Back to Journals » International Journal of Nephrology and Renovascular Disease » Volume 17
Serum Methotrexate Level Predicts Acute Kidney Injury After High-Dose Methotrexate: A Case Report and Single-Center Experience
Authors Yen PW, Lin HY, Wu CC ![]() , Huang TC, Wu SJ, Pan SY, Hung KY
, Huang TC, Wu SJ, Pan SY, Hung KY
Received 17 July 2024
Accepted for publication 29 October 2024
Published 5 November 2024 Volume 2024:17 Pages 277—285
DOI https://doi.org/10.2147/IJNRD.S487368
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pravin Singhal
Pao-Wen Yen,1 Hsing-Yu Lin,2 Chien-Chih Wu,2 Tai-Chung Huang,3 Shang-Ju Wu,3 Szu-Yu Pan,1,4 Kuan-Yu Hung1,5
1Division of Nephrology, Department of Internal Medicine, National Taiwan University Hospital, Taipei City, Taiwan; 2Department of Pharmacy, National Taiwan University Hospital, Taipei City, Taiwan; 3Division of Hematology, Department of Internal Medicine, National Taiwan University Hospital, Taipei City, Taiwan; 4Department of Integrated Diagnostics & Therapeutics, National Taiwan University Hospital, Taipei City, Taiwan; 5Graduate Institute of Clinical Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan
Correspondence: Chien-Chih Wu, Department of Pharmacy, National Taiwan University Hospital, Taipei City, Taiwan, Tel +886-2-23123456, Email [email protected] Kuan-Yu Hung, Division of Nephrology, Department of Internal Medicine, National Taiwan University Hospital, Taipei City, Taiwan, Tel +886-2-23123456, Email [email protected]
Background: Acute kidney injury (AKI) is a serious complication following high-dose methotrexate (HD-MTX) treatment, despite established preventive measures. This study presents a case report and a retrospective review of patients treated with HD-MTX, aiming to identify risk factors for AKI and propose a modified treatment protocol.
Methods: We report a case of a 43-year-old man with diffuse large B-cell lymphoma who developed severe AKI after HD-MTX therapy. Additionally, a retrospective review of 70 patients receiving HD-MTX at our institution was conducted to identify predictors of AKI. Serum methotrexate levels were analyzed to determine their significance in predicting AKI.
Results: The index patient developed methotrexate intoxication and severe AKI despite receiving standard prophylactic measures, requiring temporary hemodialysis. The retrospective review identified serum methotrexate levels as a significant predictor of AKI (OR 11.84, 95% CI: 2.62– 53.53, p = 0.001). Higher initial serum methotrexate levels correlated with the development of AKI.
Conclusion: Timely measurement of serum methotrexate levels is crucial in managing and preventing AKI in patients undergoing HD-MTX therapy. Based on our findings, we propose a modified HD-MTX treatment protocol to reduce the incidence of AKI. This includes earlier serum methotrexate level monitoring and adjustments in urine alkalization and leucovorin dosing strategies.
Keywords: methotrexate, acute kidney injury
Introduction
Methotrexate (MTX), an antifolate metabolite, is widely used for malignant diseases. High-dose MTX (HD-MTX), defined as a dose higher than 500 mg/m2, is used to treat acute leukemia, osteosarcoma, and non-Hodgkin lymphoma, especially in the central nervous system (CNS). MTX induces cell death by inhibiting dihydrofolate reductase (DHFR), a critical enzyme catalyzing the conversion of dihydrofolate to tetrahydrofolate.1 HD-MTX may cause side effects including acute kidney injury (AKI) (2–12%), mucositis (10–30%), chemical hepatitis (up to 60%), high-grade myelosuppression (5–10%), and neurotoxicity (15%).1,2 Because approximately 90% of MTX is eliminated through the kidney, the development of AKI significantly reduces MTX clearance and potentiates the severity of other side effects.3 As a result, prevention of AKI in patients receiving MTX is essential. The principal mechanisms of MTX-induced AKI are crystal nephropathy and direct tubular injury.4,5 Timely measurement of serum MTX level, urine alkalization to increase urinary MTX solubility, avoidance of drugs interfering with MTX elimination, fluid administration to augment urinary flow, and third space fluid removal are the keys to prevention of MTX-induced AKI.6 In addition, leucovorin, an active metabolite of folic acid, is commonly used to reduce MTX toxicities.3
We present a case of severe AKI after HD-MTX for the treatment of CNS lymphoma. Hemodialysis was instituted for severe MTX intoxication because glucarpidase was not available. The patient recovered well after treatment. We also reviewed 70 patients who received HD-MTX at our institution. Possible predictors of AKI and potential preventive strategies are discussed.
Methods
A retrospective review of patients receiving HD-MTX was conducted at NTUH. The study included patients treated with HD-MTX between May 1st, 2017, and December 31st, 2019. The Institutional Review Board at NTUH approved the study (201910088RINA). The informed consent was waived because of the retrospective nature of this study and all patient identification was removed. This study was conducted in accordance with the Declaration of Helsinki. Data were collected from medical records, including patient demographics, baseline characteristics, laboratory results, treatment protocols, and outcomes. AKI was defined as the detection of SCr higher than the upper limit of normal according to Common Terminology Criteria for Adverse Events (CTCAE). Continuous data are described as mean±standard deviation, and categorical data are described as number with percentage. The independent t-test is used to assess continuous data, while either a Chi-square or Fisher’s exact test is used to assess categorical data. A multivariate logistic regression model is constructed to identify risk factors associated with AKI. Odds ratios and 95% CI were calculated. Statistical significance is accepted at p ≤ 0.05. All statistical analyses will be performed using IBM SPSS (version 29.0, IBM Corp., New York, NY, USA).
Results
A 43-year-old man with hypertension, dyslipidemia, and diabetes mellitus, presented to the emergency department with a headache and vomiting for one month. The patient was taking metformin, pioglitazone, pitavastatin, and amlodipine for the above medical conditions. Magnetic resonance imaging of the brain revealed a well-defined mass, measuring 6x6x4.5 cm in the right temporal-occipital lobe, with prominent mass effects. Emergent craniotomy and tumor resection were performed. Histologic examination of the tumor showed diffuse large B-cell lymphoma (DLBCL). Positron emission tomography for staging revealed hypermetabolism restricted to the post-operative right temporal-occipital region. The diagnosis of primary CNS DLBCL was made.
The patient underwent adjuvant chemotherapy with HD-MTX. On examination before chemotherapy, the patient was alert and fully oriented. There were no neurological deficits after the surgery. The blood pressure was 151/95 mmHg. The weight was 117.8 kg, the height was 188.0 cm, and the body mass index was 33.3. The patient was euvolemic, and the remainder of the examination was unremarkable. No third space fluid accumulation, such as pleural effusion or ascites, was noted. Serum creatinine (Scr) level was 0.8 mg/dL, and urine pH was not measured before chemotherapy. He did not receive any medication that has known significant interaction with MTX. The patient was deemed as low risk for AKI after MTX treatment. According to the HD-MTX protocol at National Taiwan University Hospital (NTUH), the patient received an infusion of MTX at 4000 mg/m2 (9000 mg according to adjusted body surface area) for 12 hours on Day 1 (Figure 1). Hydration and urine alkalization were instituted (33.2 mEq sodium bicarbonate in 1000 mL 0.9% saline every 24 hours). Leucovorin infusion (100 mg every 6 hours) was initiated on Day 3.
 |
Figure 1 HD-MTX protocol at NTUH. Day 1 is defined as the date on which MTX infusion is initiated. On Day 1, urine alkalization, intravenous hydration, daily measurement of urine pH and body weight, and discontinuation of medications with significant interaction with MTX are also instituted. Leucovorin starts on Day 3. Daily measurement of serum MTX levels begins on Day 4 and continues until serum MTX levels are below 0.05 μmol/L. Rituximab is administered on Day 0 when included in the HD-MTX regimen. Abbreviations: HD-MTX, high-dose methotrexate; NTUH, National Taiwan University Hospital. |
On Day 4, surveillance blood tests showed severe AKI (Scr level increased from 0.8 mg/dL to 8.8 mg/dL) and a surprisingly high serum MTX level (40.61 μmol/L). Anuria developed despite the placement of a urinary catheter. The patient was at a slightly hypervolemic fluid status based on weight gain (from 117.8 kg at admission to 119 kg). Renal sonography showed bilaterally enlarged kidneys without hydronephrosis. Transient gross hematuria developed. Urinalysis showed proteinuria, glucosuria, and hematuria without dysmorphic red blood cells or casts. Severe AKI due to MTX intoxication was suspected. Because the patient had anuric AKI and glucarpidase was unavailable at NTUH, hemodialysis was promptly initiated on Day 4 within 6 hours of diagnosis of MTX intoxication to enhance elimination. Hemodialysis was performed for 4 hours at a blood flow rate of 250 mL/min and a dialysate flow rate of 500 mL/min with a high-flux dialyzer. The leucovorin dose was increased to 200 mg every 6 hours.
After the first hemodialysis session, serum MTX level decreased to 14.74 μmol/L. Urine output increased to 1920 mL per day after two consecutive daily hemodialysis treatments. He received an additional nine sessions of hemodialysis treatment until Scr and serum MTX levels decreased to 5.7 mg/dL and 2.17 μmol/L, respectively. In addition to severe AKI, the patient developed severe pancytopenia (absolute neutrophil count < 500/μL, platelet count < 1x104/μL, and hemoglobulin < 7.0 g/dL), hepatitis [alanine transaminase level up to 316 U/L (7.7 times of the upper normal limit), aspartate transaminase level up to 156 U/L (5.0 times of the upper normal limit)], and gastrointestinal toxicity (nausea and decreased appetite). These adverse events were likely attributable to MTX intoxication. His condition improved gradually under supportive care. The patient was discharged at an independent performance status five weeks after HD-MTX chemotherapy. Before discharge, his Scr level decreased to 1.3 mg/dL without hemodialysis. Serial changes in serum MTX and Scr levels were summarized in Figure 2. After discharge, the Scr levels were stable at around 1.3 to 1.4 mg/dL during a three-month follow-up at the outpatient clinic.
 |
Figure 2 Serial serum creatinine levels, serum MTX levels, and daily urine output following MTX infusion. Day 1 was defined as the date of MTX commencement, as in Figure 1. The Orange line and green dotted line denoted serial serum MTX levels and SCr levels, respectively. Arrow indicated hemodialysis treatment. Hemodialysis treatment was performed for 11 sessions and discontinued on Day 22. The below sheet shows the daily urine output of the patient. Abbreviation: SCr, serum creatinine. |
This patient’s unexpected severe adverse events prompted joint discussions among hematologists, nephrologists, and pharmacists on preventing future MTX intoxication. Severe AKI was considered the most crucial factor contributing to MTX intoxication in this patient. We retrospectively reviewed 70 patients treated by HD-MTX between May 1st, 2017 to December 31st, 2019, at NTUH and analyzed the risk factors for AKI. Among the 70 patients, 15 (21.4%) developed AKI (Table 1). Compared with patients without AKI, patients with AKI had significantly lower serum albumin levels. The mean estimated glomerular filtration rate was lower, and the proportion of chronic kidney disease was higher in patients with AKI, although statistical significance was not achieved. Notably, although the dose of MTX, the timing of serum MTX level measurement, the urine pH before chemotherapy, and the administered dose of sodium bicarbonate were similar, the first available serum MTX levels were much higher in patients with AKI than in patients without AKI (non-AKI: 1.2 ± 4.1 μmol/L vs AKI: 14.4 ± 35.1 μmol/L, p = 0.007). Notably, the proportion of patients receiving urine pH tests before chemotherapy was low [non-AKI: 13 (24%), AKI: 5 (33%)]. The proportion of patients receiving urine pH tests during D1-D3 was also low [non-AKI: 22 (40%), AKI: 8 (53%)]. Among patients who received urine pH tests during D1-D3, the proportion of patients achieving desirable urine pH level before measurement of serum MTX level was also low [non-AKI: 13 (59%) vs AKI: 4 (50%), p = 0.70], indicating unsatisfactory effects of urine alkalization.
 |
Table 1 Patient Characteristics and MTX Treatment |
To investigate the risk factors associated with AKI, we constructed a multivariable logistic regression model incorporating age, sex, serum albumin level, comorbid chronic kidney disease, MTX dose, first available serum MTX level, dose of sodium bicarbonate, and dose of leucovorin (Table 2). Only the first available serum MTX level significantly predicted the development of AKI in our cohort [odds ratio and 95% confidence interval (CI): 11.84 (2.62–53.53), p = 0.001 in the adjusted model]. Because the serum MTX level is affected by the timing of blood sampling after MTX infusion, we plotted serum MTX level against time and stratified the data according to the development of AKI (Figure 3). Compared with patients without AKI, the first available serum MTX levels were higher in patients with AKI 24 to 72 hours after MTX infusion. In addition, the index case had the highest level of serum MTX at 72 hours.
 |
Table 2 Risk Factors Associated with AKI |
 |
Figure 3 The first available serum levels of MTX in patients with or without AKI. In each patient, the levels of MTX were plotted against T1, which was the duration between the start of MTX infusion and the first available serum MTX levels. The value of MTX was logarithmically transformed with a base of 10. Green triangles denoted patients without AKI. Red inverted triangles denoted patients with AKI. The blue square denoted the index case. Linear regression with 95% CI for the association between MTX level and T1 was estimated separately in patients without and with AKI. Abbreviation: AKI, acute kidney injury. |
Discussion
We presented a case who developed anuric AKI after HD-MTX administration despite preventive measures including urine alkalization, hydration, and leucovorin supplement according to the prior protocol at NTUH. High-flux hemodialysis was performed to enhance HD-MTX elimination. The patient’s renal function partially recovered after 11 times of hemodialysis treatment. We also reviewed 70 patients who received HD-MTX at our hospital. We identified the first available serum MTX level as a significant risk factor predicting the development of AKI in our cohort.
For AKI induced by HD-MTX, prior studies reported risk factors including pre-existing impaired renal function, third-space fluid accumulation, drug-drug interactions impairing MTX clearance, and sustained elevation of serum MTX level.3,7–10 Several preventive measures were generally adopted to decrease the risk of AKI, including adequate hydration, urinary alkalization, avoidance of drug interactions, drainage of third-space fluid (when present), and serial monitoring of MTX serum concentration with appropriate leucovorin rescue.5,6,11,12 Adequate hydration can augment urinary flow rate and enhance urinary clearance of MTX. Alkalization of urine can increase the urinary solubility of MTX. After raising the urine pH level from 6.0 to 7.0, the solubility of MTX and its metabolites increases about 5 to 8-fold.3 Drainage of third-space fluid prevents accumulation of MTX in the third-space. Serial monitoring of MTX serum concentration enables early detection of AKI. Ramsey et al presented guidance for serial serum MTX concentration measurement.5 Measurement of serum MTX levels routinely at 24 and 48 hours after MTX administration is suggested. Additional measurements may be needed if an elevated serum MTX level is detected. Adjustment of leucovorin dose based on MTX serum concentration is proposed to reduce MTX toxicity.1,7
In our index case, AKI developed after HD-MTX administration despite preventive measures based on protocol at NTUH. After discussion with oncologists and pharmacists, we consider the following measures in the protocol can be modified to reduce future AKI complications. First, the timing of serum MTX concentration measurement. Second, fluid administration for urine alkalization and hydration. Third, urine pH measurement. Fourth, a dose of leucovorin. The modified protocol is illustrated in Figure 4.
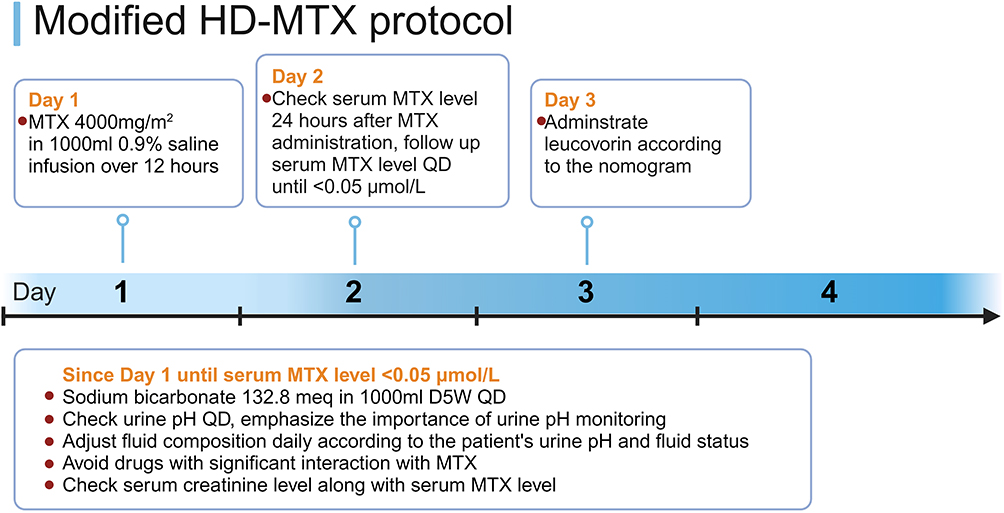 |
Figure 4 Modified HD-MTX protocol at NTUH. In the modified HD-MTX protocol, several preventive measurements are changed. First, serum MTX level is checked at 24 hours rather than 48–72 hours after MTX initiation. Second, urine alkalization is changed from sodium bicarbonate 33.2 mEq in 1000 mL 0.9% saline to sodium bicarbonate 132.8 mEq in 1000 mL 5% dextrose in water. Third, the importance of daily urine pH measurement is emphasized. Fourth, leucovorin is administered according to the nomogram rather than a fixed dose of 100mg Q6H. Fifth, serum creatinine level is checked along with serum MTX level. The infusion time of MTX infusion time may be adjusted based on clinical judgment. |
In our cohort of 70 patients receiving HD-MTX, the first available serum MTX level was obtained at 55.0 ± 18.4 hours after the start of MTX infusion. This timing was much delayed, and we should manage to obtain serum MTX level at 24 hours according to the literature.5 Delayed measurement of serum MTX level may contribute to delayed diagnosis and may hamper timely management of MTX intoxication. Our prior protocol suggests fluid administration with sodium bicarbonate 33.2 mEq in 1000 mL 0.9% saline daily since D1 for urine alkalization and hydration. However, among patients with available urine pH reports, the proportion of patients having urine pH ≥ 7.0 during D1-D3 was only 57%. We suggest the fluid composition be changed to sodium bicarbonate 132.8 mEq in 1000 mL 5% dextrose in water (D5W) daily. Compared with the prior regimen, the new fluid composition has the advantages of higher alkali load, lower sodium load, and lower fluid tonicity. The fluid composition may be individually adjusted daily based on urine pH and fluid status.13 Notably, only a small proportion of patients in our cohort had available urine pH reports before (26%) and during D1-D3 (43%) after MTX administration. We must emphasize the importance of urine pH monitoring before and during MTX administration at our institution. Our current protocol suggests a fixed dose of leucovorin rescue (100 mg every 6 hours after 48 hours of HD-MTX infusion). Because pharmacokinetically guided leucovorin rescue based on serum MTX level may reduce toxicity,14 we suggest leucovorin be dosed according to the standard nomogram.1 Notably, timely measurement of serial serum MTX levels is mandatory for the successful application of leucovorin dosing nomogram. In our index patient, the serum MTX level after 72 hours of MTX infusion exceeded 40 μmol/L. According to the nomogram, the leucovorin dose should be increased to 1000 mg/m2 per 6 hours, but the patient actually received only 200 mg every 6 hours. The insufficiency of leucovorin dose might result in inadequate intracellular leucovorin levels and lead to severe MTX toxicities. Importantly, leucovorin can be removed by hemodialysis, and a supplement dose may be needed after hemodialysis treatment.15
Based on the literature,5 glucarpidase should be considered in patients with ongoing AKI and high serum MTX levels despite preventive measures such as urine alkalization and hydration. Glucarpidase, a recombinant enzyme, is specifically designed to hydrolyze methotrexate into inactive metabolites, thereby facilitating its elimination. It has demonstrated efficacy in rapidly lowering serum methotrexate levels, particularly in patients with impaired renal function and delayed clearance.5 However, due to its high cost, glucarpidase is not readily available in many institutions, including ours. Retrospective studies have shown that patients receiving glucarpidase had reduced hospital length of stay, inpatient mortality, and 90-day mortality compared to those not receiving glucarpidase, including patients treated with hemodialysis.16 Given these clinical benefits, economic simulation analyses suggest that glucarpidase is more cost-effective than hemodialysis.17 Therefore, the availability of glucarpidase for patients experiencing methotrexate intoxication is an urgent necessity.
Due to lack of glucarpidase, the index patient received high-flux hemodialysis for the treatment of MTX intoxication. The role of extracorporeal treatment for MTX intoxication is reviewed by Ghannoum et al.2 MTX is a relatively small molecule (molecular weight 454 dalton) with a relatively low volume of distribution (0.4–0.8 L/Kg) and 50–70% protein binding. Circulating MTX can be removed by hemodialysis, but rebounding of serum MTX concentration can occur rapidly after cessation of hemodialysis due to tissue redistribution. The 2022 EXtracorporeal TReatments In Poisoning (EXTRIP) workgroup did not recommend extracorporeal treatment use for severe methotrexate toxicity as an addition to standard care including glucarpidase.2 However, extracorporeal treatment can be considered in several special situations, such as when glucarpidase is not available. In our index patient, eleven sessions of high-flux hemodialysis were performed until serum MTX concentrations were < 2.0 μmol/L. Because glucarpidase is not available in Taiwan, high-flux hemodialysis may be considered in patients with extremely high serum MTX concentrations and impaired urinary MTX clearance.
In summary, we reported a case of severe AKI and MTX intoxication after HD-MTX administration. High-flux hemodialysis was instituted to enhance MTX elimination. We reviewed 70 patients receiving HD-MTX at NTUH and identified serum MTX level as a risk factor for the development of AKI. We proposed a new HD-MTX protocol to reduce future complications after HD-MTX at our institution. This report may interest healthcare personnel who care for patients under HD-MTX treatment.
Ethics Approval and Consent to Participate
A retrospective review of patients receiving HD-MTX was granted a waiver of informed consent by the Institutional Review Board at NTUH (201910088RINA).
Consent for Publication
The index patient provided written informed consent for publication.
Acknowledgments
We thank the nursing staff for caring for patients at the National Taiwan University Hospital. We thank Mrs. Hsiu-Chin Lee Kidney Research Fund for supporting this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Chien-Chih Wu was supported by the National Taiwan University Hospital (NTUH-113-S0214 and NTUH-113-S0036).
Disclosure
All the authors declared no competing interests.
References
1. Howard SC, McCormick J, Pui CH, Buddington RK, Harvey RD. Preventing and managing toxicities of high-dose methotrexate. oncologist. 2016;21(12):1471–1482. doi:10.1634/theoncologist.2015-0164
2. Ghannoum M, Roberts DM, Goldfarb DS, et al. Extracorporeal treatment for methotrexate poisoning: systematic review and recommendations from the EXTRIP workgroup. Clin J Am Soc Nephrol. 2022;17(4):602–622. doi:10.2215/CJN.08030621
3. Widemann BC, Adamson PC. Understanding and managing methotrexate nephrotoxicity. Oncologist. 2006;11(6):694–703. doi:10.1634/theoncologist.11-6-694
4. Garneau AP, Riopel J, Isenring P. Acute methotrexate-induced crystal nephropathy. N Engl J Med. 2015;373(27):2691–2693. doi:10.1056/NEJMc1507547
5. Ramsey LB, Balis FM, O’Brien MM, et al. Consensus guideline for use of glucarpidase in patients with high-dose methotrexate induced acute kidney injury and delayed methotrexate clearance. Oncologist. 2018;23(1):52–61. doi:10.1634/theoncologist.2017-0243
6. Alsdorf WH, Karagiannis P, Langebrake C, Bokemeyer C, Frenzel C. Standardized supportive care documentation improves safety of high-dose methotrexate treatment. oncologist. 2021;26(2):e327–e32. doi:10.1002/onco.13603
7. Bleyer WA. Methotrexate: clinical pharmacology, current status and therapeutic guidelines. Cancer Treat Rev. 1977;4(2):87–101. doi:10.1016/S0305-7372(77)80007-8
8. Li J, Gwilt P. The effect of malignant effusions on methotrexate disposition. Cancer Chemother Pharmacol. 2002;50(5):373–382. doi:10.1007/s00280-002-0512-9
9. Joerger M, Huitema AD, Illerhaus G, Ferreri AJ. Rational administration schedule for high-dose methotrexate in patients with primary central nervous system lymphoma. Leuk Lymphoma. 2012;53(10):1867–1875. doi:10.3109/10428194.2012.676177
10. Li W, Mo J, Yang Z, Zhao Z, Mei S. Risk factors associated with high-dose methotrexate induced toxicities. Expert Opin Drug Metab Toxicol. 2024;20(4):263–274. doi:10.1080/17425255.2024.2332366
11. Green MR, Chowdhary S, Lombardi KM, Chalmers LM, Chamberlain M. Clinical utility and pharmacology of high-dose methotrexate in the treatment of primary CNS lymphoma. Expert Rev Neurother. 2006;6(5):635–652. doi:10.1586/14737175.6.5.635
12. Song Z, Hu Y, Liu S, et al. Medication therapy of high-dose methotrexate: an evidence-based practice guideline of the division of therapeutic drug monitoring, Chinese pharmacological society. Br J Clin Pharmacol. 2022;88(5):2456–2472. doi:10.1111/bcp.15134
13. Perazella MA, Moeckel GW. Nephrotoxicity from chemotherapeutic agents: clinical manifestations, pathobiology, and prevention/therapy. Semin Nephrol. 2010;30(6):570–581. doi:10.1016/j.semnephrol.2010.09.005
14. Stoller RG, Hande KR, Jacobs SA, Rosenberg SA, Chabner BA. Use of plasma pharmacokinetics to predict and prevent methotrexate toxicity. N Engl J Med. 1977;297(12):630–634. doi:10.1056/NEJM197709222971203
15. Relling MV, Stapleton FB, Ochs J, et al. Removal of methotrexate, leucovorin, and their metabolites by combined hemodialysis and hemoperfusion. Cancer. 1988;62(5):884–888. doi:10.1002/1097-0142(19880901)62:5<884::AID-CNCR2820620506>3.0.CO;2-A
16. Demiralp B, Koenig L, Kala J, et al. Length of stay, mortality, and readmissions among Medicare cancer patients treated with glucarpidase and conventional care: a retrospective study. Clinicoecon Outcomes Res. 2019;11:129–144. doi:10.2147/CEOR.S188786
17. Kala J, Nelson R, Drudge C, Zhou A, Ward S, Bourque M. Glucarpidase for treating adults with delayed methotrexate elimination due to impaired renal function: an economic simulation analysis. Clinicoecon Outcomes Res. 2023;15:165–179. doi:10.2147/CEOR.S397154
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.