF-β1, MMP-9, SDF-1α, and hyaluronan) and midkine compared with healthy controls (all P < 0.001) (Table 2).
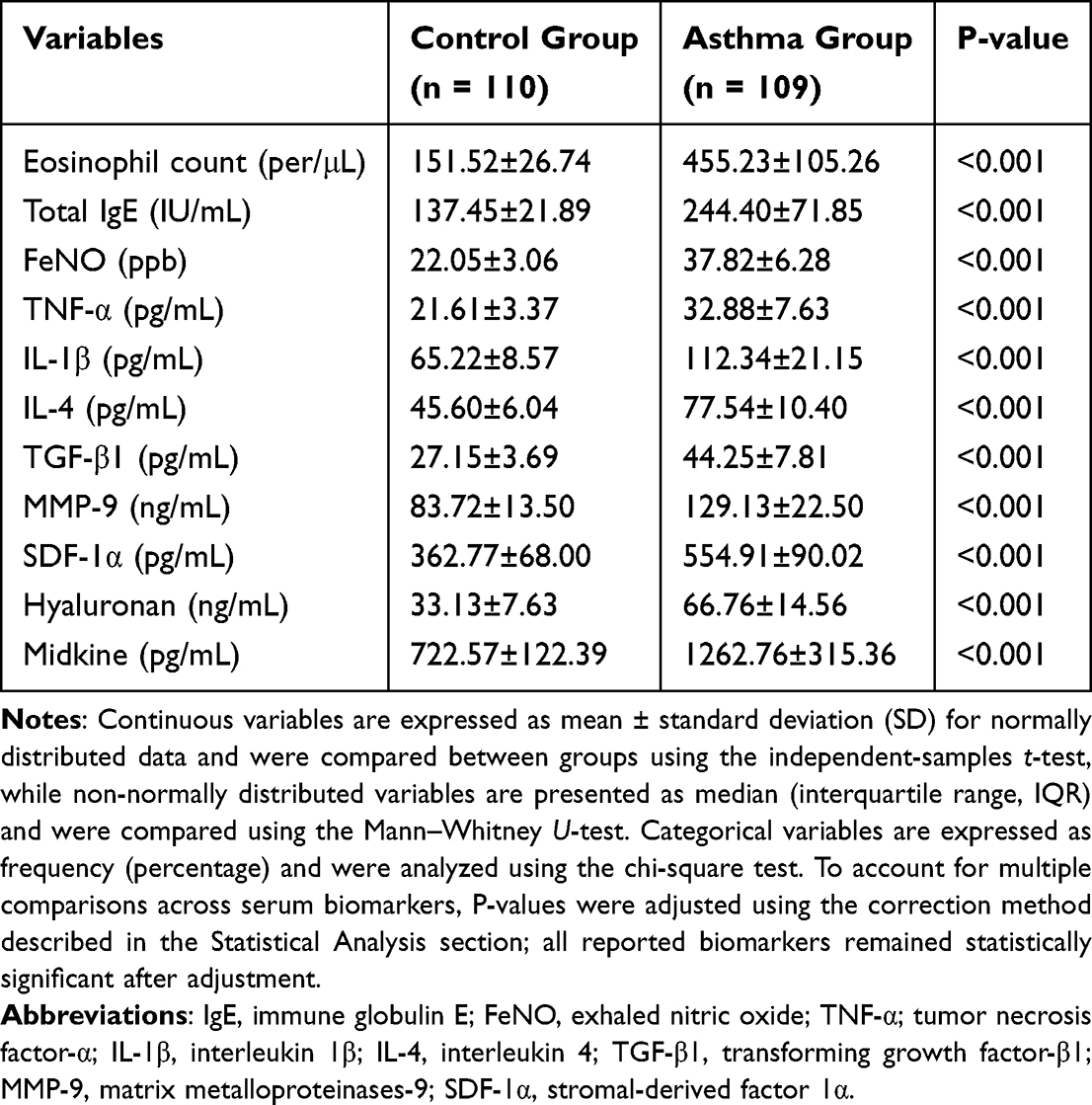 |
Table 2 Serum Biomarkers of Inflammation, Immunity, and Airway Remodeling in Healthy Controls and Asthma Patients |
Comparative analysis of asthma severity subgroups using one-way analysis of variance (ANOVA) revealed that children with severe asthma had a longer disease duration and greater lung function impairment, with significantly lower FEV1, FEV1/FVC, and PEF values than those with mild or moderate asthma. In parallel, the severe asthma subgroup exhibited markedly higher levels of eosinophils, total IgE, FeNO, inflammatory cytokines, airway remodeling biomarkers, and serum midkine (Table 3). No significant differences were observed among asthma subgroups for age, sex, BMI, fever duration, atopy, respiratory tract infection, or cough (P > 0.05). These findings underscore the distinct clinical and biological profile of severe asthma, characterized by greater airflow limitation and an enhanced inflammatory and remodeling burden.
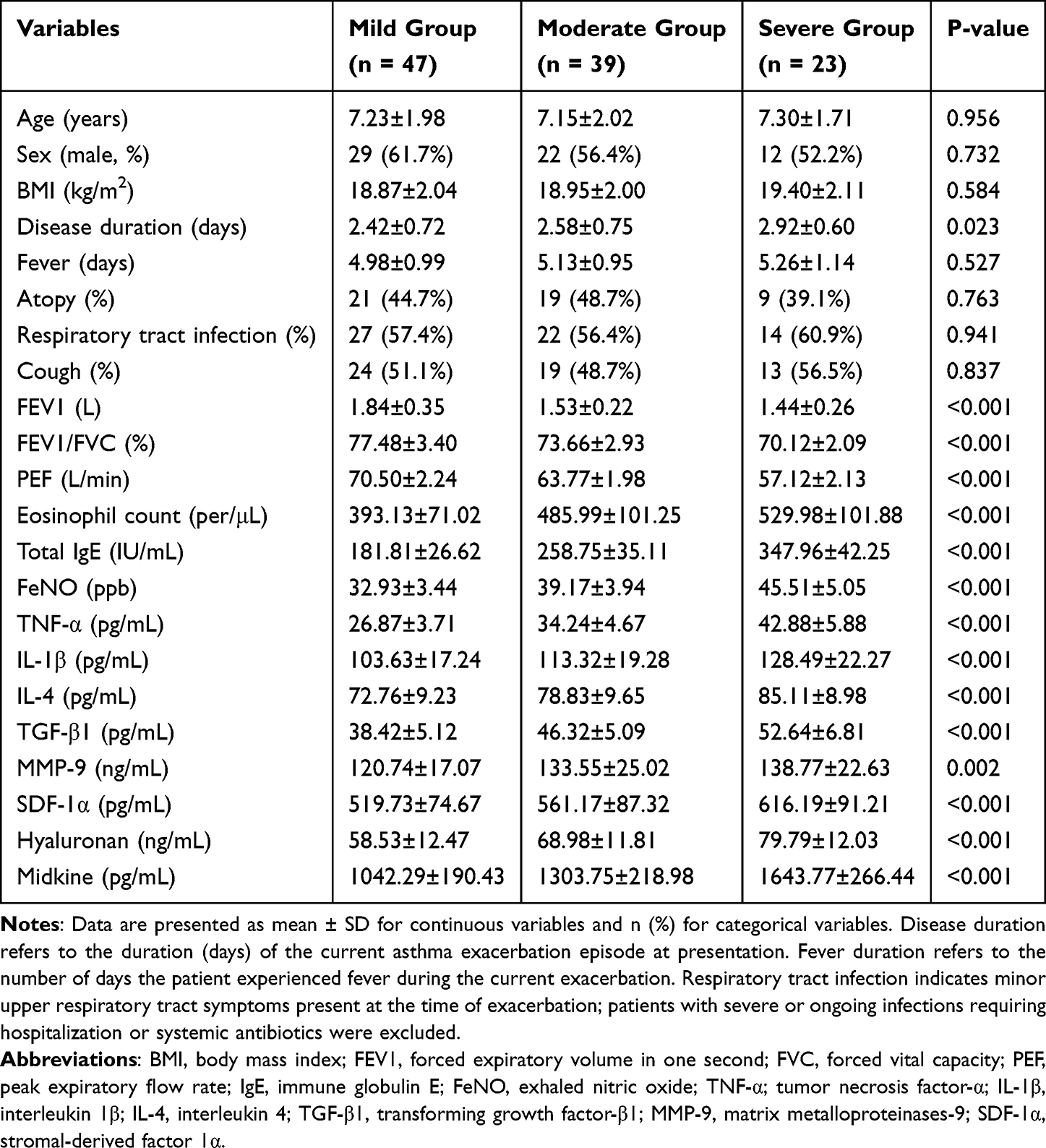 |
Table 3 Characteristics of Asthma Patients with Different Disease Severity |
Serum Midkine Levels in Children with Asthma
Serum midkine levels were quantified in patients with asthma (n=109) and healthy controls (n=110) using ELISA. The findings indicated that midkine concentrations were significantly elevated in patients with asthma compared to those in healthy controls (Figure 1A). Additionally, serum midkine levels were compared between groups stratified according to asthma status: mild asthma (n=47), moderate asthma (n=39), and severe asthma (n=23). It was observed that midkine levels were significantly increased in patients with severe asthma compared to those with moderate and mild asthma subgroups (Figure 1B). Moreover, Receiver Operating Characteristic (ROC) curve analysis revealed that the optimal cutoff value for serum midkine was 948 pg/mL, with a sensitivity of 87.2% and a specificity of 94.5%, resulting in an Area Under the Curve (AUC) of 0.949 (Figure 1C). These findings suggest that serum midkine levels may serve as a potential biomarker for asthma, with higher levels being associated with disease severity.
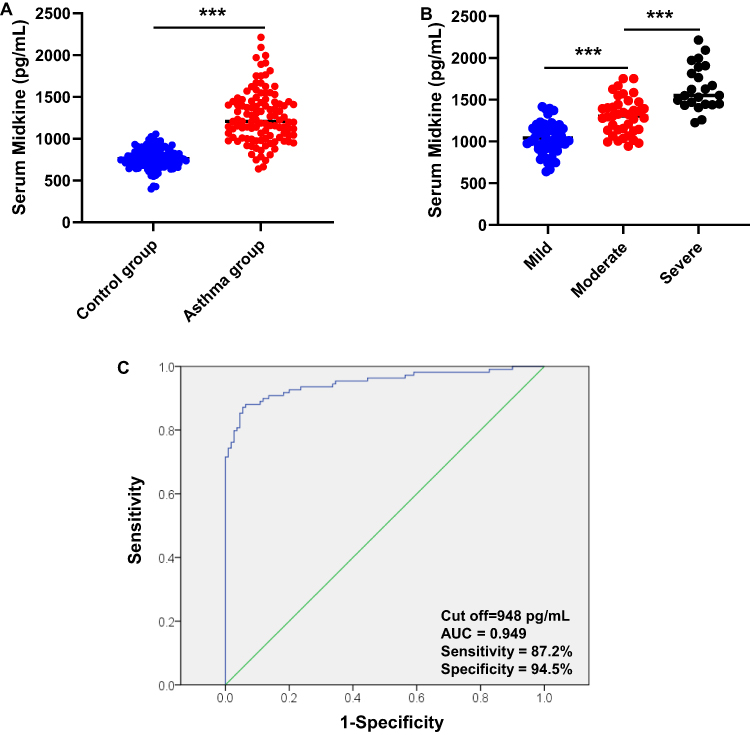 |
Figure 1 Serum midkine levels in asthma patients. (A) Serum midkine levels were measured by ELISA in control subjects (n=110) and asthma patients (n=109). (B) Serum midkine levels were compared in children with mild asthma (n=47), moderate asthma (n=39), and severe asthma (n=23). (C) The ROC curve is used to obtain the cut-off point of serum midkine levels that diagnose asthma. The optimal cut-off point is 948 pg/mL. The area under the curve is 0.949. T-test was used to compare the differences between two groups, and ANOVA was used to compare the differences between three groups. ***P<0.001. |
Correlation Between Serum Midkine Levels and Lung Function in Children with Asthma
Pearson’s correlation analysis revealed a significant negative correlation between serum midkine levels and lung function parameters in children with asthma, including FEV1 (r=−0.222, P=0.021), FEV1/FVC (r=−0.472, P<0.001), and PEF (r=−0.646, P<0.001) (Figures 2A–C). The findings suggest that elevated serum midkine levels are associated with worse lung function in children with asthma, as indicated by lower FEV1, FEV1/FVC ratio, and PEF values. This implies that midkine may play a role in asthma severity or airway obstruction.
 |
Figure 2 Correlation between serum midkine levels and lung function in children with asthma. Serum midkine is negatively correlated with (A) forced expiratory volume in one second (FEV1), (B) FEV1/forced vital capacity (FEV1/FVC), and (C) peak expiratory flow rate (PEF). Pearson correlation analysis was performed. |
Correlation Between Serum Midkine Levels and Inflammatory Markers in Children with Asthma
Pearson’s correlation analysis identified a notable positive correlation between several inflammatory markers in children with asthma, such as eosinophil count (r=0.295, P=0.002), total IgE (r=0.667, P<0.001), FeNO (r=0.553, P<0.001), TNF-α (r=0.562, P<0.001), IL-1β (r=0.312, P=0.001), and IL-4 (r=0.225, P=0.019) (Figures 3A–F). These results indicate that serum midkine is significantly linked to eosinophilic inflammation, allergic reactions (IgE), airway inflammation (FeNO), and the activity of pro-inflammatory cytokines (TNF-α, IL-1β, and IL-4) in children with asthma.
 |
Figure 3 Correlation between serum midkine levels and inflammation in children with asthma. Serum midkine is positively correlated with (A) Eosinophil count, (B) Total IgE, (C) FeNO, (D) TNF-α, (E) IL-1β, and (F) IL-4. |
Correlation Between Serum Midkine Levels and Airway Remodeling Markers in Children with Asthma
Serum midkine levels demonstrated significant positive correlations with key airway remodeling markers in children with asthma, including TGF-β1 (r=0.550, P<0.001), MMP-9 (r=0.281, P=0.003), SDF-1α (r=0.300, P=0.002), and hyaluronan (r=0.435, P<0.001) (Figures 4A–D). These findings suggest that elevated serum midkine levels are associated with increased expression of airway remodeling mediators, potentially implicating midkine in the pathogenesis of asthma-related structural changes.
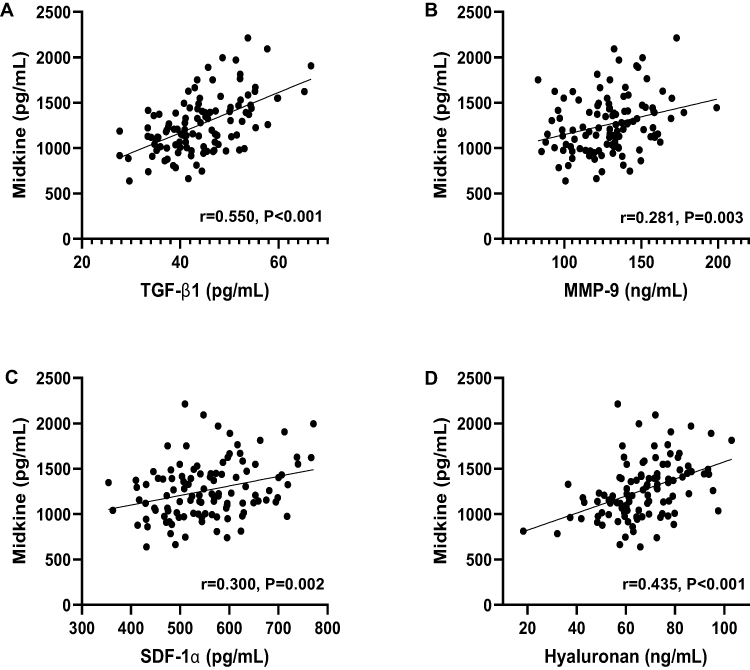 |
Figure 4 Correlation between serum midkine levels and serum airway remodeling markers in children with asthma. Serum Midkine is positively correlated with (A) TGF-β1, (B) MMP-9, (C) SDF-1α, and (D) Hyaluronan. |
Discussion
This study investigated serum midkine levels in children with asthma and examined their associations with disease severity, lung function impairment, and circulating markers of airway inflammation and remodeling. We found that serum midkine levels were significantly elevated in children with asthma compared with healthy controls and increased progressively with disease severity. Higher midkine levels were associated with poorer lung function, as reflected by lower FEV1, FEV1/FVC, and PEF values, and were positively correlated with eosinophilic inflammation, total IgE, FeNO, pro-inflammatory cytokines, and multiple remodeling-related mediators. Importantly, given the cross-sectional design of this study, these findings should be interpreted as associations rather than evidence of causation.
Asthma is a chronic inflammatory airway disease characterized by variable airflow obstruction, bronchial hyperresponsiveness, and airway remodeling.15 Identifying noninvasive biomarkers that reflect disease severity and structural airway changes is particularly important in pediatric populations, where ethical and technical constraints limit direct assessment of remodeling. Midkine, a heparin-binding growth factor that is minimally expressed in healthy tissues but upregulated in inflammatory and fibrotic conditions,7 has emerged as a candidate biomarker in this context. Experimental and adult clinical studies have reported increased midkine expression in severe asthma and have linked it to eosinophil recruitment, Th2-biased inflammation, and airway smooth muscle proliferation.16,17 Our findings extend this evidence to children and demonstrate that elevated serum midkine is associated with asthma severity and functional impairment in a pediatric cohort.
To our knowledge, this study is among the first to comprehensively examine serum midkine in children with asthma in relation to both lung function indices and a broad panel of circulating inflammatory and airway remodeling–related biomarkers. Unlike previous reports that focused primarily on adult patients or experimental models, our study included treatment-naïve children at first diagnosis, thereby minimizing the confounding effects of long-term therapy. This pediatric-specific evidence advances current knowledge by suggesting that midkine-associated biological signals are present early in the disease course and are linked to markers commonly interpreted as surrogates of airway remodeling.
The observed associations between serum midkine and established inflammatory biomarkers, including eosinophil count, IgE, and FeNO, indicate that midkine may reflect underlying type-2 inflammatory activity. At the same time, its correlations with TGF-β1, MMP-9, SDF-1α, and hyaluronan suggest a relationship with pathways implicated in extracellular matrix turnover, fibroblast activation, and tissue remodeling. In this regard, midkine may provide complementary rather than redundant information to existing biomarkers. While IgE and FeNO primarily capture allergic sensitization and airway inflammation, midkine may integrate signals related to both inflammatory burden and remodeling-associated processes, although this hypothesis requires further validation.
It is important to emphasize that the present data do not establish whether midkine actively contributes to airway remodeling or whether its elevation reflects a downstream consequence of chronic inflammation or structural changes. Experimental studies have shown that midkine can promote fibroblast activation, collagen deposition, and angiogenesis,12,18 but such mechanisms cannot be inferred from our clinical observations. Therefore, serum midkine should currently be viewed as a potential marker of disease activity and remodeling-associated inflammation, rather than a confirmed pathogenic mediator in pediatric asthma.
Study Limitations and Future Directions
This study has several limitations. First, because of its cross-sectional and correlational design, causal relationships between serum midkine levels and asthma severity, airway inflammation, or remodeling cannot be established. Consequently, it remains unclear whether elevated midkine is a driver or a consequence of disease activity. Longitudinal and mechanistic studies are therefore required to determine whether midkine directly contributes to disease progression, lung function decline, airway remodeling, or treatment response in pediatric asthma. Second, although serum midkine levels were correlated with asthma severity and multiple inflammatory and remodeling-related biomarkers, multivariate analyses were not performed. Thus, it cannot be determined whether midkine is independently associated with disease severity after adjustment for established markers such as eosinophil counts, total IgE, and FeNO; future studies with larger cohorts should incorporate multivariate models to address this issue. Third, airway remodeling was assessed using circulating biomarkers rather than direct structural measurements. While the use of noninvasive markers is appropriate in pediatric populations, future research integrating biomarker analyses with imaging or functional assessments would provide more comprehensive insight into airway remodeling. Finally, although including treatment-naïve, first-onset pediatric asthma patients minimized therapeutic confounding, this may limit the generalizability of the findings to children with long-standing or previously treated asthma. Further studies encompassing different disease stages are therefore warranted.
Conclusion
This study shows that serum midkine levels are elevated in children with asthma and are significantly associated with markers of airway inflammation, remodeling-related mediators, and impaired lung function. These findings support the potential utility of midkine as a non-invasive biomarker reflecting disease severity and remodeling-associated inflammatory burden in pediatric asthma. However, given the cross-sectional nature of the study, causal relationships cannot be established, and it remains unclear whether elevated midkine is a driver of airway remodeling, a downstream consequence of chronic inflammation, or an epiphenomenon. Figure 5 summarizes only the observed associations. Further longitudinal studies, external validation in independent cohorts, and mechanistic investigations are required to clarify the temporal role of midkine in pediatric asthma and to determine its potential value for clinical risk stratification or therapeutic targeting.
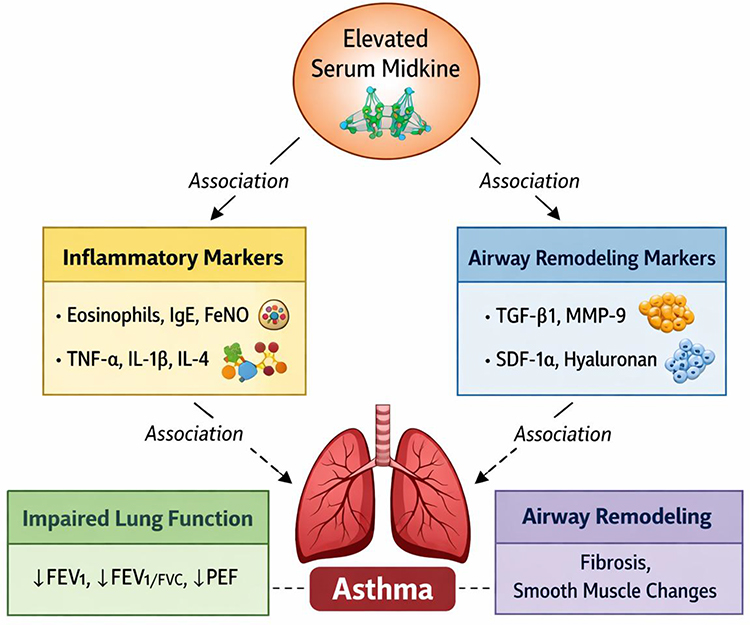 |
Figure 5 Schematic diagram of serum midkine associations in pediatric asthma. Serum midkine levels were positively associated with inflammatory markers (eosinophils, IgE, FeNO, TNF-α, IL-1β, IL-4) and airway remodeling biomarkers (TGF-β1, MMP-9, SDF-1α, hyaluronan), and negatively associated with lung function (FEV1, FEV1/FVC, PEF). Solid arrows indicate observed correlations; dashed arrows indicate relationships with asthma outcomes. |
AI Declaration
We used the AI tool ChatGPT (version 5; GPT-5) to assist in the preparation of this manuscript, specifically for language editing and improving its readability.
Data Sharing Statement
The datasets used/analyzed during the present study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The Ethics Committee of the Shanghai University of Medicine and Health Science Affiliated Gongli Hospital approved this study (GLYY1s2024-052). The authors followed all standard protocols in accordance with the 1964 Declaration of Helsinki. Written informed consent was obtained from the legal guardians of all minor participants prior to study commencement.
Consent for Publication
The legal guardians of all minor participants provided consent for the publication of the participants’ data.
Acknowledgment
We sincerely thank all of the participants in our study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is supported by the Construction of key weak disciplines in the Health System of Shanghai Pudong New Area (PWZbr2022-06).
Disclosure
The authors declare that they have no competing interests.
References
1. Holgate ST. Pathogenesis of asthma. Clin Exp Allergy. 2008;38(6):872–12. doi:10.1111/j.1365-2222.2008.02971.x
2. Guilbert TW, Morgan WJ, Zeiger RS, et al. Long-term inhaled corticosteroids in preschool children at high risk for asthma. N Engl J Med. 2006;354(19):1985–1997. doi:10.1056/NEJMoa051378
3. James AL, Elliot JG, Jones RL, et al. Airway smooth muscle hypertrophy and hyperplasia in asthma. Am J Respir Crit Care Med. 2012;185(10):1058–1064. doi:10.1164/rccm.201110-1849OC
4. Benayoun L, Druilhe A, Dombret MC, Aubier M, Pretolani M. Airway structural alterations selectively associated with severe asthma. Am J Respir Crit Care Med. 2003;167(10):1360–1368. doi:10.1164/rccm.200209-1030OC
5. Saglani S, Lloyd CM. Novel concepts in airway inflammation and remodelling in asthma. Eur Respir J. 2015;46(6):1796–1804. doi:10.1183/13993003.01196-2014
6. Kadomatsu K, Kishida S, Tsubota S. The heparin-binding growth factor midkine: the biological activities and candidate receptors. J Biochem. 2013;153(6):511–521.
7. Muramatsu T. Midkine, a heparin-binding cytokine with multiple roles in development, repair and diseases. Proc Jpn Acad Ser B Phys Biol Sci. 2010;86(4):410–425. doi:10.2183/pjab.86.410
8. Weckbach LT, Groesser L, Borgolte J, et al. Midkine acts as proangiogenic cytokine in hypoxia-induced angiogenesis. Am J Physiol Heart Circ Physiol. 2012;303(4):H429–38. doi:10.1152/ajpheart.00934.2011
9. Horiba M, Kadomatsu K, Nakamura E, et al. Neointima formation in a restenosis model is suppressed in midkine-deficient mice. J Clin Invest. 2000;105(4):489–495. doi:10.1172/JCI7208
10. Leung S, Liu X, Fang L, Chen X, Guo T, Zhang J. The cytokine milieu in the interplay of pathogenic Th1/Th17 cells and regulatory T cells in autoimmune disease. Cell Mol Immunol. 2010;7(3):182–189.
11. Ikematsu S, Yano A, Aridome K, et al. Serum midkine levels are increased in patients with various types of carcinomas. Br J Cancer. 2000;83(6):701–706. doi:10.1054/bjoc.2000.1339
12. Misa K, Tanino Y, Wang X, et al. Involvement of midkine in the development of pulmonary fibrosis. Physiol Rep. 2017;5(16):e13383. doi:10.14814/phy2.13383
13. Global Initiative for Asthma. Global strategy for asthma management and prevention, 2025 update. GINA; 2025.
14. Dweik RA, Boggs PB, Erzurum SC, et al. American thoracic society committee on interpretation of exhaled nitric oxide levels (FENO) for clinical applications. An official ATS clinical practice guideline: interpretation of exhaled nitric oxide levels (FENO) for clinical applications. Am J Respir Crit Care Med. 2011;184(5):602–615. doi:10.1164/rccm.9120-11ST
15. Reddel HK, Bacharier LB, Bateman ED, et al. Global initiative for asthma strategy 2021: executive summary and rationale for key changes. J Allergy Clin Immunol Pract. 2022;10:S1–S18. doi:10.1016/j.jaip.2021.10.001
16. Hernandez-Lara MA, Yadav SK, Shah SD, et al. Regulation of airway smooth muscle cell proliferation by diacylglycerol kinase: relevance to airway remodeling in asthma. Int J Mol Sci. 2022;23(19):11868. doi:10.3390/ijms231911868
17. Sorrelle N, Dominguez ATA, Brekken RA. From top to bottom: midkine and pleiotrophin as emerging players in immune regulation. J Leukoc Biol. 2017;102(2):277–286.
18. Filippou PS, Karagiannis GS, Constantinidou A. Midkine (MDK) growth factor: a key player in cancer progression and a promising therapeutic target. Oncogene. 2020;39(10):2040–2054. doi:10.1038/s41388-019-1124-8
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.